
Abstract
Keywords
This paper compares public health and legal policies to reduce the harm associated with cannabis use in Canada and Australia. Both countries have similar problems in this area. In Canada, data on the consumption of psychoactive substances, alcohol, tobacco and illegal drugs come from national surveys conducted from 1985 to 1994 [1], [2]. Nearly 25% reported consuming cannabis at least once in their lifetime, with higher rates for men, those under 35 years old, and residents of British Columbia and Alberta [2].
An alternative way of measuring prevalence is cannabis use over the previous 12 months. This may be a more sensitive indicator, as reporting is less dependant on long-term memory [1]. Approximately 5–10% of the adult population had used cannabis in the previous year and there is a similar pattern as in lifetime use, with higher rates for men and those under 30 years old (3]. About half of the marijuana available in Canada is produced in British Columbia, Ontario and Quebec [1].
Cannabis use in the previous 12 months 1998–2001 (adults <30)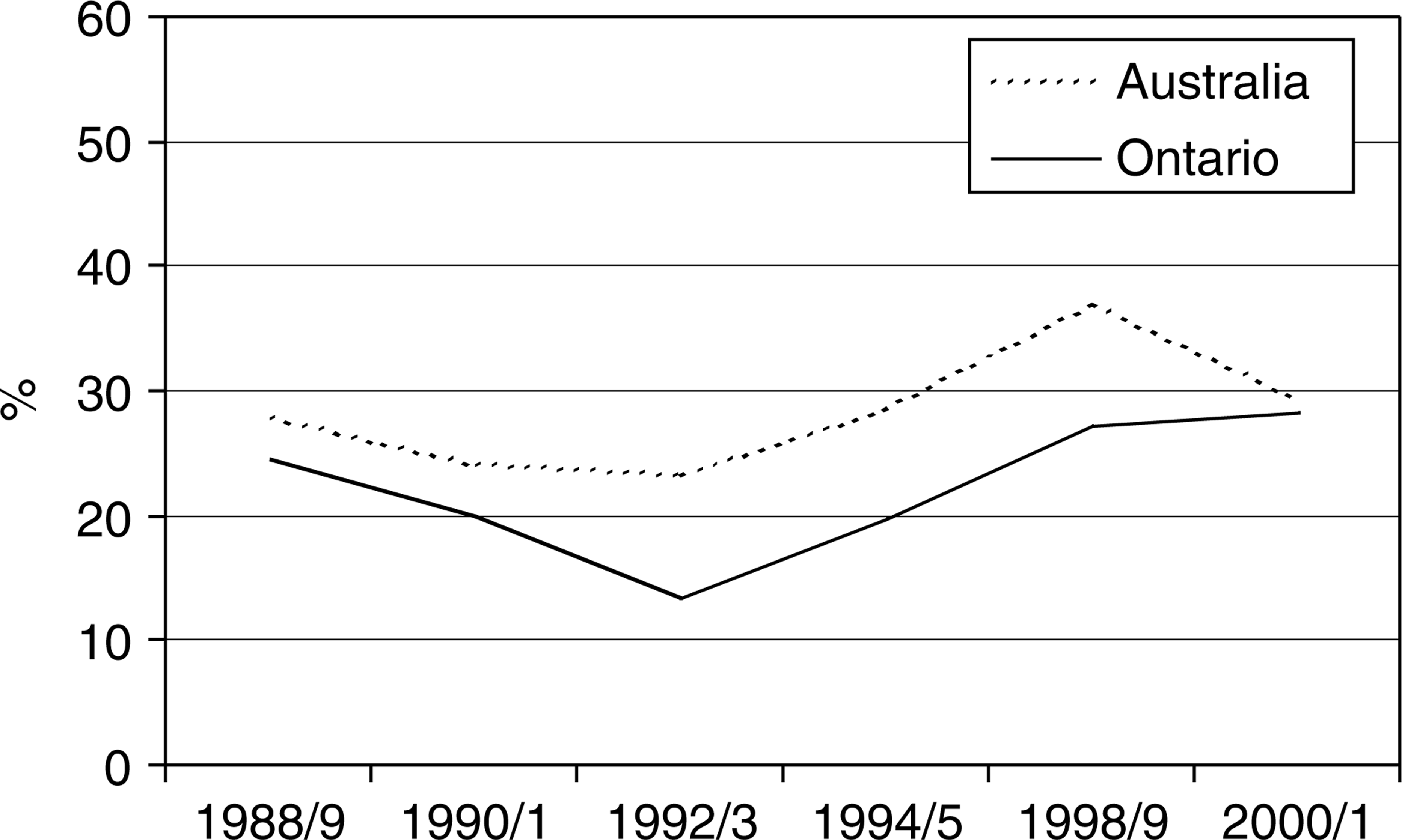
Cannabis use in the previous 12 months for Canada and Australia (adults >18)
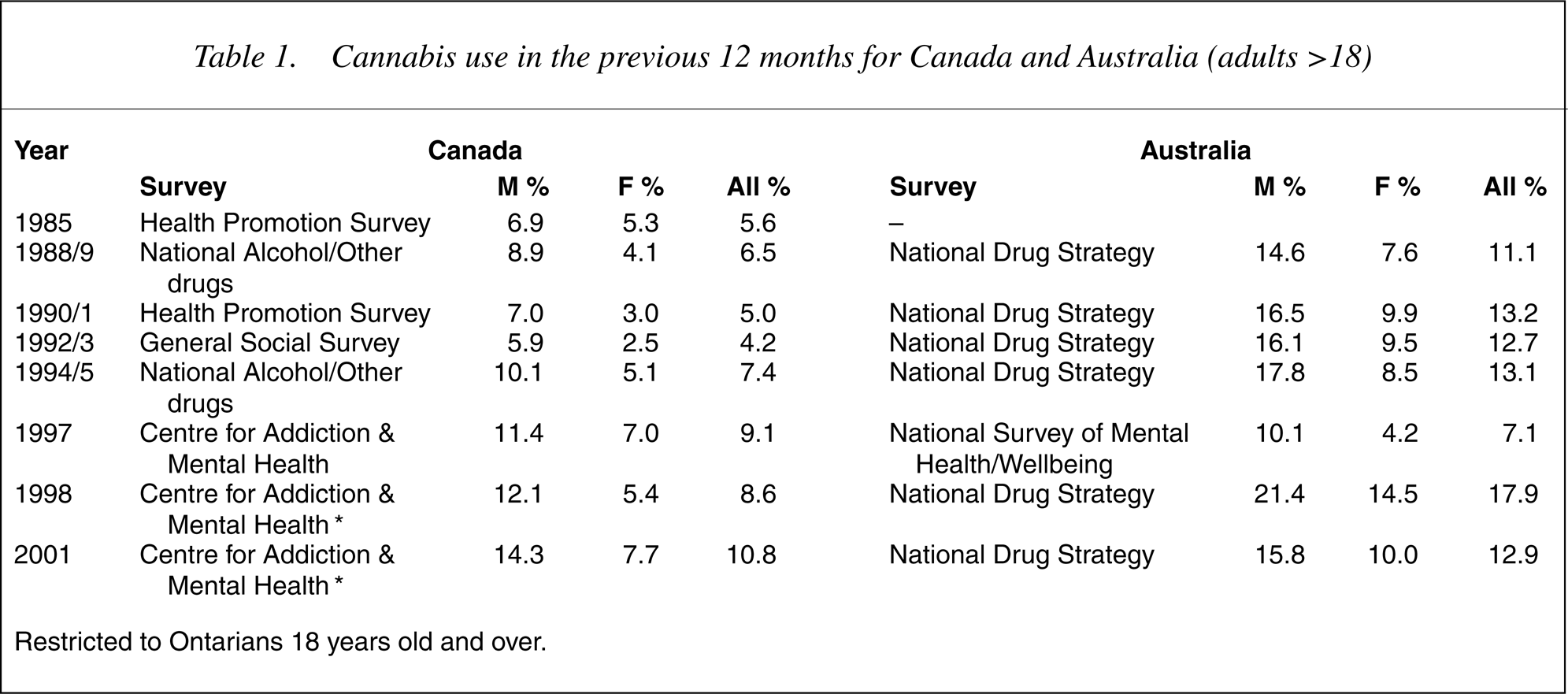
Restricted to Ontarians 18 years old and over.
These figures are similar to those in Australia [4–9], where most information on substance use comes from the National Drug Household Survey [7], [9]. This has been carried out every 2–3 years since 1985. In 2001, a third of the population had used cannabis in their lifetime [9]. Depending on the survey, rates of use among adults in the previous 12 months tend to be higher than in Canada at between 10 and 18%. (10]. However, a major problem in comparing both countries is the absence of a national drug survey in Canada since 1994. Of the provinces, only Ontario has had regular community drug surveys of the same frequency as the National Drug Household Survey in Australia [1], [7] (11].
Adverse affects
Problems of acute intoxication include increased risks of accidents with motor vehicles or machinery, or adverse reactions [1], [6], [12], [13]. Findings are more equivocal for longer-term effects. Dependence may occur in 10–20% of users, but symptoms are less severe or frequent than alcohol or tobacco dependence [4]. Because of the difficulty of distinguishing between the causes and effects of cannabis use, and the absence of controlled studies, no firm conclusions can be reached as to the existence of an amotivational syndrome [4]. Long-term use may lead to subtle cognitive impairments in areas such as memory, attention, and the organization and integration of complex information, but these are considerably less than those found in chronic heavy alcohol use [12].
Several long-term cohort studies from Australasia, Sweden and the US suggest an association between cannabis use and subsequent risk of schizophrenia and depression [2], [4],[14–16]. Assuming causality, it has been estimated that the elimination of cannabis use would reduce the incidence of schizophrenia by approximately 8% at a population level [16]. A dose–response curve for both conditions suggests that reducing levels of use may reduce the incidence of illness, although we still do not know whether cannabis use only triggers illnesses in people who were already vulnerable, or actually causes them in people who would not have otherwise fallen ill [14]. Most studies are unable to establish whether prodromal symptoms of schizophrenia preceded cannabis use [16]. Even if there is a causal relationship, cannabis is only one of a number of predisposing or precipitating factors [16].
Studies have also noted an association between the rise in youth suicide and the use of alcohol and other drugs, especially cannabis in the 15–24 years old age group [6]. Cannabis intoxication may lead to impulsive self-harm, and long-term use to the exacerbation of pre-existing mental disorders [12]. However, we do not know whether this is a direct association, or if it is dependent on other factors that may be causing both, such as social deprivation, environmental or familial factors in earlier life [2]. Similarly it is difficult to separate the effects of comorbid alcohol use [6].
In terms of physical side-effects, smoking cannabis can also result in chronic lung disease such as bronchitis and carcinoma of the upper respiratory tract [12]. There may also be endocrine or reproductive changes but findings are equivocal, and reported changes minor [2], [4]. Women who continue to smoke during pregnancy may increase the risk of a low birth weight baby [6].
These findings have implications for public health and legal policies on cannabis use. Both Australia and Canada have adopted a policy of harm minimization. This accepts that the eradication of psychoactive substances is impossible and may result in greater harm to society [14], [17]. The policy has three components: law enforcement to reduce supply, harm reduction and demand reduction through education and service provision.
Law enforcement
The past situation
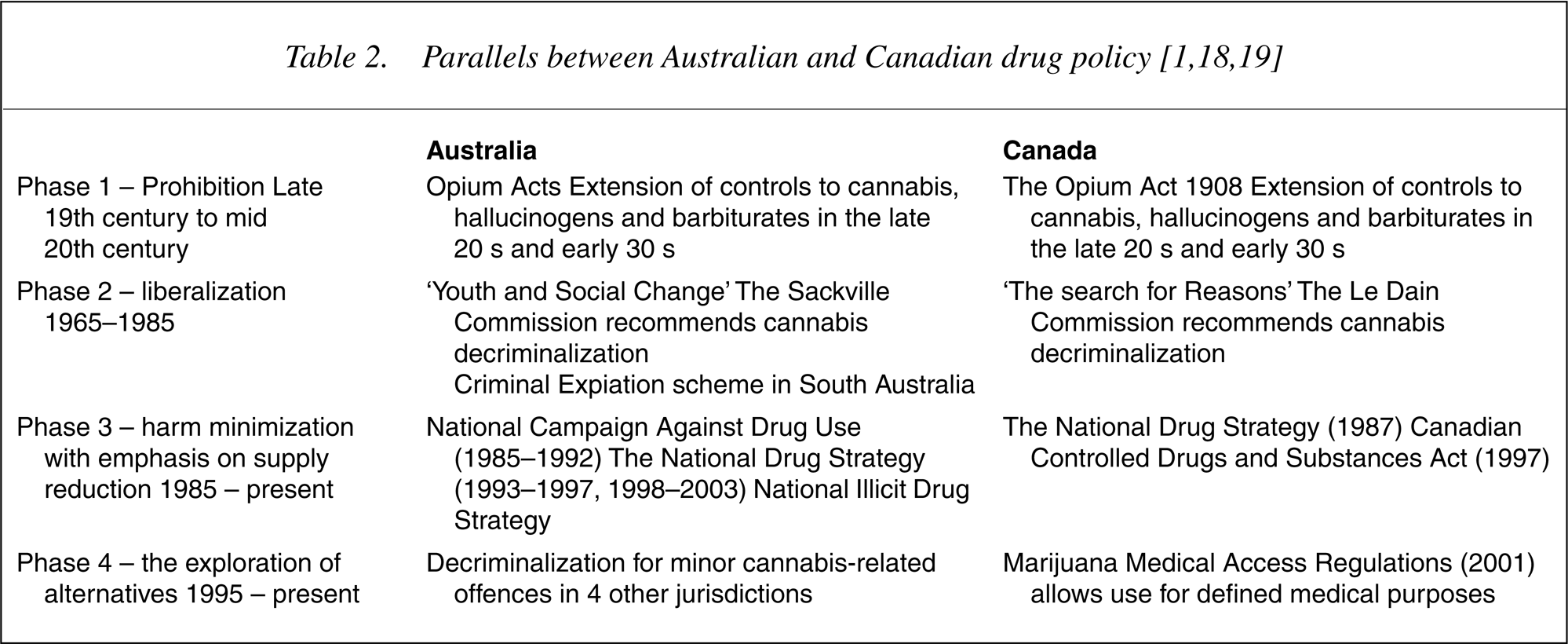
The history of law enforcement in Canada has been reviewed by a Senate Inquiry in Canada and has parallels with Australia [1], [18] (19]. In Canada, these regulations became increasingly severe including the introduction of wider police powers of search and forfeiture, as well as a reverse onus provision. This meant an accused person had to prove that he/she had not committed a crime with which they were charged.
Although there had been considerable medical interest in the use of cannabis for therapeutic purposes at the end of the 19th century [20], [21], its use waned, and by the early 1930s, controls were extended to cannabis, hallucinogens and barbiturates [1], [18], [19]. This was partly in response to pressure from the US where, again, links were made between certain drugs and isolated minorities. In this case, as well as linking Chinese immigrants to opium, cannabis was linked to Mexicans [19].
Phase 2 in both countries was accompanied by a period of social change and youth protest in both countries. The Le Dain Commission in Canada (1972) and the Sackville Commission in South Australia (1976) both recommended the decriminalization of cannabis [1], [18], although only South Australia proceeded with the introduction of a Cannabis Expiation Notice (CEN) scheme [1], [18].
By the mid-80 s the legislative climate had changed and following the declaration by US President Reagan of a ‘war on drugs’, both countries became increasingly involved in international efforts to combat drug trafficking [1]. National drug strategies in both countries reflected the change in emphasis from decriminalization to a mixture of supply reduction and harm reduction (Phase 3) (1]. Of the $620 million spent by commonwealth, state and territory governments in Australia in 1992 on their response to illicit drugs, 84% was allocated to law enforcement, 6% to treatment and 10% to prevention and research. Phase 3 was accompanied by an increasing complexity in legislation with harsher penalties for trafficking and/or the use of ‘hard’ drugs.
The present situation
Both Australia and Canada have a federal system of government with responsibility for law enforcement divided between provincial and federal authorities. Unlike Australia, the decision to prosecute in Canada rests with the Federal Prosecution Service (FPS), not state authorities.
In spite of the high expenditure on supply reduction, indicators of cannabis use are either steady or rising. Surveys of drug use in both countries show no decrease in self-reported current use (1].
The number of incidents related to drugs has also nearly doubled to 92 000 per year from 1995 to 2001 [1]. Most of this increase was due to cannabis-related offences. In 2001, cannabis-related offences accounted for 71 624 of reported incidents, almost 77% of all drugrelated incidents. Of these, 70% were for possession, 16% for trafficking, 13% for cultivation, and 1% for importation [1]. Thus, more than a half of all reported drug-related incidents are for possession. In Australia, cannabis accounted for 70% of all illicit drug arrests in 1998–1999 [1].
This apparent lack of response to the initiatives of the past has led to renewed interest in alternatives to supply reduction (Phase 4). One is the diversion of people caught in possession of cannabis away from the criminal justice system to heath services. Although incidents related to drugs have increased in Canada, prosecutions by the FPS have declined in the same period to as low as 35% in some areas [1].
A further development in Canada has been the introduction of the Marijuana Medical Access Regulations in 2001 that allow use for defined medical purposes. These include terminal illness, uncontrolled seizures and severe pain secondary to multiple sclerosis, spinal cord disease, carcinoma or AIDS [1]. However, there has been limited uptake because of the reluctance of physicians to participate secondary to medico-legal concerns and the lack of access to legal sources of cannabis [1].
In Australia, there is now a greater emphasis on education and treatment. The National Illicit Drug Strategy has established ‘drug courts’ to divert people into rehabilitation services [1], [6]. Some jurisdictions such as the Australian Capital Territory and the Northern Territory have followed the lead of South Australia and experimented with criminal expiation schemes. Victoria and Western Australia have introduced cautions for minor cannabis offences. The latest phase of the National Drug Strategy reaffirms the Commonwealth Government's commitment to harm minimization and also includes a plan targeted at Aboriginal and Torres Strait Islanders [22]. However, although the document refers to evidencebased practice, there is no mention of evaluating the effects of decriminalization in several Australian jurisdictions.
Financial and social costs
The annual costs for drug enforcement in Canada are between $700 million and $1 billion [1]. A further $5 million is spent in prosecuting people for cannabis possession [1]. In Toronto, drug investigations account for up to a third of the police budget [1]. Recent figures for Australia suggest that enforcing the law on illicit drugs costs the criminal justice system $500 million a year [1]. A comparison of three European countries, Australia, Canada and the US showed that cannabis consumption appeared to be unaffected by the amount of money spent on enforcing legislation [1]. Given the opportunity costs in terms of other police priorities, amendments to legislation on cannabis could produce substantial savings or redeployment of police resources to more effective areas.
Social costs include the stigma of arrest, lost incomes and ruined careers [1]. If prohibition does deter some people from trying illicit drugs, many are not deterred and, for some, the forbidden status of the drug is actually attractive [6]. Informal social controls and socio-cultural norms may be more important than formal controls in influencing drug use [6].
Imprisonment of otherwise law-abiding citizens for the use of cannabis can criminalize them and have unnecessarily harsh consequences [6]. Many are already socially disadvantaged and so criminal penalties are particularly difficult to bear [1]. In the US, there is evidence that certain racial groups are disproportionately represented in arrests for cannabis possession, with half of those arrested being of Hispanic origin [23]. Young males are also more likely to be charged than other groups [1]. The legal system can lose respect if penalties are inappropriately harsh and out of step with community values [6].
Aside from the financial and social cost, another criticism of law enforcement is that it is ineffective. Consumption of cannabis continues to grow irrespective of whether there is strict law enforcement or not, and there is no evidence that this has been any greater in countries where laws have been liberalized [1]. In the 11 American states that effectively decriminalized cannabis use in the 1970s, use has not risen beyond that experienced by comparable states where it is prohibited [24]. An identical picture is seen in Australia, where the introduction of the CEN scheme in South Australia was not associated with an increase in cannabis use compared to other states. Similarly, the Netherlands, where cannabis was effectively decriminalized 25 years ago, has a similar prevalence to that in Germany and France and well below that in the United States [24]. There is no direct relationship between consumption levels and public policy direction [1]. Very liberal countries show low rates (Spain, the Netherlands, Portugal), whereas countries that have very restrictive policies stressing prohibition and abstention show high rates (USA, Canada, France).
Similarly, there appears to be no direct relationship between the type of public policy and arrests. Switzerland and Australia, both of which have far more moderate policies than the US, arrest proportionally larger numbers of people than that country, although Switzer-land's consumption rate is far lower than that of the US, and Australia's is virtually the same [1].
There are also no hard data as to whether cannabis is a ‘gateway’ drug that leads to use of other drugs. Although cannabis is usually the first illicit drug of use of those who subsequently use opiates or cocaine, adolescents who start using cannabis early are independently at risk of using other drugs. In addition, early initiation to cannabis and use of other drugs may both be dependant on predisposing factors in the environment. They are also more likely to have peers who are heavy users [25].
Proponents of law enforcement argue that the health effects of cannabis are often underestimated [26], [27]. A World Health Organization report concluded that cannabis smoke is twice as carcinogenic as tobacco [26]. Even if the incidence of adverse events such as dependence, respiratory disease, psychiatric problems and low-birth weight babies is low, the potential public health impact is high because of the prevalence of cannabis use [6], [27]. The number of cannabis users seeking treatment has doubled in the last 10 years in the UK, and the psychological consequences (e.g. suicide) although unproven may be catastrophic [26]. Legalization may not curtail the black-market as two-thirds of cannabis sales in the Netherlands take place outside designated coffee shops [26].
If cannabis were legalized, there would be the risk that use would increase through aggressive marketing as it would be impossible regulate the market [26]. Governments would be no more successful in controlling the cannabis industry than they have been with the tobacco industry [26]. An Australian study suggested that there was a high risk of being killed while driving under the influence of cannabis [6]. In a UK study of fatal road accidents, no alcohol was found in 80% of people found positive for cannabis at autopsy [26]. Cannabis has been compared with tobacco in terms of the potential for causing mortality and morbidity particularly carcinoma, respiratory disease and myocardial infarction, although data come from small clinical rather than epidemiological studies [27]. In one study, myocardial infarctions were over four times as likely to occur in the hour after smoking cannabis [26]. If cigarettes cause an annual excess of 120 000 death among 13 million smokers, the corresponding excess mortality among 3.2 million cannabis smokers would be 30 000 [27].
However, experience in Australia has shown that a mixture of education and law enforcement has been successful in reducing the rate of licit drugs such as tobacco [28]. As regards excess morbidity and mortality from cannabis, it is misleading to extrapolate from small studies, and there are no supporting data from epidemiological surveys in Sweden and the US [29]. The length of exposure also needs to be considered. Whereas the proportion of older adults who smoke cigarettes is 60% that of younger people, the proportion for cannabis in older adults is only 18% [29].
Prevention through education and treatment
Prevention includes screening and early treatment for those encountering problems with cannabis. Education refers to both individual lifestyle and social/systemic approaches that consider the political, legislative and physical environments in which cannabis use occurs [30]. These might be family or school factors such as parental attitudes and poor academic performance, or peer and environmental factors such as drug availability and social deprivation.
As in Australia, education and treatment in Canada fall within the remit of provincial or state governments. A review by the Senate Committee found that resources for both were inadequate [1]. While the United States spent about $12 per capita on prevention awareness, Canada spent less than $1 [1].
The Royal Canadian Mounted Police (RCMP), runs the only comprehensive education program in Canada [1]. The Drug Abuse Resistance Program uses an exclusively individual lifestyle approach to teach resistance to peer pressure, the ability to make personal choices, conflict resolution and anger management. It is delivered by a uniformed police officer and includes lectures, group discussions, audio-visual presentations, exercises and role-playing. Although there is high satisfaction with the program, changes in behaviour are much harder to measure and appear to be short-term [1]. Work from Australia suggests that drug education in schools cannot be done in isolation from efforts to create community partnerships, improve the functioning of local community institutions and foster peer-lead initiatives [6].
Mass media campaigns may have a role in setting the agenda but have to be complemented with other approaches to counter contradictory messages from personal sources such as peers or family. The National Action Plan on Illicit Drugs in Australia highlights the need to maximize benefit through analysis of the environment, audience and channel of communication with review of the process and outcome [6]. Any approach also has to consider protective and risk factors with developmental interventions at early stages of pathways to antisocial behaviour [6].
In terms of harm reduction, work in Canada has focused on opiate rather than cannabis use [1]. As with the harmful effects of injecting opiates, this might focus on the risks associated with heavy, frequent use over a long period and those associated with impaired driving, especially when the cannabis is mixed with alcohol.
Treatment services for this population are underdeveloped as most specialist drug teams are geared towards helping users of opiates [26]. This is in spite of figures from the UK where the number of cannabis users seeking specialist help doubled over 10 years [26].
When planning treatment services for cannabis users, we need to consider the low rate and intensity of dependence compared to other drugs. About 10% of regular users are at risk of becoming dependant, although a withdrawal syndrome has not been clearly defined probably because of the long half-life of THC [6]. Immediate management is supportive with treatment of any adverse effects. In terms of longer-term interventions, there are no data on cannabis specifically but social skills training, motivational interviewing and community reinforcement approaches may be effective [1].
Those in greatest need, such as marginalized young people, may not use services for early treatment. We also do not know how effective services are for cannabis users, as opposed to users of other illicit drugs [6]. As with all health promotion, changes in knowledge may not translate into behavioural change. However, given each prosecution in Canada costs $4500, and imprisonment costs an average of $47 000, these approaches are likely to be rather more cost-effective [1].
Conclusions
This review of public policy on cannabis demonstrates a heavy reliance on legislative and punitive approaches to control in both Canada and Australia that have failed to arrest the increase in cannabis use, especially among young people. This is in contrast to tobacco, which as a licit drug has been the focus of considerable health promotion (with some health protection such as banning sales to those under 16 years old). Overall rates of tobacco use are falling and tobacco use is less than that of cannabis in some surveys of young people [3].
A Senate inquiry in Canada has recommended an alternative approach with the liberalization of laws on the possession of cannabis for personal use while tightening legislation against operating vehicles or machinery while intoxicated [1]. These are only recommendations, and it is unclear whether the Canadian government will adopt them. In adopting change, Canada would be in contravention of several international conventions and treaties governing drugs. This is likely to be opposed by the US, with the risk of disruption to cross-border trade.
Canada has also experimented with legalized access to cannabis for medical reasons, although uptake of the scheme has been limited. Lessons for both countries in this area include greater consultation with the medical profession, access to research-grade cannabis and less restrictive criteria for eligibility [1]. This might include removing the requirement that all conventional treatments have been considered. We also need more information on the optimal dose and route of administration, as well as therapeutic and adverse effects [20].
In turn, Canada can learn from Australia's experience in decriminalizing the possession of small amounts of cannabis in several states. In particular, the CEN scheme in South Australia has not been associated with an increase in cannabis use compared to prohibitionist states. Unlike Canada, where there has been no national drug survey since 1994, Australia has conducted these every 2 to 3 years with the results of the latest one in 2004 expected shortly.
More research is also required to quantify differences between types of cannabis product and the physical or psychiatric consequences, including the effect on fitness to drive [25]. More research is also needed to evaluate different national policies and the impact that this has on cannabis use. If alternatives to decriminalization are considered, which strategy produces the best results? Is it the coffee-shop model in the Netherlands or a scheme that tolerates home cultivation of small quantities as in Alaska, South Australia or Western Australia [31]? More data may mean that decisions made by policy-makers are based on better evidence than past decisions [25].