
Abstract
Objective:
To measure the provincial government cost of mental health–related activities for youth ages 12 to 17 in Alberta in 2014 to 2015.
Methods:
The target population was Alberta youth ages 12 to 17 (the federal justice definition) who received or were funded for mental health–related or complementary services from Alberta Health Services, Alberta Health, Alberta Human Services, Alberta Justice and Solicitor General, and Alberta Education (public schools). Data on services and expenditures were obtained from each source for the target youth population.
Results:
Costs for mental health–related services for all ministries were $175 million for 27,169 youth who used mental health services as defined by Policy Wise, $6460 per youth. Public school special education supplements for youth with emotional problems was the largest group, amounting to 30% of all costs. Other prominent sources of expenditures were hospital inpatient mental health services (18%), community mental health services (11%), physician mental health services (10%), and secure services with treatment requiring judicial approval (9%).
Conclusion:
Economists in several countries have developed countrywide measures of mental health expenditures and have used these to generate national benchmarks for mental health spending. We have estimated spending for Alberta provincial mental health and addiction services for a distinct and highly vulnerable group. This measure can be used to develop measures and benchmarks for other provinces, which will be valuable policy indicators.
Keywords
Both the Canadian Mental Health Commission 1 and the Canadian Centre on Substance Abuse and Addiction 2 have emphasized the importance of mental health and addiction issues among Canadian youth nationwide. Currently, we do not have a unified measure of the resources committed to youth mental health and addictions in any province in Canada, one that incorporates services of the major providers of mental health, addiction, and complementary services.
In Alberta, youth with mental health and addiction problems are served by a variety of public agencies, with varying degrees of coordination between them. The various organizations have separate budgets, and publicly available details are insufficient to provide a comprehensive view of the public resources directly devoted to youth mental health and addictions problems.
We conducted a cross-ministerial survey of public mental health–related spending in Alberta for youth who have used the basic mental health system. Using a variety of sources including data collected by agencies, publicly available budgets, publicly published documents, and direct information, we estimated the number of youth served and the annual public expenditures in Alberta for these services.
Methods
Setting
Youth with mental health and addiction problems are served by a variety of agencies in Alberta. Alberta Health (AH), the health ministry, funds physician services and some pharmaceuticals. Alberta Health Services (AHS) provides or funds community clinics, hospital emergency and inpatient care, and treatment residences. AHS is primarily funded by AH. The Children’s Services ministry directly provides or funds family enhancement services and child intervention programs for those with a demonstrated social need. The Human Services Department operates the Child and Family Services support program; mental health disability is one criterion for this support. The Justice and Solicitor General provides prosecution, court and sentencing services, and alternative judicial services. Forensic mental health services within the criminal justice system are provided by AHS. The municipal police, along with provincial mental health and social service agencies, provides alternative judicial measures that have preventive components.
Our target population is children between the ages 12 to 17; this grouping is used in the federal Youth Criminal Justice Act. 3 We used the fiscal year 2014 to 2015 as our period of analysis, because that was the last year for which some indicators were available when we conducted the analysis. In some cases where 2014/2015 data were not available, we used the adjacent year, 2015/2016. We did not adjust for inflation between these 2 years, as the annual inflation rate for Alberta was 2%, and the differences between the 2 years would not be material.
Benchmark Population
The benchmark population includes those who have received mental health services and support as defined in the Child and Youth Data Laboratory (CYDL) database developed by Policy Wise, an Alberta research organization devoted to the analysis of child and family services. 4 This comprises youth who received hospital, emergency department, and physician services with primary mental health diagnoses and/or those who received support for mental health disabilities from Alberta Child and Family Services (ACFS).
Services and Costs
In Supplemental Appendix 1, we present the methods used to estimate total annual expenditures and number of distinct users for each of the services in our analysis. We summarize our sources as follows.
Hospital inpatient and emergency care is provided by AHS. Data were obtained from AH. Utilization data for inpatient cases with a mental health or substance abuse diagnosis were obtained from the Canadian Institute for Health Information (CIHI) discharge abstract database (DAD), using mental health and addictions International Classification of Diseases, 10th Revision (ICD-10) codes (see Supplemental Appendix). An unduplicated count of users was obtained. AH obtained a cost per case using the CIHI resource intensity weights (RIWs) for each case. The RIWs are relative index weights; these were monetized using a standard cost per hospital stay (SCHS) developed by CIHI for Alberta hospitals. Emergency visits for mental health and addictions were obtained from AH in a similar way, using the same diagnosis codes, RIWs, and costs per visit. Physician service data were also obtained from AH, using physician billings. Billings were for claims in the Diagnostic and Therapeutic Psychology and Psychiatry group of services. These claims were reported separately by specialty. The unduplicated number of patients was also obtained for each physician specialty group. We requested AH to add shadow billings for services provided by physicians who were not funded by fee-for-service.
Community mental health and addiction services are provided by AHS, which also provided data on costs and number of persons served. AHS provided data for 3 types of services: community outpatient care, treatment residential care, and secure services (those requiring a court order). Community services are generally provided in health centres rather than hospitals, although in smaller centres, it may be difficult to distinguish the two. Unit costs for each group were obtained from AHS financial services.
Child intervention services were provided through the Alberta Human Services Ministry. We included estimates for residential care only—treatment care and secure services. Estimates of the number of youth in both types of care were based on the Alberta Human Services Child Intervention Data Tool. Costs were based on AHS community mental health and addictions services costs, whose services are similar to those for Alberta Human Services child intervention costs. The total count of youth receiving child services was adjusted by the percentage of these youth who were ages 12 to 17 and who were also designated as being mental health/addictions related according to criteria set in the Policy Wise CYDL data; these percentages were based on cross-ministerial surveillance data from the Policy Wise Child and Youth Data Lab (CYDL) (see below for an explanation). The Child and Family Services (CFS) program provides support for families with mental health disabilities. Data on the number of youth aged 12 to 17 who were enrolled in the program and the program costs for these youth were obtained directly from the program.
Criminal justice services for youth include prosecution, judicial, and corrections (community sentences and custodial sentences). Mental health– and addiction-related services are provided by the AHS Forensic Psychiatry unit. Estimates of the number of Alberta youth who were prosecuted and tried in Alberta were obtained from Statistics Canada’s Crime and Justice data. We separated the 3 components and obtained data for youth and adults for persons charged, court decisions, and youth who received community and custodial sentences. Expenditure data were obtained from the Alberta Justice and Solicitor General Annual Report (2014/2015) for provincial prosecutors, court, and corrections. The ratios of youth to total persons charged and tried were applied to these expenditures to obtain total youth expenditures in criminal justice divisions. We then applied the ratio of youth in the justice system who received mental health and addictions services to total youth in the system, based on cross-program data from the Policy Wise CYDL. Youth diversion services were obtained for Calgary only from Calgary Police Services.
We estimated mental health–related public school services from provincewide data found in annual reports from Alberta Education. We used 2 categories of students who receive special education for mental health–related conditions: severe emotional/behavioural disabilities (code 42 in the Special Education Coding Criteria) and mild/moderate emotional/behavioural disabilities (code 53). As public schools now receive block grants that include allotments for disabilities, we used school funding rates for private schools; these rates are paid individually to the private schools for students. We obtained funding rates for code 42 and code 53 students in private schools and deducted the base funding rates. Based on an earlier study of Alberta schools by Calder et al., 4 we assumed that 80% of this differential rate goes to special education for emotional/behavioural disabilities. These are estimates of payments, not direct measures of resources themselves.
We assume that the number of students in grades 7 to 12 is the same as those aged 12 to 17. The total number of students by grade and by special education code was obtained from Alberta Education Student Enrolment Data. We applied the number in each code group to the total number of youth ages 12 to 17 to estimate the number of youth in Alberta schools receiving special education for students designated by code 42 and 53 categories. We then multiplied these numbers by the code 42 and code 53 private funding rates to estimate excess dollars flowing to youth with emotional/behavioural disabilities.
Hospital, physician, and education mental health services were directly estimated. However, 2 types of service, criminal justice and child services, are complements to mental health and addiction services. The initial cut of data for these services includes all users, whether or not they were provided for youth with mental health and addiction problems. For both of these types of services, we used Policy Wise estimates for the proportion of users of these services who were users of direct mental health care. Based on CYDL data, the average number of youth who used basic mental health services (physician, hospital, Family Support for Children with Disabilities [FSCD]) was 9.2%. 5
Results
According to estimates from Statistics Canada, 6 there were 279,000 youth ages 12 to 17 living in Alberta in 2015. Policy Wise estimated that 9.2% of these (27,169 youth) used hospital, emergency, physician, or child and family support related to mental health services.
Total expenditures for all identified uses were $175.5 million, about $629 for each youth in the population and $6460 for each mental health “attached” youth, according to the Policy Wise criteria. A breakdown of the expenditures by major group of service is shown in Figure 1. Public school grants for special services for youth with emotional problems (both severe and moderate) accounted for 30% of all expenditures, followed by hospital care (inpatient and emergency) at 18%, community outpatient services at 11%, and physician services at 10%. Alternative judicial measures, provided through police departments, were the smallest group, accounting for less than 1% of all identified expenditures.
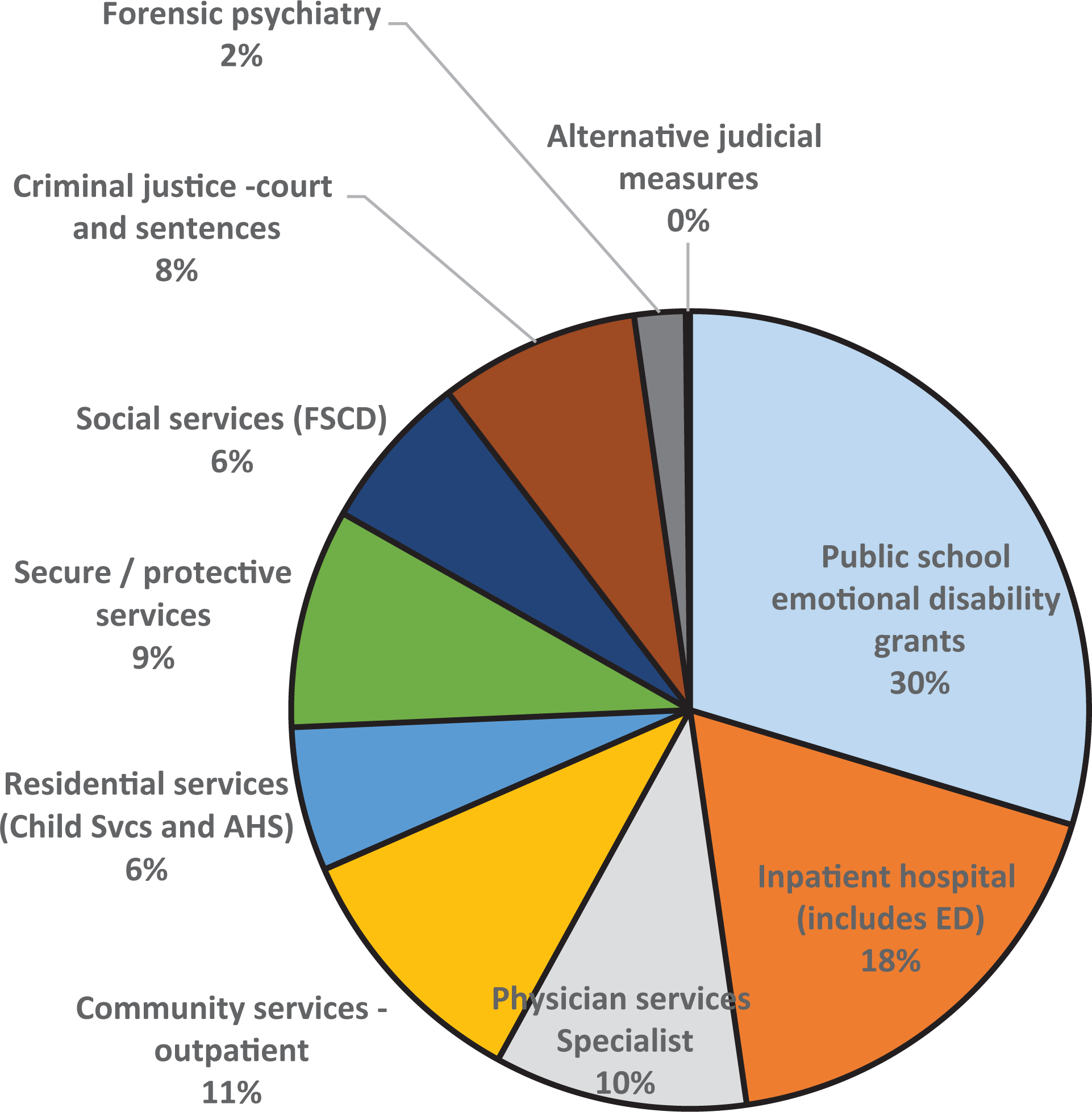
Percentage of mental health costs by category, youth, ages 12 to 17, Alberta.
The number of users by category of services is shown in Table 1. The services used most were community mental health (20,940 separate users) and physician services (20,508 users). The most frequently visited specialists in the physician group were family doctors (11,054 distinct youth seen) and psychiatrists (9,987 distinct youth). Pediatricians were less visited by this older child and adolescent 12 to 17 age group. However, payments to psychiatrists amounted to $15 million of the total of $18 million for the entire physician group, while payments to family doctors were $2.3 million in total.
Youth and Mental Health–Related Costs.
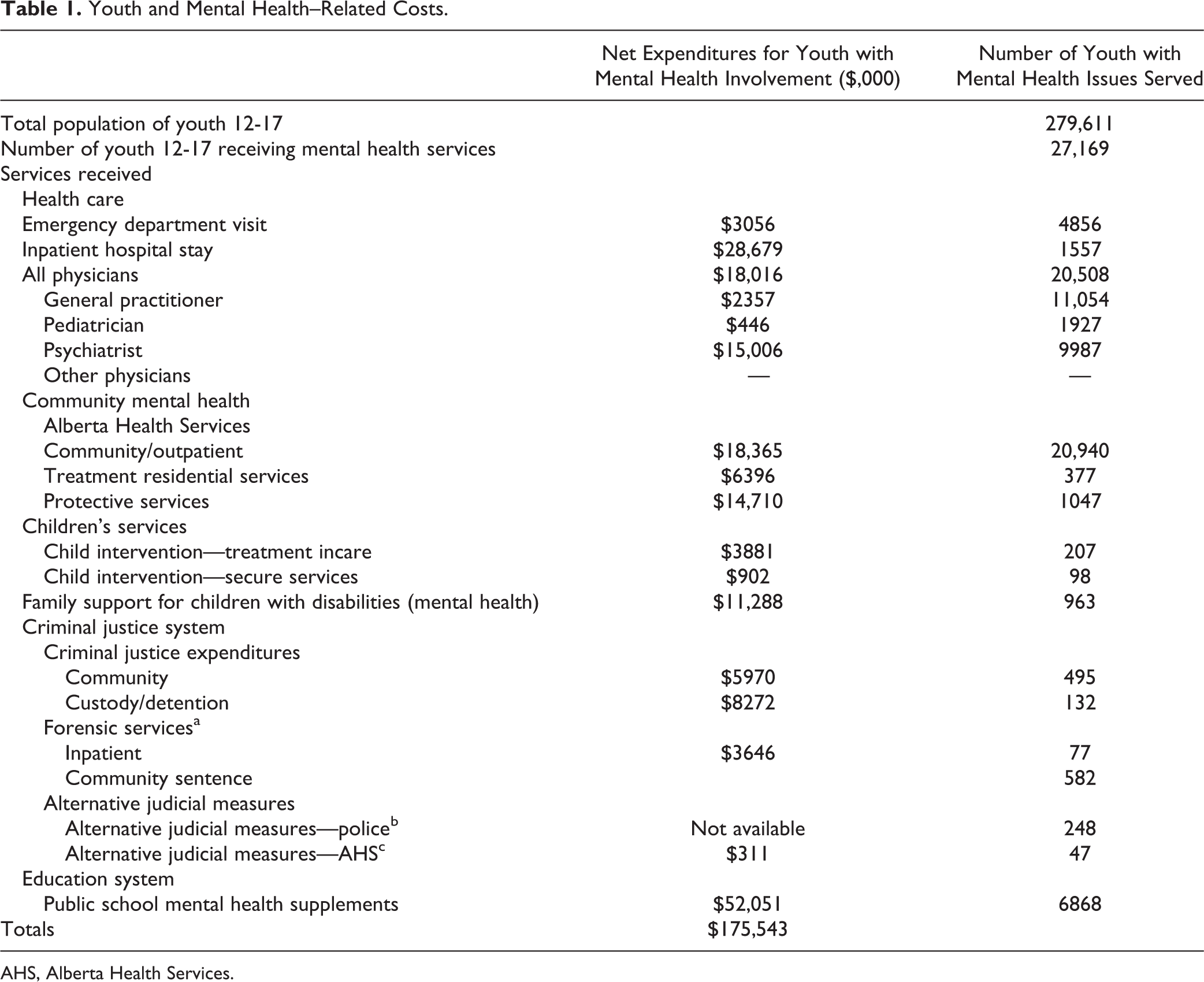
AHS, Alberta Health Services.
The public school system—the service that cost the most—enrolled 6868 youth in special education programs. A total of 4856 youth visited an emergency department for mental health services at least once while 1557 youth were hospitalized for mental health reasons. A total of 627 youth with mental health issues received a criminal sentence, and slightly more than this amount received forensic psychiatry services.
Discussion
We identified services related to mental health that are provided to youth ages 12 to 17 in Alberta for the year 2014/2015. In total, there were 27,169 youth who used at least one of the basic mental health/addiction services designated by Policy Wise, 4 out of an age-specific population of 279,600. The services used by most of the identified population were outpatient mental health services provided or funded by AHS and physician services. The most costly services were public school special education, community outpatient, and physician services. Secure or protective services were also quite costly. The least used of the identified services were preventive alternative judicial measures, which are jointly provided by police, children’s services, and AHS.
We believe that this is the first measure of the provincial mental health expenditures with such a broad scope but focused on this specific group. We have used health, social services, criminal justice, and education data to obtain a wide view of the services used by youth with mental health/addictions problems. The availability of the Policy Wise CYDL data allowed us to adjust for the percentage of youth in certain programs who were receiving mental health and social support and who were also using criminal justice or other social services. However, the CYDL database does not contain costs, and so we have added an economic perspective to this innovative Policy Wise endeavor.
As this study was exploratory, a number of limitations have been identified. First, education, criminal justice, and social services databases that were accessible to us do not contain information on individual patient costs. This is unlike hospital and physician data, where individual data have been developed since the mid-1980s and can be obtained in aggregative forms upon request. In using criminal justice, social service, and education data, we had to average costs over all users, which put a limitation on what we could do with the data (e.g., separately identify high-cost users).
Second, we have omitted some mental health– and addictions-related services that are used by youth. These include some health promotion programs such as family education, outpatient mental health services provided by child services, mental health–related education services provided to students who are not included in codes 42 and 53, private psychologists and therapists paid out of pocket or through private insurance schemes, and mental health and addiction services for Alberta Aboriginal youth that are funded by the federal government. Data for these programs or private insurers were not available. In addition, we left out services provided by some nonprofit agencies. Some of these services are funded by AHS and child services and are included, but others are funded through charitable funds. We did not include these.
Third, we did not include the cost of some services for youth who had mental health or addictions problems but were not in the CYDL database. Some of these youth would have received criminal justice or secure services but did not receive health care services or were not enrolled in the Child and Family Services Program (i.e., the CYDL criteria). We could not tell how many of these there were.
This is the first study of systemwide mental health– and addictions-related costs for a complete jurisdiction that is restricted to a single population group—in our case, youth. There have been population-wide estimates on national and provincial 7 bases. These studies have proven valuable in developing economic benchmarks and comparing the economic performance of different jurisdictions. 8 To address systemwide questions about subgroups, we need to drill down in the databases to understand broad patterns of use for these groups. The amount of resources that are devoted to youth mental health and addictions is an important input in understanding use patterns and formulating provincewide and nationwide policies; this study is a contribution toward that end.
A large number of program and government staff helped us to understand what is a very complex youth mental health and social system. Those who helped us include Wendy Vidlak, Alberta Community and Social Services; Denise Salanski and Ken Morrison, Alberta Health; Laurene Black, Karen Bozocea, Charlene Douglas, Kim Hahn, Aggy King Smith, Christine Mummery, Jaime Paget, Tasha Parmar, Susan Ponting, and Shireen Surood, Alberta Health Services; Jodie Bakker, Alberta Justice and Solicitor General; Jennifer Hansen, Alberta Treasury Branch and Finance; Rebecca Davidson and Tom Lange, Calgary Police; Sean Illerbrun, LaDene Keith, Michelle Rice, and Judy Shine, Children’s Services; John Paul Boyd, Canadian Research Institute for Law and the Family, Calgary; Amanda Starchuk, Wood’s Homes; Marie-Eve Bedard and Yvan Clermont, Statistics Canada; Michelle Anderson-Draper, Anderson Draper Consulting; and Tracy With, Banister Consulting.
Supplemental Material
Supplemental Material, METHODS_APPX - The Public Cost of Mental Health– and Addiction-Related Services for Youth (Ages 12-17) in Alberta
Supplemental Material, METHODS_APPX for The Public Cost of Mental Health– and Addiction-Related Services for Youth (Ages 12-17) in Alberta by Philip Jacobs and Alain Lesage in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
Arvi Ohinmaa helped us with the data analysis. Rebeccah Marsh of CASA Services and Fay Leggat helped us to sort out who the providers in the nonprofit sector were and what they did. Robyn Blackadar, Cathy Scott, Xinjie Cui, and Shannon McInnis of Policy Wise provided helpful suggestions.
Data Access
Health care expenditures data were obtained by request from Alberta Health and Alberta Health Services. The data were obtained in aggregate form and can be obtained by others who make formal requests. We did not have access to patient-level data. Data on social services, criminal justice, and education were obtained from publicly available websites.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no funding for this project. Policy Wise provided a grant to IHE for an economic analysis of the Youth Community Services demonstration Program (YCSP). Many of the insights for this article on the general system came from discussions with persons connected to that project (listed), but the topics are separate. No YCSP data appear in this study. A. Lesage is an invited scholar at IHE and received travel and stay stipends from IHE.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.