
Abstract
Objective
There is increasing interest in early intervention and detection strategies for youth at-risk of developing a serious mental illness (SMI). Little is known about early factors that may be related to the later development of a SMI; thus, the aim of this study was to determine what clinical factors might relate to the development of in this study psychosis, bipolar disorder and severe or recurrent major depression in at-risk youth.
Method
The sample consisted of 162 youth aged 12–26 years at different stages of risk. Thirty-one participants developed a SMI during the study. Those who made a transition were compared on a range of baseline clinical and functional measures with those who did not make the transition. A Cox regression model was used to assess the association between measures and later development of a SMI.
Results
Female sex, attenuated psychotic symptoms as assessed with the Scale of Psychosis-Risk Symptoms (SOPS) and ratings on the K-10 Distress Scale, were found to be significantly associated with the later transition to mental illness. Females were 2.77 times more likely to transition compared to males. For the SOPS and K-10 scales, there is a 14% increase in the transition rate relative to a one-scale increase in SOPS and a 7% increase in the transition rate relative to a one-point increase in the K-10.
Conclusions
Results from these longitudinal data provide further insight into the specific clinical measures that may be pertinent in early detection of mental illnesses.
Introduction
Mental disorders typically begin in adolescence and can cause significant personal and global burden 1 and are the leading cause of disability in adolescents and young adults. 2 Given the possible long-term adverse consequences of mental illness, early identification of those at-risk of developing a mental disorder is warranted with the goal of preventing more serious mental illnesses (SMI). A transdiagnostic clinical staging model has been developed that describes disorders according to multiple stages (stage 0–stage 4), that increase in severity and intensity. 3 For those considered to be at-risk for a mental illness, the relevant stages are stage 0, the pre-symptomatic stage and stage 1 which is divided into two substages: stage 1a those with mild to moderate symptoms but no clear diagnosis and stage 1b those with an attenuated syndrome. The later stages (2–4) are relevant for those with diagnosed disorders. It is beyond the scope of this paper to adequately review in more detail transdiagnostic clinical staging, but readers are referred to more detailed reviews, position papers and consensus statements.4–6
The Clinical High At-Risk Mental State (CHARMS) study in Australia used clinical staging principles to better understand transition to a SMI in individuals at-risk for developing psychosis, severe depression, mania or borderline personality disorder. 7 Their preliminary findings suggest a transition rate of 3% for those in stage 1a and 34% for those in stage 1b. 8 A second Australian study observed a transition rate 12.8% for stage 1b participants who transitioned to a SMI. Of those who transitioned, 24.2% developed a psychotic disorder, 44.3% bipolar disorder (BPD) and 31.4% an anxiety or depressive disorder. 9 Thirdly, the Canadian Psychiatric Risk and Outcome (PROCAN) study was a longitudinal study conducted in Calgary and Toronto of youth at different stages of risk (0–1b) based on the stage model of McGorry and Hickie. 10
The overall aim of PROCAN was to determine factors that might be associated with the later development of psychosis, BPD or serious depression (severe or recurrent). The specific aim of this paper is to examine a range of baseline clinical measures to determine which might be associated with the development of psychosis, BPD or severe or recurrent major depression over a four-year period.
Methods
Participants
A total of 201 individuals at-risk for SMI aged 12–25 years were recruited for the PROCAN study in Toronto and Calgary. Since participants (n = 27) from the Toronto site ended their participation after one year, this paper focuses only on participants from Calgary. Recruitment for PROCAN was through advertisements and referrals by mental health professionals, counselling services, schools and self-referrals to our At-Risk Mental Health Research Clinic.
The sample included youth with early mood symptoms (stage 1a, n = 44) or sub-threshold psychotic symptoms (stage 1b, n = 102), and youth at risk due to a family history of a SMI (stage 0; n = 28). Exclusion criteria included: (i) current or lifetime Axis I BPD, psychotic disorder or severe or recurrent depression (other Axis I disorders are not necessarily exclusionary in stages 1a or 1b as they may be precursors to mood or psychotic disorders); (ii) IQ < 70; and (iii) past or current history of a significant central nervous system disorder or serious medical disorder. None of the participants in stage 0 met any of the criteria for stages 1a and 1b.
The stage 0 group included participants with a first-degree relative with a psychotic disorder, BPD or recurrent mood disorder based on the Family Interview for Genetic Studies (FIGS). Stage 1a participants were clearly distressed, based on published ranges of the Kessler-10 Distress Scale (range 20–24), 11 and had reported that they had concerns about depression or anxiety but did not meet any diagnostic criteria based on the Structured Clinical Interview for DSM-5 (SCID-5). 12 Stage 1b participants met established criteria for being at clinical high risk (CHR) for psychosis as determined by The Structured Interview for Psychosis-Risk Syndromes (SIPS) 13 or had a moderate major depressive episode according to DSM-5 or had subthreshold manic symptoms. Criteria for allocation to the different stages have been published by McGorry and Hickie 14 and are presented in detail in Supplementary Tables 1 and 2.
Twelve participants dropped out after baseline with no follow-up. One hundred and sixty-two had at least one follow-up assessment and are the first sample addressed in the analyses. Of those, 31 made a transition to SMI within the four years of the study. Of the 131 non-transitioning participants with at least one follow-up, only 69 participants completed a final assessment between 42 and 48 months. Thus, our second sample to be analysed includes the 31 transitions and the 69 participants who completed a final assessment at 48 months.
Measures
To determine participant stage at baseline the following measures were used: The FIGS to determine if there was a family member with a SMI, 15 the SIPS to determine CHR criteria, 13 the Quick Inventory of Depressive Symptomatology (QIDS SR-16), 16 and the K10 distress scale. 11 The SCID-5 was used to assess the presence of Axis 1 disorders. 12
Transition to a SMI is defined as meeting DSM-5 criteria for a schizophrenia spectrum disorder, BPD or severe or recurrent major depression.
The following measures were administered at baseline: the Calgary Depression Scale for Schizophrenia (CDSS), 17 Young Mania Rating Scale, 18 the Social Anxiety Scale (SAS), 19 and the Global Functioning: Social (GF:S) scale which was specifically designed for youth at risk 20 and the Global Assessment of Functioning (GAF). The severity of attenuated psychotic symptoms (APS) and negative symptoms were assessed using the Scale of Psychosis-Risk Symptoms (SOPS) which is part of the SIPS. 13 Traumatic experiences before the age of 18 years were assessed using an adapted version of the Childhood Trauma and Abuse Scale. 21 Trauma was scored yes if any of the following were endorsed; psychological abuse, physical abuse, sexual abuse or emotional neglect. Bullying was scored yes if the participant endorsed psychological and/or physical bullying. All measures, except trauma, the FIGS and the GAF were repeated at all follow-ups (6–48 months).
Procedures
Individuals who responded to recruitment efforts were screened by telephone and, if suitable, invited to an in-person assessment to determine eligibility. All clinical raters, under the supervision of Dr. Addington, were required to complete a rigorous protocol for training, standardization of procedures and maintenance of reliability developed for previous multi-site projects (Addington et al., 2012). Dr. Addington supervised weekly meetings during which written comprehensive vignettes were presented for each participant to determine a consensus on that participant's clinical stage. Allocation of participants to the different stages was based on DSM-5, the SIPS, the K-10 and the QIDS. The vignette summarized the interview and data collected and determined the stage. All available data was reviewed in the weekly meetings so that a consensus on the stage could be made. In a later publication, we reported that additional assessments of depression, anxiety, self-evaluation and level of functioning completed at baseline validated the placement into these different stages. 22
Informed consent was obtained from all participants, and parental informed consent was obtained for those under the age of 18. The University of Calgary Conjoint Health Research Ethics Board provided ethical approval of the study.
Participants were assessed at baseline on all measures, followed by short clinical assessments at 6, 12, 18 and 24 months. Subsequently, additional funding was acquired to follow the Calgary sample for two more years to complete short clinical assessments, at 30, 36, 42 and 48 months after baseline. All assessments up to 24 months were conducted in person by August 2019. The majority of the 30–48-month assessments were conducted virtually during COVID. If there was a suspected transition to a SMI, the consensus decision-making process was used to confirm the transition by reviewing all available data. More details on recruitment and methodology have been reported elsewhere.10,22
Statistical Analyses
Statistical analyses were performed with SPSS 28 and STATA 17. T-tests were performed for continuous socio-demographic variables and chi-squared test for categorical variables, to compare transition and non-transition groups Cox regression analysis was to examine which factors impact transition to SMI. Univariable Cox proportional hazard regression analyses were performed to decide which predictors to include in the Cox model. Predictors were considered for the model if P < 0.25 in the univariable analyses. Backward variable selection was performed for the final Cox regression model. Interactions between predictors were also assessed. The interactions with P < 0.05 were included in the model. The models with and without the interactions were compared to see which model better fit the data. Lastly, the Schoenfeld and scaled Schoenfeld residuals were used to test the proportionality assumption. All analyses will be completed with both Sample 1 and Sample 2.
Results
Demographics
There were 162 participants, with 131 participants in the non-transition group (62 males, 69 females, mean age 17) and 31 participants in the transition group (5 males, 26 females, mean age 17.18). The majority were white, single, lived at home, enrolled as students and not employed. For both samples, there were significantly more females than males in the transition group (Table 1).
Demographics of Transition and Non-Transition Groups.
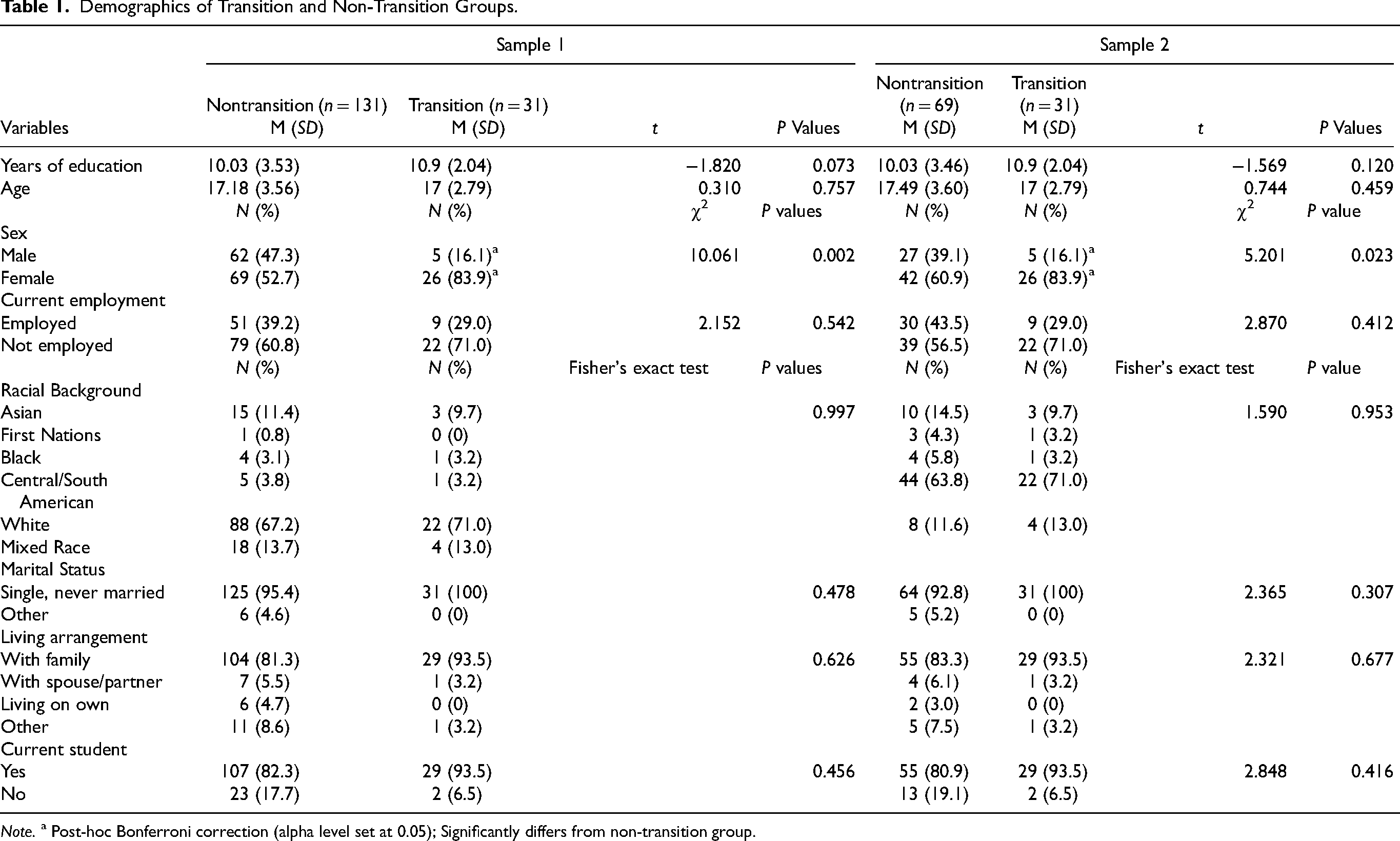
Note. a Post-hoc Bonferroni correction (alpha level set at 0.05); Significantly differs from non-transition group.
Transitions to SMI
Of the 31 participants who transitioned to a SMI, 27 transitioned to major depressive disorder (MDD), three to BPD and one to psychosis. Details of transition diagnoses are presented in Table 2. The mean number of days from baseline to time of transition was 767 (SD = 435, range = 133–1460) days. Ten participants transitioned in year 1, five in year 2, eight in year 3 and eight in year 4.
Details of Transition.
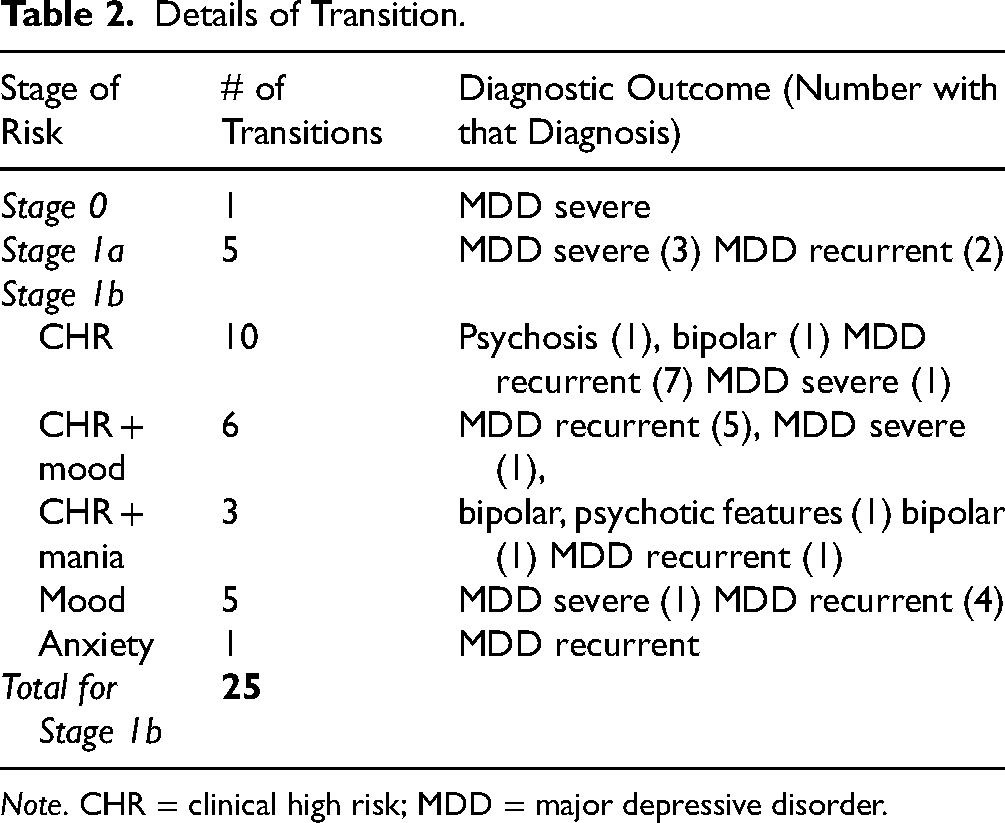
Note. CHR = clinical high risk; MDD = major depressive disorder.
Comparison of Baseline Measures
Participants who dropped out after baseline did not differ from those who continued, the one exception being dropouts having significantly lower ratings on the GAF. For those who dropped out after at least one follow-up, there were no differences between those groups and those who remained for 42–48 months (see Supplementary Tables 3 and 4).
Differences between the transition and the non-transition groups are presented in Table 3. For both samples, the transition and non-transition groups differed significantly on all variables apart from negative symptoms, social functioning, family history and past bullying and trauma.
Clinical Differences Between Those Who Transitioned and Those Who Did Not.
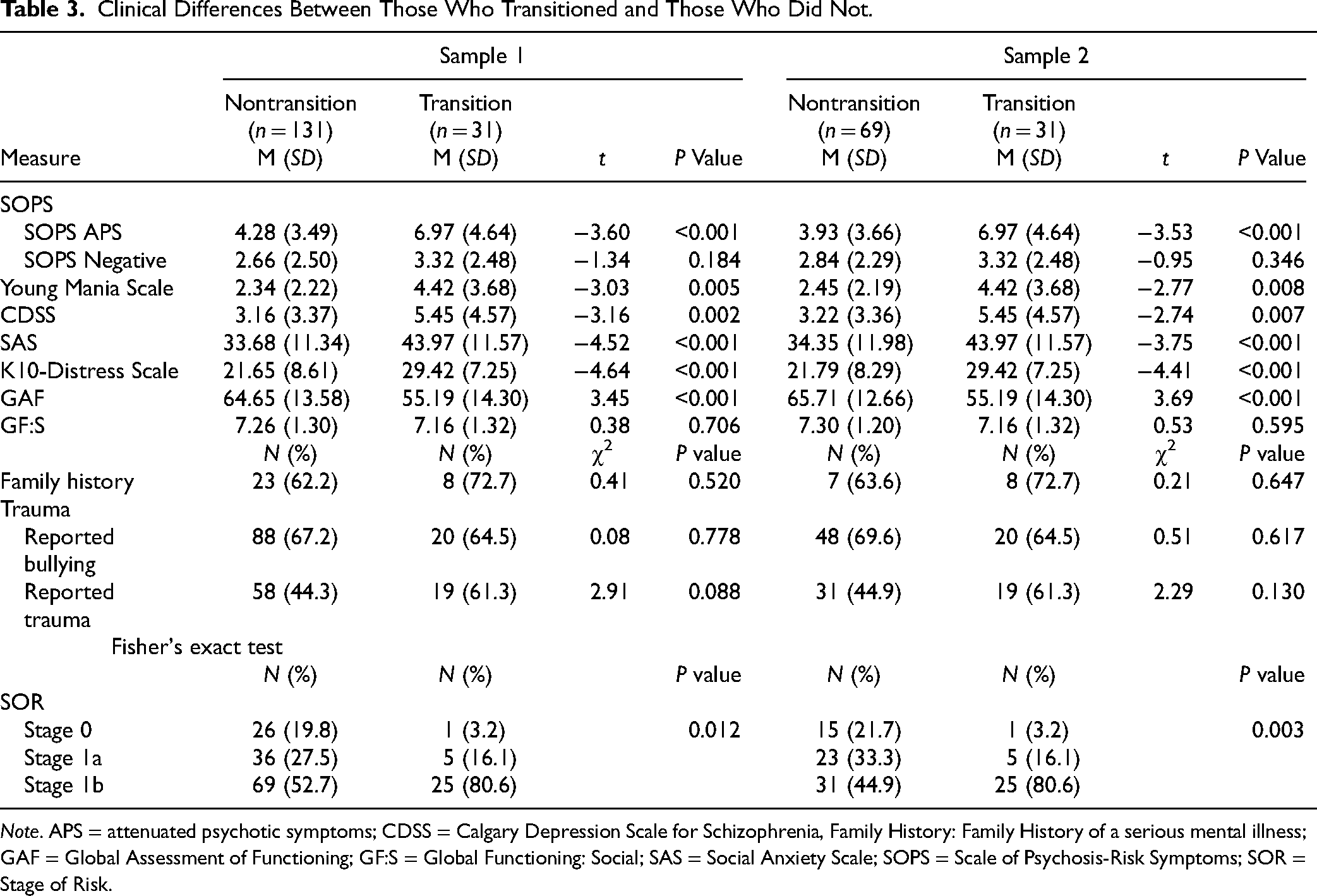
Note. APS = attenuated psychotic symptoms; CDSS = Calgary Depression Scale for Schizophrenia, Family History: Family History of a serious mental illness; GAF = Global Assessment of Functioning; GF:S = Global Functioning: Social; SAS = Social Anxiety Scale; SOPS = Scale of Psychosis-Risk Symptoms; SOR = Stage of Risk.
Model Building
Cox regression analysis was performed on the clinical measures first from the 162 participants in Sample 1 and then for the 100 participants in Sample 2 to test the association between time to transition and predictor variables. The hazard is the development of a SMI, and the hazard ratio reflects the likelihood of developing a SMI at any point in time. Univariable Cox proportional hazard regressions were performed on all variables in Sample 1 and Sample 2 before proceeding to model building (see Supplementary Tables 5 and 6). The Kaplan–Meier survival estimate of the probability of non-transition is presented in Figure 1. In a backward selection fashion, the least significant variables were removed from the full model until the final model was obtained, χ2 (3, N = 162) = 32.13, P < 0.0001. The final model included APS, the K10-Distress Scale and sex. Similarly, the final model for Sample 2 was obtained, χ2 (2, N = 99) = 23.71, P = 0.0000. This model included APS and K10 Distress Scale with sex approaching significance (see Table 4).
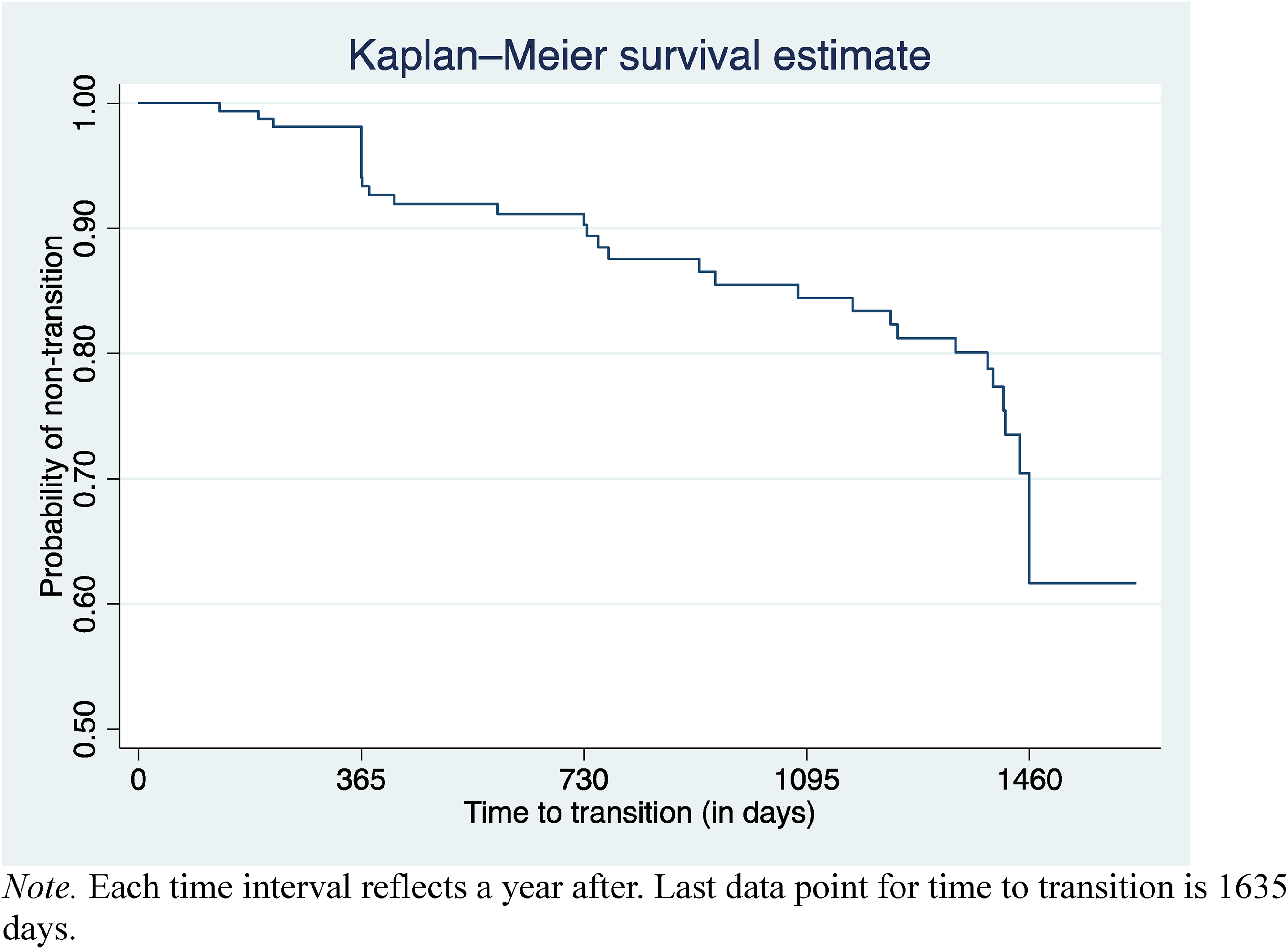
Kaplan–Meier survival estimate of the probability of non-transition.
Cox Proportional Hazards Estimates of the Determinants of SMI by Baseline Measures.
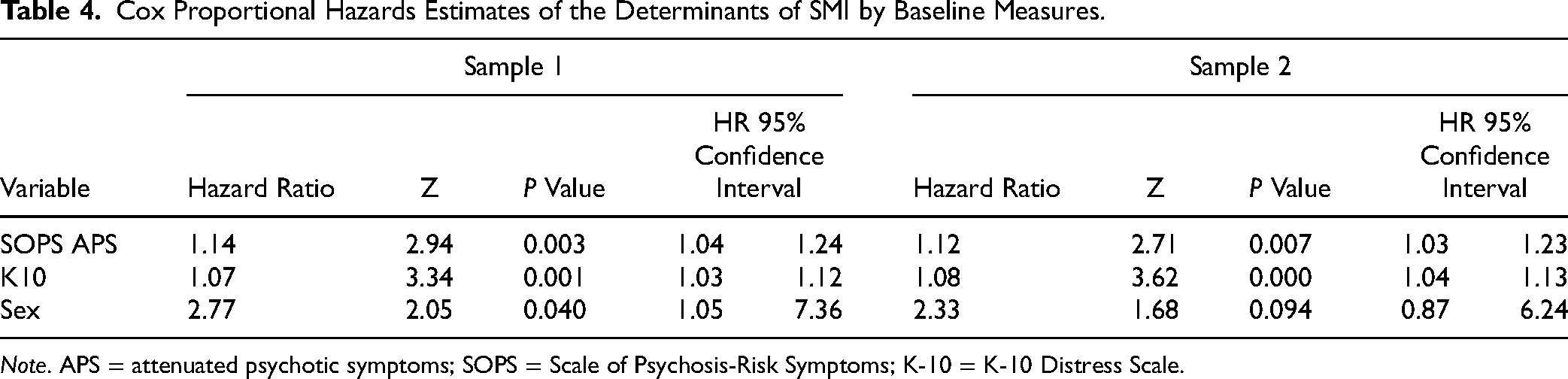
Note. APS = attenuated psychotic symptoms; SOPS = Scale of Psychosis-Risk Symptoms; K-10 = K-10 Distress Scale.
SOPS APS. In Sample 1, there were significant differences between the mean scores of the non-transition group (M = 4.28, SD = 3.49) and the transition group (M = 6.97, SD = 4.64). In the model, more severe APS rating reflected an increased risk of SMI (HR = 1.14, Z = 2.94, P = 0.003, 95% CI [1.04–1.24]). In Sample 2, there were significant differences between the mean scores of the non-transition group (M = 3.93, SD = 3.66) and the transition group (M = 6.97, SD = 4.64). Again, the model suggested an increased risk with more severe APS ratings (HR = 1.13, 95% CI [1.03–1.23]).
K10-Distress Scale. In Sample 1 the transition group had significantly more severe distress scores (M = 29.42, SD = 7.25), compared to the non-transition group (M = 21.65, SD = 8.61). The model indicated an increased risk of developing SMI with higher K10 ratings (HR = 1.07, Z = 3.34, P = 0.001, 95% CI [1.03–1.12]). In Sample 2, the transition group had significantly more severe scores on the K10 (M = 29.42, SD = 7.25), compared to the non-transition group (M = 21.79, SD = 8.29). The model once again indicated an increased risk of developing SMI with more severe K10 ratings (HR = 1.08, 95% CI [1.04–1.13]).
Sex. For Sample 1, there were 62 males (47.3%) and 69 females (52.7%) in the non-transition group, and 5 males (16.1%) and 26 females (83.9%) in the transition group. The model indicated that females had a greater risk of developing a SMI compared to males (HR = 2.77, Z = 2.05, P = 0.04, 95% CI [1.05–7.36]). In Sample 2, there were 27 males (39.1%) and 42 females (60.9%). The model was not significant although it did approach significance perhaps due to the small sample size (HR = 2.33, Z = 1.68, P = 0.09, 95% CI [0.87–6.24]).
All possible interactions between variables were considered and none were significant. Therefore, no interaction terms are included in the final model. Proportionality assumption was tested using the Schoenfeld and scaled Schoenfeld residuals. The overall test and individual variables were non-significant, suggesting no violation of the proportionality assumption.
Discussion
In this paper, sex, age, depression, APS, negative symptoms, anxiety, mania, social functioning, trauma and family history were examined as possible factors that might be associated with the later development of a SMI in youth. At baseline, it was observed that the transition group had more severe ratings on APS, the Young Mania Scale, the CDSS, the SAS and the K10-Distress Scale and had poorer ratings on the GF scale. Those that transitioned to SMI tended to be female, and at an increased stage of risk (1b). The increased likelihood of developing a SMI with increasing stage of risk is to be expected and has been demonstrated elsewhere. 9
For transitions, 31 made a transition to a SMI. Thus a 17.8% transition rate overall, with 3.5% of stage 0, 11% of stage 1a and 24.5% of stage 1b transitioning. These rates are slightly higher than the 12.8% for stage 1b and 2.6% for stage 1a reported in a previous study. 9 Although both this and the Iorfino study attempted to follow participants for up to 42 months, 45% of the transitions in the Iorfino study occurred within the first year whereas in PROCAN only 35% occurred in the first year. 22
In the final model of potential predictors of developing a SMI, more severe ratings on and K-10 distress scales plus being female were most significant. A one-point increase in the score on the SOPS APS was associated with a 14% increase in risk of developing a SMI. The significance of APS is interesting since the majority of participants transitioned to a depressive disorder, and not psychosis yet 61% of stage 1b participants who did transition initially met 1b criteria for being at CHR for psychosis. This supports the idea from the International Consensus Statement that: “Transdiagnostic clinical staging in youth mental health….acknowledges the fluid, heterotypic nature of the evolution of emerging mental disorders, and the pluripotentiality of later outcomes for those who present at earlier stages.”(p237). 4 Heterotypic shifts would include the onset of psychosis in someone who had previously been diagnosed with depression alternatively there exists homotypic progression which is the case when an individual, for example, develops severe or recurrent major depression following a mild episode.23,24
Furthermore, it is well established that approximately 50% of CHR participants have a high rate of comorbid depression at baseline 25 and for some CHR youth more serious depression or recurrent depression can develop over the course of two years following baseline. 26 Secondly, in CHR studies typically less than 20% go on to develop a psychotic illness and some CHR individuals, although presenting with APS, are more at risk of developing a mood versus a psychotic disorder. Thirdly, it has been suggested that prior to developing a SMI such as BPD or a schizophrenia spectrum disorder an individual may first develop an MDD, 27 establishing APS as indicative of a more SMI. Finally, similar to our findings, the Iorfino study found that psychotic-like experiences were a risk factor for the development of a SMI and not just a psychotic disorder. 9
The K-10 Distress scale was a significant variable in the model suggesting that each one-point increase in K-10 scores is associated with a 7% increased risk of developing a SMI. The K-10 was used in a large Australian epidemiological study of over 10,000 respondents. For those who scored in the same range as our non-transitioning group, approximately 10% developed an affective disorder whereas of those who scored in the same range as our transition group approximately 28% developed a mood disorder. 28
Finally, being female was associated with almost three times greater risk of developing a SMI. Although sex was not significant in the second model, it is likely that the smaller sample size affected the power. Several studies have shown that females have a higher prevalence of depressive disorders compared to males29,30 and that this sex difference emerges during adolescence and persists through early adulthood. 31 Since the transition from adolescence to early adulthood is a stressful period that predisposes some to developing mood and anxiety disorders, it has been suggested that females experience more interpersonal stressors which mediates the increased prevalence of depression in adolescence.32,33 Additionally, sex differences in severity of depressive symptoms have been attributed to females having a higher ruminative response style that could lead to greater reporting of depressive symptoms among females. 34 Increased mental health literacy observed in young women may lead to more accurate recognition of depressive symptoms. 35 Finally, neurobiological underpinnings, such as puberty-related changes in the estrogen levels and associated changes in the HPA axis, have been suggested. 36
One of the strengths of this study is the use of a clinical staging model which allowed consideration of the different stages of risk relative to transition. Secondly, to the best of our knowledge, there are only two other longitudinal youth studies7,9 examining transition to a SMI, both from Australia. In this Canadian study, a significant number of at-risk youth were assessed every six months with many participants being followed up to 48 months.
However, there are several limitations. First, for a study that is examining transition to a SMI the sample is small. Although higher rates of transition to a SMI would be expected compared to transition rates to a psychotic illness, key CHR studies have samples in excess of 600 participants. Secondly, although we report on follow-up to 48 months, this was not planned in the initial proposal, and additional follow-ups were added as more funding became available. Thus, not only were there dropouts over the course of four years but also a number of participants who had completed the original study and could not be found for these later follow-ups. Longer term follow-ups need to be included as part of the initial design. It is, therefore, unclear how many of the 131 non-transitioning participants might have made a transition. Although in Sample 2 that consisted of those who did not transition by the 48-month assessment, we found similar associations between variables and risk of SMI. Fourthly, both the Iorfino and CHARMS studies recruited participants already engaged in youth mental health with the Iorfino study data coming directly from clinical files. In contrast, only a small proportion of our sample came directly from clinical services, the majority being recruited by advertising and talks to community clinics and to the public which might have resulted in a diluted risk group in that participants with more concerning symptoms may already be in care and less likely to be referred to research. Fifthly, although transition to a severe MDD was the most common diagnosis even in CHR participants, it is possible that some of these transitions may still go on to develop a psychotic disorder. Unfortunately, once a participant made a transition to an SMI, as per our protocol, their study participation ended. This does not mean that an individual cannot develop a second SMI. Thus, we are unable to comment on the complex trajectories of SMI from a risk stage. Finally, this paper is limited in that it only reports on those who developed SMI and lacks equally important information on predictors of recovery.
Currently, there is growth and progression in efforts to improve outcomes in youth mental health. For example, there is an international organization with biennial meetings, the International Association for Youth Mental Health; an International Consensus Statement has been published 4 and, led by the Australian network of Headspace Programs Statement, 37 new service structures that aim to address mental health difficulties for youth including at-risk or early stage pluripotential syndromes are gradually developing.5,38 Considering the challenges that exist in developing programs for youth who are at-risk for SMI, a recent publication 4 outlines directions and implications for what is called “next-generation early intervention infrastructures”. However, supporting data for these endeavours is scarce. Results of the PROCAN study begin to add to this need. However, there is need for much larger-scale longitudinal studies first, to validate and expand on these results, and secondly to monitor different illness and remission trajectories.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437231195959 - Supplemental material for Factors Associated with Transition to Serious Mental Illness
Supplemental material, sj-docx-1-cpa-10.1177_07067437231195959 for Factors Associated with Transition to Serious Mental Illness by Sara Jalali, Lu Liu, JianLi Wang and Sidney H. Kennedy, Glenda MacQueen, Catherine Lebel, Benjamin l. Goldstein, Signe Bray, Jean Addington in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank Amy Braun BA for her help with the final version of this paper.
Data Access
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research: This trial was funded by a Brain Canada Grant with matching funding from the Hotchkiss Brain Institute, University of Calgary to J. Addington. The 3- and 4-year follow-up was funded by a grant from the Calgary Health Trust to J. Addington. Calgary Health Trust, Hotchkiss Brain Institute, University of Calgary, Fondation Brain Canada.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.