
Abstract
Objectives:
We investigated the prevalence of substance use disorders (SUDs) among emerging adults and quantified the extent to which emerging adults, compared with young adults, have increased odds for SUDs.
Methods:
Data were from the 2012 Canadian Community Health Survey–Mental Health (CCHS-MH). Respondents were 15 to 39 y of age (n = 9228) and were categorized as: early emerging adults (15 to 22 y); late emerging adults (23 to 29 y); and, young adults (30 to 39 y). SUDs [alcohol or drug abuse/dependence (AAD or DAD)] were measured using the WHO Composite International Diagnostic Interview 3.0. The prevalence of SUDs was compared across age groups, and odds ratios (OR) and 95% confidence intervals (CI) were computed from logistic regression models adjusting for sociodemographic and health covariates. Analyses were weighted to maintain representativeness to the Canadian population.
Results:
The prevalence of AAD was 8.0%, 6.6%, and 2.7% for early emerging adults, late emerging adults, and young adults, respectively. For DAD, the prevalence was 6.4%, 3.6%, and 1.3%. After covariate adjustment, early and late emerging adults had greater odds of reporting AAD (OR = 3.2, 95% CI = 2.2 to 4.9 and OR = 2.4, 95% CI = 1.6 to 3.4, respectively) or DAD (OR = 4.2, 95% CI = 2.5 to 7.0 and OR = 2.5, 95% CI = 1.6 to 4.1, respectively) compared with young adults. Differences between early and late emerging adults were not significant.
Conclusion:
Emerging adults are at increased odds for SUDs. Lack of differences between early and late emerging adults provide evidence of the extension of emerging adulthood into the late 20s. Findings have implications for the provision of screening and treatment of SUDs during this developmental period.
Introduction
Due to demographic shifts, such as delayed marriage, parenthood, and long-term employment positions, a novel and distinct period of development referred to as “emerging adulthood” has been identified for today’s young people in industrialized societies. Although emerging adulthood has typically referred to the developmental period between 15 and 25 y of age, researchers have suggested that emerging adulthood can persist into the late 20s. 1,2 In some cases, this developmental period, characterized by features that distinguish it from both adolescence and adulthood (i.e., identity exploration, instability, a focus on self, a feeling of in-betweenness, and optimism), 3 is divided into 2 categories: 1) early emerging adulthood and 2) late emerging adulthood. However, the age demarcations associated with these categories are not clearly defined in the literature and have been scantily investigated. 4
Substance use during emerging adulthood is a major public health problem. 2,5 Compared with all other age groups, emerging adults (18 to 25 y) have the highest past-year (76%) and past-month (58%) prevalence of alcohol consumption. Past-year (38%) and past-month (22%) illicit drug use is also the highest among emerging adults. 6 Similar trends have been observed in other epidemiological studies in North America. 7,8
Accompanying the high rates of substance use in emerging adults are the peaks in the prevalence of substance use disorders (SUDs). Based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) 5, recent estimates found that the prevalence of past-year and lifetime alcohol use disorder were 27% and 37% among emerging adults (18 to 29 y), percentages higher than all other age groups. Likewise, the prevalence of past-year (8%) and lifetime (14%) drug use disorder were the highest among emerging adults. 9,10 Although recent Canadian studies assessing SUDs among emerging adults are not readily available, one cross-sectional study reported that emerging adults (15 to 24 years old) had the highest prevalence (12%) of any past-year SUD as compared with all other age groups during the year 2013. 11 However, this study did not include the full spectrum of emerging adulthood and did not report estimates for alcohol abuse/dependence (AAD) and drug abuse/dependence (DAD) separately.
Knowledge gaps remain within the literature, despite our understanding of the negative life trajectories, altered brain development, potential lifelong substance abuse and dependence, and losses to productivity among emerging adults, 12 and despite the significant emphasis placed on addressing alcohol and drug problems in young people by the World Health Organization (WHO). 13,14 First, as highlighted above, there have been remarkably few recent Canadian studies on the prevalence of SUDs among emerging adults; contemporary prevalence estimates are needed to highlight economic and social burdens, generate policies aimed at the prevention and treatment of SUDs, and inform the effective provision of health services. 9,10 Second, most estimates of SUDs have failed to include the full spectrum of emerging adulthood, thus limiting the generalizability across this developmental period. 15 Third, significant variability in psychiatric outcomes among early emerging adults, late emerging adults, and young adults has been identified. 16 However, no study has examined subgroup differences among these age groups for SUDs.
In the context of these knowledge gaps, this study used contemporary national epidemiological data to: 1) Estimate the overall, age-, and sex-specific past-year prevalence of SUDs for early emerging adults, late emerging adults, and young adults; 2) Quantify the extent to which early and late emerging adults, compared to young adults, are at increased odds for SUDs; and 3) Examine the potential moderating effects of sex, presence of a mental disorder, and number of chronic physical conditions on the association between age and SUDs.
Methods
Data and Sample
Data were from the 2012 Canadian Community Health Survey-Mental Health (CCHS-MH). The CCHS-MH employed a multi-stage, stratified, cluster sampling design to generate a representative sample of Canadians (≥15 y of age) residing in the Canadian provinces. First, clusters or geographical areas within the 10 provinces were selected. Second, households within the sampled clusters were selected. Third, one respondent per selected household was randomly selected. For the CCHS-MH, the household-level response rate was 79.8%, the person-level response rate was 86.3%, and the combined (household and person) response rate was 68.9%. Canadians residing in the territories, persons living on Aboriginal settlements, full-time members of the Canadian Forces, and the institutionalized population were excluded. Overall, the excluded population comprised 3% of the target population. 17
Data were collected by decentralized field interviewers from January 2, 2012 to December 31, 2012 using in-person computer-assisted personal interviewing. For this study, the sample was restricted to participants aged 15 to 39 y (n = 9,228). Respondents were advised that participation in the CCHS-MH was voluntary and that privacy was guaranteed by Statistics Canada. All analyses were approved by Hamilton Integrated Research Ethics Board (HiREB).
Measures
SUDs
Past-year AAD and DAD, derived by Statistics Canada, were the primary outcomes for this analysis. The assessment of these disorders was based on the WHO version of the Composite International Diagnostic Interview 3.0 (WHO-CIDI) adapted for the CCHS-MH. The WHO-CIDI is a standardized, valid, and reliable instrument that is widely used in population surveys for the assessment of SUDs. 11,18 –20 The WHO-CIDI 3.0 consists of a comprehensive, fully-structured, diagnostic interview and employs computerized algorithms to provide lifetime and 12-mo diagnoses for mental and SUDs based on DSM-IV and the International Classification of Diseases 10 (ICD-10). 18
AAD
This measure identified individuals who met the WHO-CIDI criteria for AAD within the 12-mo before the interview. According to the CCHS-MH, alcohol abuse was defined as experiencing at least 1 of the 4 abuse symptoms (i.e., failure in fulfilling obligations, alcohol use in physically hazardous situations, recurrent alcohol-related problems, continued use despite problems caused or exacerbated by alcohol). Alcohol dependence was defined as having at least 3 of the 7 grouped dependence symptoms (i.e., tolerance, withdrawal, increased consumption, attempts to quit, time lost, reduced activities, continued consumption) and reporting a maladaptive pattern of alcohol use. The criteria to assess past-year AAD employed in this study has previously been used in various studies. 21 –25
DAD
This measure identified individuals who met the WHO-CIDI criteria for DAD within the 12-mo before the interview. Similar to that for alcohol abuse, drug abuse was defined in the CCHS-MH as experiencing at least 1 of the 4 abuse symptoms (e.g., recurrent drug-related problems) and drug dependence was defined as having at least 3 of the 7 grouped dependence symptoms (e.g., tolerance) and reporting a maladaptive pattern of drug use. Cannabis abuse and dependence were assessed independently from other drugs (e.g., sedatives, tranquilizers, nonmedical stimulants, nonmedical analgesics). However, due to sparse data, drug-specific analyses could not be conducted (i.e., cannabis and other drugs were aggregated into a single variable). The DAD criteria have been used previously. 25 –27
Mental Disorders
Past-year mental disorders, derived from the CCHS-MH, included in the analysis were major depressive episode and generalized anxiety disorder. The presence of past-year mental disorders was measured using the WHO-CIDI.
Chronic Health Conditions
Chronic physical conditions were measured using a standard checklist, which asked participants if they had been diagnosed by a health professional with a long-term health condition (e.g., asthma, diabetes, epilepsy, heart disease) that had lasted or was expected to last for 6 mo or longer. Such checklists have been shown to yield complete and accurate reports 28,29 and have moderate to good concordance with administrative medical records. 28 –30 The number of chronic physical conditions endorsed was summed, and participants were categorized as having none, 1, 2, or 3 or more conditions. This categorization captured the escalating public health and medical problem associated with multiple, chronic health conditions, and has been used previously to estimates rates of chronic health conditions in large epidemiological studies. 31 –33
Pain
Pain was assessed using responses from the following 2 items that captured the presence and intensity of pain: 1) Are you usually free of pain or discomfort? and 2) How would you describe the usual intensity of your pain or discomfort? Participants who responded “yes” to the first question were coded as having no pain. Participants who responded “no” were then classified according to the intensity of their pain or discomfort into 3 separate categories: mild, moderate, or severe. Due to the small number of participants endorsing moderate or severe pain, these 2 categories were aggregated in the analyses. The assessment of pain in the CCHS-MH has been used successfully in other studies. 34 –36
Sociodemographic Covariates
Sociodemographic covariates were included in the analyses to provide unbiased estimates of the association between age and SUDs. These were: participant sex, education, household income (in increments of $10,000), employment (not employed, employed part-time, or employed full-time), and immigrant status (born or not born in Canada).
Analysis
Emerging adulthood was divided into 2 categories: 1) Early emerging adulthood and 2) late emerging adulthood. Although the age demarcations for early and late emerging adulthood are not clearly defined, we defined early emerging adulthood as encompassing individuals between the ages of 15 and 22 y to ensure adequate group sizes and capture those who are likely to be attending secondary or post-secondary educational institutions (n = 3,160). Late emerging adulthood consisted of individuals aged 23 to 29 y (n = 2,470), those who had completed post-secondary education and were either continuing their education or entering the workforce. SUDs within these 2 age groups were then compared to SUDs among those aged 30 to 39 y (young adults; n = 3,598).
The overall, age-, and sex-specific prevalence of SUDs in the 12-mo before the interview were estimated. The overall prevalence of SUDs was then compared across age groups and sex using the Rao-Scott χ2 and subsequently converted into an F statistic. 37 Hierarchical logistic regression models were built to quantify the association between age and SUDs. Product-term interactions between age and participant sex, the presence of a mental disorder, or the number of chronic physical conditions were included in the models to examine potential moderating effects. Because of the complex design of the CCHS-MH, sample weights were applied to ensure representativeness of the sample, and bootstrap methods were used to calculate variance estimates. Data were missing for 269 (2.9%) participants. Because this was minimal (≤5%) and none of the study variables predicted missingness, listwise deletion was used to handle missing data. 38,39 All analyses were conducted using STATA 13.
Results
Sample Characteristics
The mean age was 27.0 (SD, 7.7) y and 50.7% of the population was male. Nearly half (52.9%) were employed full-time, 82.2% had at least completed secondary school, 84.5% had household incomes above or equal to $30,000 (Canadian low-income cut-off), 22.9% were immigrants, and 88.0% were usually free from pain and discomfort. A small percentage of the population met the criteria for past-year major depressive episode (6.2%) or generalized anxiety disorder (2.7%). Over half had no chronic physical condition, 23.2% had one condition, 10.7% had 2, and 9.0% had 3 or more. As compared to young adults, the group of emerging adults included significantly more males and, as expected, fewer immigrants and lower educational attainment. Similarly, and not surprisingly, early emerging adults were significantly less likely to be employed or to be experiencing pain as compared to late emerging adults or young adults. There were no differences in household income among the early emerging, late emerging, and young adults. Pairwise contrasts by age groups are shown in Table 1.
Weighted sample characteristics by age groups.
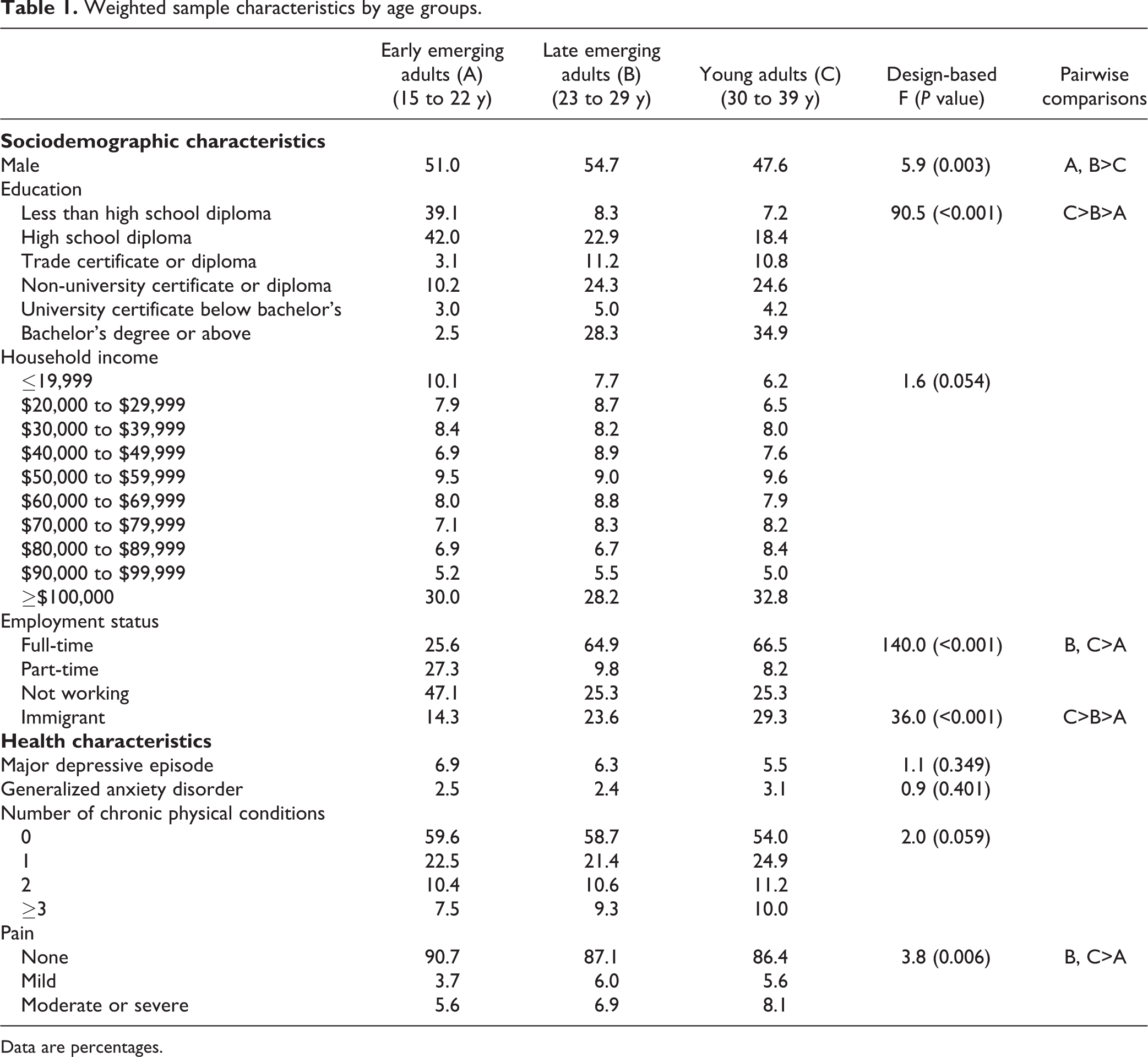
Data are percentages.
Past-year Prevalence of SUDs
The prevalence of AAD was 5.5% and DAD was 3.6%. Specifically, the prevalence of AAD was 8.0% for early emerging adults, 6.6% for late emerging adults, and 2.7% for young adults (F = 23.0; P < 0.001). For DAD, the prevalence was 6.4% for early emerging adults, 3.6% for late emerging adults, and 1.3% for young adults (F = 30.5; P < 0.0001). The prevalence of both SUDs was significantly higher among males compared with females across all age groups (Table 2).
Weighted age- and sex-specific prevalence of alcohol and drug abuse or dependence.
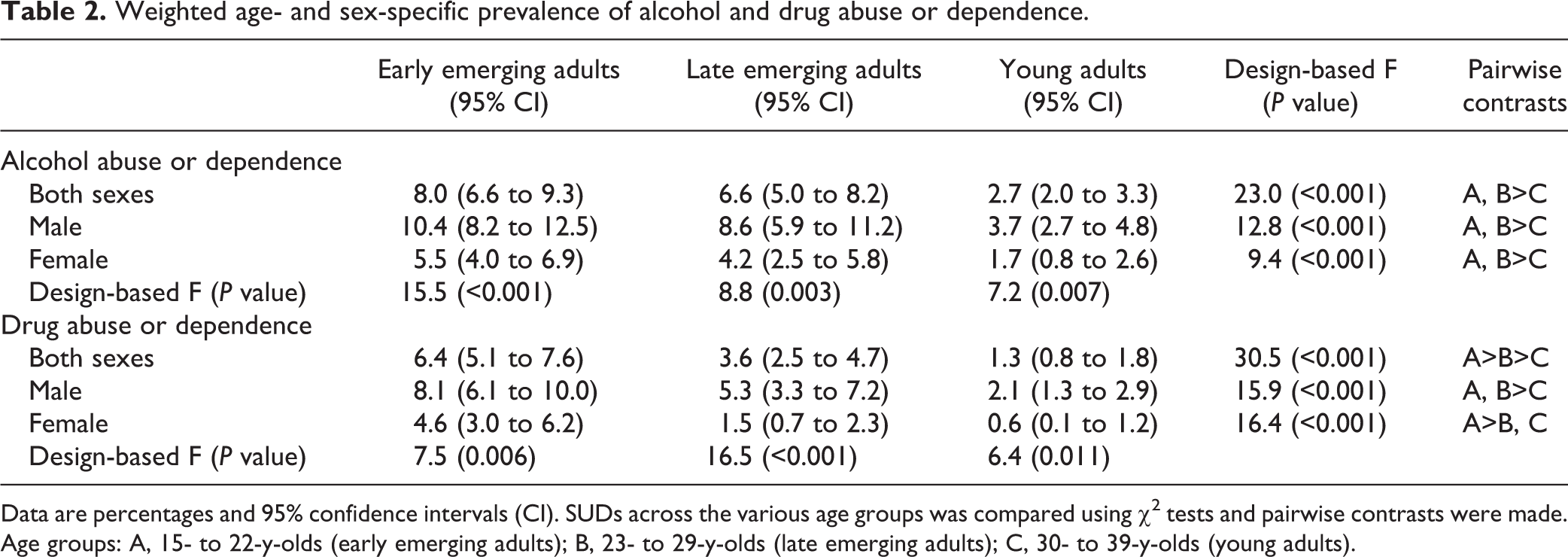
Data are percentages and 95% confidence intervals (CI). SUDs across the various age groups was compared using χ2 tests and pairwise contrasts were made. Age groups: A, 15- to 22-y-olds (early emerging adults); B, 23- to 29-y-olds (late emerging adults); C, 30- to 39-y-olds (young adults).
Association of SUDs and Age
Compared with young adults, early (OR, 3.2; 95% CI = 2.2 to 4.9) and late (OR = 2.4; 95% CI = 1.6 to 3.4) emerging adults had greater odds for AAD. Males (OR = 2.3; 95% CI = 1.7 to 2.9), those with major depressive episode (OR = 2.2; 95% CI = 1.4 to 3.5), or those with generalized anxiety disorder (OR = 2.5; 95% CI = 1.3 to 4.8) were more likely to report AAD, whereas participants not employed full-time (OR = 0.8; 95% CI = 0.6 to 0.9) and immigrants (OR = 0.4; 95% CI = 0.2 to 0.7) were less likely to report AAD (Table 3).
Weighted logistic regression models for alcohol abuse or dependence.
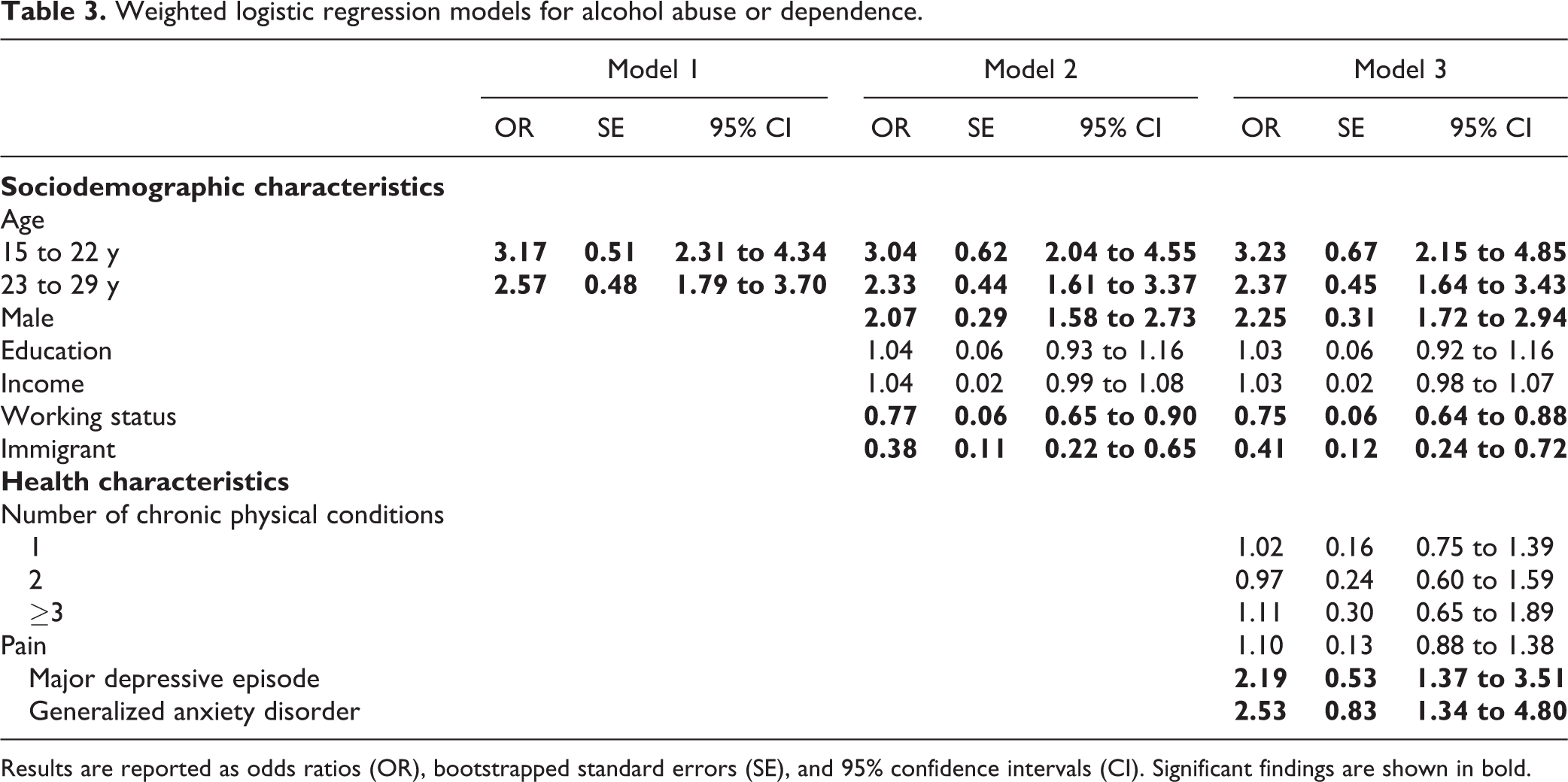
Results are reported as odds ratios (OR), bootstrapped standard errors (SE), and 95% confidence intervals (CI). Significant findings are shown in bold.
Early (OR = 4.2; 95% CI = 2.5 to 7.0) and late (OR = 2.5; 95% CI = 1.6 to 4.1) emerging adults were more likely to report DAD compared to young adults. Males (OR = 2.9; 95% CI = 2.0 to 4.2), those with lower educational levels (OR = 1.2; 95% CI = 1.1 to 1.4), with 3 or more chronic physical conditions (OR = 1.9; 95% CI = 1.1 to 3.3), with higher levels of pain (OR = 1.5; 95% CI = 1.1 to 1.9), or with major depressive episode (OR = 4.4; 95% CI = 2.6 to 7.5) had greater odds for DAD. Similar to AAD, immigrants (OR = 0.4; 95% CI = 0.2 to 0.8) were less likely to report DAD (Table 4).
Weighted logistic regression models for drug abuse or dependence.
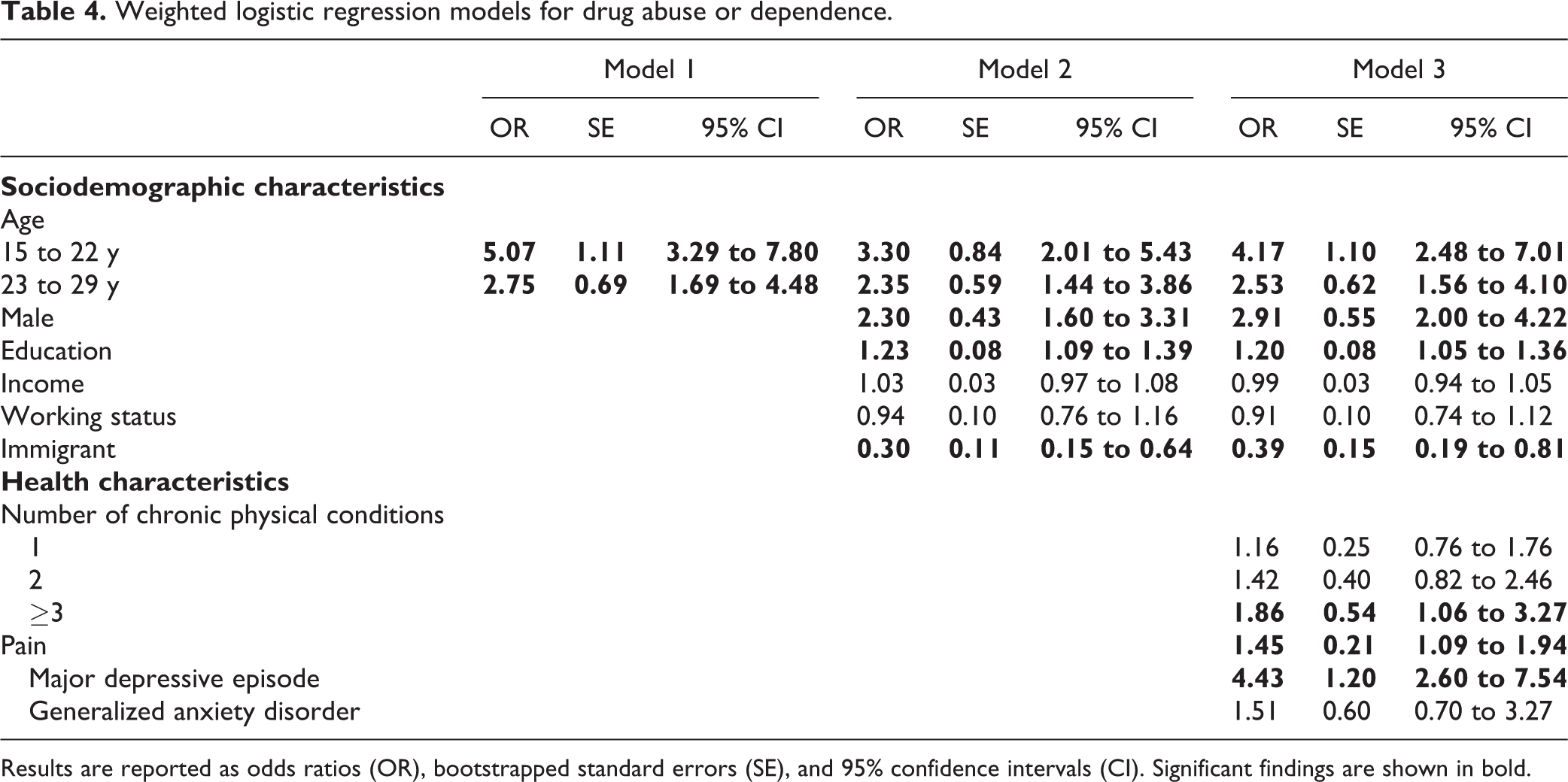
Results are reported as odds ratios (OR), bootstrapped standard errors (SE), and 95% confidence intervals (CI). Significant findings are shown in bold.
Moderating Effects
As shown in Table 5, generalized anxiety disorder (OR = 0.3; 95% CI = 0.1 to 0.9) was found to moderate the association between developmental period and AAD. Specifically, among early emerging adults, the odds of reporting AAD were higher for those without generalized anxiety disorder; however, among late emerging and young adults, odds were higher for participants with generalized anxiety disorder. No moderating effect was found for the association with DAD.
Moderating effects of sex and health characteristics on the association between age and SUDs.
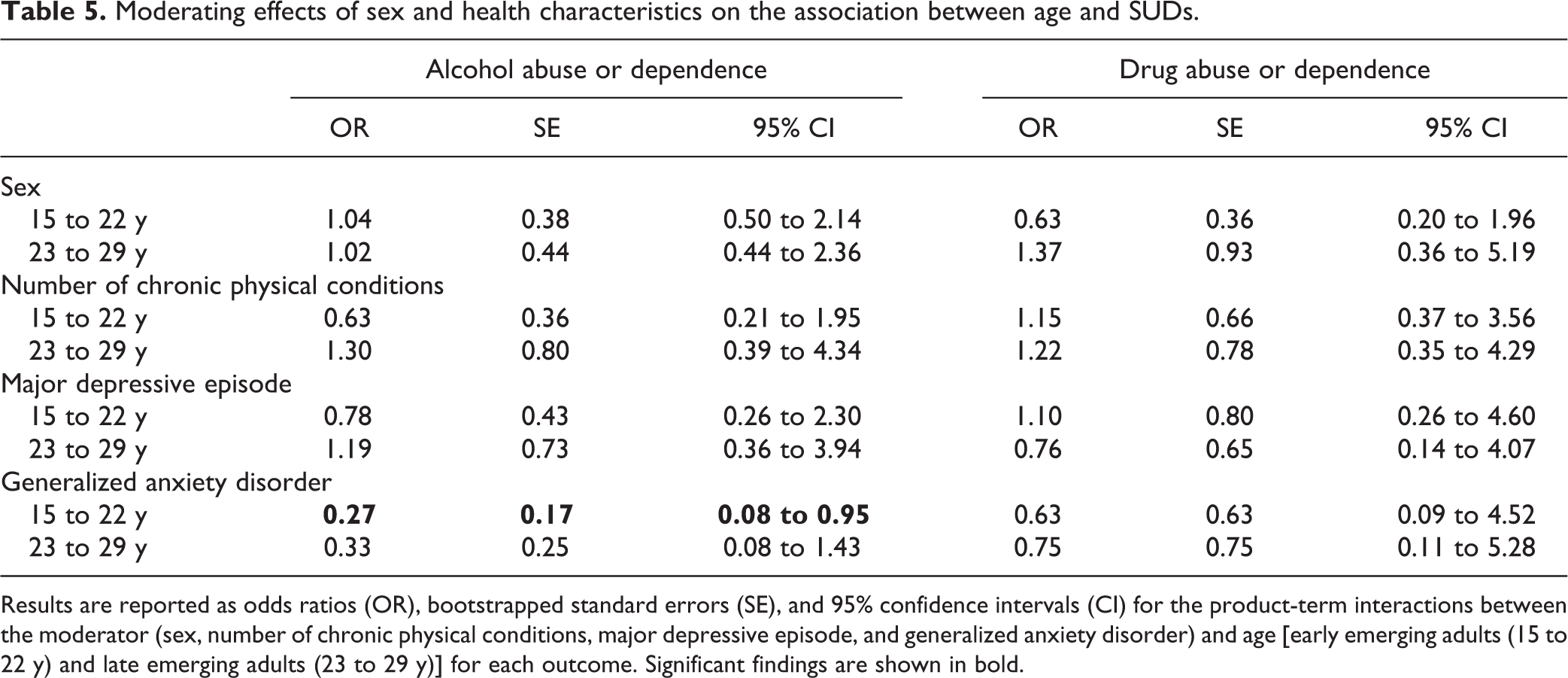
Results are reported as odds ratios (OR), bootstrapped standard errors (SE), and 95% confidence intervals (CI) for the product-term interactions between the moderator (sex, number of chronic physical conditions, major depressive episode, and generalized anxiety disorder) and age [early emerging adults (15 to 22 y) and late emerging adults (23 to 29 y)] for each outcome. Significant findings are shown in bold.
Discussion
Using recent data from a large nationally-representative Canadian survey, our findings suggest that the prevalence of past-year SUDs was highest among early emerging adults and lowest in young adults. After adjusting for relevant sociodemographic factors, age was inversely associated with SUDs. These findings align with those from previous cross-sectional epidemiological studies assessing SUDs in young people. 6,9,10 However, our estimates were slightly lower than those reported previously. For instance, according to the National Epidemiologic Survey on Alcohol and Related Conditions-III (NESARC-III), the prevalence of past-year AAD was 27% among 18- to 29-y-olds and 16% among 30- to 44-y-olds. Additionally, the prevalence of past-year DAD was 8% among 18- to 29-y-olds and 4% among 30- to 44-y-olds. 9,10 Several methodological factors might have contributed to such discrepancies, including the distinct conceptualizations of the age sub-groups and the varying diagnostic criteria (DSM-IV v. DSM 5). Research has suggested that prevalence estimates obtained using DSM 5 criteria are greater than those using DSM-IV because of 2 key changes: 1) Substance abuse and dependence have been combined into one category, and 2) thresholds for the diagnostic criteria for SUDs have been altered. 40 According to a systematic review of 12 studies, DSM 5 diagnostic criteria can increase the prevalence of alcohol disorders by 61% when compared to DSM-IV. 41 Similarly, research has also suggested an increase in the prevalence of drug disorders among adolescents (14 to 18 y) and young adults (18 to 35 y) with the DSM 5 v. DSM IV criteria. 42,43
To our knowledge, this is the first study assessing subgroup differences in SUDs for emerging and young adults. One other cross-sectional study has directly compared the prevalence of SUDs between emerging adults (18 to 25 y) and young adults (26 to 34 y) and found that emerging adults were twice as likely to report either past-year AAD or DAD. 44 That study however, did not include the full spectrum of emerging adulthood, did not stratify early and late emerging adults, and did not control for relevant mental disorders in their analyses—important factors which likely contributed to differences in the reported measures of association.
Notably, findings provide novel evidence for the extension of emerging adulthood into the late 20s. Evidence for this stems from the following: 1) The prevalence of SUDs was greater among emerging adults as compared with young adults, indicating that substance use behaviours during these 2 developmental periods are distinct and unique. It is important to note that early and late emerging adults had prevalence rates of SUDs that were significantly greater than that of young adults. 2) The phenomenon used to explain the decrease in the prevalence of SUDs from emerging adulthood to later developmental periods is termed “maturing out”; i.e., processes involved in maturation (e.g., parenting children, career establishment) that are incompatible with substance use explain the decrease in the prevalence of SUDs. 45 –47 Young people today view maturation processes, such as parenting, as perils to be avoided instead of achievements to be pursued until they reach their 30s; thus, substance use—a hallmark of emerging adulthood—has extended to the late 20s. 1,5,15 3) In post hoc analyses, we compared adjusted ORs for early and late emerging adults to examine whether magnitudes of effect were similar between these subgroups. The differences for AAD (ΔOR = −0.9, 95% CI = −2.64 to 0.65) and DAD (ΔOR = −1.6, 95% CI = −4.6 to 0.7) were not statistically significant, providing further evidence of the similarity between these subgroups and the extension of emerging adulthood into the late 20s.
Our findings also suggest that generalized anxiety disorder moderated the association between developmental period and AAD. Specifically, among early emerging adults, the odds of reporting AAD were higher for those without generalized anxiety disorder; however, among late emerging and young adults, odds were higher for participants with generalized anxiety disorder. Early emerging adults with anxiety disorders portray interpersonal deficits and often abstain from social activities. 48,49 Because the onset of alcohol use commonly occurs in social settings during early emerging adulthood, 50 early emerging adults with generalized anxiety disorder may be less frequently exposed to alcohol and subsequently develop AAD. This moderating effect is a novel finding; we encourage replication in other samples.
Limitations
This study included a large sample size, minimal missing data, reliable and valid measures of substance use disorders and other psychopathologies, and rigorous methodological methods (e.g., use of weights to adjust for non-response errors). However, the results should be interpreted in the context of the following limitations. First, due to the cross-sectional nature of the survey, temporal associations between developmental period and SUDs could not be assessed. Furthermore, it is possible that differences in SUDs between age groups were due to cohort effects. Second, while questions regarding student status are asked in the CCHS-MH, all educational institutions (e.g., secondary school, college, university) are aggregated. Research suggests that the risks for SUDs vary according to the type and level of study. 51,52 Third, due to sparse data, drug-specific disorders were aggregated. The prevalence and associations between developmental period and DAD may be heterogeneous across different illicit drugs. Additionally, possibly due to sparse data, generalized anxiety disorder was not found to moderate the association between developmental period and DAD.
Implications
Our findings support the need for tailored programs and greater systematic focus on preventing and treating SUDs among young people, especially early emerging adults. Considering the high prevalence of SUDs, school and non-school based prevention programs are required, such as motivational interventions with personalized feedback targeting emerging adults. 53 For emerging adults with SUDs, early interventions and empirically validated treatment approaches, such as cognitive-behavioural therapies and motivational enhancement in primary and tertiary care settings, have been deemed to be effective. 9,10 Within the health system, interventions aimed at early emerging adults, especially males, could also reduce the persistence of SUDs to later developmental periods and prevent functional impairment. 6,54 The education system is uniquely positioned to deliver broad risk-reduction strategies that have sustained effectiveness and reduce the stigma associated with seeking addiction and psychiatric services. 55,56 Additionally, social services should integrate their services with the education system to support participation, social and employment opportunities, and community engagement for young people thereby facilitating the prevention and reduction of substance use. 57
However, programs and policies should recognize the unique aspects of this developmental period that have contributed to decreased usage of services (e.g., transition out of pediatric system, less family involvement). 58 As such, services that uniquely target emerging adults may be required. For example, in the United Kingdom, YouthSpace works with general practitioners to treat psychiatric illnesses among 16- to 25-y-olds. 59 In the absence of recent epidemiological evidence for SUDs in young people, the results from this study can help inform the development and implementation of such programs in Canada.
Conclusions
In Canada, SUDs among young people are common, and emerging adults are at increased odds for SUDs as compared with young adults. In the context of SUDs, emerging adulthood appears to be extending further into adulthood, presenting challenges in the provision of addiction services. Integration and coordination of services within and across public sectors for young people with SUDs must be prioritized to reduce individual and societal burden. Longitudinal research is needed to expand these findings to investigate the extent to which SUDs in emerging adulthood is chronic, results in co-morbidity, and whether moderating and mediating factors persist across the life course.
Footnotes
Acknowledgments
We would like to thank the Research Data Centres Program at Statistics Canada for providing access to the data. While the research and analyses are based on data from Statistics Canada, the opinions expressed do not represent the views of Statistics Canada.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ferro is a member of the Editorial Board for the Canadian Journal of Psychiatry. None of the remaining authors has any conflict of interest to disclose. Findings from this manuscript were presented by Dr. Ferro at the 2018 Section Meeting in Epidemiology and Social Psychiatry of the European Psychiatric Association in Vienna, Austria.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mr. Qadeer was supported by an Ontario Graduate Scholarship. Dr. Ferro holds the Canada Research Chair in Youth Mental Health from the Canadian Institutes of Health Research (CIHR) and Early Researcher Award from the Ontario Ministry of Research, Innovation and Science.