
Abstract
Objective:
While mental illness is a risk factor for suicidal behaviour and many suicide decedents receive mental health care prior to death, there is a comparative lack of research that explores their experiences of mental illness and care. Suicide notes offer unique insight into these subjective experiences. Our study explores the following questions: “How are mental illness and mental health care experienced by suicide decedents who leave suicide notes?” and “What role do these experiences play in their paths to suicide?”
Method:
We used a constructivist grounded theory framework to select a focus of qualitative analysis and engage in line-by-line open coding, axial coding, and theorizing of the data. Our sample is a set of 36 suicide notes that explicitly make mention of mental illness and/or mental health care, purposefully selected from a larger sample of 252 notes.
Results:
The primary themes from our sample were 1) negotiating personal agency in the context of mental illness, 2) conflict between self and illness, and 3) experiences of mental health treatment leading to hopelessness and self-blame. These experiences with mental illness and mental health care can give rise to exhaustion and a desire to exercise personal agency, contributing to suicidal behaviour.
Conclusions and Relevance:
This study highlights unique perspectives by suicide decedents, whose voices and experiences may not have been heard otherwise, addressing a critical deficit in existing literature. These insights can potentially enrich clinical care or strengthen existing suicide prevention programs.
Suicide is one of the leading causes of premature death in Canada, with 4405 suicide deaths occurring in 2015. 1 Epidemiological data and demographic characteristics of suicide attempters and decedents are often used to propose pathways to suicide. 2,3 For example, empirically demonstrated risk factors for suicide, such as presence of mental disorders, past suicide attempts, and gender, have been used to substantiate the interpersonal theory of suicide. 4 There is far less research, however, that explores the subjective experiences of people who die by suicide, yet this is critical clinical information that provides the subjective context of risk factors. 5 Suicide notes are firsthand accounts that offer unique insight into the thought processes and emotional experiences of those who have died by suicide, information that is missed by quantitative analyses of suicide risk factors. Most studies examining suicide notes have used the notes to validate existing theories about suicide. Joiner and colleagues, 6 for example, compared the notes from completed versus attempted suicides. They found that perceived burdernsomeness (a key component of the interpersonal theory of suicide) was correlated with completer versus attempter status. There is a small but growing body of literature that takes an inductive approach to the study suicide notes, allowing for the generation of new ideas and theories about suicide. Sanger and Veach 7 investigated broad interpersonal themes within a large sample of suicide notes using grounded theory analysis, finding 7 themes that included “positive relationships,” “explanations,” and “concern for others.”
Suicide notes are left by approximately 15% to 38% of suicide decedents. Whether the findings from studies of suicide notes can be generalized to all those who die by suicide has been controversial, and the literature is inconsistent. 8,9 While suicide notes are not necessarily representative of the experiences of all people who die by suicide, they are an important way of understanding the lived experiences of individuals who have died by suicide. This type of understanding can guide us in identifying targets for interventions, which can then be tested in more generalizable samples, with the intent of developing more effective and impactful strategies to decrease the burden of suicide. 10 –13
Suicide notes can also provide insight into the role of mental illness, the feature that unites almost all people who die by suicide. Psychological autopsy studies show demonstrable mental disorders in at least 90% of suicide decedents. 14,15 In a cluster analysis of suicide deaths in Toronto, males aged between 18 and 65 years, who had had depression or another major mental illness, accounted for the majority of suicide deaths. 16 The epidemiological finding that mental disorders are nearly universally present in people who die by suicide has been well documented, but little is known about how mental illness is experienced by suicide decedents. A growing body of literature, however, suggests that illness identity and experience can have a significant impact on multiple psychiatric variables, including suicide. 17,18 In a cluster analysis, for example, individuals who had insight into their illness and self-stigmatizing beliefs about their condition had lower levels of hope and self-esteem than those who did not hold self-stigmatizing beliefs. 19
To our knowledge, suicide notes have not been used to explore perspectives on illness identity and experience. Our study aims to bridge this gap in literature; through the study of suicide notes, we intended to explore the subjectivity of illness and treatment experiences, to enhance our understanding of pathways to suicide. Specifically, we sought to answer the following questions: “How are mental illness and mental health care experienced by suicide decedents who leave suicide notes?” and “What role do these experiences play in their paths to suicide?”
Methods
Data Sources and Study Design
This study was approved by the Research Ethics Board at Sunnybrook Health Sciences Centre. A total of 1565 cases of suicide in Toronto between 2003 and 2009 were identified through the Office of the Chief Coroner for Ontario. A total of 516 files of suicide deaths made mention of a suicide note, and 290 contained notes or copies/transcriptions of the notes within the file. Exclusion criteria included notes solely written in another language (26 excluded), illegibility (6 excluded), and ambiguity about a particular document’s role as a suicide note (6 excluded). The remaining 252 notes were typed into a Word document by an investigator (J.Z.). To provide demographic characteristics of the note writers, we collected the age of the note writer, gender, and method of suicide from the original files, a key component of ensuring transferability in qualitative research. 20
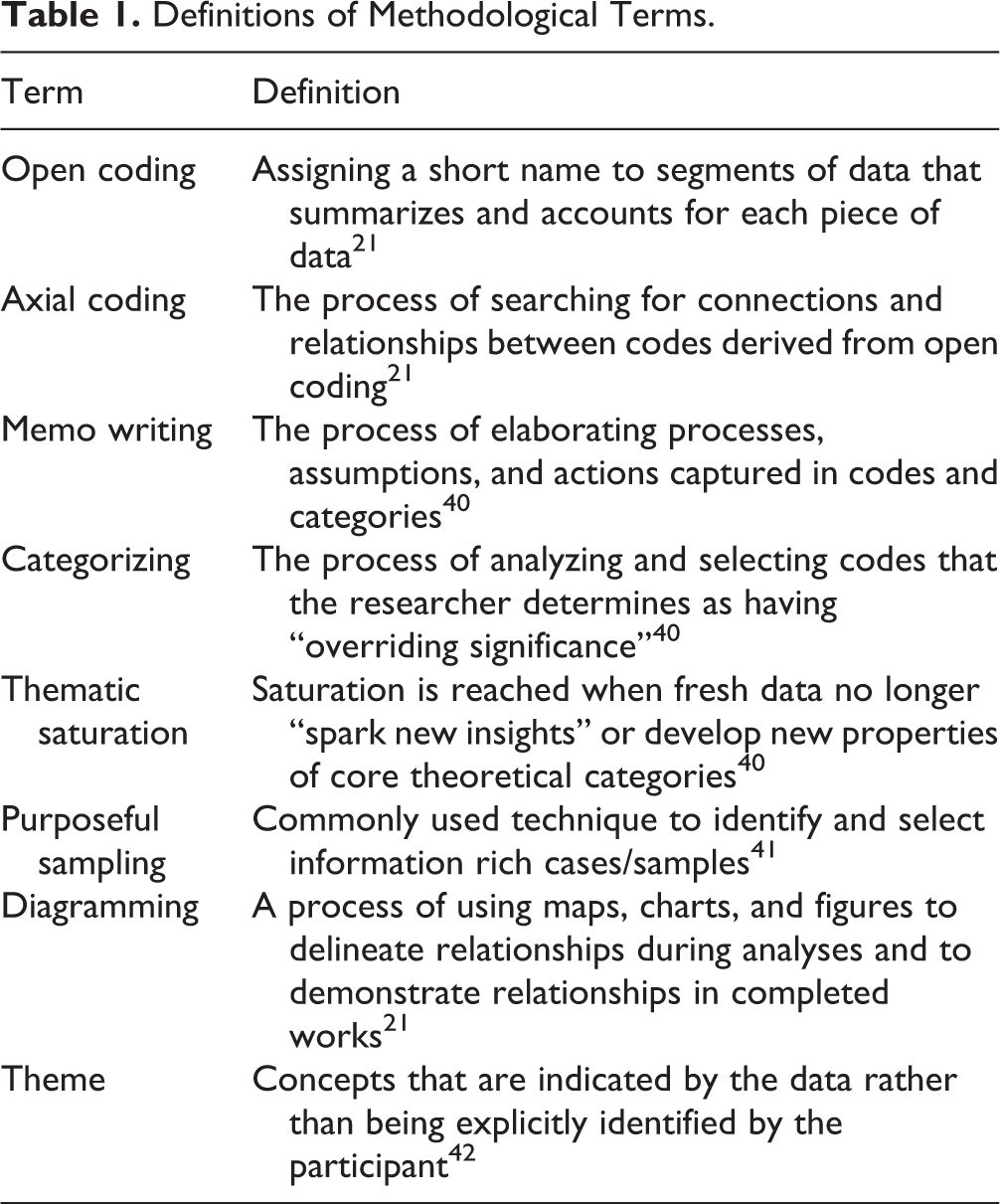
A constructivist grounded theory approach was used to both design the study and analyze the data. All variants of grounded theory include the following strategies: a) simultaneous data collection and analysis, b) exploring emergent themes through early analysis, c) discovery of basic social processes, d) construction of abstract categories that explain these processes, e) sampling to refine the categories. and f) integration of categories into a theoretical framework. Constructivist grounded theory specifically refers to the acknowledgement of multiple subjective realities, including those of both the researcher and the participants. A constructivist approach encourages the researcher to take a reflexive stance, allowing for a review of existing literature and formulation of research questions that guide data collection. 21 Definitions of methodological terms used in this section are presented in Table 1.
Definitions of Methodological Terms.
Selection of Purposeful Sample
In line with constructivist grounded theory, a specific area of focus was not selected at the outset, although potential areas of interest and gaps in literature were discussed. Two investigators (J.Z. and Z.F.) coded the notes independently, using line-by-line open coding, and discussed each set of 10 notes. Both coders were in regular contact through in-person and phone meetings to discuss and resolve any areas of ambiguity/disagreement. Memos were written after each note was coded and subsequently shared, discussed, and incorporated into data analysis. Next, the process of axial coding allowed the coders to produce categories that were revised as the coding progressed. Coding was continued until thematic saturation was reached. Both coders agreed that they were approaching thematic saturation after 60 notes. The next 11 notes were coded together, with both coders finding that no new theoretical concepts were emerging after 71 notes. From this initial open and axial coding, multiple code categories were delineated. One emergent category was “experiences of mental illness and mental health care.” Purposeful sampling was used to gather further data about this category. This code category of “experiences of mental illness and mental health care” was chosen due to the gap in literature around the intersections of illness identity and suicide identified above. All 252 notes were reviewed, and the coders independently extracted notes for the purposeful sample based on the following selection criteria: explicit naming of a mental illness (e.g., depression, addiction), reference to mental suffering, or mention of any form of psychiatric treatment. In total, a purposeful sample of 36 notes was chosen from the larger sample of 252 notes (Figure 1).

Selection of purposeful sample.
Analysis of Purposeful Sample and Model Development
All notes in the purposeful sample were recoded by Z.F. and subcategories were created, with a particular focus on searching for negative cases, a qualitative tool to ensure credibility. 20 Investigator J.Z. reviewed all codes and memos by author Z.F. The categories were used to develop tentative themes. While each theme reported below did not appear in every note, each theme was present within a significant portion of each subset of notes. Diagramming was used to propose links and connections between themes, to produce a descriptive narrative about the central phenomenon of the study (i.e., the interaction of illness identity and experience with suicidal behaviour). Our proposed model is presented in Figure 2. Composite quotes, created from multiple direct quotes illustrating each theme, are presented in the Results section. This was done to avoid directly quoting writers, so that writers remain unidentifiable, even by those who may have read the suicide notes. The composite quotes were reviewed by the entire research team to ensure that they represented the content of the original notes. To further ensure anonymity, the results are presented about groups of writers (n ≥ 3) rather than individual writers.
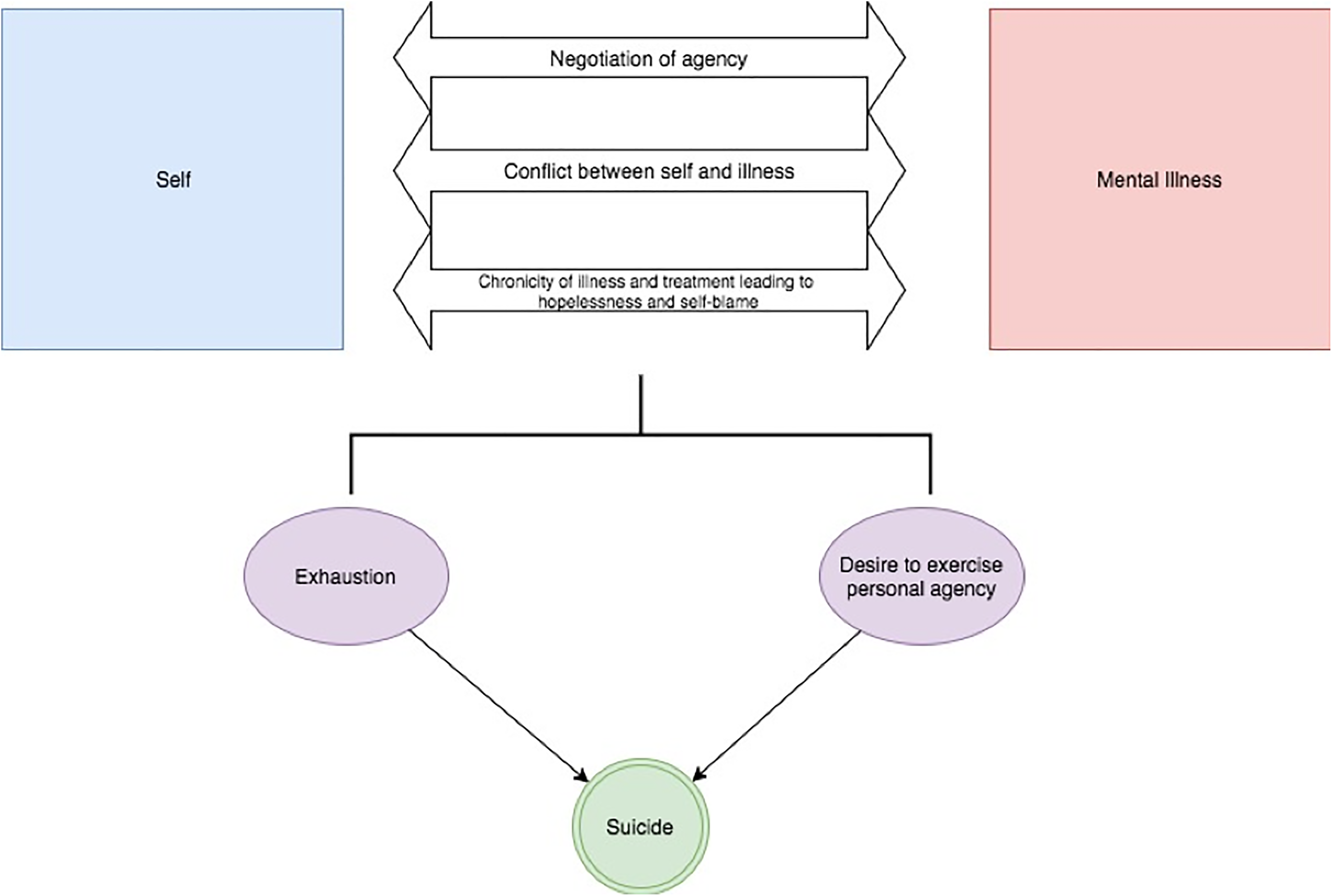
Pathways to suicide.
Reflexivity statement
Dr. Furqan is a resident in psychiatry and a trainee in the clinician scientist program (CSP) at the University of Toronto. She is supervised by Dr. Zaheer. Dr. Furqan has experience in qualitative research and her interests include suicidology. All 4 senior members of the research team are psychiatrists who have expertise in suicide research. In addition, Dr. Zaheer has expertise in qualitative research and methodology.
Results
In the following section, we present themes that emerged from the purposeful sample of 36 notes. Demographic data of the note writers along with characteristics of the notes are presented in Table 2.
Summary of Sample Demographics of Note Writers and Characteristics of Suicide Notes (N = 36).
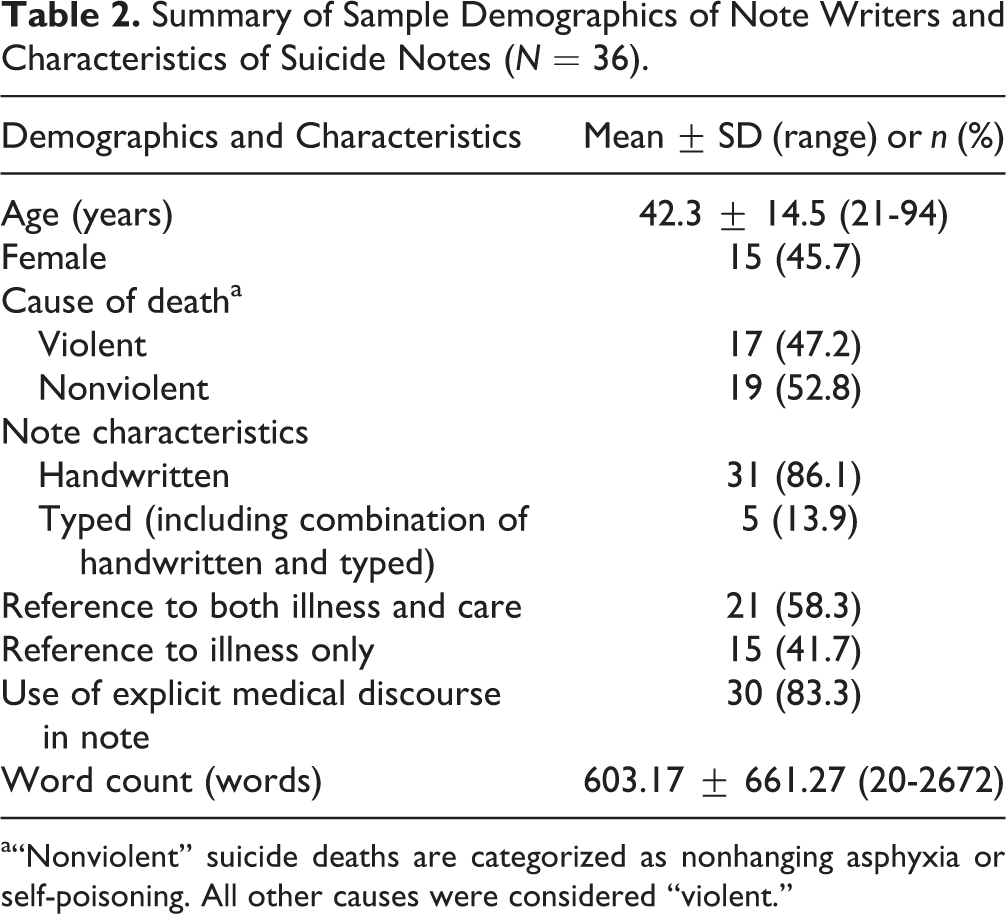
a“Nonviolent” suicide deaths are categorized as nonhanging asphyxia or self-poisoning. All other causes were considered “violent.”
Negotiating Personal Agency in the Context of Mental Illness
In total, we found that 16 people wrote about the degree to which they had control over their suffering in the context of mental illness. Some writers portrayed themselves as agents who were able to exercise control over their lives despite having mental illness, while others described themselves as having no control and seeing mental illness as dictating the course of their lives. In the following sections, we provide examples of writers grappling with concepts of agency in the context of mental illness.
High levels of perceived agency
Composite quote: “I had so much in my life—family, friends, career—but I let the disease, addiction, and my own personality take over me and it ruined everything in my life. Looking back, there were times that I should have changed the course of my life but I didn’t and now there is no hope left.”
Six writers described struggling with beliefs about high levels of personal agency in the context of a mental illness. These writers mentioned an inherent aspect of the self that was prone to mental illness but also their own perceived lack of effort to mitigate suffering in the context of this susceptibility. The tone of these writers indicates significant anger and resentment toward the self. These writers seemed to believe that since they had choice over the course of their illness and associated suffering that they should also be blamed for their condition.
Low levels of perceived agency
Composite quotes: “I sank into a deep depression. It was the depression that ruined my relationships. I want my family to know that.” “Forgive me. It’s not my fault, it’s a disease, I hope you can understand that.”
Ten people wrote about mental illness as an agent in itself, leaving the writer with limited or no agency. Their mental illness was described as directly causing problems in their life, as demonstrated by the composite quote above.
The writers who described mental illness as an agent with powerful control over their lives also asked their family and friends for forgiveness by describing negative outcomes in their life as consequences of mental illness. In this way, writers seemed to be commenting on not only agency but blame as well. Ascribing agency to mental illness seemed to allow these writers to shift blame away from themselves.
Illness as biological
Composite quote: “There is a problem in my brain. I think the chemistry is all wrong. No one could have fixed that.”
Six writers explicitly talked about biological or genetic causes of mental illness, and all of these writers portrayed a sense of hopelessness and pessimism associated with the biological nature of this illness. The biological underpinnings of disease are portrayed to be fixed and permanent. Inherent within the idea of permanent illness or illness that is incurable is the idea that no one, including the writers, has the power to actually change the course of their illness. Thus, it appeared that for these writers, agency might have been also restricted by their belief about the biological underpinnings of their illness.
Conflict between Self and Illness
Composite quote: “I have fought against my thoughts, depression and alcohol constantly. I am too tired to keep going.”
Five of the writers explicitly described a sense of conflict between “self” and “illness,” using words like fight, struggle, and battle. The difficulty, however, appears to be that self and illness are not entirely separate, and some writers tactically acknowledged that the line is not so clear between the illness and self. Thus, in some cases, writers appeared to be engaged in a struggle against their own selves. Four out of these 5 writers used terms such as tired and exhausted in association with this struggle, indicating that this process of fighting parts of the self uses significant mental and physical resources, leading to a sense of depletion.
Experiences of Mental Health Treatment
Among our sample of 36 notes, 20 writers discussed their experiences with mental health treatment or care. Forms of treatments that writers referred to include hospitalization, medications, psychotherapy, electoconvulsive therapy (ECT), naturopathic treatments, and lifestyle changes. In the following 2 sections, we highlight a subset of writers who wrote about repeated or multiple treatment trials.
Hopelessness secondary to chronicity of illness and treatment
Composite quote: “After trying multiple treatments, without curing my mental illness, I have realized that a solution other than death just does not exist.”
Ten writers spoke specifically about multiple attempts at trying to access care. In each case, the chronicity of the writer’s struggle with mental illness was highlighted and linked with the experience of hopelessness. Multiple attempts at treatment were seen as further evidence that their mental illness and subsequent suffering was permanent and untreatable.
Treatment failure as personal failure
“Medication, therapy, counseling, alcohol—I’ve tried everything and I can’t seem to figure out a way out of this, I can’t crack the code.” “It doesn’t matter how many treatments I try, there is something so wrong with me. It’s not the treatments, it’s me.”
In 5 of these 10 notes, the language used to describe ineffectiveness of the treatment was highly personalized and indicated that it was the writer who was responsible for relieving his or her own suffering. Writers used terminology like “I couldn’t” and “I just don’t know how to figure it out” or “I did try” to indicate that their attempts yielded unsatisfactory results—namely, that there was no ease to their suffering because their attempts and efforts had failed. Three writers also wrote about the belief that there is a deficiency within them that makes them unresponsive to treatment. For these 8 writers, the personalization of perceived failure or inadequacy seemed to heighten these writers’ suffering of experiencing not only the pain of mental illness but also the blame associated with their continued and prolonged suffering.
Exhaustion
Composite quote: “I am exhausted from trying to fix everything. No one understands, not even doctors or my family, and I keep trying to get help. I feel like I’m a dead man walking for a long time. I’ve been judged by society and have been made to feel ashamed. I’m burned out and tired and trying to find some way to rest.”
A common emotional experience within this sample of notes was the experience of tiredness or exhaustion. Twelve out of our total sample of 36 writers described a strong sense of fatigue associated with their path to suicide. Out of the 12 notes that explicitly made mention of tiredness and exhaustion, 8 of these notes specifically linked the sense of exhaustion to experiences of illness and treatment of mental illness. It is based on this that our model links experiences of mental illness and treatment to exhaustion and subsequently suicide.
Suicide as Exertion of Personal Autonomy
Composite quote: “I am the person who decides what I’m going to do with my life. After being isolated and marginalized, I’m done with it all. This is my life and my decision.”
Fourteen out of the 36 writers described the act of suicide as a purposeful choice or decision that highlighted their own autonomy. In the quote provided above, the writer first described the ways in which society or the external world took dignity away from the writer, leaving him or her with nothing to contribute. And then the writer explicitly described suicide as an independent decision. This quote is an example of the way that some writers contrast a sense of helplessness and lack of control in other areas of their life with the deliberate and independent act of suicide. Eleven out of these 14 writers specifically discussed either helplessness in other areas of their life or hopelessness about the idea that their life could improve. As we have described, experiences of mental illness and mental health care had an impact on perceptions of agency and hopelessness. Therefore, we propose that by limiting hope and perceptions of agency, experiences of mental illness and mental health care could contribute to a desire to exercise personal autonomy in the form of suicide.
The Model
The themes identified above were used to build a model of suicide that incorporates experiences with mental illness and mental health care (Figure 2). The dominant themes that emerged from our sample were 1) a struggle over agency stemming from biological and psychological beliefs about illness, 2) conflict between self and illness, and 3) hopelessness and self-blame in the context of treatment inefficacy. We propose that these conceptualizations of mental illness and treatment can contribute to a sense of exhaustion and a desire to exercise agency, both of which can contribute to suicidal behaviour.
Discussion
The aim of this study was to explore the subjective experiences of mental illness and care as described by suicide decedents. The importance of intersections between identity, self-image, and illness has been well established. Specifically in relation to mental illness, illness identity is described as “the set of roles and attitudes that people have developed about themselves in relation to their understanding of mental illness.” 17 “Self-efficacy” or “agency” is an important component of the phenomenon of illness identity. 22,23 Higher scores of self-stigma have been quantitatively linked with decreased self-efficacy or agency. 22,24 Our findings indicate that for some people, agency can be undermined by the acceptance of being “mentally ill.” However, on the other end, for those note writers who did perceive themselves as having greater agency, there was significant blame associated with being responsible for illness and suffering.
A previous study demonstrated that individuals who attributed biological causes to their depression seemed to express greater prognostic pessimism about their symptoms than individuals who did not have these aetiological views about their illness. 25 Similarly, we found that writers who held beliefs about biological aetiologies of their illness also described hopelessness about attaining relief from their illness.
Ideas about illness identity and empowerment have been studied in the context of chronic medical illness, with existing literature suggesting that “empowerment” in the context of chronic illness involves both “holding on” to preillness identities and “letting go” of total control and integrating postillness limitations into a new sense of self. 26 Given our findings, it is also possible that integration of chronic mental illness into a coherent sense of self may allow some individuals to feel more empowered than a continued struggle to separate self from mental illness.
Negative self-evaluation and low self-esteem have been linked with depression and suicidal ideation. 27,28 Our findings indicate that some individuals use inefficacy of treatment as evidence of their incompetency/failure, leading to heightened overall distress and exhaustion. The experience of exhaustion in suicide pathways has been discussed in previous literature. A previous model of suicide describes “suicidal exhaustion,” which is defined as exhaustion arising from living rather than one component of living and hopelessness about imagining a future that involves less exhaustion. 29
Our findings indicated that hopelessness was also exacerbated by experiences of multiple attempts at treatment and lack of treatment efficacy. Similar themes also emerged from a qualitative study of men who experienced depression and suicidal ideation. For these men, experiences of pain, ineffective medical or self-management, and escalating dysfunction contributed to the induction of despair/hopelessness. 30
Our findings regarding the theme of autonomy are supported by Pearce and Martin, 31 who demonstrated that an external locus of control (i.e., decreased sense of personal agency) was positively correlated with suicidal behaviour. The authors postulated that the reason for this may be that suicidal behaviour provides individuals with what is perceived to be the rare opportunity to exercise personal autonomy. A qualitative study involving Chinese Canadian women with a history of suicidal behaviour also highlighted “lack of agency” as a factor in pathways to suicidal behaviour. 32 Hill and Pettit, 33 however, found that autonomy indirectly influenced suicidal ideation via thwarted belonging and perceived burdensomeness, rather than directly impacting suicidal ideation. Our findings confirm that autonomy is significant in suicide pathways, although the exact mechanism of impact requires further exploration.
Implications for Clinicians
Limitations
This study was focused on exploration of the subjective experiences of 36 note writers who died by suicide. While this is a small sample size, it is comparable to other in-depth studies of suicide notes. 6,37,38 Our sample only included English notes or notes that were in English and another language, which also limits generalizability. It is important to note that our model does not suggest all suicide decedents who struggle with mental illness experience suicide as proposed by this model; rather, the purpose of this study is to highlight subjective and personalized experiences of mental illness and received care, valuable information that is missed in traditional epidemiological analyses. We would like to highlight that multiple aspects of identity, including gender, sexual orientation, race, and socioeconomic status, can inform people’s view of themselves and their illness and can be areas of further study. In addition, qualitative research involving participants with a history of suicidal behaviour, focusing on experiences of mental illness and mental health care, may also deepen our understanding of this topic.
This study is the first investigation of suicide notes to explore illness identity in the context of mental illness and suicide. The study highlights unique perspectives by suicide decedents whose voices and experiences may not have been heard otherwise, and we believe this addresses an important deficit in existing literature. This study adheres to the Standards for Reporting Qualitative Research (SRQR) recommendations. 39
Footnotes
Acknowledgements
We thank the Office of the Chief Coroner for Ontario for its assistance in providing us access to the suicide notes used in this study.
Access to Data
Due to ethics constraints, the authors are unable to share the data with interested investigators without permission from the Office of the Chief Coroner for Ontario.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.