
Abstract
Objectives:
The National Standard of Canada for Psychological Health and Safety in the Workplace (the Standard) was released in 2013. The objectives of this study were to 1) estimate the proportion of Canadian employers who were aware of the Standard, 2) examine the extent to which the Standard has been implemented, and 3) describe perceived barriers to implementing the Standard in Canadian organizations.
Methods:
A cross-sectional survey in Canadian employers was conducted between February 2015 and January 2017. A random sample of Canadian employers was selected, and the individuals who were knowledgeable about the occupational health policies of the organizations were interviewed by telephone. The participants answered questions about the awareness, implementation, perceived effects, and barriers to implementation. Descriptive statistics and chi-square tests were used to characterize the results.
Results:
A total of 1010 companies participated in the study. Overall, 17.0% reported that they were aware of the Standard; 1.7% and 20.3% reported that their organizations had implemented the entirety or elements of the Standard, respectively; and 71.4% of participants believed that elements of the Standard would be implemented within the next year. The perceived effects associated with implementation of the Standard included increased job satisfaction and employee retention while the greatest barrier to implementing the Standard was the belief that psychological health and safety are irrelevant in the workplace.
Conclusions:
Many Canadian employers are still unaware of the Standard’s existence; however, most Canadian employers are positively inclined toward the Standard in its potential to help employee productivity and job satisfaction.
In 2010, the Global Burden of Disease study reported that mental and behavioural disorders accounted for 7.4% of disability-adjusted life years (DALYs) out of all global diseases. 1 Specifically, Murray et al. 1 found that major depressive disorder (MDD) (2.5%), anxiety disorders (1.1%), drug use disorders (0.8%), alcohol use disorders (0.7%), and schizophrenia (0.6%) are the 5 leading mental health conditions contributing to more than 15 million DALYs. In Canada, the observed DALYs for mental health and substance use disorders are 2836.89 DALYs per 100,000. 2 These statistics are further corroborated by the Mental Health Commission of Canada (MHCC) estimating that about 500,000 Canadians are unable to attend work each week due to mental health issues. 3 A study conducted under the guidance of the MHCC, using the 2010 Canadian Community Health Survey (CCHS) data, found that individuals with higher levels of work stress had higher odds of being diagnosed with mood and anxiety disorders. 4 The lifetime prevalence of mood and anxiety disorders from that study was 6.7% and 4.8%, respectively, while the lifetime prevalence of mental disorders in the workplace reported using CCHS data was estimated to be about 16.5%. 4 In 2010, the MHCC reported that mental health problems cost Canadian employers $6 billion per year in lost productivity due to presenteeism and absenteeism. 5 Hence, prevention of mental health problems in the workplace has important health and economic implications.
Improving employee mental health requires a thorough understanding of the determinants of workplace mental health problems. In the past decades, epidemiological research has identified a number of factors that may precipitate the risk of mental health problems in workplaces. For example, a recent systematic meta-review reported that high job demands, low job control, high effort–reward imbalance, low relational justice, low procedural justice, role stress, bullying, and low social support in the workplace are associated with a greater risk of developing common mental health problems. 6 In principle, changing employee exposure to these risk factors could lead to reduced risk of developing a mental health problem. 6,7 There are different strategies for changing employee exposure to these risk factors. One important strategy could be a policy intervention targeting all employers, which would aim to improve the work environment and change employee exposure to risk factors, reducing their risk of developing common mental health problems. In Canada, the most recent policy development in workplace mental health is the release of the National Standard of Canada for Psychological Health and Safety in the Workplace (the Standard). 8
In January 2013, the MHCC partnered with the Canadian Standards Association and the Bureau de Normalization du Québec developed and released the Standard. 8 The purpose of the Standard, a voluntary set of guidelines, was to promote employee psychological health and prevent psychological harm through the application of a Psychological Health and Safety Management System framework highlighting 5 key elements: commitment; leadership and participation; planning, implementation, evaluation, and corrective action; and management review. 8 The Standard recommended that employers should closely monitor 13 risk factors in their workplaces, including job demand, psychological support, work/family balance, organizational culture, protection from violence, bullying, and harassment. 8 The release of the Standard signified a new and important policy intervention, both from a national and a global perspective. 3,9
The MHCC created a 3-year Case Study Research Project (CSRP) that provided reports from 2015, 2016, and a final report in 2017 on the development of the Standard implementation in more than 40 organizations across the country, tracking their initial implementation of the Standard and their progress over the 3 years. 3,9 Their findings corroborated previous research that showed that many Canadian employers recognize the importance of psychological health and safety and the critical importance in finding a structured response to prevent psychological harm and promote psychological safety in response to the growing needs of their employees. 10 A qualitative study in Alberta by Kunyk et al. 10 found that the Standard resonated with employers’ organizational values and beliefs but that organizational cultures and sizes could determine how the Standard should be implemented. Since the release of the Standard, there has been little research on quantifying the awareness and implementation of the Standard using a national sample of Canadian employers and how the awareness and implementation may vary by organizational and geographic characteristics. The MHCC’s case study on the Standard was based on a small sample of employers and followed up over several years to see the effects of implementing the Standard. 3,9 Similarly, the study by Kunyk et al. 10 used qualitative methods to understand employer perspectives toward the Standards.
The objectives of this study were to 1) estimate the proportion of Canadian employers who are aware of the Standard, overall and by organizational characteristics; 2) examine the extent to which the Standard has been implemented by Canadian employers, overall and by organizational characteristics; and 3) describe perceived barriers to implementing the Standard in Canadian employers.
Methods
Study Design
For the objectives, a cross-sectional study was conducted in a sample of Canadian employers between February 2015 and January 2017. The Dun & Bradstreet’s Hoover Business directory (D&B) (www.dnb.com) was used as a sampling frame for selecting Canadian employers. The D&B is considered a leading source of commercial information containing more than 140 million business records, of which approximately 1.3 million are Canadian companies. The D&B database has also been used by the US National Worksite Health Promotion Activities Survey. 11 Information available from the D&B includes but is not limited to specific worksite location, occupational sector, number of employees, telephone and fax numbers, and contact information for a variety of top executives and management positions. The Conjoint Health Research Ethics Review Board at the University of Calgary approved the study.
Data Collection
We randomly selected 50,000 employer records from the D&B database. The target population were employers who are operating in Canada and who have at least 4 employees. Data were collected using the method of computer-assisted telephone interview by trained interviewers in either English or French, as preferred by participants. The goal of the sampling strategy was to get a nationally representative sample of employers. Invitation letters along with a summary of the Standard were mailed out to employers about the study around 2 to 3 weeks before the initial telephone contact. The invitation letter explained the project, when to expect the interview call, and contact information so that employers would be prepared for contact by the interviewers. In the telephone interviews, employers were informed that their information would only be used in aggregate and informed of the privacy and confidentiality around their answers. Interviewers then obtained consent to participate in the study and made sure the organization was eligible for inclusion in the study (e.g., had more than 4 employees). The person contacted was an employer or represented the employer, who could speak with authority and knowledge on the business’s health policies, procedures, and employee wellness programs. These interviewees included health and safety managers, human resources executives, business owners, or occupational physicians.
Measurements
A questionnaire was developed based on the results of our focus group discussions 10 and input from stakeholders from Mental Health Commission of Canada, Canadian Mental Health Association–National/Calgary, and occupational mental health professionals. The interviews collected data about organizational demographics, preexisting psychological health and safety policies, awareness about the Standard prior to the invitation to participate in this study, the extent to which the Standard has been implemented by the organization, perceived effects, and barriers to implementation.
Data Analysis
Descriptive analyses included tabulating organizational demographics (e.g., size of the organization, industry of the organization), awareness of the Standard, and implementation of the Standard (or likelihood of implementing the Standard). To examine whether the awareness and implementation of the Standard changed over time, the proportions of awareness and implementation of the Standard were estimated and compared by 6-month intervals over the study period. Results were summarized using percentages and associated 95% confidence interval (CI). To account for the differences between our sample and Canadian employers in the distributions of number of employers in different provinces and size of business, we developed weights using pertinent data published by Statistics Canada. 12 The estimates presented in the manuscript were weighted. Analyses were done using Stata version 14. 13
Results
Fifty thousand Canadian companies were first randomly selected from the D&B database. Among the 50,000 companies, 19,172 were selected proportional to the population size of the regions (British Columbia, Prairie provinces, Ontario, Quebec, Atlantic region, and Northern region) and were contacted. Multiple attempts were made to contact these companies through mail and telephone between February 2015 and January 2017. Many employers were unable to be reached for a number of reasons, including no answer, wrong number, the number was no longer in service, call went straight to voicemail, business no longer existed or moved, interviewer was disconnected, or because of language barriers. A total of 2069 participants were able to be reached by telephone, of which 1010 employer representatives completed the survey (response rate = 48.8%). Table 1 shows the demographic characteristics of the employers that were included in the analysis.
Demographic Characteristics of Canadian Employer Sample.
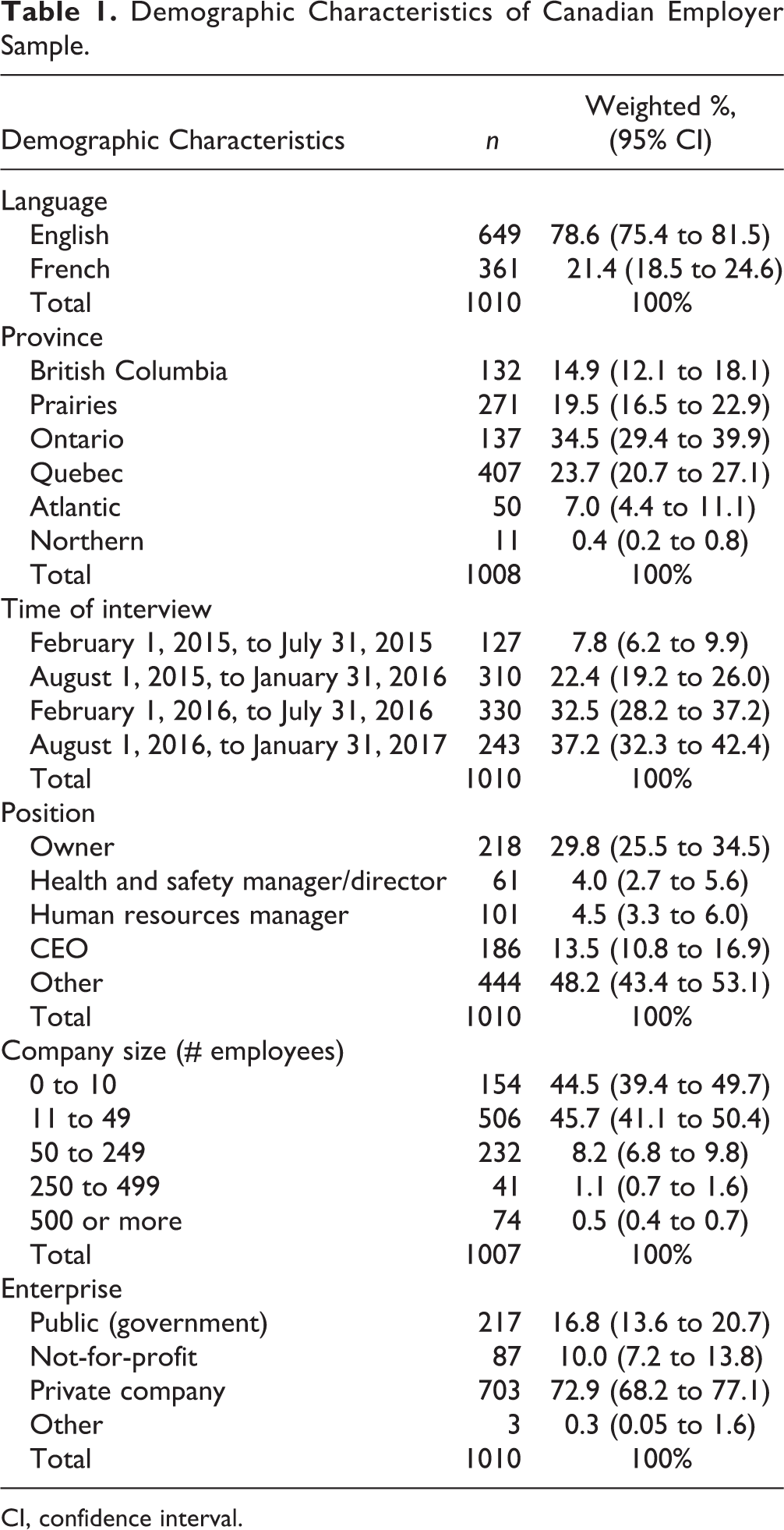
CI, confidence interval.
The data showed that over the study period, 17.0% (95% CI, 13.8% to 20.7%) (n = 226) of the participants reported that they were aware of the Standard prior to the invitation to participate in this study. Awareness of the Standard did not differ significantly by language and region but rather by employer characteristics such as position, company size, and enterprise. Employers in the government and public administration sector and of larger company size (more than 500 employees) were more likely to report the awareness of the Standard; interviewees who were human resources managers and health safety managers/directors were more likely to be aware of the Standard than others (Table 2). The awareness did not differ by the time when the interview occurred.
Awareness of Workplace Psychological Safety Standard in the Sample of Canadian Employers.
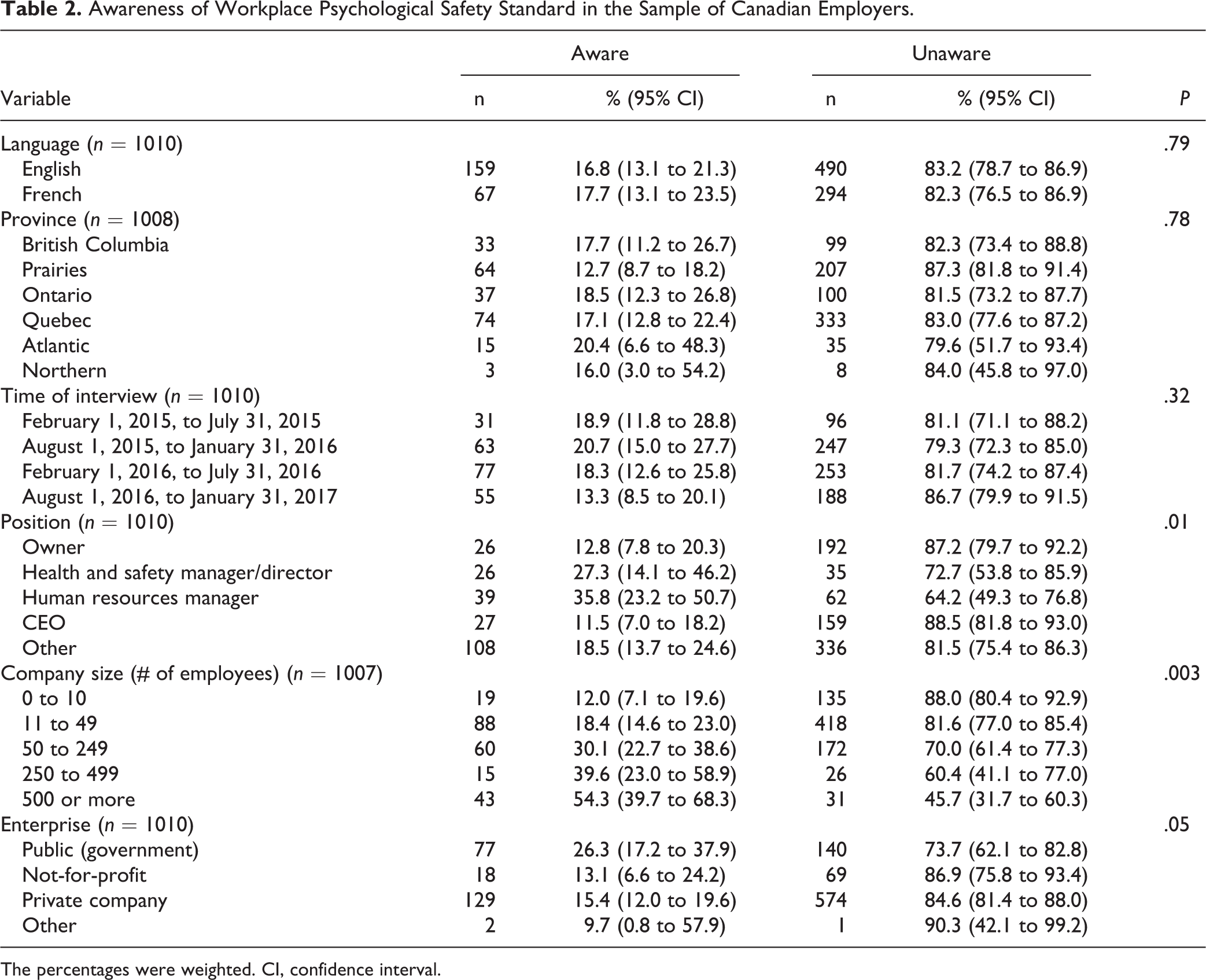
The percentages were weighted. CI, confidence interval.
We found that, at the time of the interview, 1.7% (95% CI, 1.0% to 2.9%) and 20.3% (95% CI, 16.6% to 24.5%) of the organizations (n = 240) had implemented the Standard in entirety or some elements, respectively. Table 3 displays the likelihood of implementation (in entirety or elements) by demographic and occupational characteristics. The data show that implementation differed significantly by geographic region, time of interview, and enterprise. Employers in Ontario reported the lowest level of implementation (9.9%). Among employers who had fully or partially implemented the Standard, about 40% of them implemented the Standard between February 2015 and July 2015; the proportions of implementation in subsequent intervals decreased. The not-for-profit organizations had the highest level of implementation (34.2%) compared with others. The level of implementation did not differ by language, participant position, or company size.
Likelihood of Implementing the Standard.
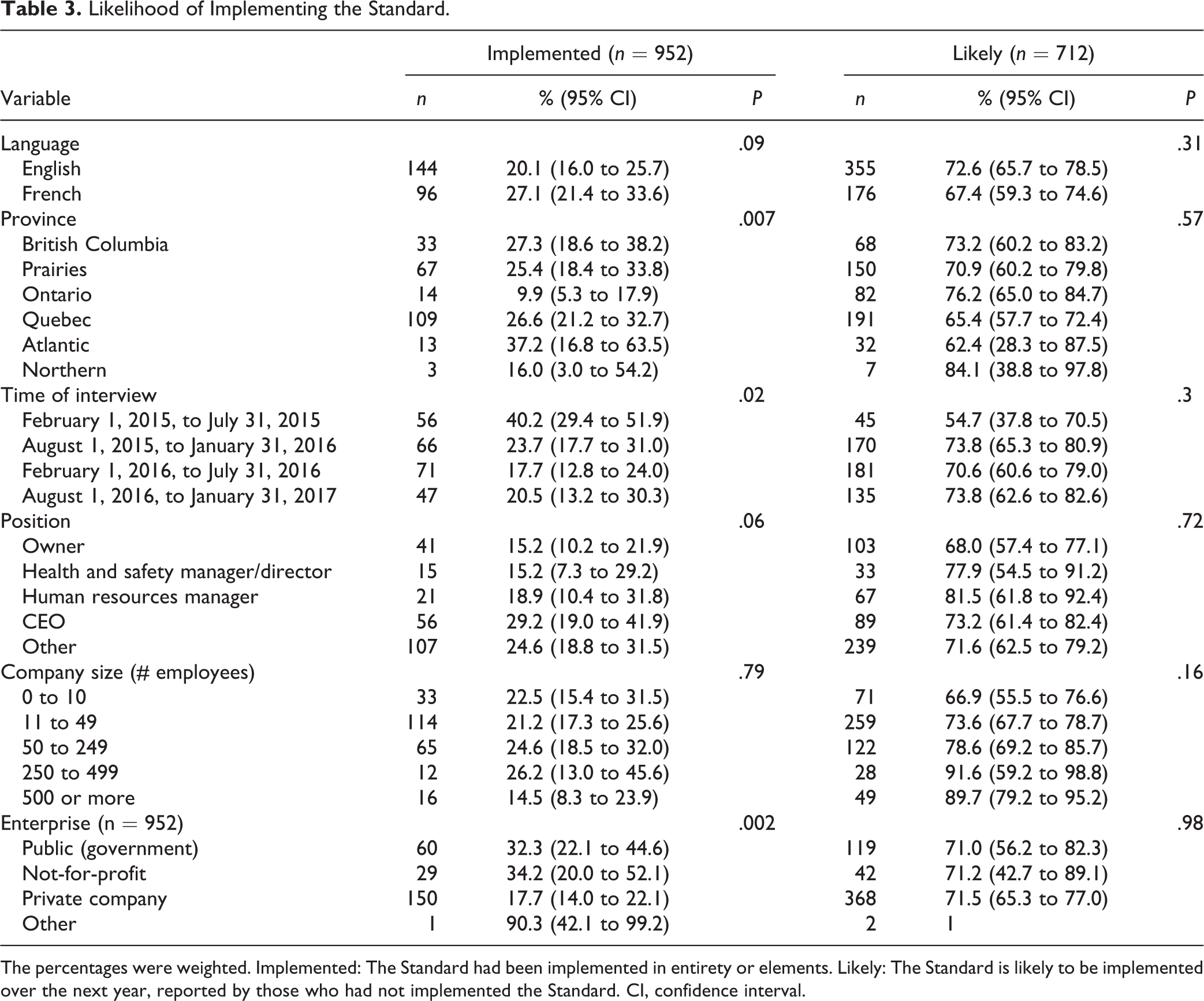
The percentages were weighted. Implemented: The Standard had been implemented in entirety or elements. Likely: The Standard is likely to be implemented over the next year, reported by those who had not implemented the Standard. CI, confidence interval.
Among those who had not implemented the Standard (n = 712), when asked whether the entire Standard or elements of the Standard would be implemented within the next year, 71.4% (n = 531) said that this was likely, and 28.6% (n = 181) reported that it was unlikely. The likelihood of implementing the entire standard or elements of the Standard within the next year did not differ significantly by language, province, or occupational characteristics (Table 3).
In addition, participating organizations were asked about the perceived effects of implementing the Standard or elements of the Standard among those who had already implemented it (n = 240). From the employer’s perspective, the greatest benefits of implementing the Standard were “increased job satisfaction” and “increased employee retention,” with 56.2% (n = 105) and 49.8% (n = 90) of employers answering, “a great deal” to these 2 questions (Table 4).
Effects of Implementing the Workplace Psychological Safety Standard/Elements.
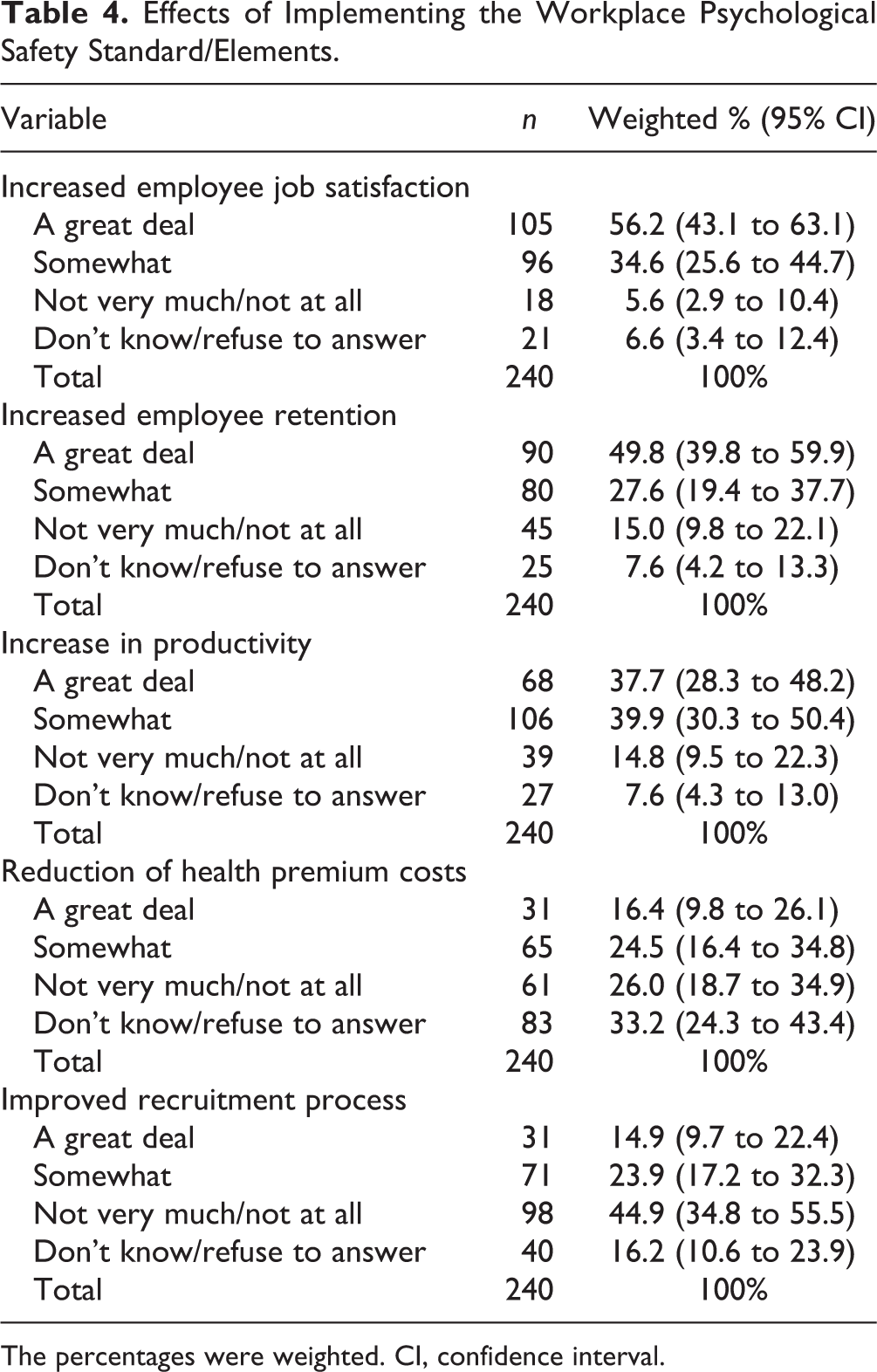
The percentages were weighted. CI, confidence interval.
Table 5 shows the perceived barriers to implementing the Standard or elements of the Standard among the participants who reported that their organizations were unlikely to implement the Standard (n = 181). The significant barriers to implementing the Standard were the following: “don’t have the personnel resources” (13.9%), “psychological health and safety is irrelevant to us” (13.3%), and “don’t have the knowledge to implement it and track it” (12.3%).
Barriers to Implementing the Workplace Psychological Safety Standard (n = 181).
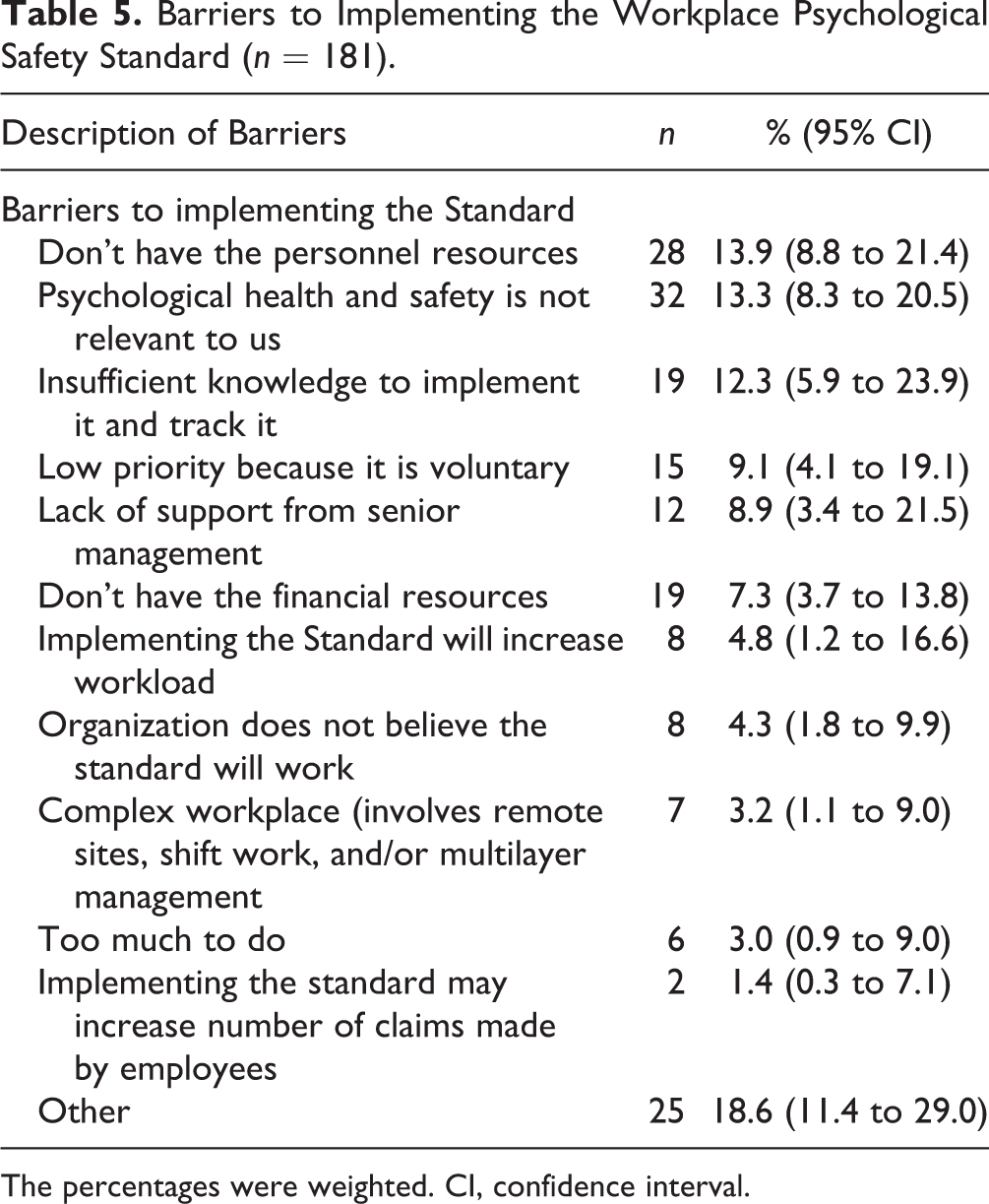
The percentages were weighted. CI, confidence interval.
Discussion
With this cross-sectional study, we found that the awareness level of the Standard in Canadian employers was low (17.0%), and it has not increased over the study period. Larger companies and employers in the sector of government and public administration were more likely to know the Standard compared to their counterparts. Geographically, Atlantic Canada was most aware of the Standard, and Quebec was most unaware of the Standard. Only 1.7% of employers had fully implemented the Standard while about 20.3% had partially implemented the Standard. Increased job satisfaction and increased employee retention were the top perceived benefits reported by those who implemented or partially implemented the Standard. The major barriers to implementing the Standard included “don’t have the personnel resources,” “psychological health and safety is not relevant,” and “don’t have the knowledge to implement it and track it.”
There has been limited research on the awareness and implementation of the Standard since it was introduced in 2013. MHCC conducted the 3-year Case Study Research Project from 2014 to 2017, looking at the progress and experiences of more than 40 employers that had implemented the Standard in their organizations. 3,9 Over time, the MHCC found that organizations improved from baseline scores in 2014 in compliance with 5 elements of the Standard (commitment and policy, planning, implementation, evaluation and corrective action, and management review) until the end of the study. 8 The most common actions taken by organizations participating in the project were around implementing workplace polices regarding respect, courteous communication, and bullying as suggested by the Standard, as well as providing education to employees, providing early intervention through employee assistance programs like Employee & Family Assistance Programs (EFAP) to help address mental health issues, and also raising general awareness about mental health among employees to reduce the stigma associated with mental illness. Unlike our results, MHCC found that a lack of personnel support or “psychological health/safety does not apply to us” was not a barrier to implementation but rather factors like “inconsistent data collection” and “uncertainty in defining and reporting excessive stress and critical events” were considered barriers to implementation. 9 Their findings are consistent with one of the barriers identified in our study (i.e., “don’t have the knowledge to implement it and track it”). The Case Study Research Project stressed the importance of consistent and ongoing leadership support and involvement and adequate structure and resources as facilitators to implementation. 9
Similar legislations/regulations exist in other countries as well, such as the Work Health Promotion (WHP) Council Directive 89/391/EEC by the European Union (EU). 14 Adopted in June 1989, the WHP directive has undergone multiple iterations, eventually incorporating psychosocial risks in the workplace and managing them in 2009. 14 The WHP directive is unique in that it provides the broad mandate each country in the EU must follow (i.e., have a health and safety framework covering a range of issues, including psychosocial risks) but also that the details are up to each country individually. 14 Some countries, like Latvia, incorporated the mandate into existing legislation (the Latvian Labour Protection Law). 14 The main barrier to implementation of laws governing the WHP was reported to be the absence of preexisting workplace occupational health care legislation that was separate from general occupational safety legislation. 14 Without specific workplace occupational health care legislation, there were some issues in the implementation of all aspects of the WHP, including the psychosocial aspects. 14 The lack of 2 separate pieces of legislation as a barrier is different from the findings observed in this study. The Standard has different barriers to implementation, partly due to the fact that the implementation of the Standard is voluntary, whereas the WHP seeks to set up psychosocial guidelines in the workplace for all EU members. 14 The Centers for Disease Control and Prevention (CDC) in the United States also has a voluntary model (the workplace health model) that workplaces can follow. 15 However, there has been no published research on the awareness, implementation, and barriers to implementation of the CDC framework. There has been no published research on the level of uptake for either the EU WHP legislation or the CDC framework. Therefore, direct comparisons to the Standard cannot be made.
It is not surprising that large companies were more likely to be aware of the Standard. Large employers tend to have more human resource personnel that keep current with new voluntary legislation like the Standard and have established health policies and employee wellness programs. As shown by the data, human resources personnel and occupational health and safety managers were more likely to be cognizant of the Standard, which may partly explain why many employers considered “don’t have personnel resources” as the greatest barrier to implementing the Standard. Organizations in government and public administration were also more likely to be aware of the Standard, which could be due to more extensive links between the MHCC, Canadian Standards Association (CSA), and Bureau de normalisation du Québec (BNQ)’s relationships with government. Similarly, the increased awareness of the Standard among public health care organizations is likely due to the same reason.
Despite that only a small proportion of employers were aware of the Standard before the study, among those who had not implemented the Standard, 71.4% reported that they were likely to implement the Standard over the next year, showing receptivity to the idea of the Standard. Prior to the telephone contact, we mailed invitation letters along with a summary of the Standard to the employers. Participants had the opportunity of reviewing the content of the Standard before the telephone interviews. The large proportion of potential implementation over next year may be partly due to the increased awareness after reviewing the summary. This is consistent with the qualitative finding by Kunyk et al. 10 that there was a lot of receptivity among employers in supporting the psychological health of employees in the workplace. Our data showed that the likelihood of implementation over next year did not differ by occupational characteristics. Some of the nonsignificant differences could be due to insufficient power, for example, the company size and position. Future studies need to examine if the actual implementation is consistent with this particular result. Over the 2-year study period, the rate of implementation was relatively low. This result could be explained by one of the themes by Kunyk et al. 10 in that the implementation of the Standard must be tailored to organizational culture and size and employers may not have sufficient knowledge of implementation.
The least common barrier in implementing the standard was “implementing the Standard may increase number of claims by employees,” which points to many employers not concerned about the potential for abuse or employees “faking it” as a result of implementation of the Standard. This observation gives more credence to employers being receptive to the Standard, as observed in previous studies. 10 The organizations that have implemented (or partially) the Standard observed positive benefits, including enhanced job satisfaction and increased employee retention. Future implementation and evaluation research need to pay more attention to the impact on employee productivity and costs.
This study is the first descriptive and quantitative study looking at the awareness and implementation of the Standard 5 years after its implementation. Our previous study examined qualitative themes that emerged from focus group sessions with employers that informed our survey in this study. 10 Furthermore, this study has a robust sample size collected over 2 years from all geographic regions across Canada. However, this study had several limitations. First, as this is a cross-sectional study, causal inference cannot be made. Second, more studies are needed to examine if there is an increase of awareness and implementation over time, as data collection over time may give employers increased opportunity to become aware of the Standard and consider implementing it. Third, we attempted to contact about 20,000 employers. Only 1010 participated in the study. Quebec employers were overrepresented in the sample. Despite the fact that we weighted on the number of employers in each province and the company size, selection bias may have occurred because of unweighted characteristics. Therefore, the estimates of this study should be interpreted with cautions. Nevertheless, with a large sample size, we were able to estimate the weighted proportions of awareness and implementation of the Standard by participants’ occupational characteristics to minimize the threats to the validity of the estimates.
Conclusions
The Standard is the first major policy development in preventing psychological injuries in workplaces. Since its release in 2013, the awareness of the Standard has been relatively low, pointing to a potential need for more knowledge translation and information dissemination of the Standard. The awareness and implementation varied by occupational characteristics. The high proportion of respondents affirming the importance of protecting psychological health and safety in their workplaces shows that further work on marketing and promoting the Standard is required. The results of this study indicate that more work still needs to be done on education and promoting the Standard, as well as emphasizing the relevance of psychological health and safety among Canadian employers. Further research is needed to examine the implementation strategies that tailor the Standard to organizational needs and capabilities, as well as demonstrate the economic benefits of the implementation.
Footnotes
Acknowledgements
We thank M. Craig-Broadwith, S. Gundu, N. Rewari, and M. A. Baynton for their constructive comments on the questionnaire and E. Jones, R. Huntley, J. Thomas, M. Uppal, S. McKinney, and N. G. Tafreshi for their assistance in data collection.
Data Access
The data were collected and kept by Dr. JianLi Wang’s laboratory. Please contact Dr. Wang for data access.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Department of Psychiatry, Faculty of Medicine, University of Calgary, and Mathison Centre for Mental Health Research and Education, Hotchkiss Brain Institute, University of Calgary.