
Abstract
Objective:
This study sought to examine differences in sociodemographic risk factors, comorbid mental conditions, clinical presentations, and functional impairments associated with past-year generalized anxiety disorder (GAD) between Canadian Armed Forces (CAF) Regular Force personnel and the Canadian general population (CGP).
Method:
Data were from 2 nationally representative surveys collected by Statistics Canada: 1) the Canadian Community Health Survey on Mental Health, collected in 2012 (N = 25,113; response rate = 68.9%); and 2) the Canadian Forces Mental Health Survey, collected in 2013 (N = 8,161; response rate = 79.8%).
Results:
The prevalence of lifetime and past-year GAD was significantly higher in the CAF (12.1% and 4.7%) than in the CGP (9.5% and 3.0%). Comorbid mental disorders were strongly associated with GAD in both populations. Although the content area of worry and the GAD symptoms endorsed were similar, CAF personnel were significantly more likely to endorse specific types of worries (i.e., success at school/work, social life, mental health, being away from home or loved ones, and war or revolution) and specific symptoms of GAD (i.e., restless, keyed up, or on edge and more irritable than usual) than civilians, after adjusting for sociodemographic covariates and comorbid mental disorders. CAF personnel with past-year GAD reported significantly higher functional impairment at home than civilians with past-year GAD.
Conclusion:
GAD is a substantial public health concern associated with significant impairment and disability in both military and civilian populations. GAD in military and civilian populations shows similarities and differences: Key similarities include its extensive comorbidity and significant functional impairment, whereas key differences include the focus of worries and symptom profile.
Generalized anxiety disorder (GAD) is a mental disorder characterized by excessive and uncontrollable worry over a wide variety of topics. 1 Globally, lifetime prevalence of GAD ranges from 0.4% to 31.1%, with past-year or current diagnosis estimates ranging from 0.2% to 12.7%. 2 –7 GAD is highly comorbid with other mental disorders in the general population. 2,4 –6,8 –13 The severity of GAD symptoms and comorbidity with other mental disorders is associated with an increased level of impairment. 5,7,14 However, substantial research suggests that GAD is associated with significant functional impairment independent of comorbid conditions. 3,5,9,12,13,15,16 GAD is also associated with poorer self-reported health, 16 psychological well-being, 17 impaired physical functioning, 17 lower quality of life, 9,17 and suicidal ideation and attempts. 9,18,19 Individuals with GAD are high users of primary care services; 4,6,9,14,15 yet most do not seek treatment for worry but, rather, for more vague, general, and nonspecific problems, such as headaches, gastrointestinal distress, sleep problems, muscle tension, and irritability. 4,6,20 As a result, GAD is poorly recognized in primary care settings, often not diagnosed, and results in many individuals with GAD receiving inadequate or ineffective treatment. 6,14
The impact of GAD also extends into the workplace, where it is associated with higher work absenteeism, 13 decreased work productivity, 15 and substantial functional role impairments at work. 12,16 The military is an important aspect of the workforce and fulfills an important societal role; thus, the mental health of military personnel is therefore of public interest. Although mental health problems can have a considerable impact on military populations, posttraumatic stress disorder (PTSD), depression, and alcohol use disorders have overwhelmingly been the focus of mental health research and its consequences in military personnel. GAD is also of potential importance because: 1) it has substantial incidence and prevalence in military populations; 21 2) it is associated with psychological trauma exposure—a key feature of military work; and 3) its impact may be greater given the physically and psychologically demanding nature of military work. However, research on GAD in military populations is limited. In the US, GAD was the second-most common past 30-day internalizing disorder among non-deployed soldiers. 22 In addition, the prevalence of GAD (12.0%) and PTSD (12.1%) were remarkably similar in a treatment-seeking sample of US veterans, with both disorders evidencing similar levels of impairment. 14 Existing research into GAD among military and veteran populations has confirmed functional impairments in multiple domains, 14,22,23 poorer psychological well-being, 14 comorbidity with physical health conditions, 24 –27 greater medication use, 14 sleep difficulties, 28 and suicidality. 29 –31 These findings on GAD in the military thus mirror those in the general population.
Other recent research has pointed to potential differences in the phenomenology of GAD in military personnel and civilians. Military personnel in both Canada 32 and the US 22,33 (but not Australia) 34 have a higher prevalence of GAD than comparable civilian populations. In Canada, the prevalence of past-year GAD has increased among Regular Force personnel in recent years, from 1.9% in 2002 to 4.7% in 2013. 35 There is also a paucity of research on symptom profiles and correlates of GAD in military populations. 23 Given the unique characteristics of the military environment (e.g., deployment, separation from family, reintegration issues, combat exposure), there may be important differences in the clinical presentation of GAD between military personnel and civilians. For example, there appears to be differences in the age of GAD onset between military personnel and civilians, with the proportion of individuals with pre-enlistment onset much greater in the military than among civilians. 25 There are also differences in the pattern and extent of common GAD comorbidities in military compared with civilian populations. 25,32,34 Conceptually, we might also expect differences in the nature of GAD-specific worries; for example, worries surrounding military-specific duties, continued occupational fitness, and time spent away from family are all key features of military life. Symptomatology may also differ, 36 –38 and these differences may be important given the observed differences in the impact of symptoms. 39
Past research on the epidemiology of GAD among military personnel as a sole focus is confined to a single paper that used 2002 data; 23 this is a key limitation, as it gives an incomplete and dated picture of an important disorder. Most other research on GAD in the military uses older veterans 14,24 –27 or data collected before involvement in the sustained military efforts in Iraq and Afghanistan. 23,31,40 Another important limitation of past research is that almost none of the literature on GAD in the military includes direct comparisons to the general population, making it difficult to place military findings in perspective. Past military–civilian comparisons included the use of non-comparable survey data; 25 failed to adjust for characteristics, other than age, sex, and employment status; 34 had a low response rate; 25,34 and failed to make any adjustments for comorbid disorders. 25,32,34
We thus address important limitations of past research on GAD in the military by offering this first, in depth, exploratory look at the clinical epidemiology of GAD in contemporary military personnel, and we will place those findings in perspective by comparing key features of the disorder in military personnel relative to the general population. The objectives of this study were to: 1) compare sociodemographic characteristics and co-morbid mental disorders associated with GAD in the Canadian Armed Forces (CAF) Regular Force personnel and the Canadian general population (CGP); 2) examine differences in the type of worries and symptom presentations of GAD in the CAF and CGP; and 3) examine differences in the extent of functional impairment associated with GAD in the 2 populations.
Methods
Data and Sample
Data were from 2 nationally representative surveys collected by Statistics Canada: 1) the Canadian Community Health Survey–Mental Health (CCHS-MH), collected in 2012 (N = 25,113; response rate = 68.9%), and 2) the Canadian Forces Mental Health Survey (CFMHS), collected in 2013 (N = 8,161; response rate = 79.8%). The CCHS-MH included a representative sample of Canadians aged 15 y and older living in the 10 provinces. Analyses were restricted to respondents aged 18 to 60 y to maintain age comparability across the populations (N = 15,981 in the CCHS-MH in final sample). The CFMHS included a representative sample of Regular Force military personnel (n = 6,692) and a subsample of Reserve Force personnel, who had deployed in support of the mission in Afghanistan (n = 1,469). Reservists who had not deployed in support of the mission to Afghanistan were not included in the sampling frame, thus only serving CAF Regular Force personnel were included in the analyses (i.e., Reserve Force personnel were excluded from this study). In both surveys, data were collected in-person by trained lay interviewers using computer-assisted interviewing techniques. The 2 surveys used similar methods (e.g., data collection procedures) and measures (e.g., overlapping core content), and were designed to allow for comparisons across surveys. All variables in this study were assessed using identical items and measures included in both surveys. Participation was voluntary, and written informed consent was obtained. Further details of the CCHS-MH 41 and the CFMHS 42 have been published elsewhere.
Measures
Generalized anxiety disorder
Past-year GAD was assessed using the World Health Organization’s version of the International Composite Diagnostic Interview (WHO-CIDI) 43 based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) 1 criteria. Clinical features of GAD included content area of worry (e.g., finances, relationships at work, mental and physical health) and symptoms endorsed (i.e., restlessness, irritability, difficulty concentrating, trouble sleeping, fatigue, sad or depressed, tense muscles, heart racing, sweat often, dry mouth, and trembles or shakes).
Functional impairments
Functional impairments associated with GAD were assessed with the Sheehan Disability Scale. 44 Respondents were asked to rate the extent to which their feelings of anxiousness, worry, or nervousness interfered with their ability to function on a scale from 0 (no interference) to 10 (very severe interference) across 5 separate domains: home, school, work, close relationships, and social life.
Comorbid mental disorders
Diagnoses of comorbid past-year mental disorders were assessed with the WHO-CIDI 43 and based on DSM-IV criteria. 1 Past-year mental disorders assessed in both surveys included major depressive episode (MDE) and alcohol abuse or dependence. The CFMHS also included WHO-CIDI–based assessments of past-year panic disorder and past-year PTSD. Comparable measures of panic disorder and PTSD were not included in the CCHS-MH survey.
Sociodemographic covariates
Sociodemographic covariates included sex, age, visible minority status, marital status, highest level of education, and past-year household income. Military-specific covariates included military rank (i.e., junior non-commissioned member (NCM), senior NCM, and officer) and military environment (i.e., Army, Navy, or Air Force).
Statistical Analyses
Final probability weights computed by Statistics Canada were applied to the data to ensure they were representative of the CGP and CAF Regular Force personnel. Final weights adjust for unequal selection probabilities, non-response, extreme values, and the exclusion of out-of-scope units. 8,41 Variance estimation was done with bootstrap methods, using 500 replicate weights supplied by Statistics Canada. Differences across the 2 surveys were tested in a merged dataset. In the merged dataset, both populations are treated as independent samples. That is, when the 2 populations were combined into the same dataset, final weights and bootstrap weights were applied in the same way as if they would be in independent datasets.
First, cross-tabulations were used to compute the prevalence of lifetime and past-year GAD in the CAF and CGP. Multivariate logistic regression models were computed to examine differences in the prevalence of GAD across populations. Models adjusted for sociodemographic covariates (i.e., sex, age, visible minority status, marital status, education, and past-year household income). Second, cross-tabulations and logistic regressions were used to examine the association of sociodemographic covariates with past-year GAD. Third, cross-tabulations were used to compute prevalence estimates for comorbid mental disorders and the types of worries and symptoms of GAD endorsed among respondents with past-year GAD. Multivariable logistic regressions were used to examine differences in comorbid mental disorders and the types of worries and symptoms of GAD endorsed across populations. Models examining comorbid mental conditions adjusted for sociodemographic covariates. Models examining types of worries and GAD symptoms adjusted for sociodemographic covariates and comorbid mental disorders (i.e., MDE and alcohol abuse/dependence). Finally, we calculated estimated marginal means for the total level of impairment across domains by computing coefficients derived from a linear regression model adjusted for sociodemographic variables. We calculated differences in estimated marginal means across the surveys using these coefficients.
Results
The prevalence of lifetime and past-year GAD was significantly higher in the CAF (12.1% and 4.7%, respectively) compared to the CGP (9.5% and 3.0%, respectively), after adjusting for sociodemographic covariates (adjusted odds ratios [AOR] for lifetime = 1.79, 95% confidence interval [CI] = 1.55 to 2.07; AOR for past-year = 2.23, 95% CI = 1.80 to 2.78). Relationships between sociodemographic covariates and past-year GAD are provided in Table 1. In both the CAF and the CGP, women (v. men) and individuals who were separated, divorced, or widowed (v. married/common-law) had increased odds of meeting diagnostic criteria for past-year GAD. Visible minority status, higher education (university degree v. high school or less), and higher total household income were associated with significantly decreased odds of GAD in both populations. In the CAF, increasing age was associated with increased odds of GAD. In the CGP, single marital status (v. married/common-law) was associated with significantly increased odds of GAD. Neither military rank nor military element were significantly associated with GAD in the CAF.
Sociodemographic Covariates, Military Covariates, and Comorbid Mental Disorders by Past-year Generalized Anxiety Disorder in the Canadian Armed Forces and the Canadian General Population.
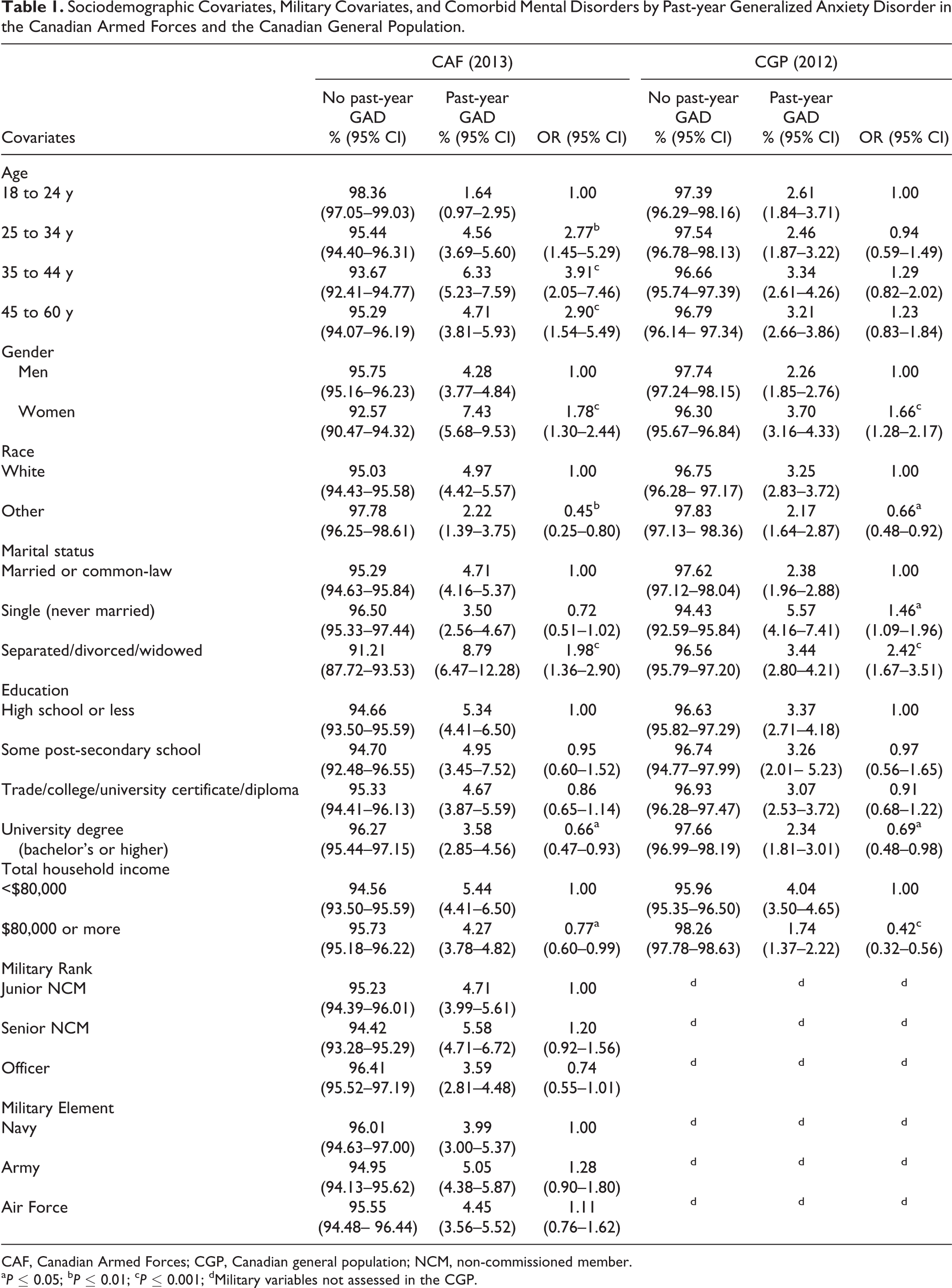
CAF, Canadian Armed Forces; CGP, Canadian general population; NCM, non-commissioned member.
aP ≤ 0.05; bP ≤ 0.01; cP ≤ 0.001; dMilitary variables not assessed in the CGP.
Relationships between past-year GAD and comorbid mental disorders are provided in Table 2. GAD was highly comorbid with other mental disorders in both the CAF (AORs ranged from 5.17 to 19.01) and CGP (AORs ranged from 3.99 to 26.86). In both populations, among those with past-year GAD, approximately 55% also met diagnostic criteria for MDE and between 10% and 15% also met diagnostic criteria for alcohol abuse/dependence. A direct comparison of comorbidity patterns between the 2 populations indicated that the pattern of comorbidity was similar for both MDE (AOR = 1.40, 95% CI = 0.84 to 2.32) and alcohol abuse/dependence (AOR = 0.91, 95% CI = 0.39 to 2.15). In the CAF, among those with past-year GAD, 19.8% also met diagnostic criteria for panic disorder and 38.4% also met diagnostic criteria for PTSD (comparable measures of these disorders were not included in the CCHS-MH).
Association of Generalized Anxiety Disorder and Comorbid Mental Disorders in the Canadian Armed Forces and the Canadian General Population.
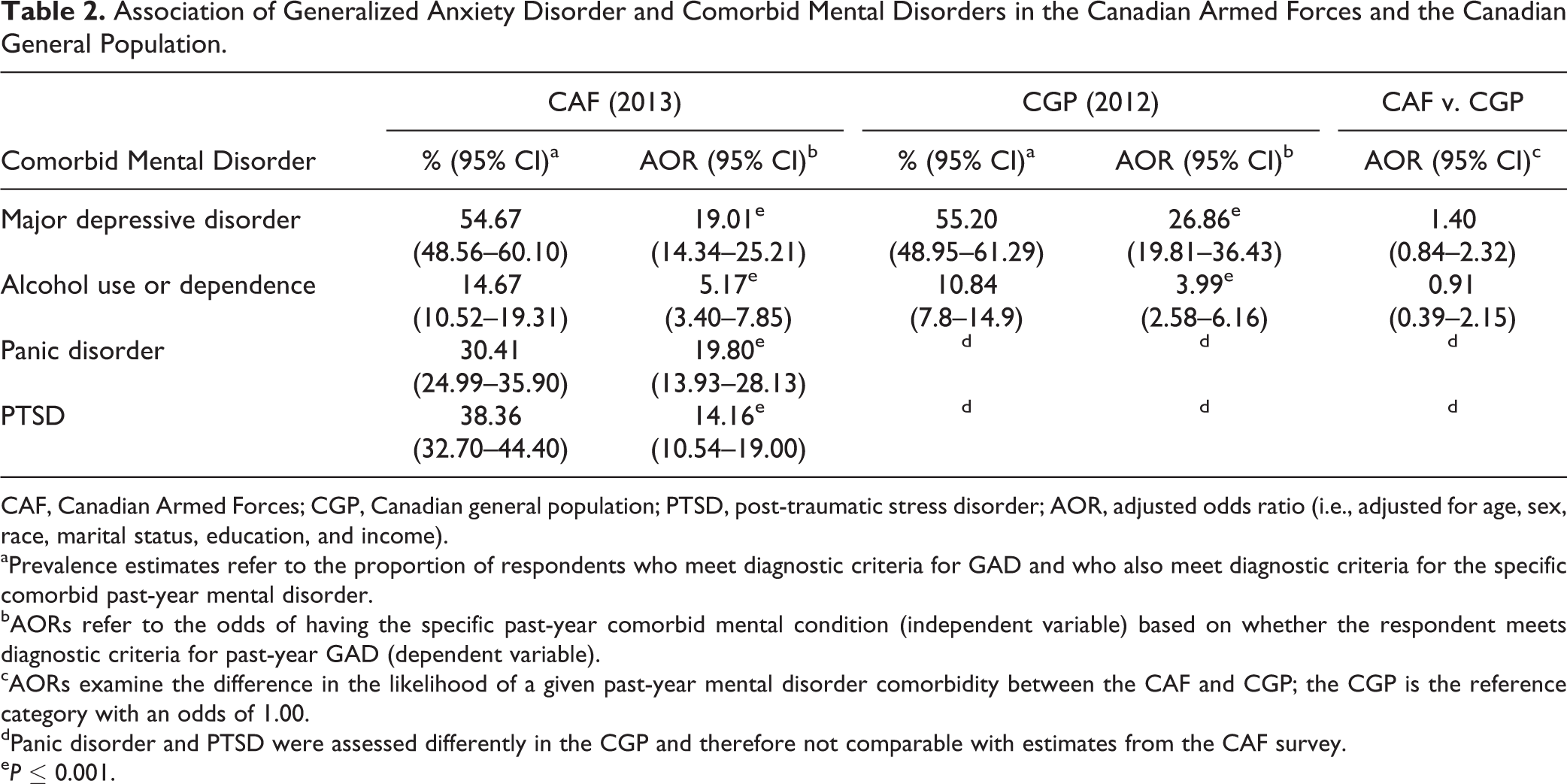
CAF, Canadian Armed Forces; CGP, Canadian general population; PTSD, post-traumatic stress disorder; AOR, adjusted odds ratio (i.e., adjusted for age, sex, race, marital status, education, and income).
aPrevalence estimates refer to the proportion of respondents who meet diagnostic criteria for GAD and who also meet diagnostic criteria for the specific comorbid past-year mental disorder.
bAORs refer to the odds of having the specific past-year comorbid mental condition (independent variable) based on whether the respondent meets diagnostic criteria for past-year GAD (dependent variable).
cAORs examine the difference in the likelihood of a given past-year mental disorder comorbidity between the CAF and CGP; the CGP is the reference category with an odds of 1.00.
dPanic disorder and PTSD were assessed differently in the CGP and therefore not comparable with estimates from the CAF survey.
eP ≤ 0.001.
Table 3 provides information on the content area of worry among CAF personnel and the CGP who met diagnostic criteria for past-year GAD. The most frequently endorsed worries among CAF personnel included being worried about their own mental health (66.7%), love life (65.3%), finances (63.3%), success at school or work (60.7%), and relationships with family (54.0%). Similarly, the most frequently endorsed worries in the CGP included being worried about finances (67.3%), their own mental health (52.0%), relationships with family (50.5%), love life (48.0%), and their own physical health (47.2%). A direct comparison of the content areas of worry between the 2 populations indicated that, after adjusting for sociodemographic covariates and comorbid MDE and alcohol abuse/dependence, CAF personnel were significantly more likely to be worried about success at school or work (AOR = 2.13, 95% CI = 1.23 to 3.71), their social life (AOR = 1.72, 95% CI = 1.01 to 2.91), their own mental health (AOR = 1.97, 95% CI = 1.10 to 3.51), being away from home or apart from loved ones (AOR = 2.40, 95% CI = 1.37 to 4.20), war or revolution (AOR = 3.55, 95% CI = 1.55 to 8.13), or other factors (AOR = 5.93, 95% CI = 1.58 to 22.24) .
Content Area of Worry among Canadian Military Personnel and the Canadian General Population Meeting Diagnostic Criteria for Past-year Generalized Anxiety Disorder.
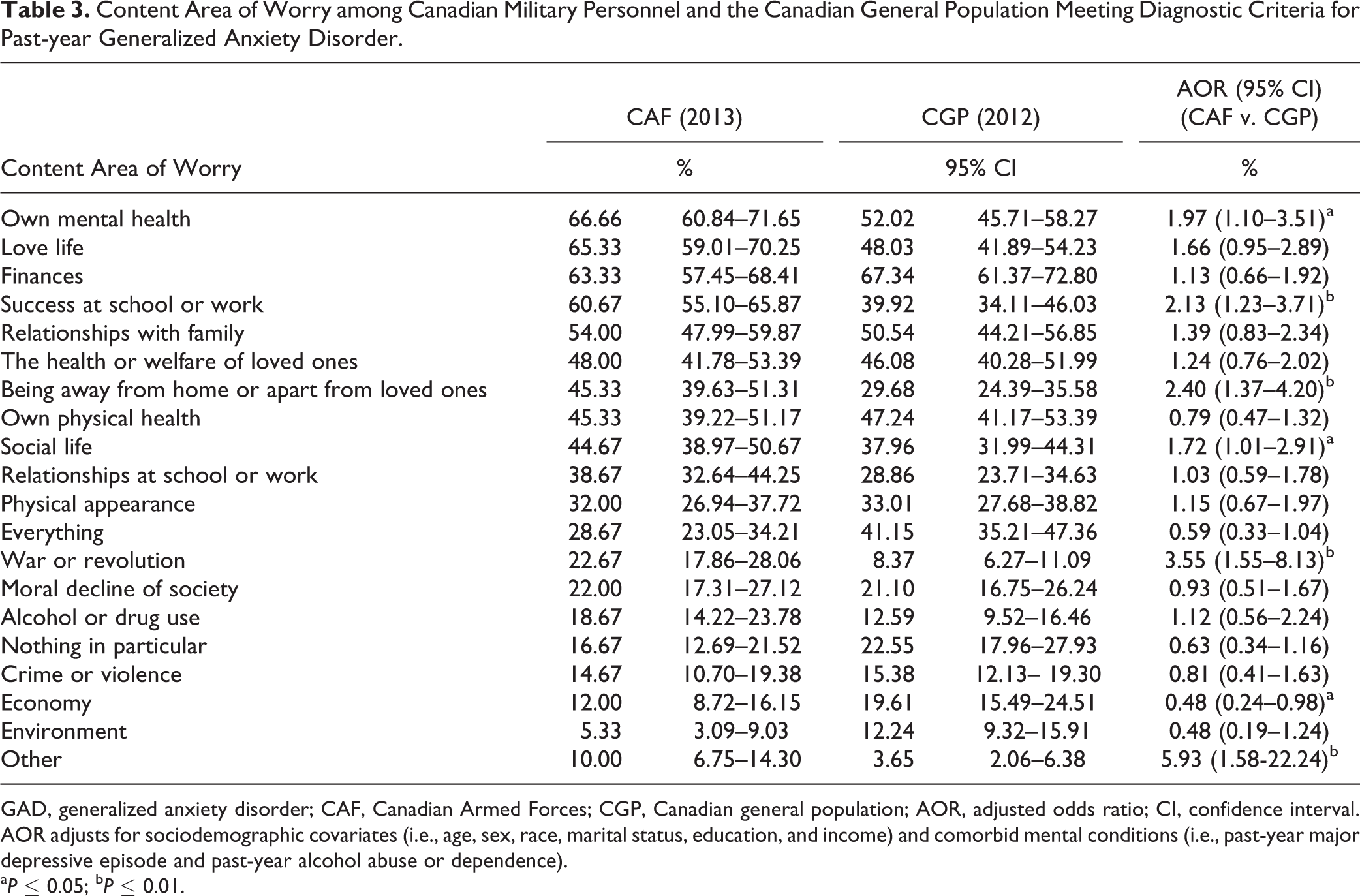
GAD, generalized anxiety disorder; CAF, Canadian Armed Forces; CGP, Canadian general population; AOR, adjusted odds ratio; CI, confidence interval. AOR adjusts for sociodemographic covariates (i.e., age, sex, race, marital status, education, and income) and comorbid mental conditions (i.e., past-year major depressive episode and past-year alcohol abuse or dependence).
aP ≤ 0.05; bP ≤ 0.01.
Table 4 provides information on GAD symptoms endorsed in the CAF and CGP groups. A similar pattern of symptoms was found in the 2 populations. The most frequently endorsed symptoms of GAD in both groups included having difficulty concentrating; being restless, keyed up, or on edge; getting tired easily; being more irritable than usual; and having trouble sleeping or staying asleep (prevalence estimates ranged from 87.3% to 95.3% in the CAF, and from 85.6% to 91.9% in the CGP). A direct comparison of GAD symptoms endorsed between the 2 populations indicated that CAF personnel with GAD were significantly more likely to report being restless, keyed up, or on edge (AOR = 3.18, 95% CI = 1.26 to 8.05) and to be more irritable than usual (AOR = 2.47, 95% CI = 1.08 to 5.66) than CGP respondents with GAD (again, after adjusting for sociodemographic covariates and comorbid MDE and alcohol abuse/dependence).
Symptoms of Generalized Anxiety Disorder among Canadian Military Personnel and the Canadian General Population Meeting Diagnostic Criteria for Past-year Generalized Anxiety Disorder.
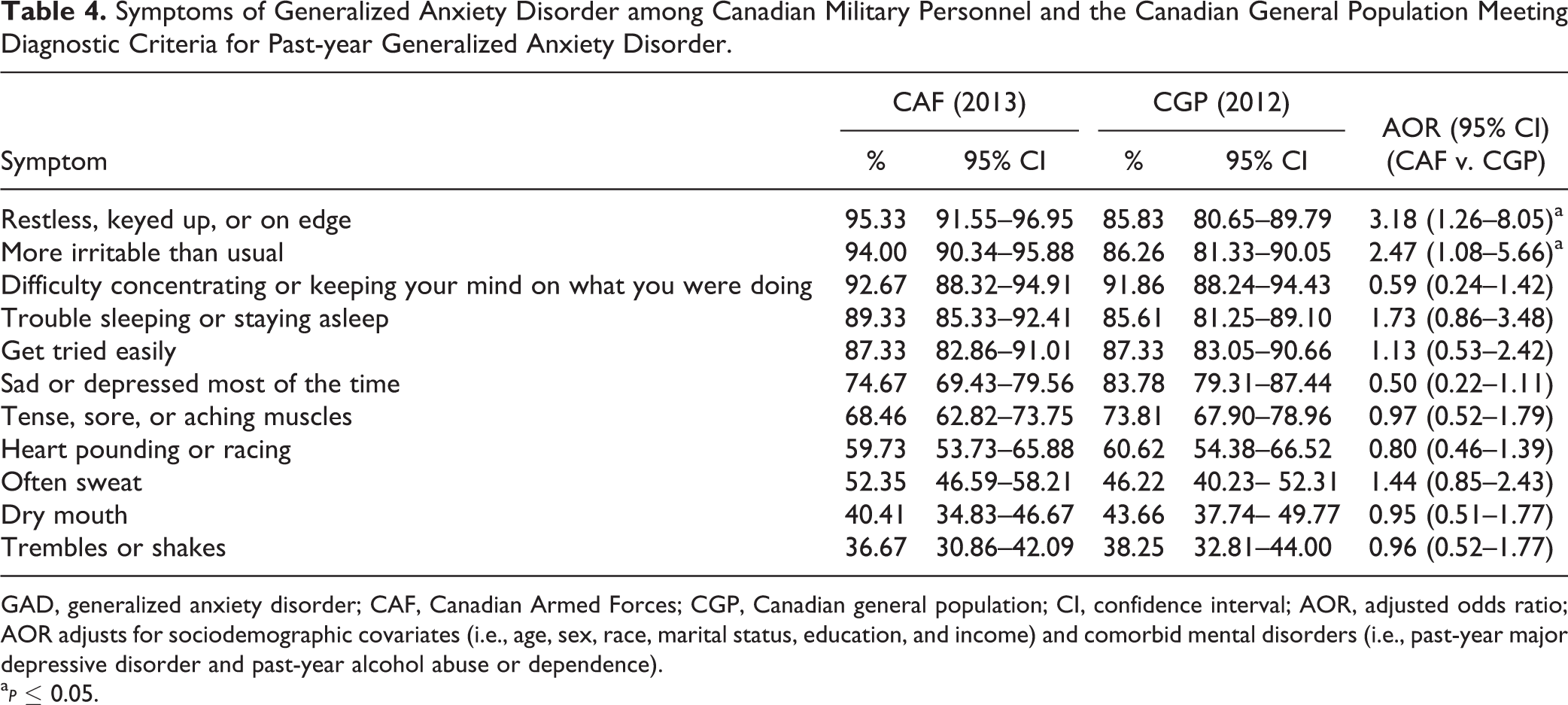
GAD, generalized anxiety disorder; CAF, Canadian Armed Forces; CGP, Canadian general population; CI, confidence interval; AOR, adjusted odds ratio; AOR adjusts for sociodemographic covariates (i.e., age, sex, race, marital status, education, and income) and comorbid mental disorders (i.e., past-year major depressive disorder and past-year alcohol abuse or dependence).
a
Table 5 provides information on the level of functional impairment associated with GAD across domains. Similar mean levels of functional impairment were reported in both the CAF and CGP groups across school, work, relationship, and social life functional domains. A direct comparison of the mean level of functional impairment between the 2 populations indicated that CAF personnel with GAD endorsed significantly higher interference scores at home as compared with CGP respondents with GAD, after adjusting for sociodemographic covariates.
Functional Impairment Associated With Past-year Generalized Anxiety Disorder among Canadian Military Personnel and Canadian General Population.
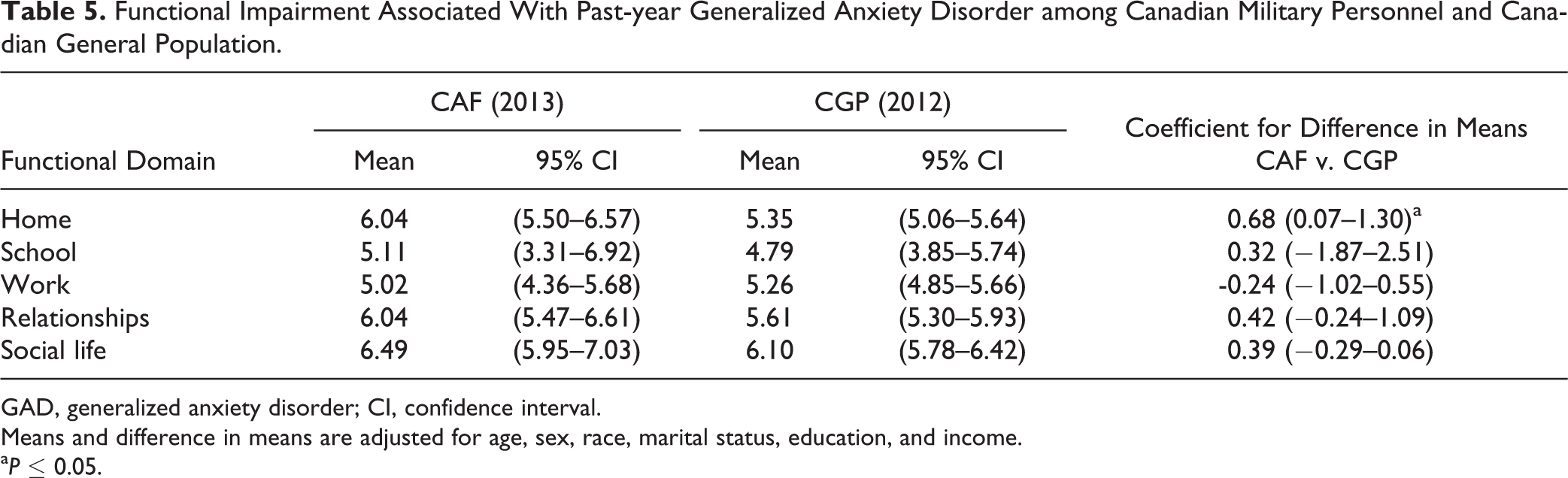
GAD, generalized anxiety disorder; CI, confidence interval.
Means and difference in means are adjusted for age, sex, race, marital status, education, and income.
aP ≤ 0.05.
Discussion
There are several novel findings in this study. First, the prevalence of lifetime and past-year GAD was significantly higher among CAF personnel (12.1% and 4.7%, respectively) than CGP respondents (9.5% and 3.0%, respectively). Lifetime and past-year prevalence estimates of GAD in the CGP differ from other studies using CCHS-MH data 8,45 (i.e., 8.7% and 2.6%, respectively) due to slight differences in the samples used to compute estimates. The current study only included respondents aged 18 to 60 y, whereas other studies using CCHS-MH data included all respondents 15 y and older (including respondents over the age of 60 y). Second, sociodemographic covariates and comorbid mental disorders were largely associated with GAD in the same way for military personnel and civilians. Third, although the content area of worries and GAD symptoms endorsed were similar among military personnel and civilians with past-year GAD, CAF personnel were significantly more likely to endorse specific types of worries (i.e., worried about success at school or work, social life, own mental health, being away from home or apart from loved ones, and war or revolution), and to endorse specific symptoms of GAD (i.e., restless, keyed up, or on edge; and more irritable than usual) than their civilian counterparts. Finally, CAF personnel with past-year GAD reported significantly higher functional impairment at home than civilians with past-year GAD.
In this study, the prevalence of lifetime and past-year GAD was significantly higher in the CAF group than in the CGP group. This is similar to findings from the US, where new soldiers in the US Army evidenced a higher lifetime prevalence of GAD as compared with a civilian sample. 33 Thus, the higher prevalence of past-year GAD among CAF personnel could be due to a higher lifetime prevalence of GAD with pre-enlistment onset. However, there is also evidence that the prevalence of past-year GAD has increased among CAF Regular Force personnel from 2002 to 2013. 35 Research from both Canada and the US also indicates that the prevalence of GAD is slightly higher after deployment to Iraq or Afghanistan. 46,47 Given the known association between trauma and GAD in many populations, and the increase in combat exposure in CAF personnel since 2002, 48 trauma exposure related to the mission in Afghanistan could, in part, contribute to the increase in GAD prevalence over time.
In general, sociodemographic covariates associated with past-year GAD were similar in both the CAF and CGP groups. Similar to previous research, women 4,5,7,8,10,16,22,23,46,49 and separated, divorced, and widowed individuals 5,8,23,25,46 were more likely to meet diagnostic criteria for past-year GAD than men and individuals in marital or common-law relationships in both populations. As well, as with other findings, visible minority status, 5,46 higher education, 49 and higher total household income 4,5,8,25 were associated with decreased odds of past-year GAD in both the CAF and CGP groups. One notable difference between the populations was the association between past-year GAD and age. Among CAF personnel, but not CGP respondents, increasing age was associated with increased odds of meeting diagnostic criteria for past-year GAD. These findings are inconsistent with previous studies that found younger age to be associated with an increased risk of GAD among both active military personnel 49 and veterans 25,28 in the US. In addition, age was not significantly associated with past-year GAD among CAF personnel in 2002. 23
In this study, and consistent with previous research, 2,4 –6,8 –14,23,24 comorbid mental disorders were strongly associated with past-year GAD in both the CAF and CGP groups. There is substantial overlap in DSM-IV criteria for diagnosis of GAD and other mental disorders, particularly MDE. 4,11 Further, GAD is characterized as constant, uncontrollable worry (i.e., similar to PTSD symptoms of arousal and re-experiencing) associated with a wide range of typically non-traumatic stressors. 14 Symptom overlap could help to explain the high comorbidity between GAD and other mental disorders reported in this study and elsewhere. Another potential explanation is the inability to distinguish between generalized anxiety related to PTSD v. “true GAD,” because of limitations in the WHO-CIDI 43 and in a population with a substantial (and increasing) burden of PTSD.
The most frequently endorsed types of worry were similar among military personnel and civilians. In both CAF and CGP groups, worries about finances, mental health, love life, and relationships with family were most frequently endorsed. The most commonly reported symptoms of past-year GAD were also similar in the CAF and CGP groups, and included having difficulty concentrating; being restless, keyed up, or on edge; getting tired easily; being more irritable than usual; and having trouble sleeping or staying asleep. The most notable findings, however, were that CAF personnel were significantly more likely to endorse specific types of worries (i.e., worried about success at school or work, social life, own mental health, being away from home or apart from loved ones, and war or revolution), and specific GAD symptoms (i.e., being restless, keyed up, or on edge; and being more irritable than usual) even after adjusting for sociodemographic covariates and comorbid MDE and alcohol abuse/dependence. CAF personnel also reported higher mean levels of functional impairment at home after adjusting for sociodemographic covariates.
CAF personnel with past-year GAD were also significantly more likely to endorse being restless, keyed up, or on edge, and being more irritable than usual than civilians with past-year GAD, even after adjusting for sociodemographic covariates and comorbid MDE and alcohol abuse/dependence. The finding that CAF personnel were significantly more likely to report these specific symptoms than civilians may be related to symptom overlap between DSM-IV diagnoses of GAD and PTSD. Specifically, being restless, keyed up, and on edge is similar to PTSD symptoms of hypervigilance and exaggerated startle response. 1 In addition, being more irritable than usual in GAD maps to the PTSD symptom of irritable behavior and angry outbursts. 1 We did not account for comorbid PTSD diagnoses in CAF and CGP comparisons, as PTSD was not assessed in the CCHS-MH survey. Research on the distinguishing features of GAD, PTSD, and other mental disorders among CAF personnel remains an important priority.
The strengths of this study include the use of contemporary, representative samples for the 2 groups. The 2 surveys used similar methods and measures, which allows for comparisons between the study populations. However, findings from the current study need to be viewed considering several limitations. First, the data are cross-sectional, making inferences about causality impossible. Second, the data are retrospective and self-reported, which introduces potential recall and same-source bias. Third, only a limited number of mental disorders were assessed in both surveys. Importantly, PTSD was not assessed in CCHS-MH. Further, although the WHO-CIDI algorithm applies DSM-IV criterion D, which requires that the excessive worry not occur exclusively in the context of another Axis I disorder, the requirement that worry not occur exclusively during PTSD is not implemented in the WHO-CIDI. Therefore, GAD detected in the survey may not, in fact, be something clinicians would diagnose as such. Research examining the incidence of diagnosed GAD in the military personnel is another important target for future research. Fourth, the general population sample was not restricted to those who were employed full-time, which may have conflated a general employment effect with a specific occupation effect (as all military personnel were employed full-time by the CAF). Finally, findings are not generalizable to CAF Reserve Force personnel or the Canadian veteran population.
GAD is a substantial public health concern associated with significant impairment and disability in both military and civilian populations. 3,5 The focus on depression in the general population and PTSD in military populations may underestimate the total burden of mental health problems. 3,14,27 Clinicians need to recognize that the clinical presentation of GAD, including content area of worries and symptom presentation, may be different in military personnel than among civilians.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Preparation of this article was supported by a Canadian Institutes of Health Research (CIHR) New Investigator Award (Afifi), CIHR Foundations Scheme Grant 333298 (Afifi), and CIHR Foundation Scheme Grant 333252 (Sareen). Funding for this article was supported by a Research Contract from the Government of Canada.