
Abstract
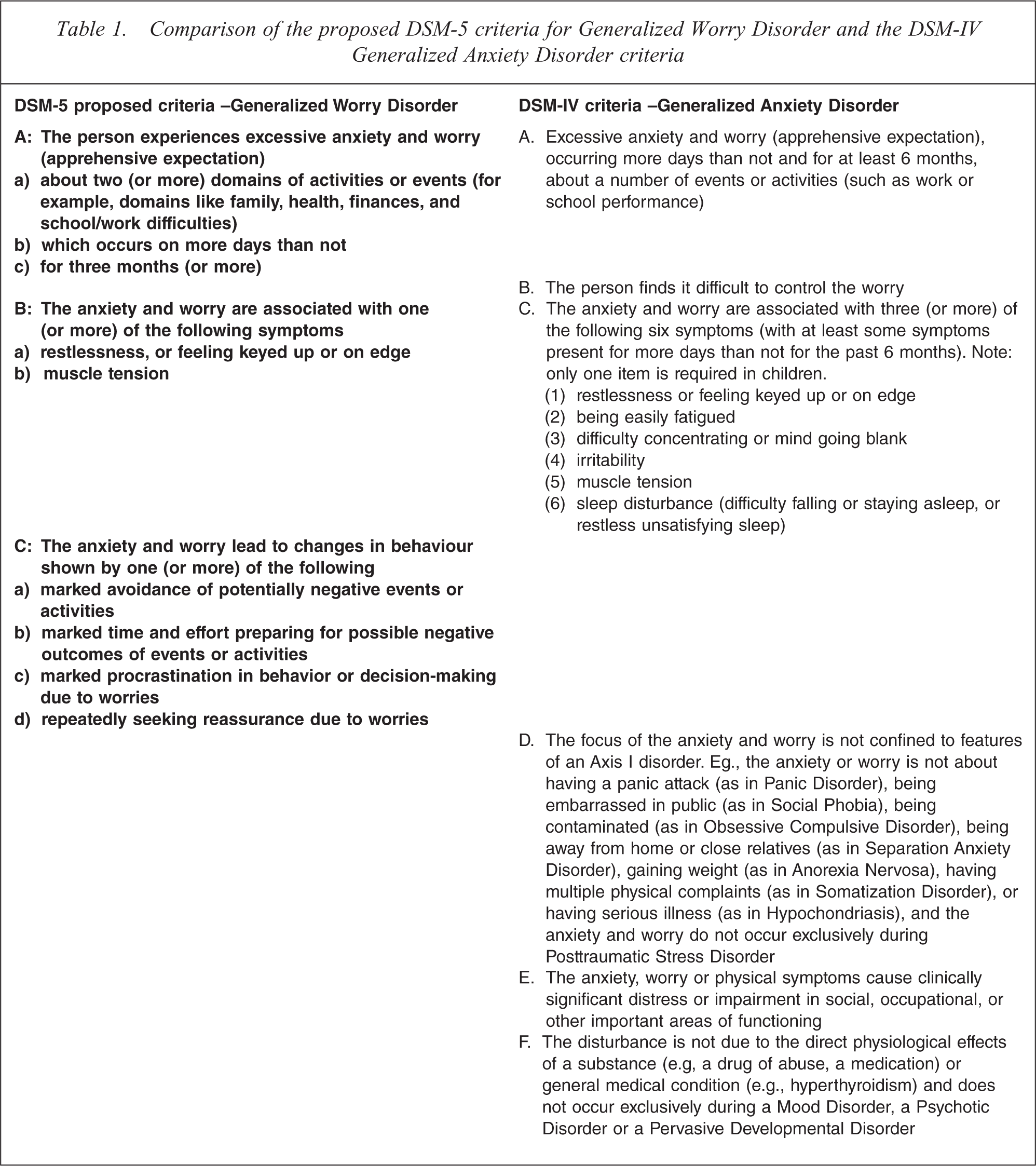
Options to revise the DSM-IV Generalized Anxiety Disorder (GAD) criteria have been made as part of the DSM-5 process [1]. These were based on extensive literature reviews, secondary analyses of existing data sets, and consultations within the Anxiety, Obsessive-Compulsive, Post-traumatic and Dissociative Disorders Work Group. In their review, Andrews, Hobbs, Borkovec et al. [1] proposed that the DSM-IV duration threshold be reduced to 3 months to reflect the risk and clinical factors that are shared by patients who experience all of the DSM-IV GAD symptoms and those patients who experience GAD symptoms but who do not meet the 6 month duration threshold [2, 3]. The difficult-to-control criterion was proposed for deletion as a result of its overlap with the ‘excessive’ criterion. For instance, only 4% of worriers report that their worry is excessive but still controllable (Beesdo et al. unpublished data, 2010). In addition, it was proposed that the associated symptoms criterion be altered to reflect the concomitants of worry that are specific to the GAD diagnosis, and that a behavioural criterion be introduced to the classification. No recommendations were made with respect to the DSM-IV criteria D and F due to scarcity of data. Moreover, as a result of the ongoing work of the DSM-5 Impairment Work Group, the GAD review did not make proposals with respect to criterion E. The authors concluded that renaming the diagnosis “Generalized Worry Disorder” could clarify the core feature of the disorder: clinically significant worry that is generalized to multiple facets of patients’ lives. The DSM-IV and the proposed DSM-5 GAD criteria are shown in Table 1.
Comparison of the proposed DSM-5 criteria for Generalized Worry Disorder and the DSM-IV Generalized Anxiety Disorder criteria
There is public interest in whether the proposed DSM-5 criteria will lead to people who have mild conditions being identified as disordered and in need of treatment. This is the first study to examine the effect of the suggested changes to the A, B and C criteria and the possible effect of omitting the clinical significance criterion on the prevalence of GAD, and the level of distress and disability of the new cases. Evidence from both population and clinical samples are used.
Study 1: The effect of modifying DSM-IV diagnostic criteria on the prevalence of GAD in a population sample
Methods
Sample
Respondents of the 2007 Australian National Survey of Mental Health and Well Being who had sought treatment from a medical doctor or other health professional about their worry, anxiety and/or nervousness at some time in their lives were included in this study. This representative population survey was conducted by the Australian Bureau of Statistics, a federal government statutory authority between August and December 2007. During that period, trained lay-assessors interviewed 8,841 Australians aged between 16 and 85 who lived in private housing about their physical and mental wellbeing (response rate 60%). All respondents gave their informed consent to be interviewed. The stratified multi-stage sampling procedures used in this survey are detailed elsewhere [4].
Diagnostic Assessment
Respondents were interviewed about their lifetime experience of DSM-IV-defined GAD symptoms using a modified version of the World Mental Health-Composite International Diagnostic Interview (WMH-CIDI v3.0) [5]. As a result of the interview structure, all respondents included here had experienced a period in their life when they were a worrier; when they had been much more nervous or anxious than most people, or a period of 1 month or more when they were anxious and worried most days. Respondents also reported experiencing multiple worries for at least 1 month and that their symptoms were clinically significant. Respondents were excluded from the study if their anxiety was confined to the focus of another Axis I disorder or their anxiety had always resulted from physical or drug causes. It was not possible to apply the exclusion hierarchies for pervasive development or psychotic disorders.
Analyses
The DSM-IV GAD criteria were manipulated one, two and three at a time to create the possible DSM-5 diagnostic variables. It was not possible to examine the effect of the proposed behavioural criteria on the prevalence of GAD in this existing dataset which used an interview based strictly on DSM-IV criteria. Given the ongoing revision process, it is nonetheless important to examine the extent of change that could occur if a restricted number of the criteria proposals were accepted for DSM-5 GAD. The lifetime prevalence estimates, diagnostic efficiency indices (e.g., sensitivity, specificity, area under the curve (AUC) and Kappa) and the associated distress and impairment of the different ways of defining GAD were examined [6]. Balanced repeated replication estimation procedures were implemented in SAS/SUDAAN to account for the complex survey design and to provide the standard errors of the prevalence estimates.
Results
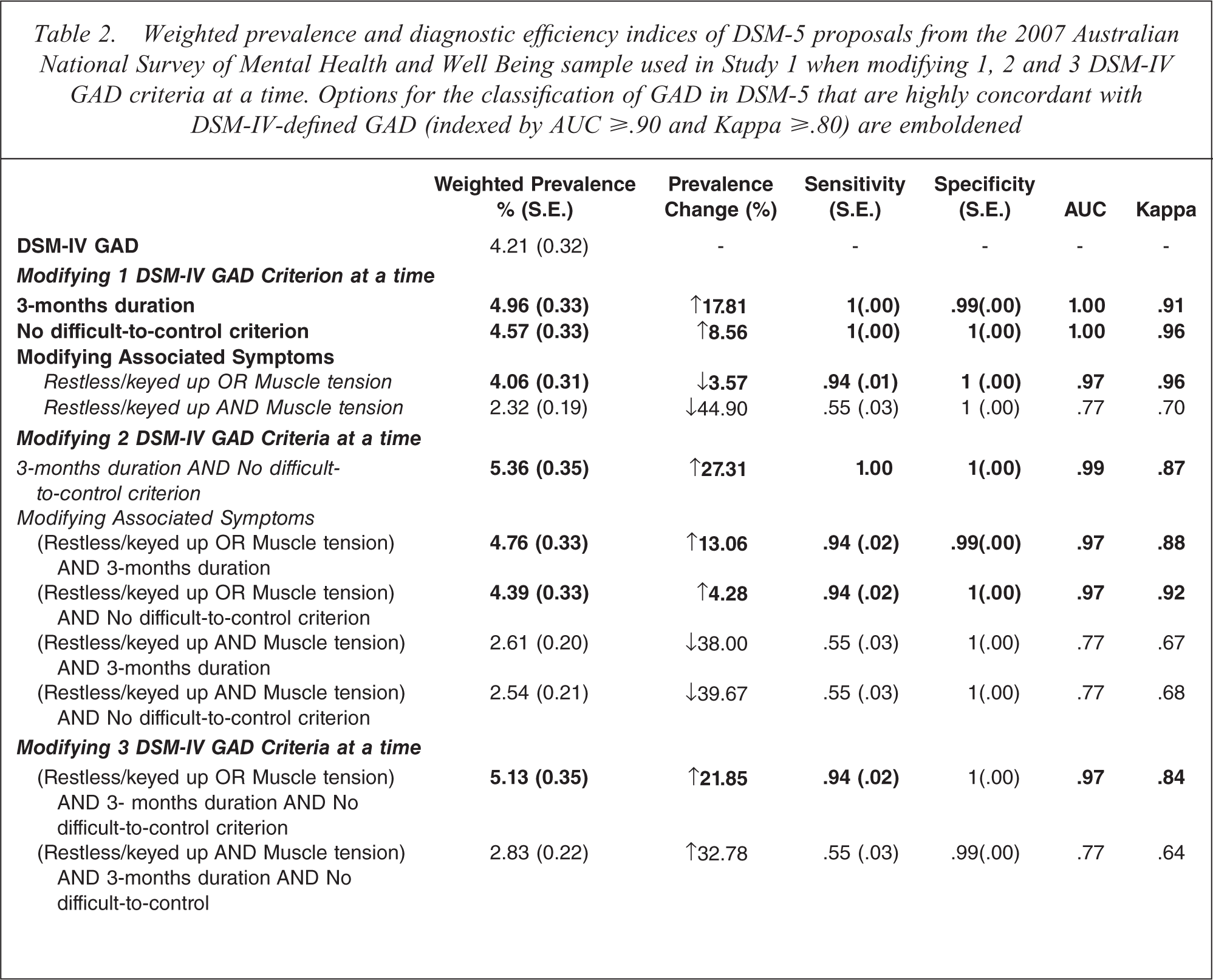
The weighted lifetime prevalence estimates and diagnostic efficiency indices of the different ways of defining GAD in DSM-5 are provided in Table 2. Seven of the 11 diagnostic variables had excellent concordance with DSM-IV-defined GAD (kappas ≥ .80 and AUC values ≥ .90). These 7 changes to the definition of GAD changed the prevalence of DSM-IV-defined GAD by −4% to +27%. The closest approximation of the proposed DSM-5 criteria (clinically significant excessive worry about multiple everyday events that is experienced for 3 months (or more) and with either/or both feelings of restlessness, keyed up or on edge and muscle tension) increased the prevalence of GAD by 22% (AUC = 0.97, Kappa = 0.84).
Weighted prevalence and diagnostic efficiency indices of DSM-5 proposals from the 2007 Australian National Survey of Mental Health and Well Being sample used in Study 1 when modifying 1, 2 and 3 DSM-IV GAD criteria at a time. Options for the classification of GAD in DSM-5 that are highly concordant with DSM-IV-defined GAD (indexed by AUC ≥.90 and Kappa ≥.80) are emboldened
Study 2: The effect of modifying DSM-IV criteria on the prevalence and severity of GAD in a clinical sample
We extended the findings of the first study to a clinical sample that allowed us to explore the effect of adding the proposed behavioural criteria and deleting the clinical significance criterion.
Methods
Sample
The clinical sample were 186 patients who were accepted for online cognitive behavioural treatment for their anxiety and/or depression. Patients were being recruited for three randomized controlled trials that were advertised on national radio (125 patients applied for a GAD trial, 35 for a Major Depression trial and 26 for a transdiagnostic anxiety trial). The demographics of these volunteers paralleled the treatment seeking population sample used in the preceding study but they were still very much a sample of convenience. The sample was predominantly female (69%), married or in a de facto relationship (57%), middle aged (M (S.D.) = 45(12.42)), and 79% had previous psychiatric treatment.
Diagnostic Assessment
Patients’ were interviewed via telephone by a registered psychologist/psychiatrist (56%) or by a trained psychology honours graduate (44%) using a modified version of the WMH-CIDI v3.0 to encompass both the DSM-IV and the new DSM-5 symptoms (additional interview items are available upon request). This proceeded from the standard diagnostic intake procedures used by this battery of online treatment programs [7].
Respondents’ total WHO-DAS2.0 and K-10 scores were used as indices of the functional impairment and emotional distress associated with their current GAD symptoms [8], [9]. All patients completed the K-10 and the 160 patients included in the GAD and MDD treatment programs also completed the WHO-DAS2.0. Patients in the transdiagnostic trial did not complete the latter measure.
Analyses
The prevalence and clinical significance of patients’ GAD symptoms, and the concordance between DSM-IV and the proposed DSM-5 classifications were calculated when manipulating 1 criterion at a time and also for the full DSM-5 proposals (3 months or more of excessive generalized worry with 1 from 2 associated symptoms, and 1 from 3 behaviours with and without the clinical significance criterion). The effect of the clinical significance criterion could not be examined in Study 1 as a result of the embedded skips in the survey interview, such that all respondents had to report that they had experienced some distress or impairment prior to being asked about their psychiatric service use.
Respondents were assigned to a diagnostic group for comparison based on whether they met DSM-IV GAD criteria, or did not meet DSM-IV criteria but would meet criteria for DSM-5 criteria. Separate multinomial logistic regressions were then conducted for patients’ K-10 and WHODAS2.0 scores for each DSM-5 diagnostic variable that had strong concordance with DSM-IV-defined GAD, and also for the DSM-5 propsal when the clinical significance criterion was omitted.
Results
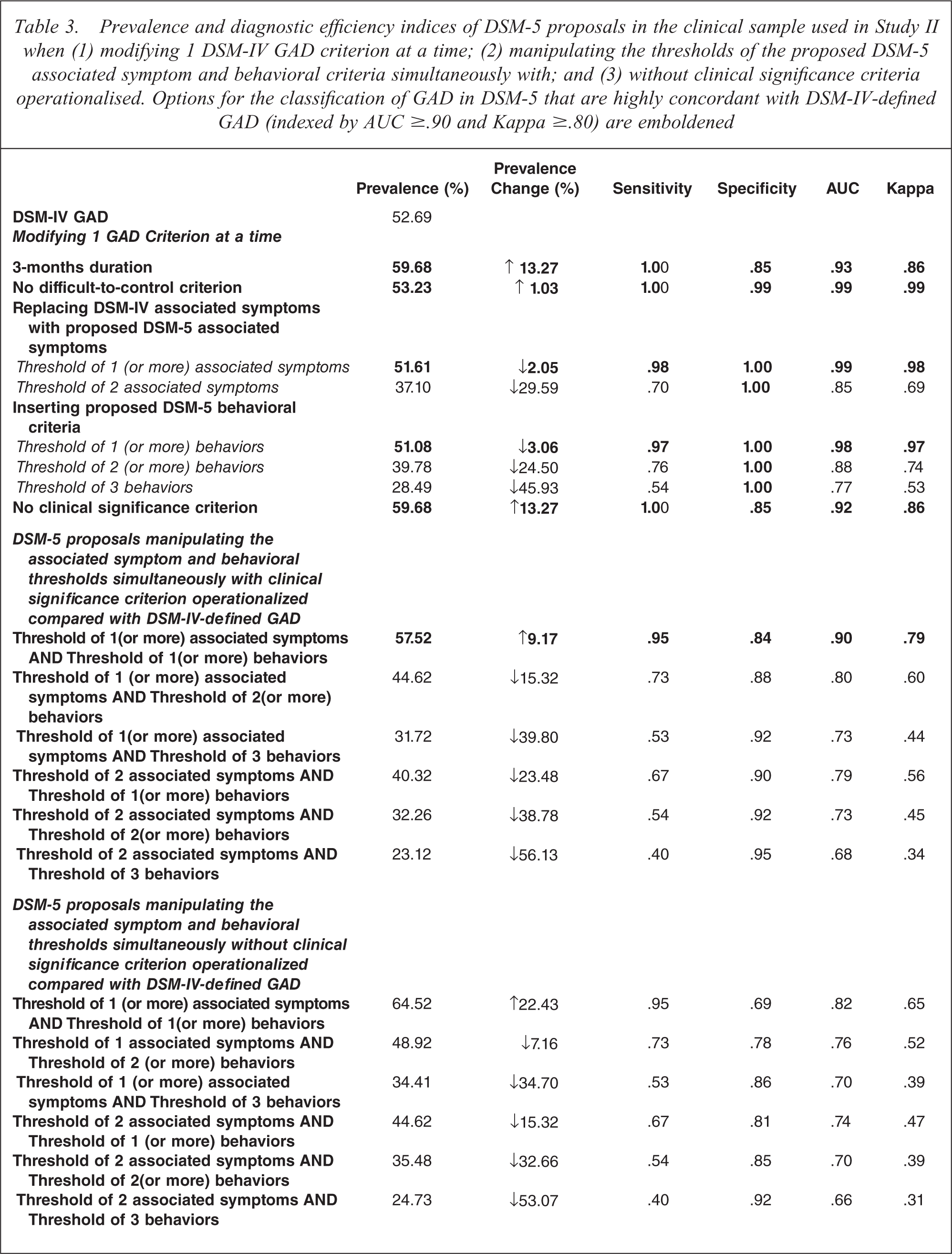
In total twenty combinations of the proposed DSM-5 criteria were examined (see Table 3). If only the duration threshold was reduced to 3 months or if the clinical significance criterion was omitted in DSM-5, the prevalence of DSM-IV-defined GAD would increase by 13%. Deleting the difficult-to-control criterion increased the number of cases by 1% whereas requiring 1/2 associated symptoms or 1/3 behaviours decreased the prevalence by 2% to 3%. In all the above situations the indices of agreement with DSM-IV remained high (AUC ≥ 0.9, Kappa ≥ 0.8). Applying all of the DSM-5 proposals (3-month duration, no difficult-to-control criterion, 1 from 2 associated symptoms, and 1 from 3 behavioural symptoms) the prevalence increased by 9% over that of DSM-IV (AUC=0.9 and Kappa=0.79). If the clinical significance criteria was also removed, the prevalence rose by 22% over that of DSM-IV and the indices of agreement with DSM-IV fell (AUC=0.82 and Kappa=0.65).
Prevalence and diagnostic efficiency indices of DSM-5 proposals in the clinical sample used in Study II when (1) modifying 1 DSM-IV GAD criterion at a time; (2) manipulating the thresholds of the proposed DSM-5 associated symptom and behavioral criteria simultaneously with; and (3) without clinical significance criteria operationalised. Options for the classification of GAD in DSM-5 that are highly concordant with DSM-IV-defined GAD (indexed by AUC ≥.90 and Kappa ≥.80) are emboldened
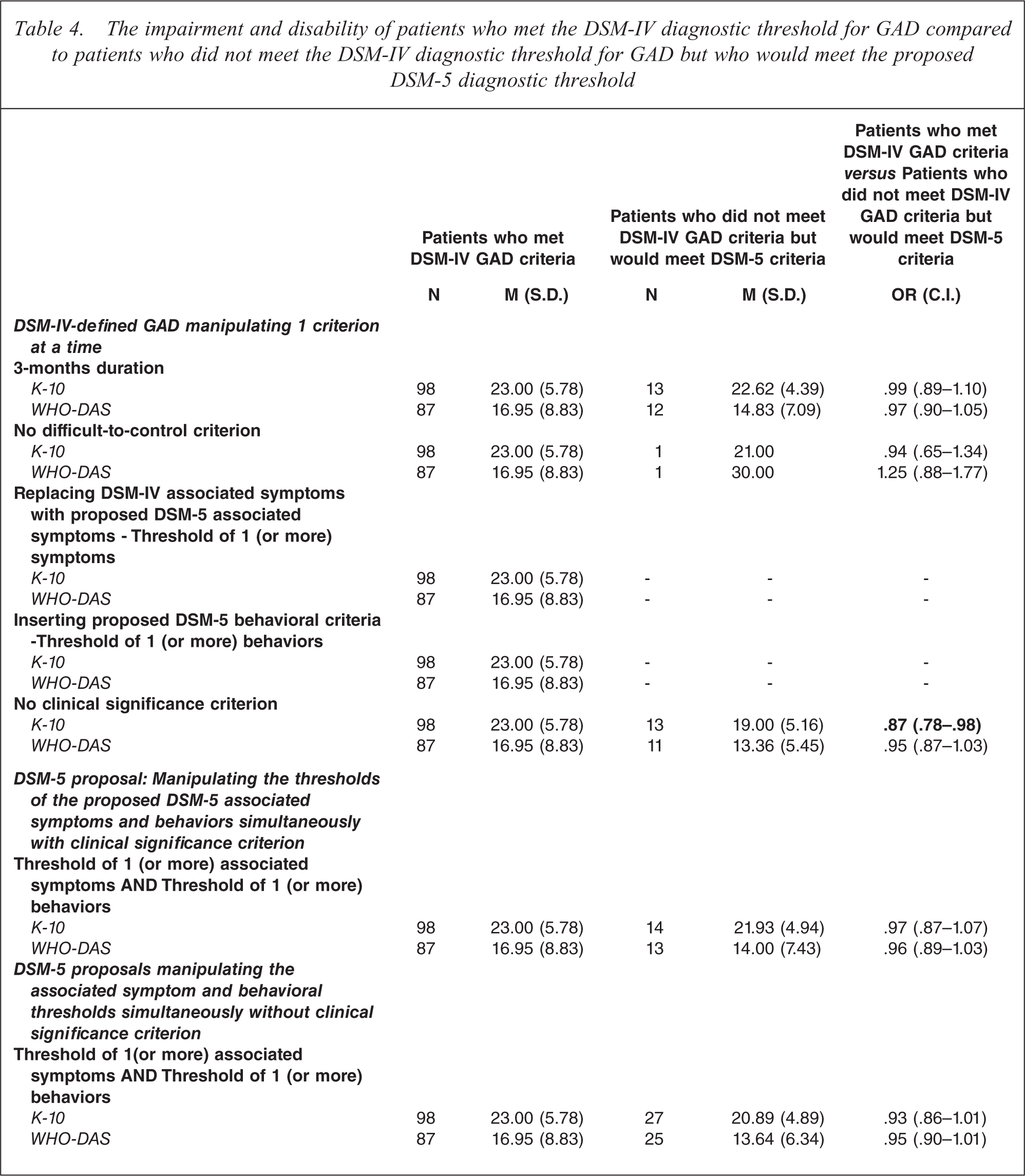
The question is, given the poorer concordance between DSM-IV-defined GAD and DSM-5-defined GAD if the proposed criteria are operationalized and the clinical significance criteria removed, are the introduced cases (patients who are DSM-IV negative but DSM-5 positive for a GAD diagnosis) less severe than the DSM-IV cases. The numbers were not large and while in all cases the scores on distress (K-10) and disability (WHO-DAS2.0) were lower in the new cases in only one analysis (removing the clinical significance criteria alone) were the odds ratios significant. The mean K-10 and WHO-DAS2.0 scores for the concordant classifications by patient group are displayed in Table 4.
The impairment and disability of patients who met the DSM-IV diagnostic threshold for GAD compared to patients who did not meet the DSM-IV diagnostic threshold for GAD but who would meet the proposed DSM-5 diagnostic threshold
Discussion
Andrews, Hobbs, Borkovec et al. [1] recommended that changes in the A, B & C criteria for DSM-IV GAD be considered to improve the transparency, reliability and validity of DSM-IV-defined Generalized Anxiety Disorder. They did not make recommendations as to the D, E & F criteria. The DSM-5 Impairment Work Group however, were asked to explore the consequences of removing the clinical significance criterion (D) and replacing it with a dimensional measure of disability. Two studies were undertaken here to examine the effect of these DSM-5 proposals on prevalence and severity.
When epidemiological data, which necessarily lacked the new behavioural criteria, were used the proposal of excessive anxiety and worry over multiple domains that occurs more days than not for 3 months (or more), no difficult to control criterion and associated with restless/keyed up or muscle tension (changed criteria are in italics) and met the clinical significance criterion resulted in a 21% increase in prevalence and a strong concordance with DSM-IV diagnoses (AUC=0.97, Kappa=0.84).
When a clinical sample of convenience was used results were comparable to the previous study. The introduction of the changes listed above plus the requirement of 1 (or more) behaviours increased the number of cases by 9%, less than the increase observed in the population sample but still with a strong concordance with DSM-IV diagnoses (AUC=0.9 and Kappa=0.79). Removal of the clinical significance criterion (Criterion E) in addition to the other proposed DSM-5 changes produced a further 13% more cases and the indices of agreement with DSM-IV fell (AUC=0.82, Kappa=0.65). The severity of the extra cases as measured from distress (K-10) or disability (WHODAS 2.0) were not significantly different to the DSM-IV diagnosed cases except for when the clinical significant criterion was removed singularly, although there was little power to detect such changes.
There are threats to the validity of these findings. In both studies the differing criteria were embedded in the same interview and this could have increased concordance over having two separate interviews administered in counterbalanced order at different times. The first study used a sample of the general population interviewed face-to-face by trained lay interviewers, the second study used a clinical sample interviewed over the phone by health professionals, and the results could differ. The first study concerned lifetime diagnoses and having had treatment at sometime, the second study used 12-month diagnoses and current treatment-seeking and again different results could have been expected. The surprise is that the results of both studies were largely concordant. Although it is likely that the proposed criteria will increase the prevalence of GAD, this work provides preliminary evidence that the criteria may not distort the severity of cases that would be identified. We now need data on the reliability, validity and utility of the new criteria and these are proper questions for the DSM-5 field trials.
Footnotes
Acknowledgements
The contributions of the clinical and research staff at the Clinical Research Unit for Anxiety and Depression in particular N. Titov, E. Robinson, L. Johnston, G. Titov, K. Solley, M. Davies, and A. Kemp for their assistance in the assessment of patients is gratefully acknowledged.
The opinions presented in this manuscript are those of the authors and not that of the DSM-5 Anxiety, Obsessive-Compulsive Spectrum, Posttraumatic, and Dissociative Disorders Work Group.