
Abstract
Objective:
Children and adolescents with a range of psychiatric disorders are increasingly being prescribed atypical or second-generation antipsychotics (SGAs). While SGAs are effective at treating conduct and behavioural symptoms, they infer significant cardiometabolic risk. This study aims to explore what patient, treatment, and health care utilization variables are associated with adherence to Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) metabolic monitoring guidelines.
Method:
A retrospective chart review of 294 children and adolescents accessing a large outpatient psychiatry setting within a 2-year study period (2014-2016) was conducted. Baseline and follow-up metabolic monitoring, demographic, treatment, and health care utilization variables were then assessed over a 1-year period of interest.
Results:
Metabolic monitoring practices did not adhere to CAMESA guidelines and were very poor over the 1-year observation period. There were significant differences between children (ages 4-12 years, n = 99) and adolescents (ages 13-18 years, n = 195). In adolescents, factors associated with any baseline metabolic monitoring were a higher number of psychiatry visits (odds ratio [OR], 1.2; 95% confidence interval [CI], 1.10 to 1.41), longer duration of contact (OR, 14; 95% CI, 2.31 to 82.4), and use of other non-SGA medications (OR, 3.2; 95% CI, 1.17 to 8.94). Among children, having an emergency room visit (OR, 3.4; 95% CI, 1.01 to 11.71) and taking aripiprazole (OR, 7.4; 95% CI, 2.02 to 27.45) increased the odds of receiving baseline metabolic monitoring.
Conclusion:
Findings from this study highlight the need for better metabolic monitoring for children and adolescents taking SGAs. Enhanced focus on opportunities for multidisciplinary collaboration is needed to improve the quality of care offered to this population.
Keywords
Children and adolescents with a range of psychiatric diagnoses and symptom clusters are increasingly being prescribed atypical or second-generation antipsychotics (SGAs) to treat conduct and behavioural symptoms. 1 For instance, the rate of pediatric prescriptions for all antipsychotic medications prescribed in 2013 was 168 per 1000 youth, which represents a 33% increase since 2010. Of these antipsychotic prescriptions, SGAs accounted for 97%. 2 Studies have provided evidence to support the use of SGAs to treat aggression, irritability, and self-injurious behaviours in youth with autistic spectrum disorder, 3,4 as adjunctive treatment to help regulate behaviour in children and adolescents with attention-deficit hyperactivity disorder (ADHD), 5 –7 to improve psychological symptoms and promote weight gain in children and adolescents with eating disorders such as anorexia nervosa, 8,9 in the treatment of adolescents with psychosis, 10 youth with bipolar disorder, 11,12 and youth with Tourette’s syndrome. 13,14
However, Health Canada has not approved the use of SGAs in pediatric populations because their efficacy and safety have not been confirmed by clinical studies. 15 –17 One exception is the use of aripiprazole in adolescent populations to treat symptoms of bipolar disorder and schizophrenia. 18 SGAs must be used with caution as they cause metabolic, neurologic, and endocrine side effects including weight gain, drowsiness, deviations in blood pressure, arrhythmias, hyperglycemia, hyperlipidemia, hyperprolactinemia, thyroid dysfunction, extrapyramidal symptoms, and diabetes. 19,20
Children and adolescents are not just smaller versions of adults; they are in a state of dynamic developmental physiology that can be negatively impacted by side effects of medications. 21,22 Experiencing early vulnerability to cardiac and metabolic instability is problematic as it can develop into serious chronic diseases later in adulthood. 21,23,24 Weight gain is particularly concerning as age-inappropriate weight gain in excess of normal growth is associated with an increased risk of obesity and metabolic syndrome in adulthood, which is linked to poor cardiovascular outcomes and affects morbidity. 25,26 Overweight children and adolescents have abnormal levels of lipids, insulin, blood pressure, and elevated adiposity, which is associated with fatty streaks, raised lesions, and calcification in the aorta in coronary arteries. These are risk factors for atherosclerosis and cardiovascular disease. 27 SGA-related weight gain in youth may be caused by pharmacodynamic medication effects such as increased appetite, decreased satiety, sleep disturbance, and sedation. These contribute to increased caloric intake and decreased physical activity and are modulated by genetic predisposition. 28 The amount of weight gain may vary depending on what type of SGA is used. For example, a 12-week cohort study of children and adolescents found that after a median 10.8 weeks of treatment, baseline weight increased by 6.1 kg (95% confidence interval [CI], 4.9 to 7.2 kg) with quetiapine (n = 36) compared with 4.4 kg (95% CI, 3.7 to 5.2 kg) with aripiprazole (n = 41). 20 SGAs are also known to cause cardiac arrhythmias such as QTc interval prolongation, a risk for potentially life-threatening ventricular arrhythmias. 29
Although weight gain is a normal part of growth and development, influenced by critical periods, including adiposity rebound (between 3 and 7 years) and puberty (between 11 and 15 years for girls and 13 and 17 years for boys), multiple studies have demonstrated that children and adolescents initiated on SGAs can experience clinically significant weight gain of at least 7% of baseline body weight. 30 –32 This is greater and faster weight gain than reported in adult populations. 25,33 –35 There is limited research comparing differences in antipsychotic-related weight gain between child and adolescent age groups. Prior research has suggested that past treatment and intensity of antipsychotic exposure lessens the impact of weight gain more so than age and developmental differences; therefore, greater weight gain experienced by youth may be best explained by their naivety to antipsychotic medication compared with adults. 25 Regardless of the aetiology, metabolic monitoring is required to prevent cardiometabolic instability for children and adolescents using SGAs. 36
Metabolic Monitoring
The Canadian Alliance for Monitoring Effectiveness and Safety of Antipsychotics in Children (CAMESA) has published evidence-based recommendations that provide a guideline for clinicians to use to monitor SGA use in pediatric patients. 37 These guidelines call for routine physical health assessments and laboratory monitoring at regular frequencies (i.e., baseline and 1-, 2-, 3-, 6-, 9-, and 12-month follow-up intervals) as a means to prevent and detect physical adverse effects of SGA use. While similar guidelines exist internationally, a systematic review of 48 studies (n = 290 534 adults with schizophrenia-spectrum disorders) examining guideline concordance conducted in Canada, the United States, the United Kingdom, Spain, and Australia concluded that metabolic monitoring practices are concerningly low among people prescribed antipsychotic medication. 38 –40 This is consistent with the monitoring rates reported in the pediatric metabolic monitoring literature. 41 –44
Given the prevalence of SGA use in pediatric populations and the adverse cardiometabolic effects associated with their use, it remains unclear why prescribers are not more pharmacovigilant with metabolic monitoring. Few studies have investigated factors that predict whether a patient will receive metabolic monitoring. Morrato et al. 44 studied children and adolescents (n = 5370) in a retrospective, SGA-naive cohort from 180 days prior and following the initiation of an SGA to measure monitoring rates and determine predictors of serum glucose and lipid testing using government social insurance claims data. It was found that having multiple psychiatric comorbidities, having serious mental illness, or having been to the emergency room or hospitalized within the 1-year study period were significant predictors of monitoring. No differences between types of SGAs were noted. 44 Other metabolic monitoring studies in adult and veteran populations found that preexisting metabolic conditions such as diabetes or hypertension were significant predictors of monitoring. This may suggest that children and adolescents with increased severity of mental or physical illness are more likely to receive monitoring. 45,46
This article builds on previous work to explore metabolic monitoring practices and factors associated with monitoring among children and adolescents taking SGAs. The primary aim of this study is to explore what patient, treatment, and health care utilization variables are associated with adherence to CAMESA metabolic monitoring guidelines among a sample of children and adolescents taking SGAs and accessing outpatient pediatric psychiatry, where the majority of SGA prescriptions are initiated in Canada.
Methods
Setting and Study Population
A retrospective chart review of all patient referrals to an outpatient child and adolescent psychiatric program (i.e., Mood and Anxiety, Neurodevelopmental, Urgent Consult) in Southeastern Ontario was performed. The data were collected by accessing the clinic’s electronic medical records, which at the time of data collection consisted only of scanned documents from paper charts and electronic laboratory results originating within the clinic’s hospital. The charts reviewed in this study were those of the patients of 4 independent child psychiatrists. Children and adolescents aged 4 to 18 years who had their first clinic visit between September 1, 2014, and August 31, 2015 (n = 1118), were reviewed for any evidence of SGA treatment (i.e., risperidone, quetiapine, aripiprazole, olanzapine, ziprasidone, paliperidone, clozapine, asenapine, or lurasidone). This time period was chosen with the intent to capture SGA treatment over a 12-month period, which is the average treatment duration, with shorter durations recommended for younger children and longer durations for older adolescents. 33 To be included in the study, the participant’s first clinic visit date had to be at least 1 year prior to the end of the study period. Participants were included even if their SGA treatment was less than 1 year. For participants who met this inclusion criteria (n = 294), we completed a detailed data abstraction across the 2-year study period (September 1, 2014, to August 31, 2016). Participants were excluded from the study if they had no evidence of SGA use within the screening window.
Data Collection
A data abstraction instrument was adapted from the CAMESA Monitoring Safety of SGA in Children Data Form to measure 16 physiological parameters across 4 time periods (i.e., 0-1 month, 1-3 months, 3-6 months, and greater than 6 months). 37 All data collected were from 1 electronic charting system in 1 setting (outpatient child and adolescent psychiatry program), and no monitoring data from outside sources (i.e., primary care or emergency services) were collected as they were beyond the scope of this review. Participant demographics and treatment data were collected by health care providers during the baseline visit. All variables were collected consistently between patients, these included age, sex (i.e., male/female), postal code, household support (e.g., 2 parents, single parent), diagnosis (e.g., ADHD, anxiety), and SGA type (e.g., risperidone, quetiapine). Other medications prescribed to participants were also recorded and categorized as ADHD medication (i.e., stimulants), antidepressant (e.g., selective serotonin reuptake inhibitors), or nonpsychotropic medication (e.g., contraception, sleep medication). Health care utilization variables that took place over the study period included duration of contact with the program, number of psychiatry visits, number of communications between psychiatrist and primary care provider, number of specialist referrals, number of hospital admissions, and number of emergency room visits.
Metabolic monitoring parameters collected included height, weight, waist circumference, blood pressure, neurologic examination, electrocardiogram, and laboratory monitoring (i.e., glucose, insulin, total cholesterol, low-density lipoprotein, high-density lipoprotein, triglycerides, aspartate aminotransferase, alanine aminotransferase, prolactin, and amylase). Glucose specimens that were not specified as “fasting,” as recommended in CAMESA guidelines, were viewed as a valid measure of monitoring as it was not possible to make the determination of whether or not the patient had fasted based on the information available in the charts. Baseline metabolic monitoring was the main outcome variable and defined as any documented parameter occurring 180 days before through 30 days after SGA initiation (i.e., any bloodwork that occurred within 6 months prior to the initiation of an SGA was also considered as baseline monitoring). Follow-up metabolic monitoring data were identified as any monitoring data recorded within 3 time points corresponding to the CAMESA guidelines (i.e., 1-3 months, 3-6 months, and greater than 6 months). Ethical approval was obtained from the Queen’s University Health Sciences Research Ethics Board (see the Supplemental Appendix).
Statistical Analysis
Participant demographics, treatment variables, and health care utilization variables were described using frequencies and descriptive statistics. Because of a priori hypothesized differences between children and adolescents, data were compared between age groups. Chi-squared and t-tests were used to test for differences between children and adolescents in terms of demographic, treatment, and health care utilization variables as well as baseline metabolic monitoring practices.
To determine how often providers engaged in metabolic monitoring practice, regardless of intensity, any evidence of baseline and follow-up documentation was determined for participants who had at least 1 parameter documented; this was referred to as “any monitoring.” Bivariate analyses (chi-squared for categorical and t-test for continuous) were performed to determine significant associations between exploratory variables and the presence of any monitoring at baseline. Significant variables (P < 0.1) were entered into a logistic regression model using forced entry to assess their relationship with the main outcome (i.e., any baseline metabolic monitoring). All analyses were performed with SPSS Statistical Software, version 24.0. 47
Results
Participant Demographics, Treatment, and Health Care Utilization
Demographic and treatment variables for participants at their baseline visit are presented in Table 1. Among the 294 children and adolescents receiving SGA treatment, the age range was 4 to 18 years, with a mean age of 13.5 (±3.27) years, and 42.9% were female. The majority of the sample was SGA naïve, with 171 (58.2%) initiating a SGA at their baseline visit. Being “SGA naïve” was defined as a participant who had no SGAs listed in their medical history or any current prescriptions of an SGA at their baseline visit. Risperidone was the most commonly prescribed SGA, with 132 (44.9%) of participants using it at baseline, followed by 88 (29.9%) quetiapine prescriptions. SGAs unrepresented in the sample were ziprasidone, paliperidone, clozapine, asenapine, and lurasidone.
Participant demographics and treatment variables at baseline.
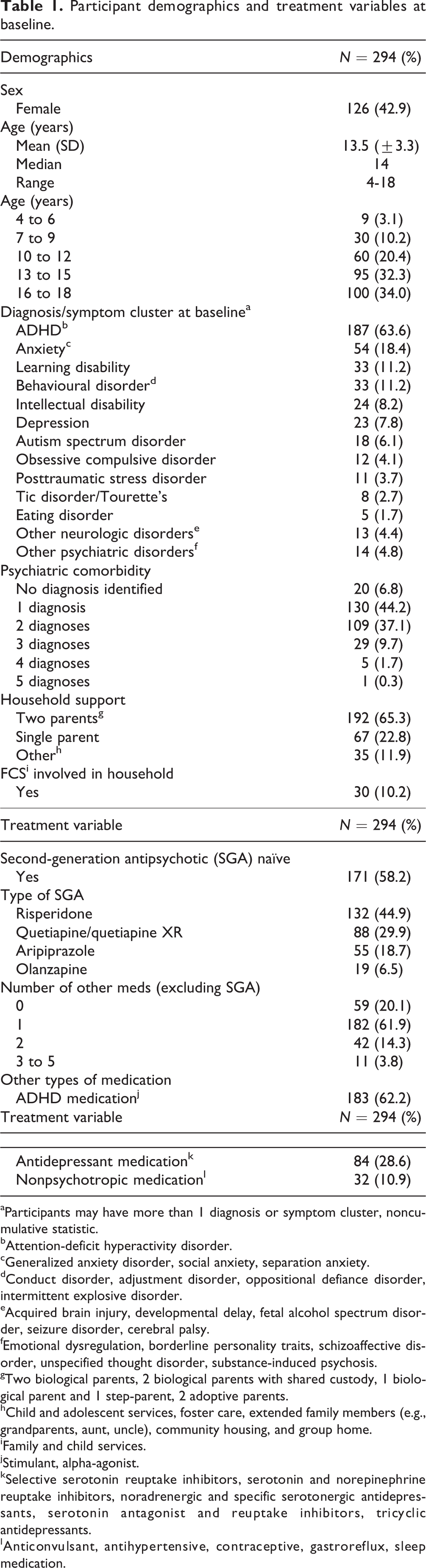
aParticipants may have more than 1 diagnosis or symptom cluster, noncumulative statistic.
bAttention-deficit hyperactivity disorder.
cGeneralized anxiety disorder, social anxiety, separation anxiety.
dConduct disorder, adjustment disorder, oppositional defiance disorder, intermittent explosive disorder.
eAcquired brain injury, developmental delay, fetal alcohol spectrum disorder, seizure disorder, cerebral palsy.
fEmotional dysregulation, borderline personality traits, schizoaffective disorder, unspecified thought disorder, substance-induced psychosis.
gTwo biological parents, 2 biological parents with shared custody, 1 biological parent and 1 step-parent, 2 adoptive parents.
hChild and adolescent services, foster care, extended family members (e.g., grandparents, aunt, uncle), community housing, and group home.
iFamily and child services.
jStimulant, alpha-agonist.
kSelective serotonin reuptake inhibitors, serotonin and norepinephrine reuptake inhibitors, noradrenergic and specific serotonergic antidepressants, serotonin antagonist and reuptake inhibitors, tricyclic antidepressants.
lAnticonvulsant, antihypertensive, contraceptive, gastroreflux, sleep medication.
As for health care utilization variables (Table 2), the majority of participants, 165 (56.1%), were in contact with the program for greater than 6 months, while 77 (26.2%) had contact with the program for less than 1 month. In terms of utilization of other health care resources, 113 (38.4%) had at least 1 visit to the emergency room, and 68 (23.1%) were admitted to the hospital at least once. Select demographics, treatment, and health care utilization variables were stratified by age group (children 4-12 years and adolescents 13-18 years) and compared in Table 3, with statistically significant differences noted between sex, diagnosis, and SGA treatment, all at significance level of P < 0.001.
Participant health care utilization variables.
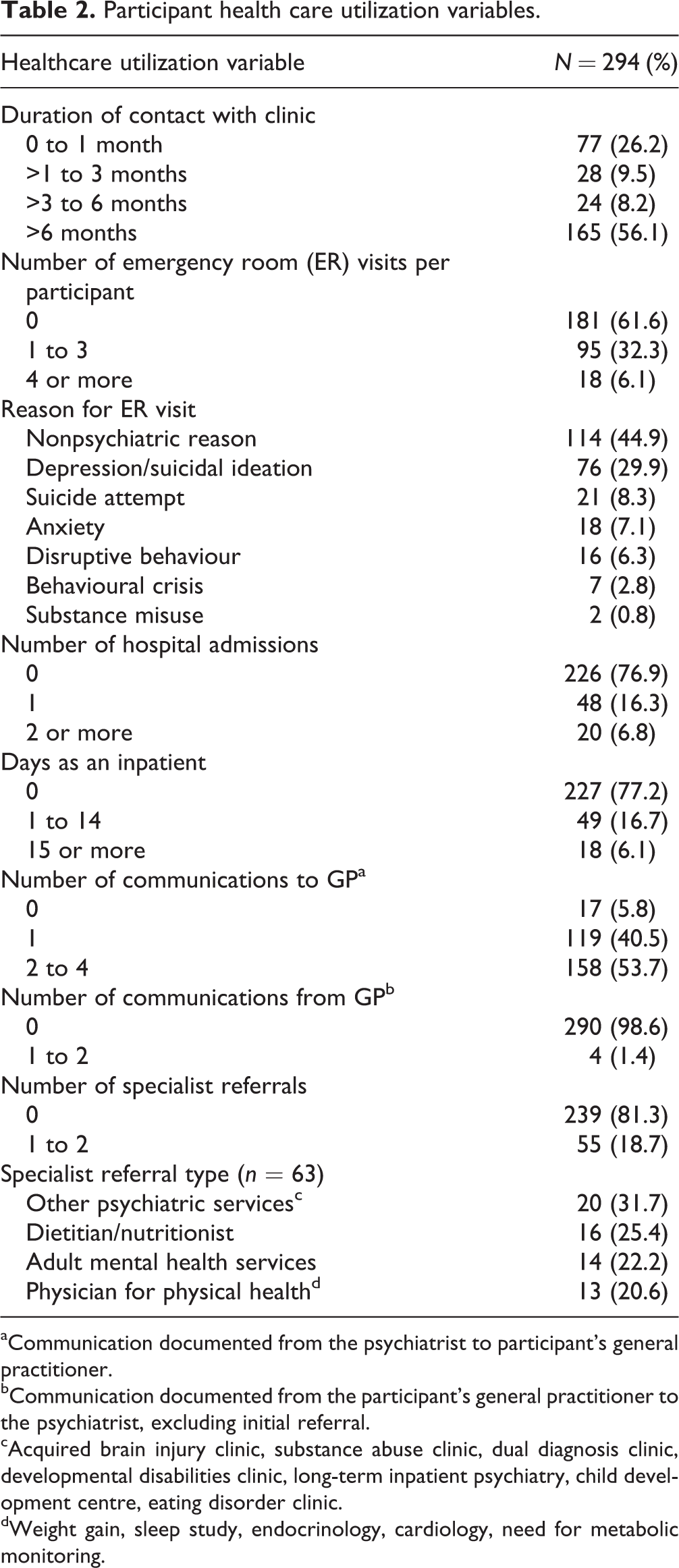
aCommunication documented from the psychiatrist to participant’s general practitioner.
bCommunication documented from the participant’s general practitioner to the psychiatrist, excluding initial referral.
cAcquired brain injury clinic, substance abuse clinic, dual diagnosis clinic, developmental disabilities clinic, long-term inpatient psychiatry, child development centre, eating disorder clinic.
dWeight gain, sleep study, endocrinology, cardiology, need for metabolic monitoring.
Participant demographics, treatment variables, and metabolic monitoring, stratified by age group.
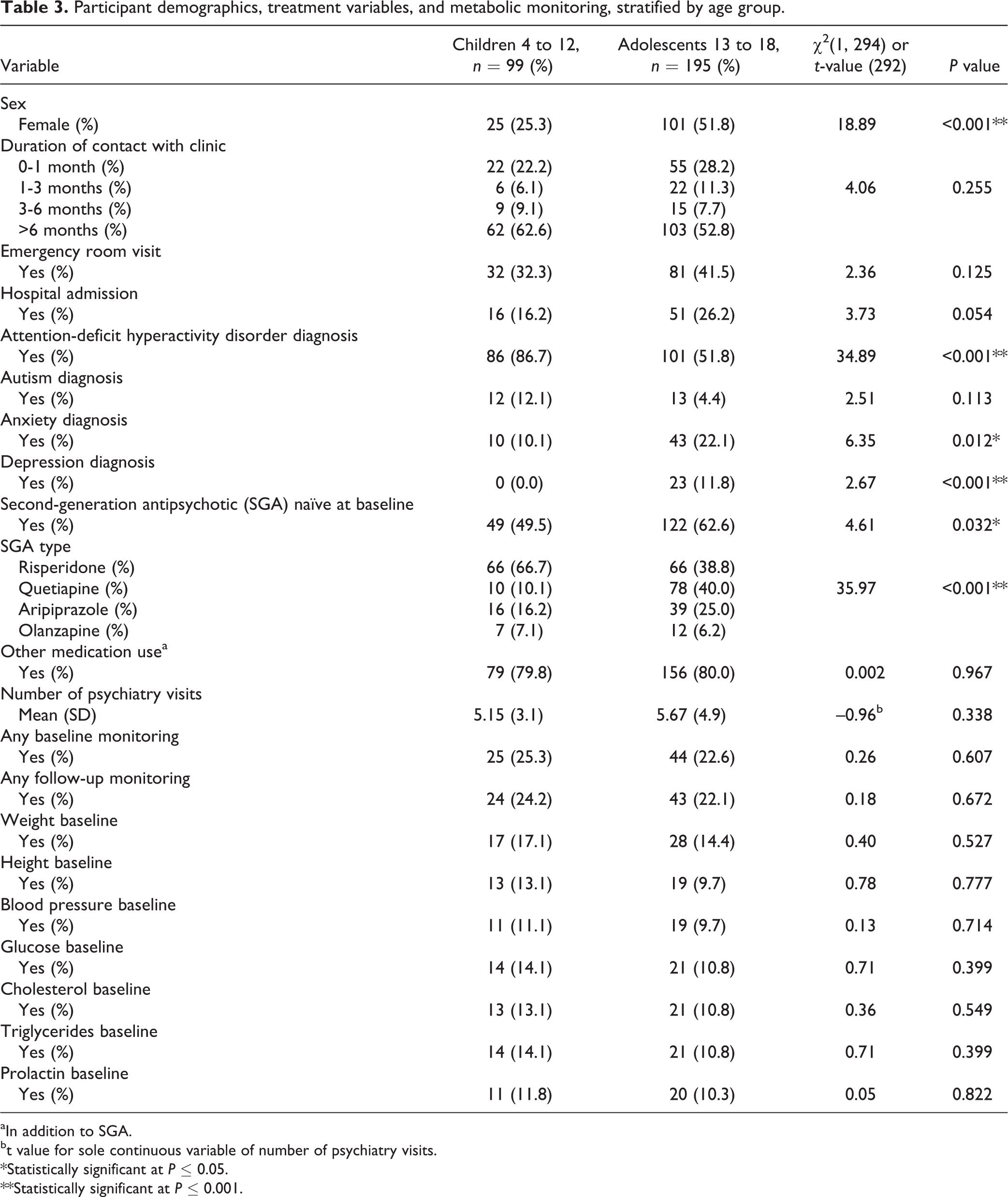
aIn addition to SGA.
bt value for sole continuous variable of number of psychiatry visits.
*Statistically significant at P ≤ 0.05.
**Statistically significant at P ≤ 0.001.
Rates of Metabolic Monitoring
Of the 294 participants, none received metabolic monitoring that would be considered adherent to the recommended CAMESA guidelines. From an individual perspective, of the possible 64 total metabolic monitoring measurements (i.e., 16 parameters across 4 time periods), the range of parameters documented was 0 to 22 for all participants. Group-level monitoring data are summarized in Table 3 and compared between age groups. At baseline, 25 (25.3%) children and 44 (22.6%) adolescents had any monitoring documented. At follow-up, 24 (24.2%) children and 43 (22.1%) adolescents had any monitoring documented. The most frequently documented parameter was weight, which 45 (15.3%) of the participants had documented at baseline and 53 (18.0%) of participants had documented in any follow-up period. Only 17 (5.8%) participants had their weight documented at baseline and at any follow-up visit. Because of low rates of follow-up monitoring, further analysis focused on any baseline monitoring and comparing the differences between age groups.
Factors Associated with Metabolic Monitoring at Baseline
Table 4 presents the results from the logistic regression model measuring factors associated with the likelihood of receiving any baseline metabolic monitoring. Baseline metabolic monitoring was defined as having at least 1 metabolic monitoring parameter documented from 180 days before through 30 days after the initiation of SGA treatment. Two logistic regression models were used, one for children that contained 3 independent variables (emergency room visit, type of SGA, and number of psychiatry visits) and one for adolescents that contained 8 independent variables (duration of contact with clinic, emergency room visit, hospital admission, psychiatric comorbidity, ADHD diagnosis at baseline, type of SGA, use of other medications, and number of psychiatry visits). The independent variables used in each of the models were determined in the preliminary bivariate analysis. In adolescents, the factors making a significant contribution to the model were participants with a higher number of psychiatry visits total (odds ratio [OR], 1.2; 95% CI, 1.10 to 1.41), duration of contact with clinic of 1 to 3 months (OR, 14; 95% CI, 2.31 to 82.4, in comparison with those with 0-1 month duration), and prescriptions of medications in addition to SGA use (OR, 3.2; 95% CI, 1.17 to 8.94). In children, the factors making a significant contribution to the model included emergency room visit (OR, 3.4; 95% CI, 1.01 to 11.71) and those with aripiprazole as the type of SGA for treatment (OR, 7.4; 95% CI, 2.02 to 27.45 in comparison with those on risperidone).
Logistic regression of factors associated with any baseline metabolic monitoring.
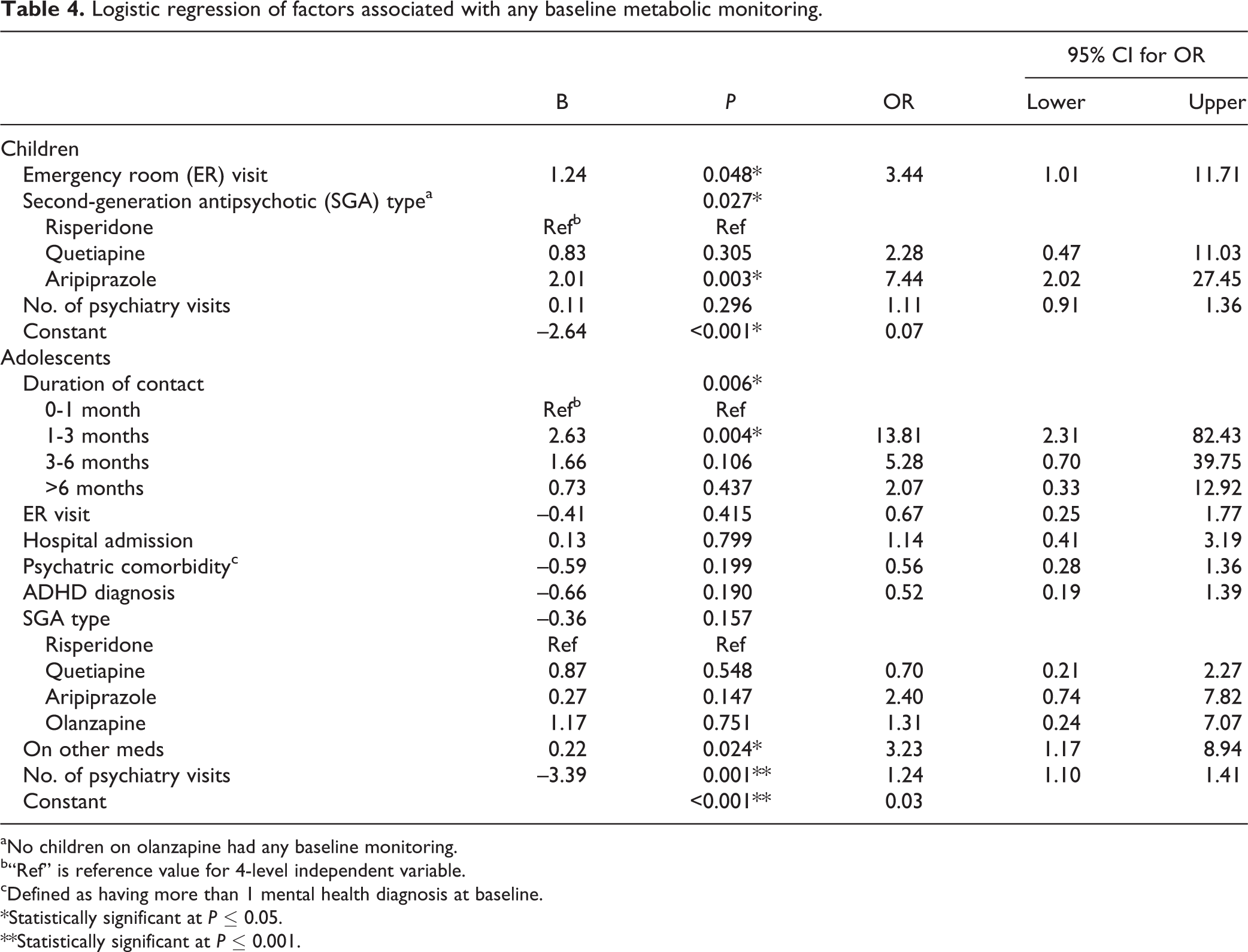
aNo children on olanzapine had any baseline monitoring.
b“Ref” is reference value for 4-level independent variable.
cDefined as having more than 1 mental health diagnosis at baseline.
*Statistically significant at P ≤ 0.05.
**Statistically significant at P ≤ 0.001.
Discussion
This study adds to previous work by quantifying metabolic monitoring practices in South Eastern Ontario, Canada, and identifies factors associated with baseline metabolic monitoring in children and adolescents on SGAs. Consistent with previous findings, the results of this study demonstrate that metabolic monitoring is inadequate in outpatient pediatric psychiatry and inconsistently implemented. 41 –44 Less than a quarter of participants were engaged in any metabolic monitoring behaviour at baseline or at any of the 3 CAMESA guideline follow-up intervals. The lack of documented monitoring is concerning in this population given the well-documented risks of metabolic, cardiovascular, and endocrine adverse effects.
Our findings are novel in that they examine metabolic monitoring among 2 age groups within the pediatric population, children and adolescents. There were more male children in the sample, diagnosed with ADHD and taking risperidone. The adolescent group was significantly more female, diagnosed with anxiety and depression and taking quetiapine for SGA treatment. These differences correspond with typical clinical presentations associated with each age group. 48 –50 The type of SGA medication being used in treatment may be an important consideration of monitoring since each SGA differs in their pharmacokinetics and side effect profile. If children are more often treated with one type of SGA and adolescents another, this presents different profiles of cardiometabolic risk to each age group and as a result different priorities for metabolic monitoring. Physiological differences between child and adolescent age groups have important implications in SGA treatment and merit further investigation.
Age differences were also evident when examining factors associated with documented baseline metabolic monitoring. For children, having an emergency room visit was associated with receiving monitoring. This is consistent with findings from Morrato et al., 44 which reported emergency room visits as a significant predictor of baseline glucose and lipids monitoring practices in a pediatric population using SGAs. Depending on their reason for accessing emergency services, previous studies have argued that patients who have received this additional blood work required medical evaluation (i.e., treatment related and not monitoring related). This study does not account for any laboratory monitoring that was done in the emergency department or outside of the outpatient psychiatry clinic. The fact that these data were collected only if they were performed within the clinic can be seen as both a limitation and strength as it does not account for monitoring performed elsewhere but also minimizes the likelihood that the blood work was for reasons other than metabolic monitoring.
Morrato et al. 44 found no differences in baseline monitoring between types of SGAs, unlike our finding that children taking aripiprazole were more likely to be monitored. The association found between baseline monitoring in children taking aripiprazole could potentially be attributed to practitioners’ knowledge that it is approved only for adolescent use, therefore potentiating the need for extra caution in children. For adolescents, taking other medications in addition to a SGA, having a longer duration of contact with the program and higher number of psychiatry visits were significantly associated with receiving baseline monitoring. It might be reasonable to hypothesize that adolescents taking multiple medications and having a higher level of engagement with the outpatient clinic could have increased severity of illness, which could positively affect receipt of monitoring behaviour. 44 –46 Understanding the factors that influence a practitioner’s decision of whether or not to engage their patient in baseline metabolic monitoring serves to inform strategies for future research and practitioners to reflect upon.
The prevalence of children and adolescents taking SGAs, diagnosed with ADHD and reporting using medications to treat ADHD, is consistent with recent studies. Individuals with ADHD have higher health service utilization, including primary care, specialist consultation, and emergency department use and a higher burden of psychiatric comorbidities. 49,51 The prevalence of psychosis is notably low among children treated with SGAs, which demonstrates that they are used primarily off-label. 49 This is an important group to highlight given the high proportion of participants with ADHD in this study, low rates of documented monitoring found among them, and undefined indications for use.
Investigating strategies to improve the uptake of CAMESA guidelines in child and adolescent psychiatry is needed to enhance medication safety and the physical health of youth taking SGAs. Multidisciplinary collaboration may serve as a practical solution to facilitating monitoring in outpatient pediatric psychiatry. Nurses, nurse practitioners, pharmacists, physiotherapists, dietitians, or other medical specialists can be collaborators who share the responsibility of physical health monitoring with psychiatrists and general practitioners. 52 –55 This suggestion aligns with the current direction of mental health care in Canada, which envisions collaborative and shared mental healthcare. The Canadian Collaborative Mental Health Initiative and the Canadian Psychiatric Association and the College of Family Physicians of Canada Collaborative Working Group on Shared Mental Health Care support the vision for co-location of health services, which would improve accessibility, facilitate multidisciplinary collaboration, and optimize care. 56,57
There are several limitations of this retrospective chart review, which used a convenient sample in one localized outpatient child and adolescent psychiatry program. Caution is advised regarding the generalizability of these results. It should be acknowledged that information that was undocumented, uninterpretable, incomplete, or missing in participant charts was not accounted for. Because of very low rates of metabolic monitoring and an incomplete data set, the analysis was restricted to analyses of baseline assessment and therefore could not explore adherence to CAMESA guidelines at multiple time points. Participant’s nonmental health comorbidities (e.g., obesity, diabetes) were not accounted for. Reason for discontinuation of SGA treatment (i.e., due to side effects) was not reported in this study as, although clinically valuable, this information was not readily available within the audited charts. Moreover, the results are limited in that monitoring data are not classified by prescriber or clinic type, therefore failing to account for individual child psychiatrist monitoring practices and/or differences in monitoring between programs (e.g., neurodevelopment compared with mood and anxiety clinic).
The global lack of documented metabolic monitoring across all participants and noted differences between child and adolescent participants are our most significant findings. This highlights the need for health care professionals to reevaluate their current metabolic monitoring practices within this vulnerable group and draws attention to a knowledge translation gap (i.e., between best practice in pediatric metabolic monitoring and behaviour in clinical practice settings). We see a need for future research investigating the use of administrative databases devoted to pediatric metabolic monitoring of SGA use, such as the Safety of Neuroleptics in Infancy and Adolescence registry, which has been trialed in Spain. 58 Such methods of documentation would allow for access to metabolic monitoring tools that are specific to the patient’s age, development, and SGA treatment. This type of registry would eliminate discrepancies between institutional charting systems and serve a dual purpose of collecting epidemiological and adverse event data to enhance patient safety.
Conclusion
This study highlights a gap between clinical practice guidelines and metabolic monitoring practices offered to children and adolescents receiving SGAs in outpatient psychiatry. It also advances our understanding of patient, treatment, and health care utilization variables associated with receiving baseline metabolic monitoring and explores differences between pediatric age groups. These factors should be further examined in practice and future research. It is evident that increasing adherence to the CAMESA metabolic monitoring guidelines should be made a priority in child and adolescent outpatient psychiatry. Moreover, multidisciplinary conversation about how to better collaborate in the outpatient settings is warranted to ensure that high-quality care is delivered to children and adolescents using SGAs.
Supplemental Material
Supplemental Material, Codebook_for_CJP_Nov_11_2017 - Patient, Treatment, and Health Care Utilization Variables Associated with Adherence to Metabolic Monitoring Practices in Children and Adolescents Taking Second-Generation Antipsychotics
Supplemental Material, Codebook_for_CJP_Nov_11_2017 for Patient, Treatment, and Health Care Utilization Variables Associated with Adherence to Metabolic Monitoring Practices in Children and Adolescents Taking Second-Generation Antipsychotics by Mary Coughlin, Catherine Lindsay Goldie, Joan Tranmer, Sarosh Khalid-Khan, and Deborah Tregunno in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, Data_Set_for_CJP_Nov_28_2017 - Patient, Treatment, and Health Care Utilization Variables Associated with Adherence to Metabolic Monitoring Practices in Children and Adolescents Taking Second-Generation Antipsychotics
Supplemental Material, Data_Set_for_CJP_Nov_28_2017 for Patient, Treatment, and Health Care Utilization Variables Associated with Adherence to Metabolic Monitoring Practices in Children and Adolescents Taking Second-Generation Antipsychotics by Mary Coughlin, Catherine Lindsay Goldie, Joan Tranmer, Sarosh Khalid-Khan, and Deborah Tregunno in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
Mary Coughlin would like to acknowledge Marina Kanellos-Sutton for facilitating access to data and sharing of her clinical expertise.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The corresponding author received funding from the Ontario Graduate Scholarship.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.