
Abstract
Objective:
This study examined relationships among hospital accessibility, socio-economic context, and geographic clustering of inpatient psychiatry admissions for adults with cognitive disorders in Ontario, Canada.
Method:
A retrospective cross-sectional analysis was conducted using admissions data from 71 hospitals with inpatient psychiatry beds in Ontario, Canada between 2011 and 2014. Data included 7,637 unique admissions for 4,550 adults with a DSM-IV diagnosis of Delirium, Dementia, Amnestic and other Cognitive Disorders. Bayesian spatial Poisson regression was employed to examine the relationship between accessibility of general hospitals with psychiatric beds and psychiatric hospitals, area-level marginalization, and hospitalization rate with the risk of admission to inpatient psychiatry among adults with cognitive disorders across 516 Forward Sortation Areas (FSA) in Ontario.
Results:
Residential instability and the overall hospitalization rate were significantly associated with an increase in the relative risk of admissions to inpatient psychiatry. Accessibility to general hospitals and psychiatric hospitals were marginally insignificant at the 95% credible interval in the final model. Significant geographic clustering of admissions was identified where individuals residing in FSA's with the highest relative risk were 2.0 to 7.1 times more likely to be admitted to inpatient psychiatry compared to the average.
Conclusions:
Geographic clustering of inpatient psychiatry admissions for adults with cognitive disorders exists across the Province of Ontario, Canada. At the geographic level, the risk of admission was positively associated with residential instability and the overall hospitalization rate, but not distance to the closest general or psychiatric hospital.
Keywords
Introduction
Care for persons with cognitive disorders is complex, involving informal and formal supports that span community and institutional contexts. For instance, persons with dementia have higher rates of physical and psychiatric service use 1 and greater care costs. 2 Coordinated care systems are essential for efficient recognition and responses to an individual’s psychological, behavioural, social and physical needs. As the disease progresses, individuals often transition out of community dwellings and use formal services, including emergency departments and acute hospital visits. 3 Community support programs may also exist in some jurisdictions to provide specialized care across the continuum. 4 The availability and coordination of these services may play a role in the person’s outcomes and health service utilisation.
Psychiatric services provide support for the assessment, stabilization, and management of individuals with cognitive disorders, particularly those with challenging behaviours. Inpatient psychiatric care may be needed in instances where the person has needs that exceed what can be provided in community-based or residential care settings. Psychiatric admissions related to cognitive disorders could be used as an indicator of both the complexity of management and the availability of intensive community supports.
Geographic variations in psychiatric admissions provide useful information about differences in the complexity and management of cognitive disorders within a health system and potential inequities in access to care. Geographic context is important to understanding the epidemiology of cognitive disorders. 5 For instance, advanced analytic techniques such as Bayesian spatial analysis have been applied to identify significant geographic variations in dementia diagnoses across Scotland and Sweden after controlling for genetic and other individual factors. 6 Geographic factors, such as neighbourhood deprivation, low social economic status, and other indicators of marginalization are associated with patterns of impaired cognition. 7 Few studies, however, have applied spatial analysis to understand patterns of health service use related to cognitive disorders. Such an analysis could provide insights into the responsiveness and equity of the health system in the management of cognitive disorders.
This study examines geographic clustering of inpatient psychiatry use for adults with cognitive disorders in Ontario, Canada. It also examines whether clustering is related to the geographic accessibility to hospitals with inpatient psychiatric care and socio-economic indicators of marginalization after controlling for overall hospitalisation rate.
Methods
A retrospective cross-sectional analysis was conducted of hospitalization data from 71 hospitals available from the Ontario Mental Health Reporting System (OMHRS) at the Canadian Institute for Health Information (CIHI). Between January 1, 2011 and December 31, 2014, there were 7,637 unique admissions representing 4,550 adults with a primary, secondary, or tertiary discharge diagnosis falling within the Delirium, Dementia, Amnestic and other Cognitive Disorders category of the Diagnostic and Statistical Manual, version 4 (DSM-IV). These data include admissions to acute psychiatric units in general hospitals as well as admissions to specialty psychiatric hospitals.
The OMHRS is based on the Resident Assessment Instrument – Mental Health (RAI-MH), an instrument used to assess every person admitted to an inpatient psychiatric bed in Ontario, Canada. The RAI-MH contains demographic, clinical, and service variables and assesses mental status, cognitive and functional status, substance use, health concerns, social life, and service utilisation. 8,9 The DSM-IV categories were designated by a psychiatrist overseeing the care of the person. The RAI-MH includes validated summary scales: The Depression Severity Index, 10 which ranges from 0 to 12, with scores of 3 or more indicating depressive symptoms; Positive Symptoms Scale, 11 measuring hallucinations and delusions on a score ranging from 0 to 12; Risk of Harm to Others Scale, 12 which ranges from 0 to 6, with scores of 3 or more being predictive of inpatient assaults; Activities of Daily Living Hierarchy Scale, 13 which measures performance in daily activity on a scale from 0 to 6; and Cognitive Performance Scale, 14 which measures the severity of impairment on a scale from 0 to 6.
Geographic Unit and Variables
This study was conducted at the Forward Sortation Area (FSA) level, a geographical unit identified by the first 3 digits of the postal code of a person’s residence. Based on the 2011 Canadian Census, there were 516 FSAs in Ontario. The median FSA population count for adults 65 y and older was 2,775, with a maximum of 18,840.
Several geographic variables were derived to examine service utilisation and accessibility using ArcGIS 10.2 software. The overall Hospitalisation Rate per FSA was calculated by dividing the total number of unique admissions in OMRHS for all age groups within each FSA by the 2011 population count (all ages). Two hospital accessibility variables were created: 1) General Hospitals with mental health units, and 2) Psychiatric Hospitals based on 10 specialty hospitals in Ontario. The hospital accessibility variables were assigned to each FSA based on the distance between the centroid of each FSA and the closest psychiatric hospital or general hospital with psychiatric beds. This measure is suited for urban and rural settings, and has been used in previous Ontario studies. 15 The hospital addresses were available from the CIHI.
Area-level marginalization was based on the Ontario Marginalization Index (ON-Marg). 16 Indicators included residential instability, material deprivation, dependency, and ethnic concentration. Indicators were scored between 0 and 1, where lower scores indicate less marginalization. The FSA scores were calculated by taking the weighted average of census tract scores within each FSA, as recommended in the ON-Marg user manual. 17
Statistical Analysis
We performed spatial regression analysis at the FSA level. Across most FSAs, there were low counts of inpatient psychiatric admissions for older adults with cognitive disorders. Therefore, we used a Bayesian approach, which borrows information from neighbouring areas to smooth out estimates of risk for areas that have low counts. 18 A spatial Poisson regression model with a convolution prior estimated the relative risk of admission among older adults with cognitive disorders. To identify potential risk factors, we included marginalization indicators and the 2 variables of hospital accessibility in the regression model while controlling for hospitalisation rate (included as a covariate). We used WinBUGS software to fit the model. Technical analytic details are available in the online supplementary file.
Results
Table 1 shows descriptive statistics for the sample of adults with cognitive disorders and aggregated descriptive statistics across the FSAs. The average patient with a cognitive disorder was 70 y old. Just over 50% had a previous admission to an inpatient psychiatric unit, with about 10% having 6 or more admissions. Approximately 58% of patients were admitted from locations other than their private residence, 71% were admitted to an acute psychiatric unit, and 20% were admitted to a designated geriatric unit. On average, patients had moderate to severe impairments in cognitive performance (mean [SD] CPS, 2.7 [1.8]), were at moderate to high levels of risk of harm to others (mean [SD] RHO, 2.6 [2.1]), and were experiencing positive symptoms (mean [SD] PSS, 2.4 [2.8]), and depressive symptoms (mean [SD] DSI, 2.8 [3.0]). The average stay for patients with cognitive disorders was 60 d; although, stays varied considerably across unique admissions.
Descriptive Characteristics of Adults with Cognitive Disorders Admitted to Inpatient Psychiatry in Ontario between January 1, 2011 and December 31, 2014.
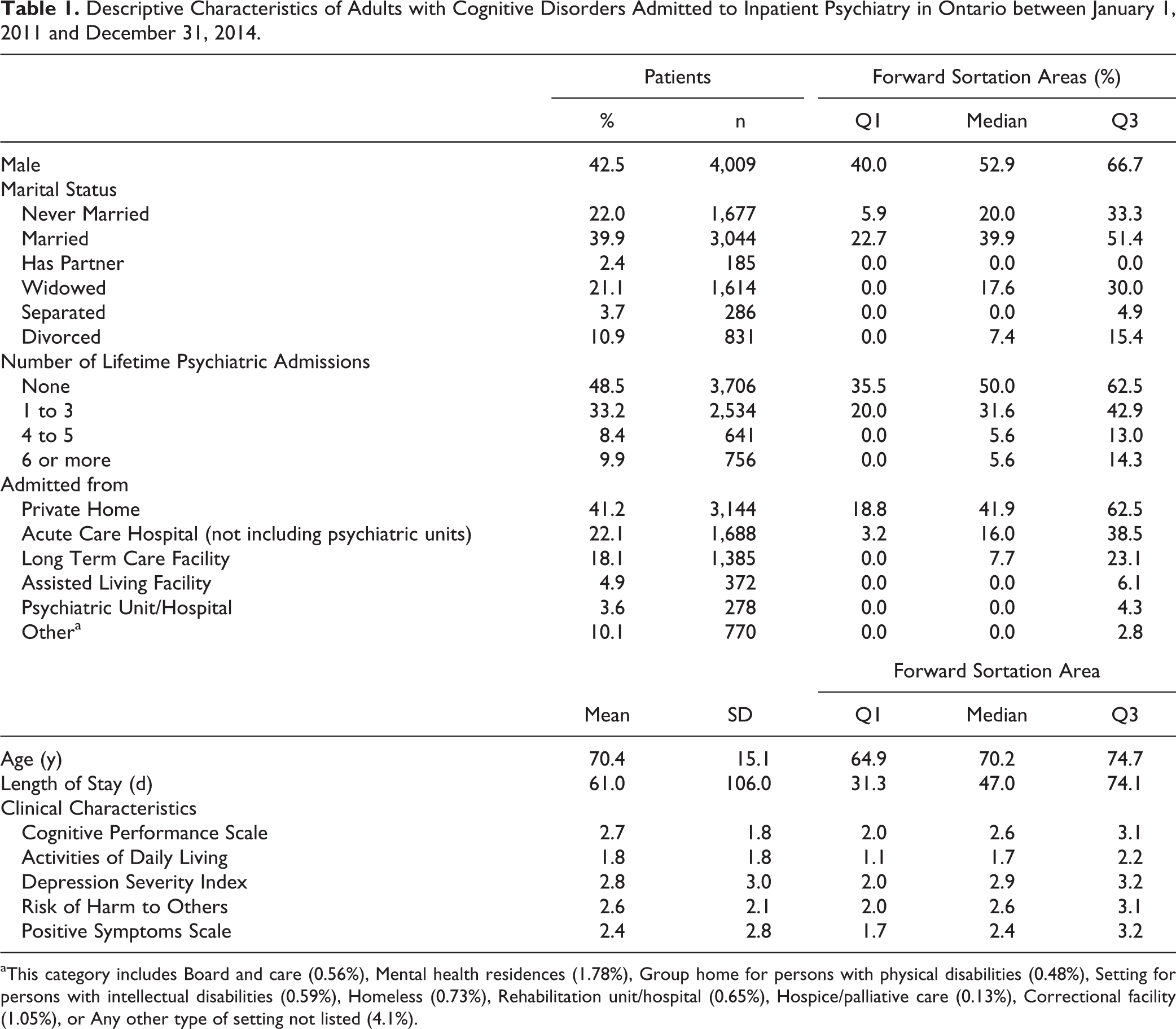
aThis category includes Board and care (0.56%), Mental health residences (1.78%), Group home for persons with physical disabilities (0.48%), Setting for persons with intellectual disabilities (0.59%), Homeless (0.73%), Rehabilitation unit/hospital (0.65%), Hospice/palliative care (0.13%), Correctional facility (1.05%), or Any other type of setting not listed (4.1%).
Ecological Variables associated with Clustering
In the multivariate analyses (Table 2), residential instability and the overall hospitalisation rate were significantly and positively associated with the relative risk of admission at the 95% credible interval (CrI). Associations among the 3 other indicators of marginalization (material deprivation, dependency, and ethnic concentration) were not significant. Significant negative associations were identified between each hospital accessibility variable in models that included only one type of hospital; this was interpreted as the greater the distance to general hospitals (Model 1) or psychiatric hospitals (Model 2), the lower the relative risk of hospitalisation within an FSA or the lower the use of inpatient psychiatric services. When entered simultaneously in Model 3 and Model 4, the negative associations diminished (marginally became insignificant at the 95% CrI). Exclusion of the overall hospitalisation rate did not change the significance of hospital supply (Model 4).
Bayesian Spatial Poisson Regression Results of the Association between Geographic Characteristics and Risk of Psychiatric Admission for Dementia.
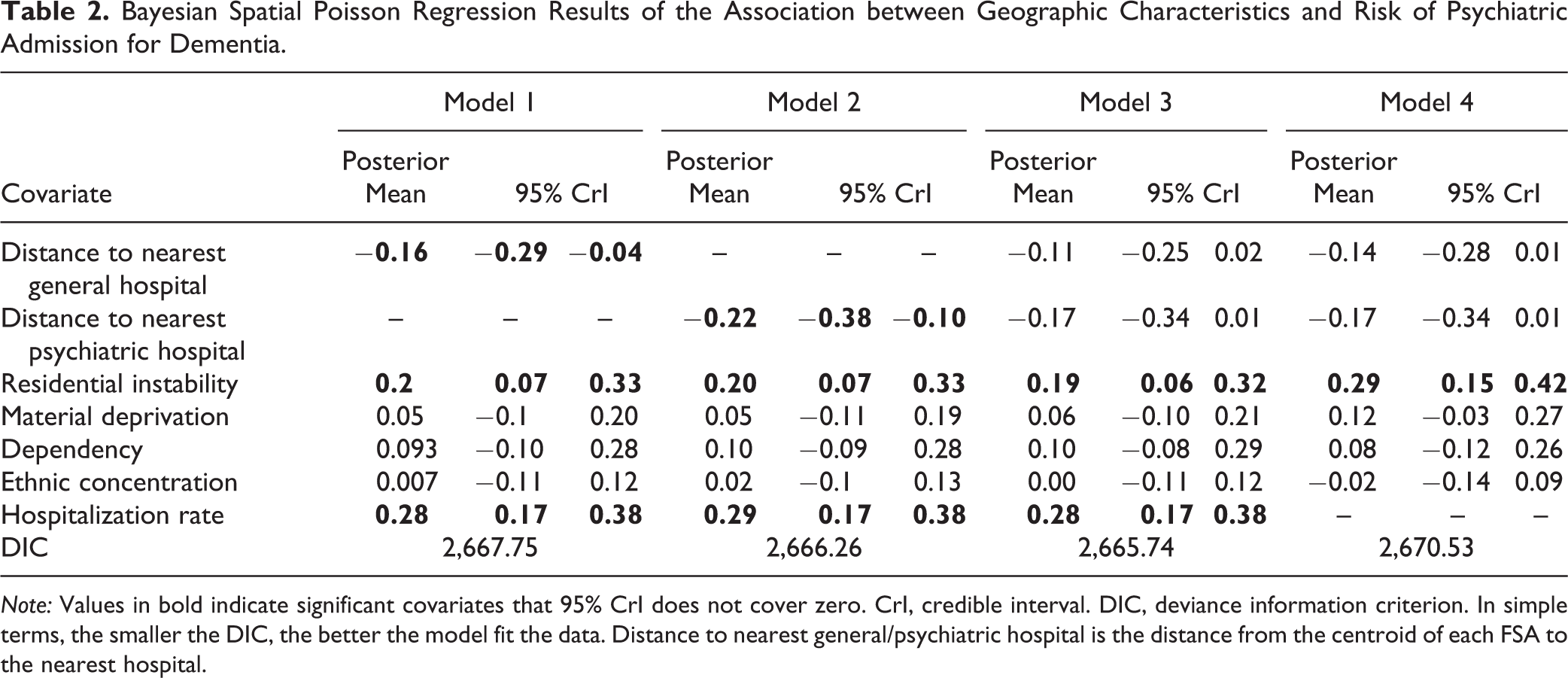
Note: Values in bold indicate significant covariates that 95% CrI does not cover zero. CrI, credible interval. DIC, deviance information criterion. In simple terms, the smaller the DIC, the better the model fit the data. Distance to nearest general/psychiatric hospital is the distance from the centroid of each FSA to the nearest hospital.
Are Psychiatric Admissions Geographically Clustered?
Figure 1 shows the relative risk of admission in persons with a cognitive disorder by all FSAs in Ontario, as well as the greater Toronto area after controlling for marginalization, distance to the closest hospital, and hospitalisation rate. Individuals residing in FSAs with the highest relative risk were 2.0 to 7.1 times more likely to be admitted than the average.
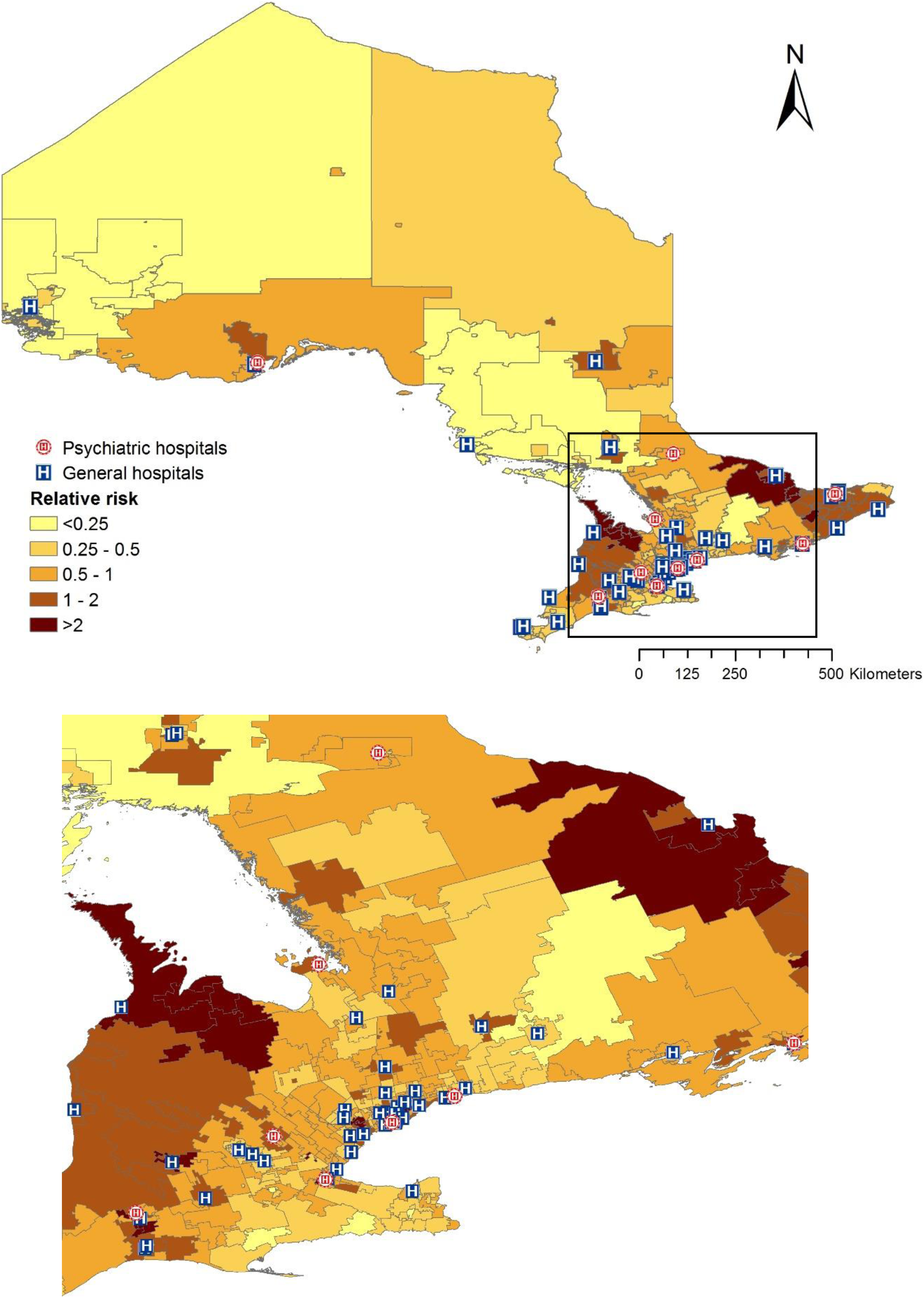
Estimated geographical variation in relative risk of admission to inpatient psychiatry among adults with cognitive disorders at the FSA level in Ontario, Canada. [Source of FSA map: Statistics Canada, 2017]. Note: Boxed area represents the Greater Toronto Area, which has been amplified.
Discussion
Admissions to inpatient psychiatric units among adults with cognitive disorders were geographically clustered across Ontario. The relative risk was particularly high for a subset of FSAs, where individuals were more than twice as likely to be admitted than in other areas. Studies have found proximity to services are related to increased utilisation. 19,20 However, our results suggest that hospital accessibility may not be associated with the relative risk of admission in adults with cognitive disorders. Residential instability, representative of areas with higher rates of isolation, and segregated built environments composed of concentrated dwellings were positively associated with admissions to inpatient psychiatry. Adults with cognitive disorders in these areas may have less informal support or engagement. This aligns with findings at the individual level, whereby being single was found to predict repeat admissions in acute geriatric psychiatry services. 21
These findings have implications for psychiatric care and the support of adults with cognitive disorders. Inequities may exist in the availability of formal and informal community supports for vulnerable adults, particularly those who reside in areas where social isolation is high. For instance, Ismail and colleagues 22 found that physical pain and medical comorbidities among patients with dementia predicted shorter lengths of stay within a specialized geriatric psychiatry service in Ontario. They suggest that earlier intervention for these conditions may prevent the exacerbation of behavioural and psychological symptoms of dementia and reduce the need for an inpatient psychiatry admission. This may be the case for the 22% of patients in our sample who were admitted from non-psychiatric acute hospitals. Our results may also indicate a need for more specialized inpatient psychiatry services, particularly given the high prevalence of admissions to acute psychiatry units in this sample.
Our study had several limitations. First, the FSA was highly variable in size and population across the Province, which may have potentially affected the homogeneity of the geographic context. Second, this study could not standardize the clustering based on the population of adults with cognitive disorders within each FSA. Instead, it was assumed the at-risk population was equally distributed, whereby areas with a higher proportion of adults aged 65 y or over would also have a larger proportion of persons with cognitive disorders. This also limited our ability to perform multi-level spatial analyses to control for differences in case-mix when studying the effects of geographic context. Third, no information on the health or social service supply per geographic unit was examined. Given that the clustering of admissions within Ontario may not be related to hospital accessibility, future research should examine if clustering is related to other factors, such as the supply of geriatric psychiatry services and resource programs.
Conclusion
Geographic clustering of inpatient psychiatry admissions for older adults with cognitive disorders exists across the Province of Ontario, Canada. The risk of admission was positively associated with residential instability and the overall hospitalisation rate, but not distance to the closest general or psychiatric hospital. Spatial analysis presents an approach to understand how geographic context and health system supply relate to patterns of service utilisation.
Statement of Access to Data
The OMHRS and hospital address data can be accessed by request to the Canadian Institute for Health Information using the following link: https://www.cihi.ca/en/access-data-and-reports/make-a-data-request. In making such a request the specific topic to request would be “Inpatient admissions to designated mental health services in Ontario”. The ON-Marg data are available online: http://www.torontohealthprofiles.ca/onmarg.php#userGD
Supplementary Material
Supplemental_File - Geographic Clustering of Admissions to Inpatient Psychiatry among Adults with Cognitive Disorders in Ontario, Canada: Does Distance to Hospital Matter?
Supplemental_File for Geographic Clustering of Admissions to Inpatient Psychiatry among Adults with Cognitive Disorders in Ontario, Canada: Does Distance to Hospital Matter? by Christopher M. Perlman, Jane Law, Hui Luan, Sebastian Rios, Dallas Seitz, and Paul Stolee in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We thank interRAI Canada and the Canadian Institute for Health Information for the collection and management of the RAI-MH data used in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Network for Aging Research Seed Grant provided by the University of Waterloo.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.