
Abstract
Objectives:
Mental health is a key area for learning within undergraduate medical education. Given the nature of mental illness, interactions may have the potential to uniquely affect patients. This study set out to systematically review studies reporting experiences and perceptions of patients with mental illness’ clinical interactions with medical students. This includes which factors encourage patients to interact with medical students and if patients perceive negative and positive effects from these interactions.
Method:
Studies reporting patient experiences of involvement in undergraduate medicine were included. A standardised search of online databases was carried out independently by 2 authors and consensus reached on the inclusion of studies. Data extraction and quality assessment were also completed independently, after which a content analysis of interventions was conducted and key themes extracted. Studies were included from peer-reviewed journals, in any language.
Results:
Eight studies from 5 countries were included, totaling 1088 patients. Most patients regarded interacting with medical students as a positive experience. Patients described feeling comfortable with medical students, and the majority believed it is important for students to ‘see real patients’. Patients described benefits to them as enjoyment, being involved in student education, and developing an illness narrative.
Conclusions:
Results suggest that most patients with mental illness want to interact with medical students, and this should be encouraged during student placements. Further research, however, is required to understand in more depth what else can be done to improve the comfort and willingness for patients to interact with students, including barriers to this.
Given that quality and safety of medical care are dependent on the education of medical students, 1 it is important to understand how patients experience the interaction with medical students. Experiential learning is an important, evidence-based part of undergraduate medical development, 2 and interaction with patients remains a requirement in order that medical students learn and develop. Learning occurs by observing and reflecting on experiences, then forming abstract concepts and generalisations based on reflections, and finally testing the concepts in new situations. 3 Medical students can interact with patients at 4 progressive levels: passive observer, active observer, actor in rehearsal, and actor in performance. 4,5 The progression through these levels occurs as students become more senior, which is imperative to an evolving sense of participation and contributing to ongoing learning and development. 5 Learning is enhanced when the student experience of participation is simultaneously challenging and supportive, 4 –6 such as increasing independence alongside quality supervision. 6 Workplace experience, including patient interaction, promotes the development of professional identity, 7 as well as the skills and knowledge required for clinical practice.
With respect to mental illness, it is regrettable that medical students can sometimes experience discouragement from clinical staff when interacting with patients, including in psychiatry placements. It is important to understand this further given the importance of experiential learning, as patients are potentially vulnerable, and medical student attitudes towards psychiatry 8,9 and people with mental illness 10 may be negative and stigmatising, compared to physical illness. Negative attitudes towards mental illness may become increasingly apparent as students progress through medical school, 10 and such negative attitudes can become harmful. 11 It is of particular interest to understand how patients experience interaction with medical students. By definition, the interaction between patients and students is a dyadic process, and whilst the literature exploring the effects of experiential and workplace learning richly describes the perspective of medical students, 12 it is equally important to understand the perspective of patients. There is a professional duty to understand the experience of patients for clinical reasons, but this information is also of undoubted value in improving the educational quality of the interaction.
We investigated the experiences of patients with mental illness with respect to clinical interactions with medical students, addressing 2 key objectives. First, we explored the nature of the experiences of interacting with medical students. This included which factors encourage or discourage patients to interact with medical students (Descriptive). Second, we explored whether patients with mental illness perceived contact with medical students as having positive or negative outcomes, either for themselves or the students (Justification). 13
Methods
We sought to understand the impact of interacting with medical students on patients with mental illness and how patients perceive this interaction as affecting the students. Whilst this work is not directly situated within an educational environment, the focus is within the context of medical education, and the review has been reported in line with the methodology of the Best Evidence Medical Education Collaborative 14 and STORIES guidelines. 15
As each patient can reasonably be expected to experience interactions with medical students differently, an absolute single truth as to this experience is not possible. Instead, we wanted to establish a ‘probable’ truth, 16 aligning with a research paradigm of postpositivism 16,17 supporting evidence-informed translation to practice of the results. 18 Ethical review was not sought as it is not required for systematic reviews.
All study designs were considered for this review, as long as they reported experiences and attitudes of patients involved with medical students. For the purpose of this review, experience was defined as observations made through contact with medical students; perception as the way in which patients regard, understand, feel, or interpret interaction with medical students; view as a particular way of considering or regarding medical students; attitude as an established way of thinking, feeling about, and behaving towards medical students; and opinion as a judgement formed about medical students.
We accepted studies with any patient with mental illness aged 18 or over who had interacted with medical students for the purpose of an assessment. All settings were acceptable, such as inpatients and outpatients, and all psychiatric diagnoses were included. Studies needed to include empirical data for selection with respect to patient experience, perceptions, views, attitudes, or opinions on either (a) how patients believed/felt clinical interactions with medical students affected them or other patients and/or (b) how patients believed/felt students’ interaction with ‘real’ patients affected medical students. We excluded studies that explored medical students’ experiences/views, health care professionals’ experiences/views, and health care students who were not medical students.
Commentary pieces, audits, and review articles were not included. We excluded from this review studies exploring the experiences of patients whose primary diagnosis was not a mental illness and the experiences of ‘professional’ patients (patients who are trained to provide specific interactions for students with specific objectives, for example, in an examination), the medical students themselves, simulated patients, or involvement of patients who have had any medical education training. The focus was the experiences of patients with mental illness who were interacting with medical students in the ‘real’ clinical environment (i.e., an assessment by a medical student). We included any empirical studies but excluded opinion pieces. Studies from all countries published in all languages were included. There was no time limit on the search.
We ran the following exploded search terms combination using Boolean operations in July 2017: [psychiatr* OR ‘mental’ OR Patient OR Patients OR ‘service user*’] AND [‘medical student*’ OR ‘student*’] AND [experience* OR Attitude OR Attitudes OR Opinion OR Opinions OR View OR Views OR perception*]. The databases searched using these terms were Medline and PsycInfo. A grey literature search was not performed due to resource limitations, but hand searching of selected article references was performed.
Citations were reviewed independently by each of the authors. Potentially relevant abstracts were independently reviewed and full papers obtained for any studies that appeared to meet the inclusion criteria. Disputes were resolved by consensus. The full manuscripts for all included studies were assessed independently by 3 of the authors.
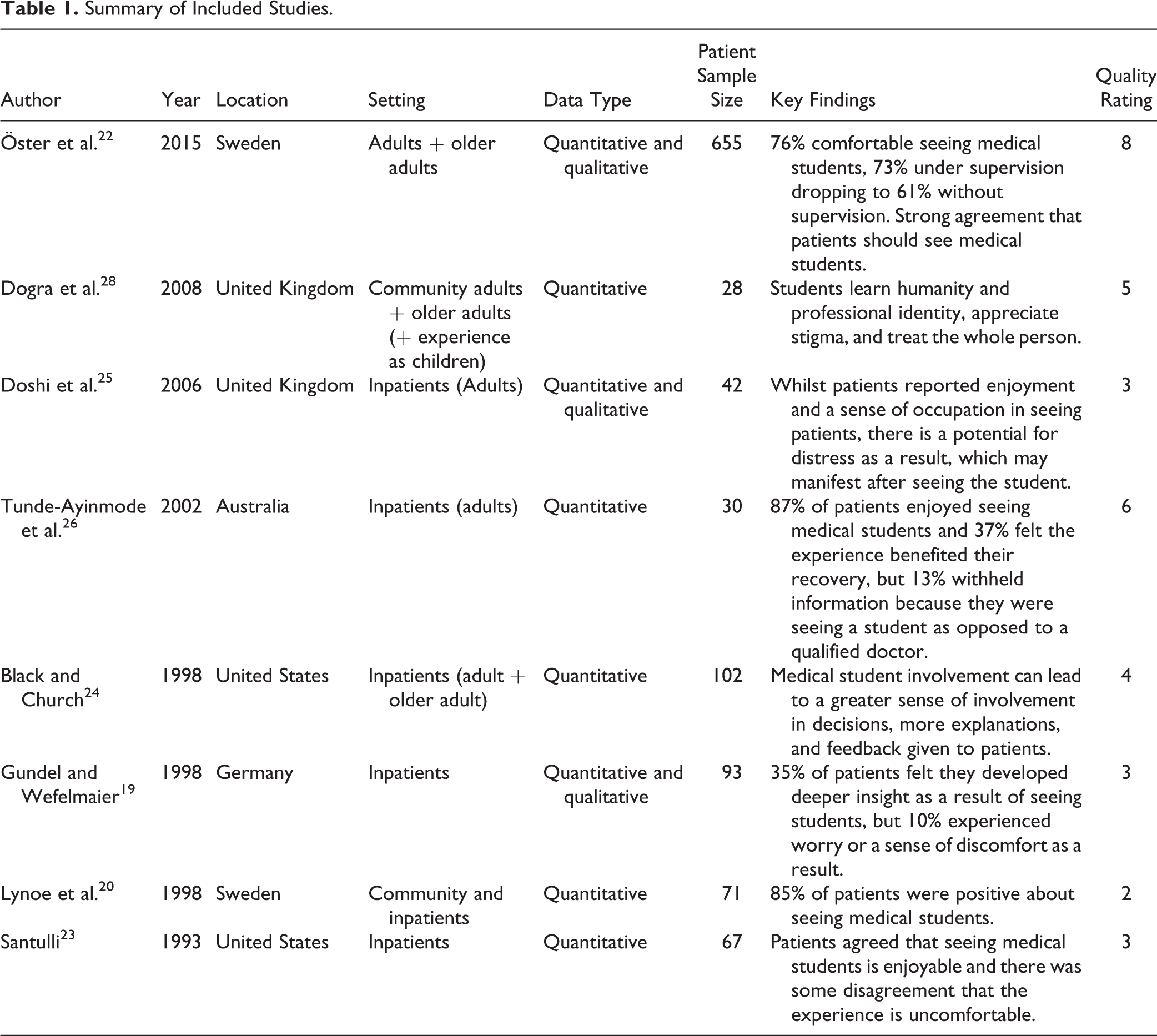
A data extraction summary was completed for each selected study. The descriptive data included study setting, sample size, country, year of study, methods and measures, key findings and outcomes, and study limitations. Given the nature of the objectives, the data were analysed using a descriptive and narrative approach. We assessed quality of the studies by scoring 5 key areas: student sample defined, patient sample defined, the study design is appropriate to answer the research question, implementation of the methods, and appropriateness of the analysis. For each of these 5 items, a score was applied where 0 = no, 1 = to some extent, and 2 = yes. Therefore, the maximum quality score was 10, and minimum was 0. The quality scores for each study are provided in Table 1.
Summary of Included Studies.
Results
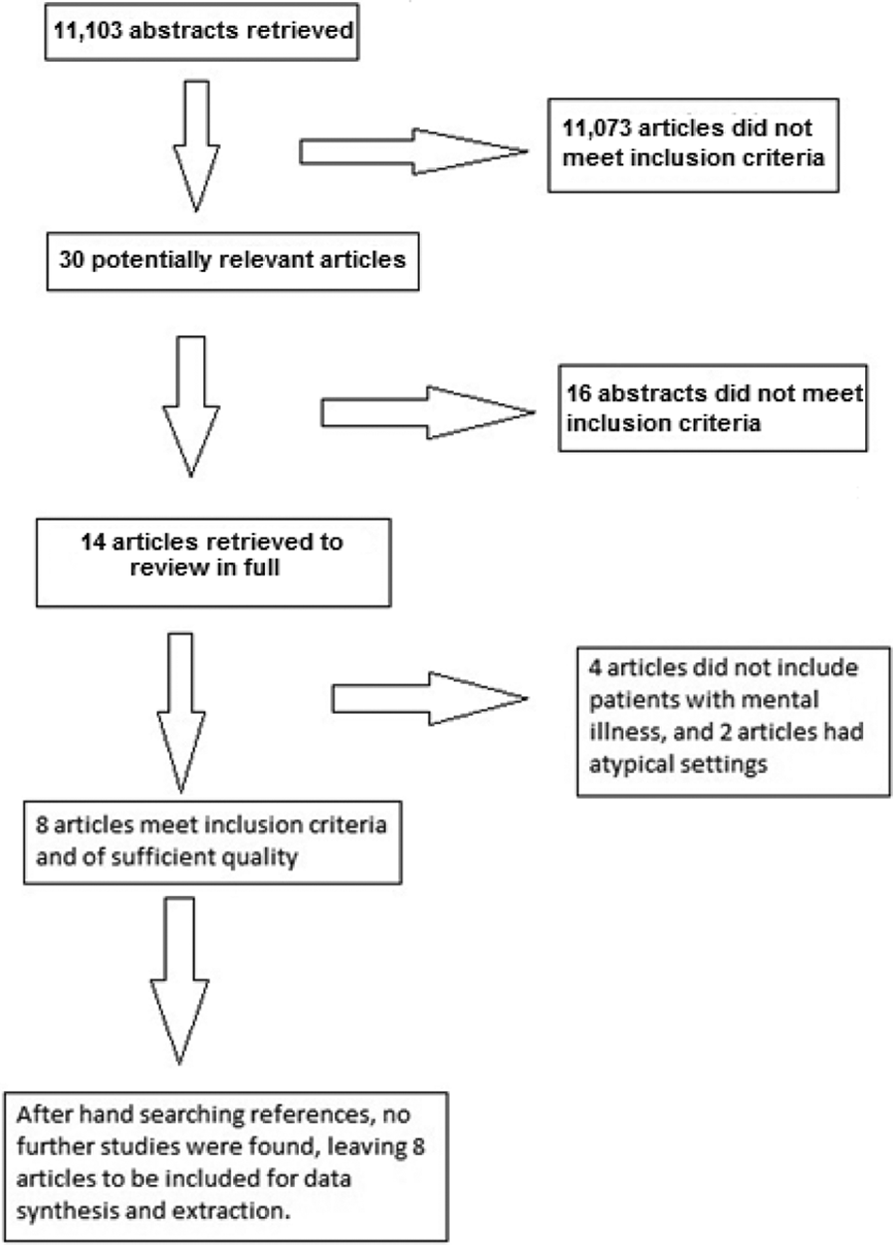
There were 11,103 potentially relevant citations retrieved through searching. Of these, 30 articles were identified as potentially relevant and abstracts were reviewed. After review of these studies, 16 were excluded as they did not meet the inclusion criteria. For 4 further studies, it was unclear if they included patients with mental illness. After communications were made with the authors, these 4 studies were excluded as no patients with mental illness were included. This left 10 articles that met the inclusion criteria. 19 –28 However, 2 of these 10 studies were excluded as they involved patients in primary care, 21 and another study described idiosyncratic practice, which is not transferable to most clinical or educational environments. 27 This left 8 studies included for data extraction and synthesis. No further articles were found as a result of hand searching of references (Figure 1). A total of 1088 patients from 5 different countries were included in the accepted studies for the data extraction and synthesis. None of the studies were conducted in Canada.
Articles found meeting search criteria.
Table 1 summarises the included studies. All studies used questionnaires/surveys with Likert scales plus open-ended questions, except that by Dogra et al., 28 which was a qualitative study using focus groups. The surveys used by Lynoe et al. 20 and Santulli 23 did not use open-ended questions. Black and Church 24 also included qualitative analysis of interviews with patients, with a mean length of interview of 5 minutes.
Nature of the Experiences of Interacting with Medical Students from the Patients’ Perspective
A ‘positive’ experience of being assessed by medical students was described by 60% 19 and 85% 20 of patients, with 1 study finding that 97% of patients experienced interactions with students as ‘valuable’. 21 Öster et al. 22 found strong agreement from patients that they should have clinical interaction with medical students, an opinion with which patients were more likely to agree with if they had previously interacted with a medical student (mean of 4.53 on a 5-point Likert scale) than not (mean of 4.34), P = 0.024.
Öster et al. 22 found that 76% of patients felt ‘comfortable’ interacting with medical students and that inpatients and outpatients were equally ‘comfortable’. In this study, reported comfort reduced slightly when the degree of supervision was specified, dropping from 73% under supervision to 61% without. In the same study, male and female patients were equally comfortable with female students, but female patients were comparatively less comfortable with male students (mean reported comfort level reduced from 3.89 to 3.38 on 5-point Likert scales). Female patients were less comfortable interacting with ‘younger’ medical students than male patients, with means of 3.14 and 3.47, respectively, P = 0.01. When provided with statements in terms of discomfort, Santulli 23 found patients generally disagreed (mean of 2.49 on a 5-point Likert scale) that interacting with medical students was an uncomfortable experience.
Two studies referred to how the patients experienced the medical students as professionals. Santulli 23 found agreement from patients that students were ‘kind’, with a mean of 4.51 on a 5-point Likert scale. Black and Church 24 found strong agreement that students were ‘warm and caring’ (mean of 4.59 on a 5-point Likert scale) as well as reporting disagreement that they felt ‘talked down to’ (mean of 1.57) or that interacting with medical students felt ‘unnatural’ (mean of 1.63).
Four studies explored patients’ willingness to interact with medical students again in the future. Santulli 23 found agreement that patients are willing to interact with medical students again in the future (mean of 4.31). Rates of willingness to interact with medical students again were reported in 3 other studies, with rates reported at 91%, 21 79%, 25 and 70%. 26
Three studies reported on consent. Doshi et al. 25 reported that 30% did not feel they received an appropriate explanation as to the student’s task, but 93% of patients felt they had been properly consented; Tunde-Ayinmode 26 reported this at 83%. Lynoe et al. 20 did not report on consent rates but found that 40% of patients stated that they would interact with medical students if put ‘under duress’.
Öster et al. 22 qualitatively explored patients’ wishes when interacting with medical students. They found that patients wanted prior notice about age, gender, seniority of students, and clarity as to the purpose of interacting with the students.
Patients’ Perception of Positive and Negative Outcomes from Interacting with Medical Students
Regarding positive outcomes, 2 studies reported rates of ‘enjoyment’ of patients interacting with medical students at 56% 27 and 87%. 26 Santulli 23 found that patients typically agreed that student interviews were enjoyable (mean of 3.95 on a 5-point Likert scale). Black and Church 24 found that as a result of interacting with medical students, 89.7% of patients felt that the medical students were helpful to their overall treatment, as well as patients agreeing they experienced greater explanations about their treatment (mean of 4.11), involvement in decisions about their care (mean of 3.94), and useful answers to their questions (mean of 4.26). Tunde-Ayinmode et al. 26 found that 37% of patients felt that interacting with patients aided their recovery. Gundel and Wefelmaier 19 found that 35% of patients reported deeper insight into their illnesses and 24.5% felt they had learnt about themselves. While these numbers appear low for sense of recovery, deeper insight, and learning about themselves, the remainder of patients did not notice any change in these domains, suggesting this may be a benefit for some patients only. Interacting with medical students did not negatively affect these domains. However, Öster et al. 22 found that patients were neutral (mean of 3.33) about whether interaction with students improved quality of care.
Qualitative results described patients feeling they benefited from student interactions by being the provider of learning, 26 enjoyment, 22,25 and having a sense of occupation. 25
Patients perceived positive outcomes not only for themselves but for the medical students also. Tunde-Ayinmode et al. 26 reported that 83% of patients felt students’ learning was ‘enhanced’ by interacting with ‘real’ patients, with a similar finding by Doshi et al., 25 where the mean score on a 6-point Likert scale was 5.01 on a scale of agreement with the statement ‘seeing real patients is valuable training for medical students’.
From qualitative data, Doshi et al. 25 found that patients felt interacting with medical students ‘helps them [students] learn’ and makes medical students ‘good doctors’. Öster et al. 22 found that patients felt students learned aspects of empathy and professionalism. Dogra et al. 28 found that patients felt that students learned about ‘humanity’ and the ‘whole person’ as well as developing a sense of ‘professional identity’. They also suggested that students benefited as the experience reduces stigma and engenders an attitude of ‘hope’ and ‘recovery’.
Four studies reported on dissatisfaction experienced by patients. Gundel and Wefelmaier 19 reported 10% of patients describing the experience as ‘unpleasant’ and ‘uncomfortable’. Öster et al. 22 found that nearly 25% of patients were ‘not comfortable’ interacting with students. Tunde-Ayinmode et al. 26 found that 23% of patients were ‘worried’ about interacting with medical students, and 13% of patients felt that interacting with medical students was a ‘waste of time’. It is concerning that 53% of patients saw students because they did not want care to be compromised, and 13% withheld clinical information because they were being assessed by medical students. 26 Doshi et al. 25 reported that 12% of patients felt that they could not decline interactions with students, 21% said they could not terminate interviews, and 14% felt that such interviews were not confidential. Doshi et al. 25 also explored the chronology of anxiety that patients experienced; they found that 11% were ‘nervous’ at the prospect of being asked to interact with a medical student (although this reduced over time), and 21% became distressed during the interview and 7% after the interview had concluded. None of these studies attempted to establish why some patients had these negative experiences or opinions.
Discussion
The published evidence demonstrates that the experience of most patients with mental illness is positive when interacting with medical students. The students were similarly described in a positive light, seen as caring, kind, and competent, and most patients would interact with medical students again. This is similar to the experiences of patients with physical illness when interacting with medical students, who also found students to be ‘polite’ and ‘kind’. 29 This trend continues when patients interact with first- and second-year medical students, with almost all patients very satisfied with the encounter and 85% prepared to interact with students again. 30 These findings seem to be consistent regardless of the physical health specialty the patients are being treated in. 31
The evidence suggests patients benefit from interacting with medical students, ranging from a sense of occupation, being a provider of learning, and feeling more involved in their own care. Patients also described improved self-esteem and insights, although the level of agreement for this appears weaker. Studies exploring the perceptions of patients with physical illness interacting with medical students have found that patients feel that the quality of care improves, when comparing a hospital before and after the introduction of medical students. 32,33 Interestingly, patients with physical illness perceived the care they received from physicians improved following the introduction of medical students to a hospital in domains such as friendliness, competence, and time spent with patients. 32
The data from the studies reviewed suggest that most patients feel strongly that they should interact with students for a variety of reasons. This would appear to counter the position often encountered in clinical practice that patients with mental illness are often felt as ‘unsuitable’ for clinical interaction with medical students. This review suggests that most people with mental illness can and should interact with medical students. There is less evidence from patients with mental illness that interacting with medical students directly improves quality of care in terms of health outcomes, but the subjective experience of care does appear to improve.
The literature also suggests there are potential negative outcomes for patients, although on a lower order of magnitude than positive outcomes. For example, about one-fifth of patients will not be comfortable interacting with medical students. This appears to relate to feelings of vulnerability such as fear of loss of confidentiality, not being able to decline, and inconvenience. It is notable that in primary care, nearly 70% of patients seeing their general practitioner for a mental health problem do not believe the quality of their care will be positively affected if a medical student is involved, contrary to those patients with physical illness in the hospital setting. 32 In physical health patient populations, the level of perceived negative outcomes appears dependent on the setting; for example, there were no perceived negative outcomes in a study in the United States, 30 while non-Caucasian populations in the United Kingdom were twice as likely to feel uncomfortable interacting with medical students as the Caucasian population. 34 In Kuwait, 20% to 25% of patients felt uncomfortable enough to refuse student participation. 35 For people with mental illness receiving care in Canada, the literature has yet to explore experiences of clinical interactions with medical students, and whilst findings from the United States and Europe are likely to be at least partially transferable, further confirmatory research is required.
Although not a specific objective of this systematic review, it is encouraging that the results serve to challenge stigma against those with mental health problems in a number of ways. Patients with mental health problems appear equally willing to engage with medical students compared to patients with physical health problems. Patients with mental health problems should not be automatically viewed as frail and not able to interact with students; in fact, a number of benefits are described. It is also important to note that patients themselves report that interacting with medical students positively affects attitude formation of tomorrow’s doctors and reduces stigma.
There is less evidence in terms of patients’ perceptions of benefits to students. However, in the small number of studies in this review that consider this, most patients view interacting with medical students as an enhancement to learning. Patients appear to view this benefit in terms of learning of empathy and humanity, as well as developing professionalism and professional identity. Encouragingly, patients with mental illness have also reported that interacting with medical students promotes a sense of hope and the possibility of recovery.
Lessons for improved practice in medical education can be drawn from these findings. It is useful for those tasked with managing student placement numbers that within the population of patients, around 4 in 5 patients will consent to see medical students, and thus the educational capacity of the services can be better understood and patients not be overwhelmed. More detailed educational improvements can be made when noting the clear and recurrent theme in use of language in both qualitative and quantitative studies, that of ‘comfort’ of patients in relation to interacting with medical students. This appears to be the preferred term or outcome. This being the case, effort should be made jointly between clinical services and medical education departments to have policies and procedures in place that aim to ensure the comfort of their patients. The aim should be to promote and increase levels of comfort. More specifically, 3 points of good practice are suggested. Firstly, patients should be provided with specific information as to the reported benefits of seeing medical students. Secondly, specific patient briefings occur prior to interacting with medical students and should include the purpose of their interaction, the level of supervision being provided, the number of students, student gender(s), and year of study. Lastly, specific support should be available during interview and afterwards, being mindful of the reported potential for delayed distress.
Strengths and Limitations
This study captures the known international body of evidence, without limits on language or date of study followed by a robust approach to selection, quality assessment, and data extraction. The resulting synthesis supports clinical interactions between medical students and people with mental illness. Therefore, this study provides a foundation to challenge any practice that is discouraging medical students from interacting with people with mental illness. This study also supports any psychiatrist who wants to incorporate medical students’ involvement in enhancing patient care.
The foremost limitation of this study arises by virtue of the nature of the primary evidence base. The majority of studies described summary descriptive statistics of Likert scales or alternatively individual comments or responses. There were no studies that undertook a deeper clarification analysis, 14 aiming to generate new theory or conceptual frameworks to aid understanding in this area. Such understanding could further explore the experiences of patients that have been raised as well as the mechanisms of positive or negative outcomes that have been synthesised. There may be a response bias in the primary research, with patients who have enjoyed or benefited from interaction with students being more likely to participate in the studies. Additionally, a lack of precision as to the terms of the metrics being considered in the primary studies is likely to put limits on what can be concluded. Although as a part of this review, we defined our terms relating to patients’ experiences and views, this was not seen in the primary literature, and in many cases, terms appear to be used somewhat interchangeably. Due to resource limitations, a variety of search terms in different combinations was not used but may have uncovered further literature, given the nature of the terms used.
A range of patients from different settings has contributed to the studies considered. Universally, the description of the patients themselves was quite limited and did not extend to the details of their current diagnoses, for example. As such, this review can conclude that, at the level of care setting, most patients are comfortable interacting with medical students and report positive experiences and benefits, but there can be no comment as to variation by other factors such as the effect of suffering from a particular mental health problem.
Conclusions
This review suggests that most patients with mental illness have positive experiences interacting with medical students and report perceived benefits to themselves and to students. Patients are more likely to be willing to interact with medical students than not, but it is important to enhance the patient experience through proper consent, which includes informing patients of the student’s gender, year of study, task expected of the student, and level of supervision the student will be receiving. This may contribute to increasing the number of patients who have a positive experience interacting with students. However, future research is required to understand what barriers patients perceive to interacting with students and what aspects of the interaction enhance the experience. This includes exploring the effects of diagnosis on this experience.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.