
Abstract
Objective:
Despite recent advances in neuroscience highlighting its potential applications in the assessment and treatment of psychiatric disorders, the training of psychiatrists in neuroscience is lacking. However, it is not clear to what extent Canadian trainees are interested in further learning and using neuroscience in their daily clinical practice. This study explored the attitudes of Canadian psychiatry trainees with regard to neuroscience education and training by asking them to assess their own understanding of neuroscience and the perceived relevance of neuroscience knowledge to effective psychiatric practice.
Methods:
An online questionnaire was sent to psychiatry residents at Canadian universities. This questionnaire consisted of self-assessments of neuroscience knowledge, attitudes toward neuroscience education, preferences in learning modalities, and interest in specific neuroscience topics.
Results:
One hundred and eleven psychiatry residents from psychiatry residency programs at Canadian universities responded to this survey. Participants represented trainees from all 5 years of residency. Almost half of all trainees (49.0%) reported their knowledge of neuroscience to be either “inadequate” or “less than adequate,” and only 14.7% of trainees reported that they feel “comfortable” or “very comfortable” discussing neuroscience findings with their patients. 63.7% of Canadian trainees rated the quantity of neuroscience education in their residency program as either less than adequate or inadequate, and 46.1% rated the quality of their neuroscience education as “poor” or “very poor.” The vast majority of participants (>70%) felt that additional neuroscience education would be moderately-to-hugely helpful in finding personalized treatments, discovering future treatments, destigmatizing patients with psychiatric illness, and understanding mental illness.
Conclusions:
Canadian trainees generally feel that their neuroscience knowledge and the neuroscience education they receive during their psychiatry residencies is inadequate. However, as the first step for any change, the majority of future Canadian psychiatrists are very motivated and have a positive attitude toward neuroscience learning.
Introduction
Neuroscience represents the broad discipline that is the study of the nervous system. Investigations in this field cover a wide scope and involve a variety of techniques and specialties, from genetics to in vitro cellular recording to animal models to functional brain mapping. 1 Over the past few decades, revolutionary new methods and approaches in neuroscience have improved our ability to understand the biological basis of many psychiatric disorders and spurred the development and implementation of novel therapeutic strategies. For example, immunohistochemical and electrophysiological techniques have helped elucidate the mechanisms underlying anti-NMDA receptor encephalitis, an autoimmune disorder with prominent psychiatric symptoms 2 ; functional imaging and network connectivity analyses continue to enhance our understanding of the dysfunctional neural circuitry underlying major depressive disorder, guiding the growing use of noninvasive brain stimulation interventions 3,4 ; and epigenetic studies have increased our understanding of the complex interaction of genetic, environmental, and experiential factors that influence the development of addictive behavior. 5,6
Advances in neuroscience offer a new framework of explanation for psychiatric illnesses and allow for a changing dialogue between clinicians and patients regarding the etiology and treatment of psychiatric disorders. However, the rising integration of neuroscience into psychiatry has not come without its warnings. For example, there is an ongoing debate as to the extent to which framing psychiatric disorders and associated maladaptive behaviors in the context of brain disease is helpful for patients. 7 –9 Additionally, despite the tremendous advances in neuroscience research in recent decades, arguments abound as to whether these neurobiological discoveries are sufficiently characterized as to have a practical impact on patient care. 10 –12 These cautions notwithstanding, the fact remains that neuroscience research is in ascendency, and the field of psychiatry will only become further inundated with neuroscience knowledge as time goes on. If psychiatrists are to have the ability to critically evaluate and synthesize neuroscience findings as they arise and determine whether new information can be incorporated into their practice, they require the tools to effectively navigate this neuro-psychiatric landscape. 13,14
Despite rapid growth in neuroscience research and an ever-increasing overlap between neurology, neuroscience, and psychiatry, there remains a large gap between neuroscience knowledge and psychiatrists’ day-to-day practice. 10,15,16 This gap may be due to a number of factors: a lack of exposure to neuroscience education during residency training, low motivation or a negative attitude toward learning neuroscience, or the aforementioned perception that there is little clinical relevance toward neuroscience knowledge in patient care. In 2014, a survey study by Fung and colleagues showed that 94% of psychiatry trainees in the United States endorsed the need for more neuroscience training, and 70% felt that advances in neuroscience would lead to the discovery of new treatments or personalized medicine in the next 5 to 10 years. 17
In this study, we conducted a similar study to Fung and colleagues focused on the attitudes and perceptions of Canadian psychiatry trainees with regard to neuroscience knowledge and education. More specifically, we wanted to know how psychiatry trainees assess their own understanding of neuroscience and how much they believe in the relevance of neuroscience knowledge to effective psychiatric practice. There are a number of differences between American and Canadian psychiatry training programs that warrant a separate investigation into the attitudes of Canadian trainees. Specifically, Canadian trainees undergo a longer program with more extensive training in psychotherapy compared to their American counterparts. 18,19 Furthermore, American training places a greater emphasis on competency in physical and neurological examinations relative to mental status examination. 20,21 These factors may play a role in alienating Canadian trainees from their background training in medicine and neurobiology.
The training of psychiatrists in neuroscience lags behind advances in neuroscience research, and finding the best ways to incorporate neuroscience teaching into the psychiatry field remains a challenge for mental health-care providers. 14 Understanding trainees’ attitudes and willingness to learn neuroscience is an important step in the successful adaptation of Canadian residency programs to train future competent and up-to-date psychiatrists.
Methods
This study was approved by the University of Manitoba’s Research Ethics Board. All participants were shown a Consent Disclosure Statement prior to filling out the survey. Participants’ subsequent willingness to complete the survey was considered receipt of their informed consent. No self-identifying information could be entered by participants, and the survey system did not record participants’ e-mail or IP addresses.
Survey
A 43-question survey was constructed using the Kirkpatrick evaluation model.
22
The full questionnaire is provided as Supplemental File 1. Aside from some minor wording changes, this study replicated all of the questions asked of American trainees in a 2014 paper by Fung and colleagues
17
with the exception of one question evaluating interest in taking a 3-day course in the neuroscience of psychiatry. In addition to collecting basic demographic information, Fung and colleagues designed the survey using categorical response items to capture three main themes:
Attitudes of psychiatry residents toward neuroscience education during residency training. These questions examined residents’ perceived usefulness of neuroscience education in understanding mental illness, decreasing stigma, and aiding the discovery of future or personalized treatments. Questions also explored the perceived difficulty of learning neuroscience versus psychotherapy and residents’ interest in learning specific domains of neuroscience.
Assessment of degree of knowledge of psychiatry and neuroscience. This was assessed through a self-evaluation of extent of knowledge of both psychotherapy and neuroscience and their clinical applications, perceived quality of education, and residents’ and their attendings’ comfort levels discussing neuroscience findings with their patients.
Methods to improve neuroscience education in psychiatry residency training as viewed by residents. This was explored by assessing the perceived usefulness of different methods of learning neuroscience as well as the perceived importance of teaching different domains of neuroscience.
An online survey was created and hosted using the Survey Monkey website. An invitation e-mail with a link to the web-based survey was sent to all psychiatry residents via the program administrator for the psychiatry department of each of 14 English-language Canadian universities. The survey remained active for 90 days. To improve response rates, two e-mail reminders were sent to potential participants at 30-day intervals following the initial invitation. The number of residents at each university was between 1 and 60, with an estimated total of 500 psychiatry residents. Based on previous similar survey studies, we anticipated a 20% response rate for a total of roughly 100 responders.
Statistical Analysis
Data analysis was performed using Systat 13.0 software (Systat Software Inc., San Jose, CA). Two-sample t tests were used to compare basic demographic information. Descriptive statistics (percentages) were used to illustrate respondents’ self-assessed knowledge, appraisal of their education, attitudes toward neuroscience, and preferences for various learning modalities and neuroscience domains.
Survey responses were given numerical values on a continuous scale based on the level of agreement/interest/perceived value for the given statement/learning modality/so on selected by the respondent. For example, for the question asking respondents to indicate the usefulness of “journal clubs” in learning neuroscience, responses were coded as 0, 1, 2, 3, and 4 for the selections “least helpful,” “somewhat helpful,” “moderately helpful,” “very helpful,” and “most helpful,” respectively. Gender and seniority were included as factors in our analysis, with seniority categorized as either junior (postgraduate year [PGY] 1–2) or senior (PGY 3–5). A multivariate analysis of variance (MANOVA) was performed comparing each survey item across gender (male vs. female) and seniority (junior vs. senior). Individual items within each model were then compared using an analysis of variance (ANOVA) if either the Pillai’s trace or Wilks’ lambda was significant for the respective MANOVA. The significance level for the MANOVAs was set a P < 0.05 for seniority and at a less stringent P < 0.10 for gender. Individual-item ANOVAs were considered significant at P < 0.05.
Results
Characteristics of Respondents
One hundred and eleven trainees from psychiatry residency programs at Canadian universities responded to the survey from December 2016 to February 2017 giving an estimated response rate of roughly 22% of all Canadian psychiatry residents. Table 1 outlines the demographic information of the survey respondents. Seventy-seven respondents represented eight separate Canadian universities, while the remaining 34 respondents chose not to identify their host institution. Participants represented trainees from all 5 years of residency: 28 participants in PGY1, 26 participants in PGY2, 20 participants in PGY3, 28 participants in PGY4, and 8 participants in PGY5 (1 participant did not respond to this question and was excluded from seniority analyses). Junior and senior residents did not differ significantly in proportion of females, anticipated scope of practice, or expectation of future teaching involvement (P > 0.05 for all comparisons).
Characteristics of Psychiatry Resident Survey Respondents.
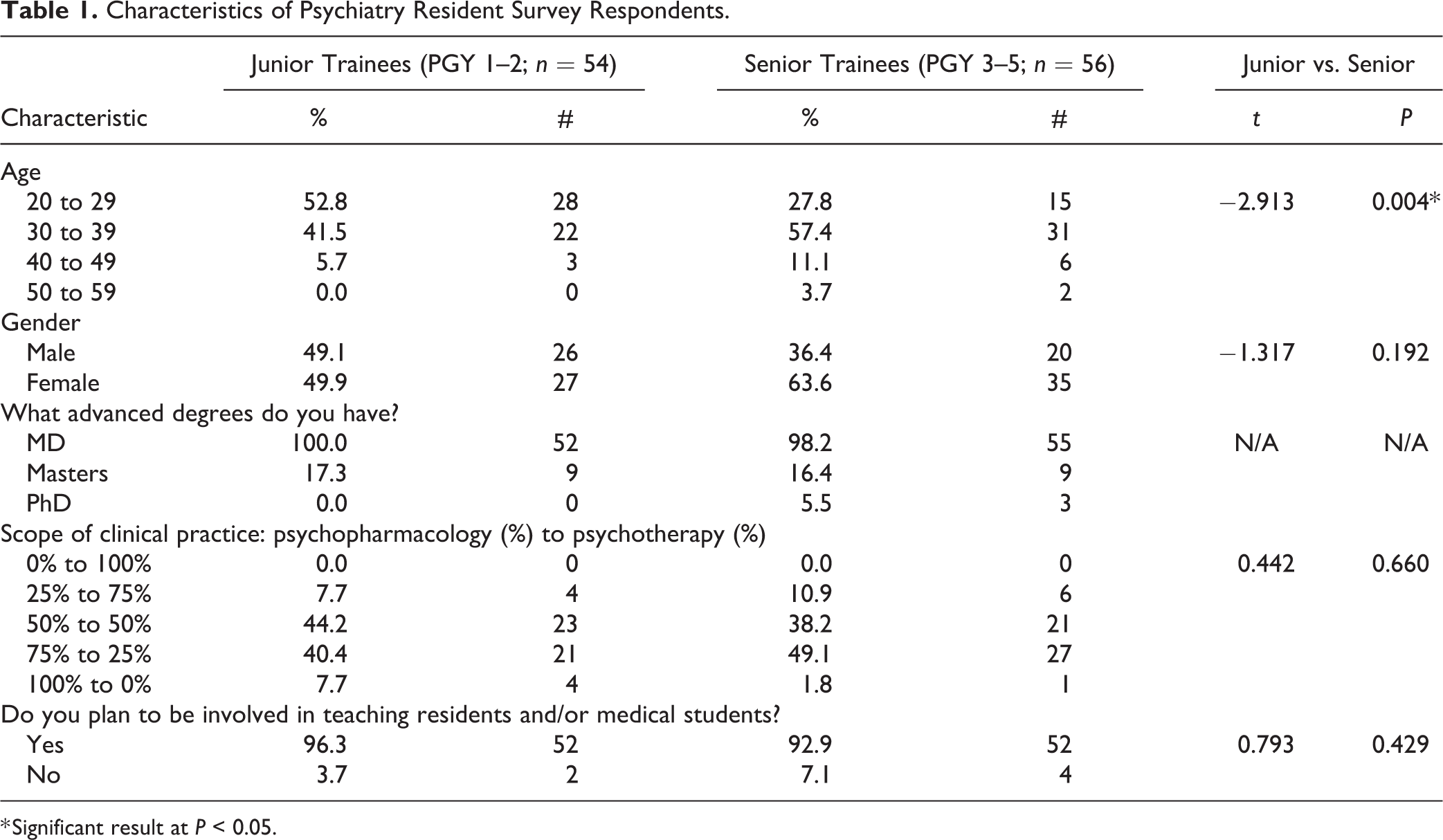
* Significant result at P < 0.05.
Half of the respondents (50.0%) anticipated that their scope of practice would encompass mostly psychopharmacology (i.e., 75% to 100% psychopharmacology) while only 9.3% predicted that their practice would be mainly psychotherapy (i.e., 75% to 100% psychotherapy). Most respondents (94.6%) planned to be involved in teaching residents and/or medical students at some point in the future.
Self-Assessed Knowledge
Almost half of all trainees (49.0%) reported their knowledge of neuroscience to be either “inadequate” or “less than adequate,” and there was no difference in self-rated neuroscience knowledge between junior and senior trainees (F = 2.595, P = 0.111; Table 2). In comparison, only 18.6% of trainees reported their knowledge of psychotherapy to be inadequate or less than adequate, with senior trainees rating their psychotherapy knowledge more highly than junior trainees (F = 20.205, P < 0.001). There was no difference in reported neuroscience (F = 0.420, P = 0.519) or psychotherapy (F = 0.528, P = 0.469) knowledge between males and females.
Self-Assessed Knowledge.
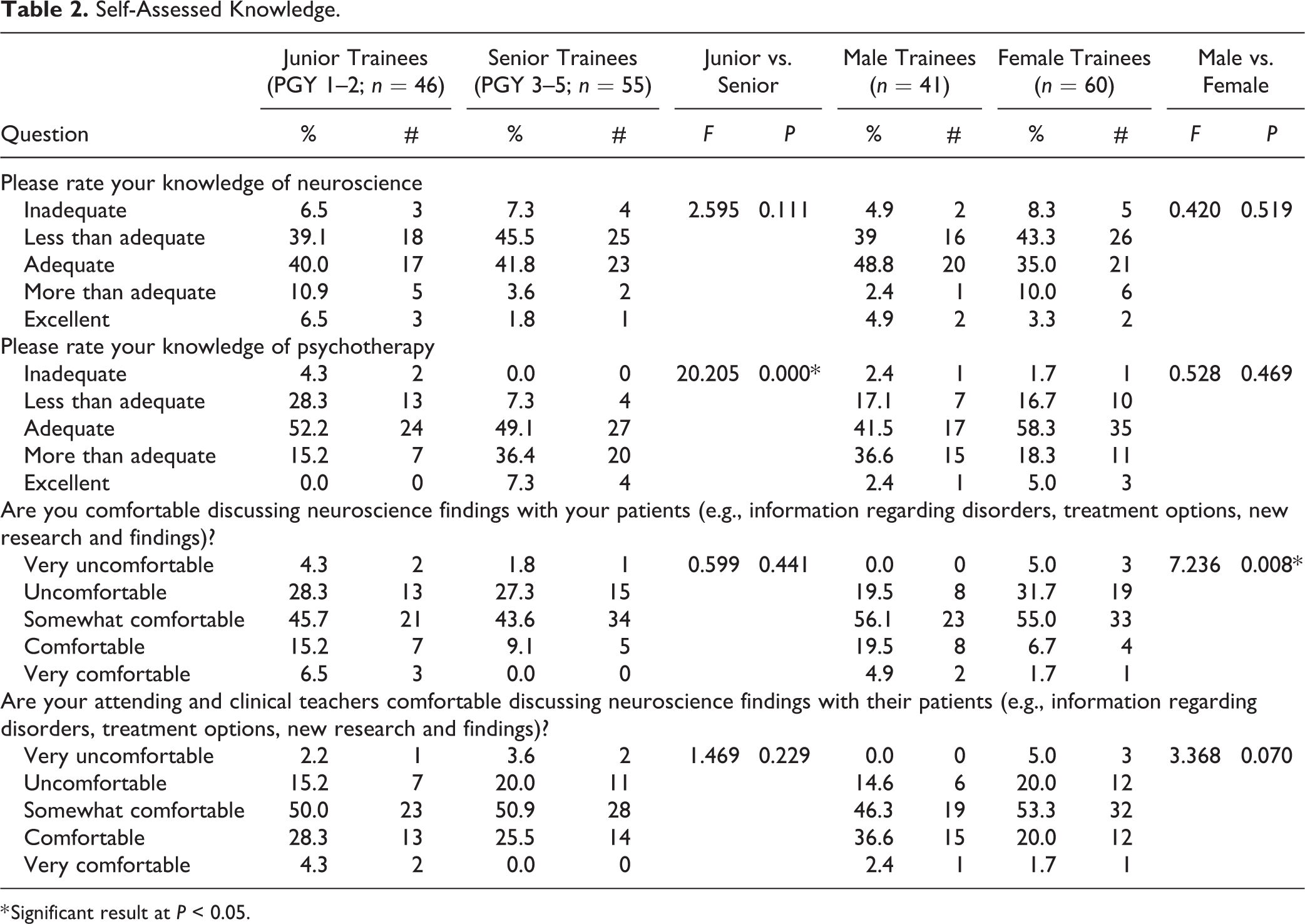
* Significant result at P < 0.05.
Only 14.7% of trainees reported that they feel comfortable or very comfortable discussing neuroscience findings (e.g., information regarding disorders, treatment options, new research and findings) with their patients, and only 28.4% rated their attending supervisors as being comfortable or very comfortable discussing neuroscience findings with their patients. There was no difference by seniority in either trainees’ self-rated comfort (F = 0.599, P = 0.441) or their perceived attendings’ comfort (F = 1.469, P = 0.229). However, males expressed a higher level of comfort in discussing neuroscience than females (F = 7.236, P = 0.008).
Assessment of Neuroscience Education
A total of 63.7% of trainees rated the quantity of neuroscience education in their residency program as either less than adequate or inadequate (Table 3). With regard to the quality of the neuroscience education they did receive, almost half of trainees (46.1%) rated their residency programs as either “poor” or “very poor,” with only 6.9% of trainees rating the quality of their neuroscience education as “above average” or “excellent.” There was no difference by seniority (quantity: F = 0.767, P = 0.384; quality: F = 1.278, P = 0.261) or gender (quantity: F = 0.170, P = 0.681; quality: F = 0.219, P = 0.641) on either of these measures.
Assessment of Education.
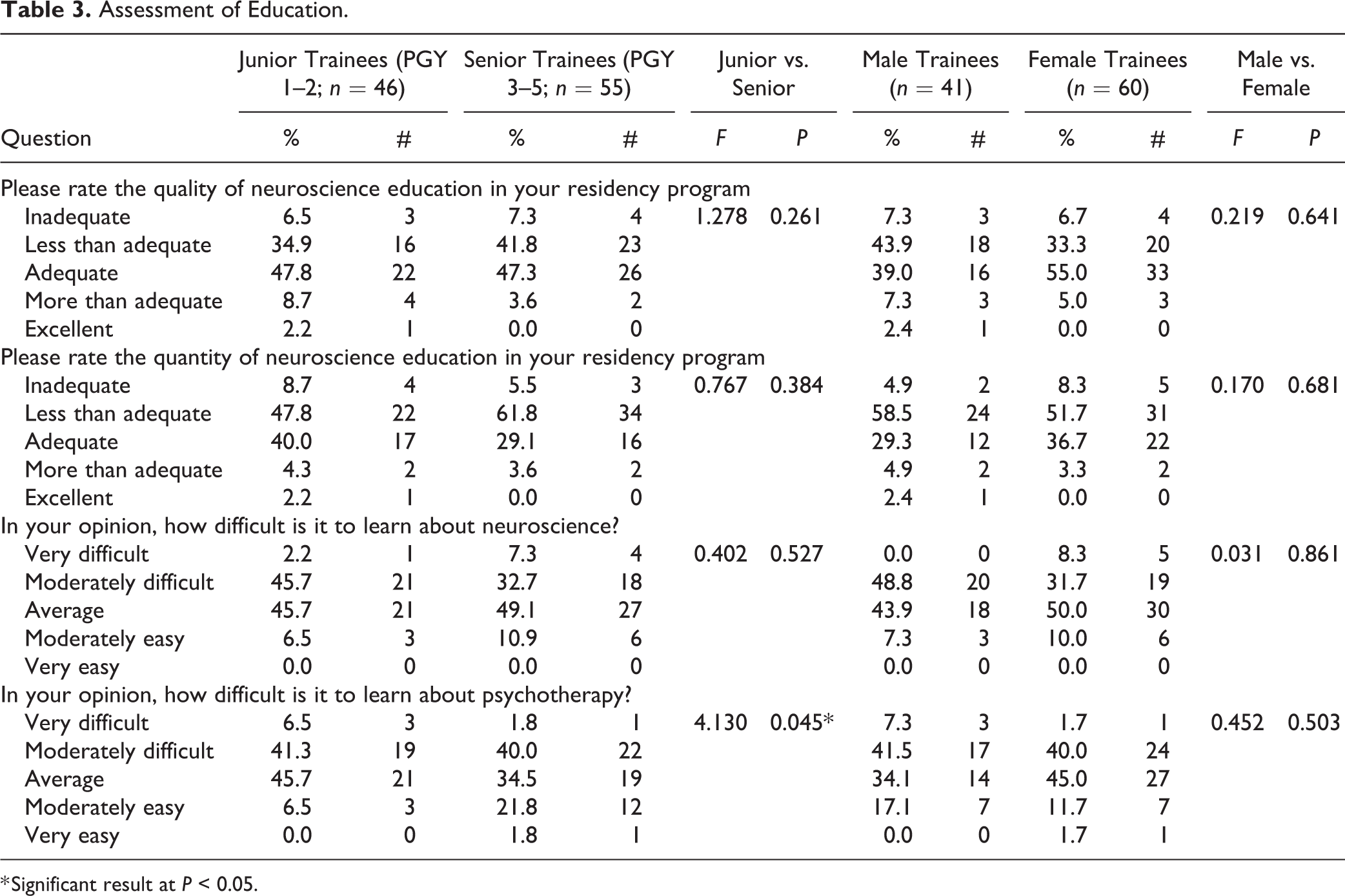
* Significant result at P < 0.05.
Respondents felt that neuroscience and psychotherapy were similarly challenging subjects to learn, with 43.1% of trainees rating neuroscience as either moderately or very difficult to learn and 44.1% rating psychotherapy as moderately or very difficult to learn. Seniors rated psychotherapy as more difficult to learn than juniors (F = 4.130, P = 0.045), but there was no difference by seniority in rating the perceived difficulty to learn neuroscience (F = 0.402, P = 0.527). Males and females reported no difference in their perceived difficulty to learn neuroscience (F = 0.031, P = 0.861) or psychotherapy (F = 0.452, P = 0.503).
Attitudes toward Neuroscience Education in Psychiatry
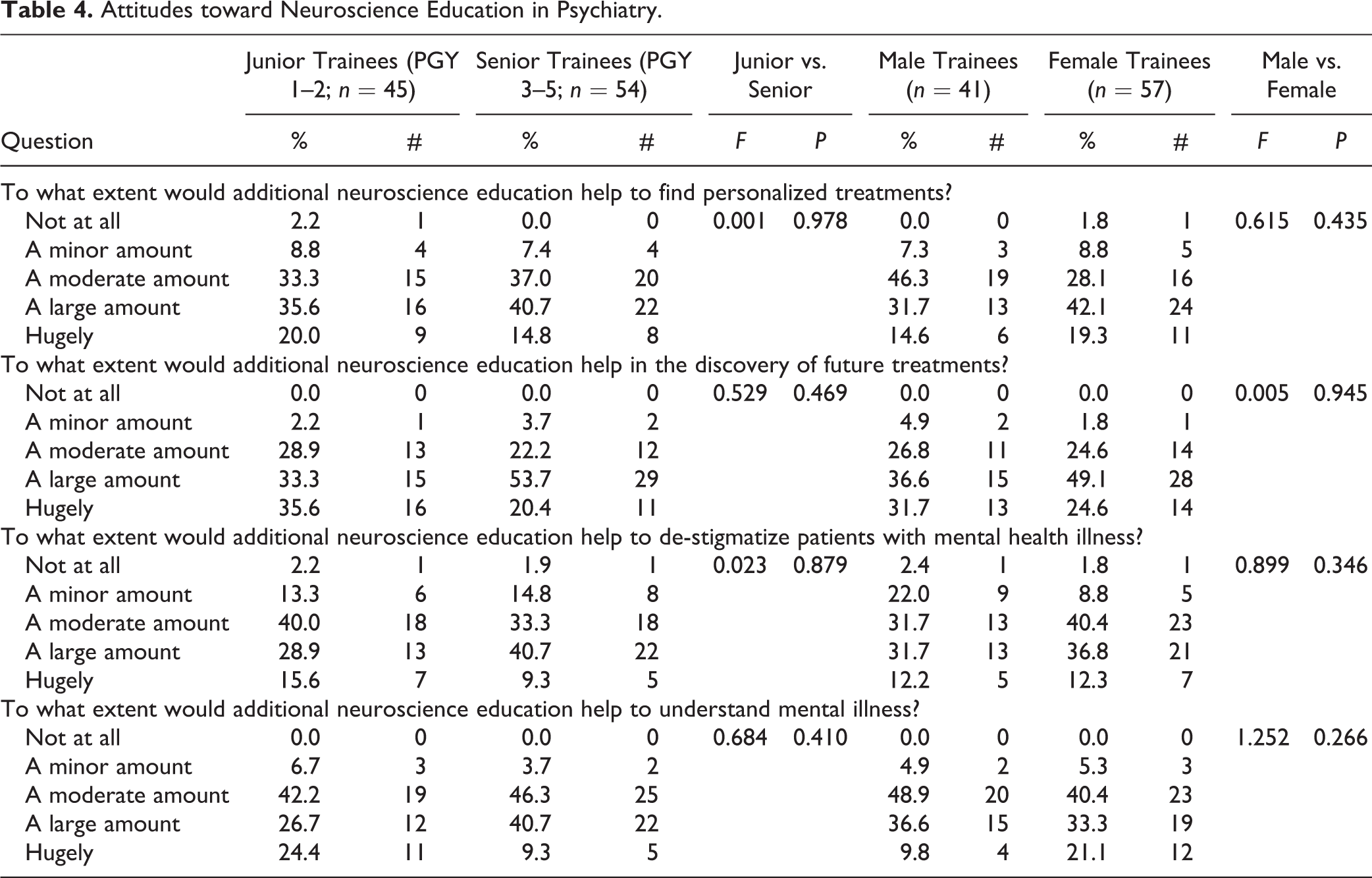
Regarding the perceived usefulness of neuroscience education, 90.9% of participants felt that additional neuroscience education would be either moderately (35.4%) or largely to hugely (55.6%) helpful in finding personalized treatments; 96.9% of participants felt that additional neuroscience education would be moderately (25.3%) or largely to hugely (71.7%) helpful in the discovery of future treatments; 83.8% of participants felt that additional neuroscience education would be moderately (36.4%) or largely to hugely (47.5%) helpful in destigmatizing patients with psychiatric illness; and 94.9% of participants felt that additional neuroscience education would be moderately (44.4%) or largely to hugely (50.5%) helpful in understanding mental illness (Table 4). There was no difference in the perceived usefulness of neuroscience education by gender or trainee seniority (P > 0.05 for all comparisons).
Attitudes toward Neuroscience Education in Psychiatry.
Preference for Neuroscience Learning Modalities
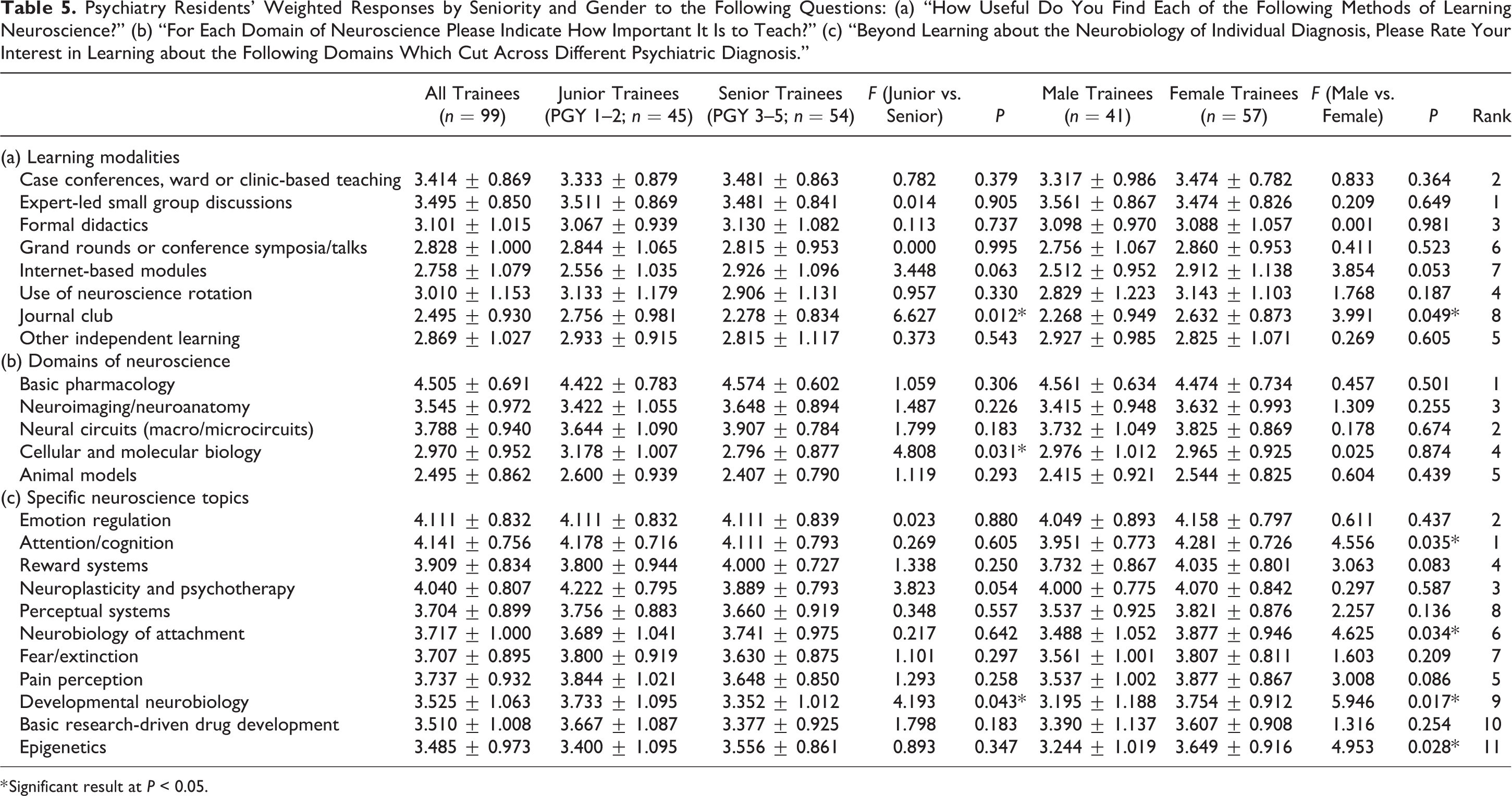
Overall, trainees rated “expert-led small group discussions” as the most useful means of learning neuroscience followed by “case conferences, ward, or clinic-based teaching” (Table 5). Journal clubs were rated as the least useful method of neuroscience education, followed by “internet modules.” Junior trainees rated journal clubs as more useful than seniors (F = 6.627, P = 0.012), and females rated the usefulness of journal clubs (F = 3.991, P = 0.049) more highly than males. There were no other differences by seniority or gender on the rated usefulness of other neuroscience learning modalities (P > 0.05 for all comparisons).
Psychiatry Residents’ Weighted Responses by Seniority and Gender to the Following Questions: (a) “How Useful Do You Find Each of the Following Methods of Learning Neuroscience?” (b) “For Each Domain of Neuroscience Please Indicate How Important It Is to Teach?” (c) “Beyond Learning about the Neurobiology of Individual Diagnosis, Please Rate Your Interest in Learning about the Following Domains Which Cut Across Different Psychiatric Diagnosis.”
* Significant result at P < 0.05.
Domains of Neuroscience and Specific Neuroscience Topics
Trainees reported “basic pharmacology” to be the most important domain of neuroscience to be taught, with “animal models” being the least important (Table 5). Junior trainees rated “cellular and molecular biology” as being more important than seniors (F = 4.808, P = 0.031). There was no difference in opinion between male and female respondents (P > 0.05 for all comparisons).
With regard to specific neuroscience topics, trainees showed the most interest in learning about “attention/cognition,” “emotion regulation,” and “neuroplasticity and psychotherapy.” The least amount of interest was shown toward “epigenetics,” “basic research-driven drug development,” and “developmental neurobiology.” Females demonstrated a higher interest in learning about the following topics compared to males: attention/cognition (F = 4.556, P = 0.035), “neurobiology of attachment” (F = 4.625, P = 0.034), developmental neurobiology (F = 5.946, P = 0.017), and epigenetics (F = 4.953, P = 0.028). Junior trainees expressed a higher interest in developmental neurobiology compared to seniors (F = 4.193, P = 0.043).
Discussion
This study reveals that a significant percentage of Canadian psychiatry residents rate the quality (46.1%) and quantity (63.7%) of neuroscience training in their residency programs poorly, and very few Canadian residents (14.7%) feel comfortable discussing neuroscience findings with their patients. Junior and senior residents report no difference in their comfort discussing neuroscience findings, and senior residents do not report a higher neuroscience knowledge than juniors, implying that psychiatry residency programs are failing to improve residents’ neuroscience competency as they progress through their training. Despite this, the majority of residents hold a very positive view toward neuroscience and the potential benefits of neuroscience education in psychiatry, endorsing the view that additional neuroscience education would help delineate personalized treatments, discover future treatments, destigmatize patients with psychiatric illness, and understand mental illness. Thus, Canadian trainees recognize a gap in their neuroscience training and consider neuroscience education useful in patient care, an opinion shared by psychiatry trainees and program directors in other countries. 17,23
A number of authors have proposed methods of improving neuroscience education in psychiatry residency training, 14 –16,24,25 and various programs are already being developed to improve neuroscience education for psychiatry trainees and psychiatrists, including the National Neuroscience Curriculum Initiative in the United States and the Royal College of Psychiatrists in the United Kingdom. Although most residency directors appreciate the importance of integrating neuroscience into psychiatry training, 23 most programs still do not teach neuroscience in a systematic and comprehensive manner. Benjamin and colleagues discuss potential reasons for this mismatch, such as neuroscience training not being mandatory by accreditation agencies, a lack of expert neuroscience teachers, and the complexity of neuroscience research making it more intimidating and distant from concrete clinical skills. 23 In our survey, formal didactic training was highly rated by respondents, suggesting a desire among residents for well-programmed learning. Introducing mandatory neuroscience didactics could be a necessary first step in expanding neuroscience education in psychiatry programs, although care must be taken not to overburden trainees who are already working through a substantial curriculum. 26
Improving the quality of neuroscience education is as important as increasing its quantity. This was illustrated by Roffman and colleagues in 2006 through a survey of North American residents and fellows, which found that despite increases in the amount of neuroscience teaching over the previous 5 years, results were disappointing regarding competency in interpreting scientific findings. 27 The challenge of keeping up with the rapidly developing and complex field of neuroscience has been speculated to be a resistance factor in embracing additional neuroscience education. 10 Residents in our survey rated expert-led small group discussion as their overall preferred method for learning neuroscience, demonstrating the value that they place on tutoring by highly knowledgeable instructors. Recruiting more qualified tutors with a background in both neuroscience and clinical psychiatry could improve the delivery of more tangible and applicable neuroscience materials. Indeed, previous authors have highlighted the importance of skilled educators with the ability to incorporate neuroscience data into patient formulations and the ability to communicate effectively with a lay audience. 23 Thus, the limited availability of competent teachers is a potential challenge to the successful implementation of quality neuroscience education. 13,23 In that frame, collaboration and partnership between scientific communities, educators, and clinicians is fundamental for successful and clinically meaningful delivery of neuroscience to trainees.
It is widely accepted that attitude is a critical first step in the quest for change, although it is important to remember that there is not a perfect correlation between attitude and behavior. 28 As such, positive feelings toward additional neuroscience education do not necessarily guarantee that enforced changes to residency curricula will be well received by future trainees. Nonetheless, “a negative attitude toward neuroscience” has been previously presented as an obstacle that may impede the integration of neuroscience education in psychiatry training, 14 and the present results work to at least assuage that concern.
Previous publications have discussed the positive social impacts that can result from neuroscience advancements, 29,30 and it is anticipated that increasing neuroscience research and education will largely result in an improvement in the understanding of mental disorders. 31 –33 However, it is important to point out that well-reasoned arguments have also been presented regarding the potential downfalls of framing mental illness purely in the context of brain disease. 7,9 For example, there is a growing body of evidence demonstrating that framing mental illness in a biological context doesn’t necessarily reduce stigma and can in fact have a negative impact on the public perception of psychiatric illness. 9,34 –36 However, providing psychiatry residents with an improved neuroscience education does not preclude other teachings, nor does it necessarily minimize the proven strengths of psychological and social therapeutic interventions nor the relevance of social and environmental factors in the development of mental disorders. Rather, improved neuroscience teaching could give psychiatrists the tools to interpret novel neurobiological findings that may shed light on the etiology of certain disorders and to better evaluate and select from the available therapies for their individual patients. Enhanced neuroscience education would help psychiatrists not only to embrace but also to be critical of neuroscience research, enabling them to appropriately evaluate the significance and applicability of novel findings. As Traicu and Joober recently argued, it is important for clinicians to maintain a healthy skepticism regarding the integration of neuroscience and psychiatry by maintaining an awareness of the limitations of our current models. 12 Arming trainees with a solid understanding of basic neuroscience principles as well as a critical eye for methodology and statistics could prevent psychiatrists from being overly seduced by new discoveries and more realistic about the practical implications of novel neuroscience findings in the clinic.
One limitation of this study is the low rate of response; less than a quarter of Canadian psychiatry residents completed our survey. This response rate is, however, similar to other published surveys of psychiatry residents. 17 Whether residents who chose not to respond to this survey have a different level of neuroscience knowledge and attitude remains unclear. Another limitation is a lack of adequate power to reliably assess differences between various Canadian psychiatry programs, as almost one-third (30.6%) of our respondents chose not to identify their training institution. This renders us unable to answer questions as to whether specific training programs in Canada are doing a better job than others of providing their trainees with an adequate neuroscience education.
Conclusions
This study demonstrates that a significant percentage of Canadian psychiatry residents feel that the neuroscience education currently provided by their residency programs is less than adequate, they recognize a gap in their neuroscience knowledge and competency, and they have a very high interest in receiving more neuroscience education. The goal of psychiatry residencies should be to train future psychiatrists who demonstrate both an interest in and the competency to incorporate relevant neuroscientific findings into their practice. Neuroscience does not compete with, but rather compliments psychotherapy, clinical knowledge, and treatment. Medical neuroscience is no longer only for neurologists and neurosurgeons, but also is a vital part of the armamentarium for psychiatry practitioners.
Supplemental Material
Supplemental Material, Neuroscience_Attitudes_Questionnaire - Attitudes of Psychiatry Residents in Canadian Universities toward Neuroscience and Its Implication in Psychiatric Practice
Supplemental Material, Neuroscience_Attitudes_Questionnaire for Attitudes of Psychiatry Residents in Canadian Universities toward Neuroscience and Its Implication in Psychiatric Practice by Taghreed Hassan, Benjamin Prasad, Benjamin P. Meek and Mandana Modirrousta in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the psychiatry residents who participated in this study. The authors would also like to thank William McPherson for his assistance in preparing the tables for this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.