
Abstract
Objective:
To evaluate the mode of implementation, clinical outcomes, cost-effectiveness, and the factors influencing uptake and sustainability of collaborative care for psychiatric disorders in older adults.
Design:
Systematic review.
Setting:
Primary care, home health care, seniors’ residence, medical inpatient and outpatient.
Participants:
Studies with a mean sample age of 60 years and older.
Intervention:
Collaborative care for psychiatric disorders.
Methods:
PubMed, MEDLINE, Embase, and Cochrane databases were searched up until October 2016. Individual randomized controlled trials and cohort, case-control, and health service evaluation studies were selected, and relevant data were extracted for qualitative synthesis.
Results:
Of the 552 records identified, 53 records (from 29 studies) were included. Very few studies evaluated psychiatric disorders other than depression. The mode of implementation differed based on the setting, with beneficial use of telemedicine. Clinical outcomes for depression were significantly better compared with usual care across settings. In depression, there is some evidence for cost-effectiveness. There is limited evidence for improved dementia care and outcomes using collaborative care. There is a lack of evidence for benefit in disorders other than depression or in settings such as home health care and general acute inpatients. Attitudes and skill of primary care staff, availability of resources, and organizational support are some of the factors influencing uptake and implementation.
Conclusions:
Collaborative care for depressive disorders is feasible and beneficial among older adults in diverse settings. There is a paucity of studies on collaborative care in conditions other than depression or in settings other than primary care, indicating the need for further evaluation.
The proportion of the world population older than 60 years is predicted to double from 12% to 22% between 2015 and 2050, pushing the absolute numbers from 900 million to more than 2 billion people. Moreover, approximately 15% of this population lives with a mental disorder, the most common being dementia, unipolar depression, and anxiety. 1
More than 50% of the older adults with mental illnesses do not receive treatment because of stigma or lack of identification and treatment. 2 Frequent co-occurrence of medical and psychiatric disorders with age 3,4 creates opportunities for their detection and treatment in general and specialist medical settings (e.g., primary care, home health care). Thus, collaboration between mental health and other medical services is crucial in this population.
Collaborative care is based on the chronic care model that includes screening, education, changes in practice, and developments in information technology. 5 Widely accepted key areas of collaborative care in mental health, derived from a model defined by Gunn et al., 6 include a multiprofessional approach to patient care, structured management plan, scheduled patient follow-ups, and enhanced interprofessional communication. There is 1 systematic review of randomized controlled trials (RCTs) on collaborative care in the primary care setting for depression in older adults that showed improved depression outcomes compared with usual care. 7 There has been no previous attempt to systematically assess its application among older adults in settings beyond primary care, including for psychiatric disorders comorbid with other medical conditions or psychiatric conditions other than depression.
We systematically reviewed collaborative care for psychiatric disorders across different settings, in a study population with mean age of 60 years and over, to assess 1) mode of implementation; 2) clinical outcomes of the psychiatric disorder; 3) other outcomes such as quality of life, functioning, outcome of comorbid medical conditions, caregiver burden, and cost-effectiveness, and 4) factors influencing uptake and sustainability.
Methods
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines 8 guided this review. The review includes published RCTs or prospective or historical cohort, case-control, and qualitative studies for health service evaluation, conducted in primary care, specialist medical inpatient and outpatient setting, home health care, and senior independent residential settings. Inclusion criteria included 1) at least 3 of 4 collaborative care criteria by Gunn et al., 6 2) focus on at least 1 psychiatric disorder, and 3) sample mean age of 60 years or older. Narrative review articles, protocols, editorials, commentaries and letters or case reports were excluded.
We used the following databases: PubMed, MEDLINE, Embase, Psychinfo, and Cochrane Library. We searched for publications in indexed journals until October 2016 without an early date limit, among the adult population aged greater than 18 years. This was done to broaden the scope and include studies in which the inclusion age may be less but the mean sample age was 60 years or older. Studies in the older population are few, and findings of studies with a mean sample age of 60 years and older were thought to be relevant to older adults.
We used the following search terms and their variations: “collaborative care,” “integrated care,” “shared care” AND “mental illness,” “psychiatric disorder.” Additional records were identified from the previous reviews on collaborative care (Figure 1).
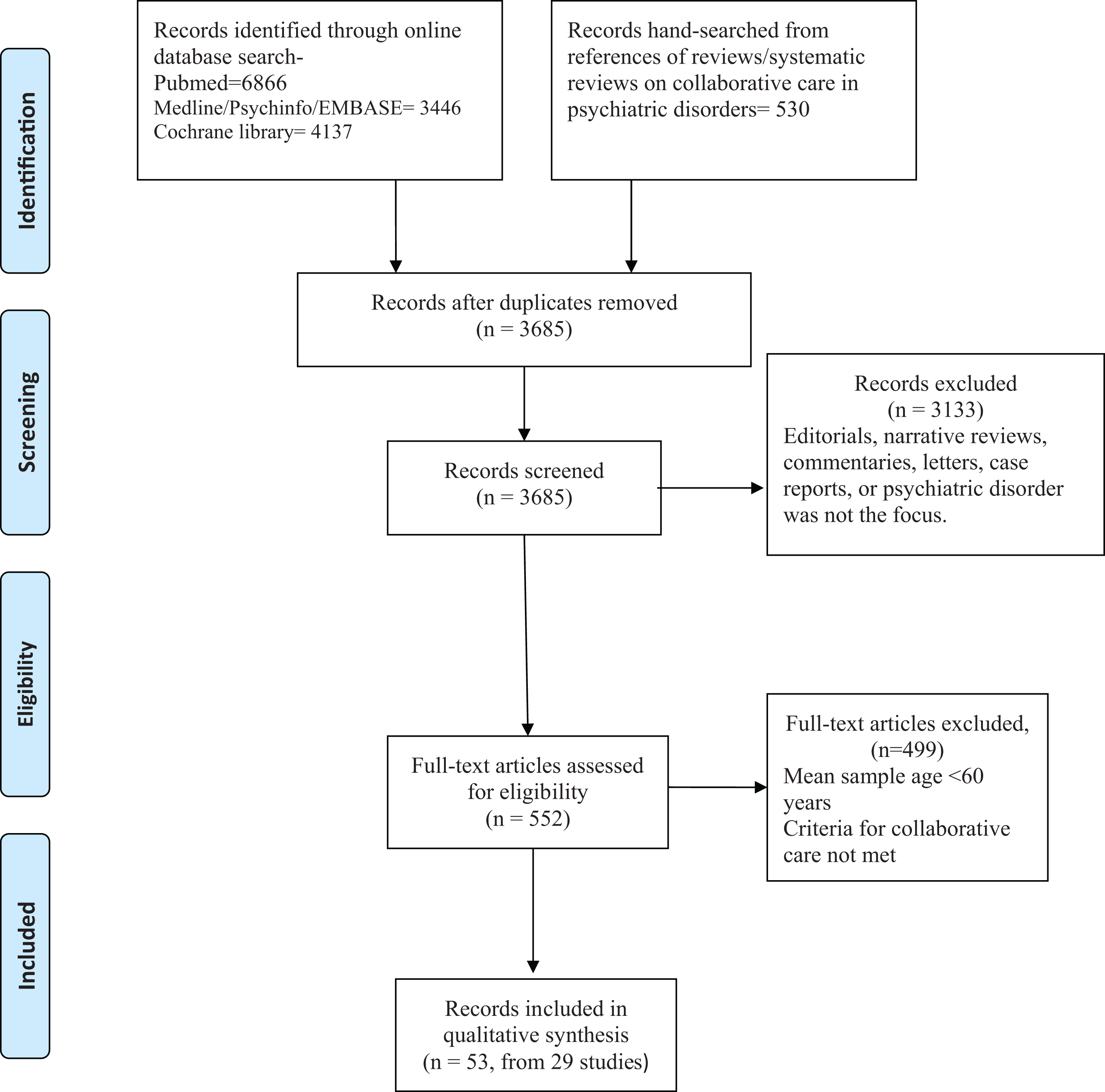
Process of selection of studies for the systematic review.
The first author (P.D.) screened the titles and abstracts to assess eligibility for inclusion. Full articles were reviewed in case of doubt regarding eligibility. From the eligible studies, information was extracted using a predesigned form on 1) first author last name; 2) year of publication; 3) setting; 4) study design; 5) psychiatric disorder; 6) study population characteristics; 7) process of implementation of collaborative care; 8) outcomes including rates of intervention, clinical outcomes of psychiatric disorder, outcome of comorbid medical illness, quality of life, functioning, caregiver impact, cost-effectiveness; and 9) factors influencing uptake and implementation.
It was not feasible to carry out a meta-analysis because of methodological heterogeneity among the studies included, the lack of consistent quantitative data in some of them, the different types of information reported in the original papers, and different scales used for outcome measures. Thus, the results of the review are presented in a narrative way.
Results
Figure 1 describes the selection process of the reviewed publications. Using the search terms and limits, 6866 published articles were identified on PubMed, 3446 on MEDLINE/Psych Info/Embase, and 4137 in the Cochrane Library. After removing the duplicates, 3685 publications were identified for screening. On excluding editorials, narrative reviews, commentaries, letters, case reports, and studies that did not focus on a psychiatric disorder, 552 publications remained. Of these, 53 publications (29 individual studies) met criteria for qualitative synthesis.
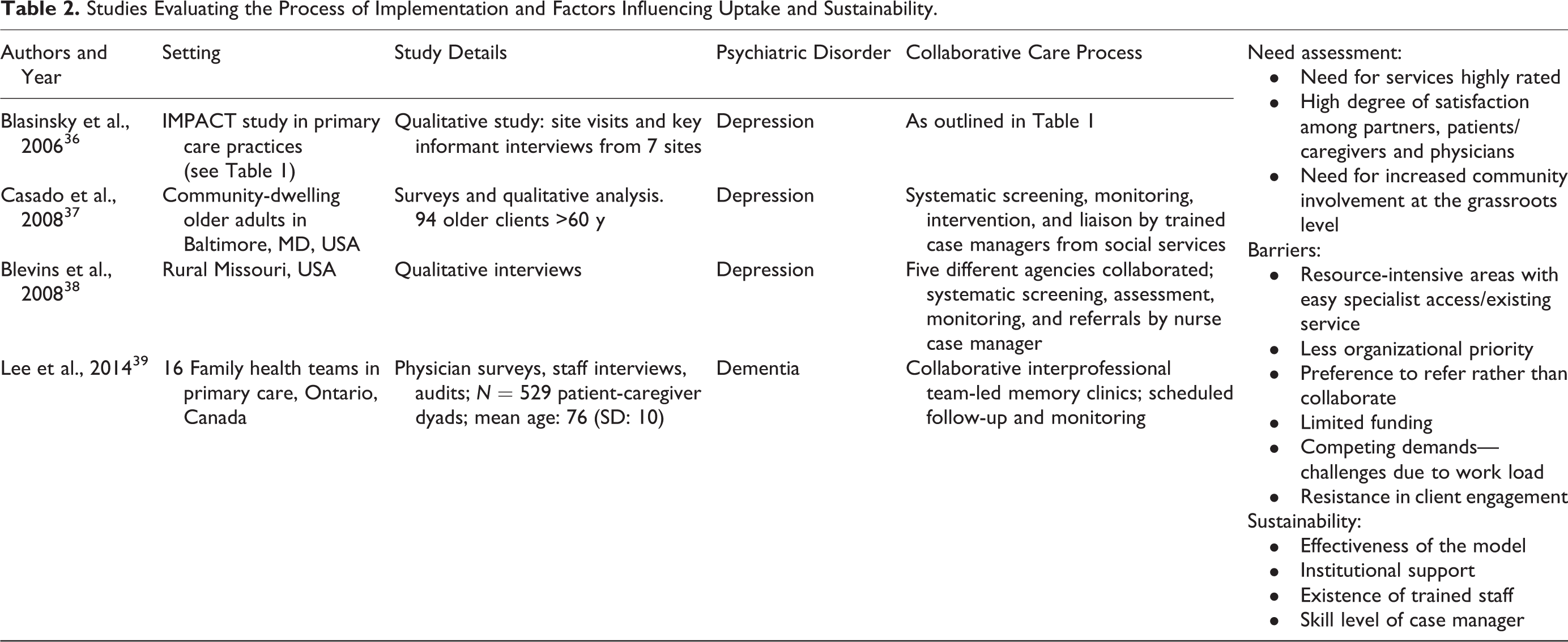
Table 1 describes the studies on clinical outcomes and cost analysis clustered by settings, and Table 2 describes the studies evaluating uptake, implementation, and sustainability. More details about individual studies can be found in Supplementary Tables S1 and S2.
Studies on Collaborative Care Evaluating Clinical and Cost Outcomes.a
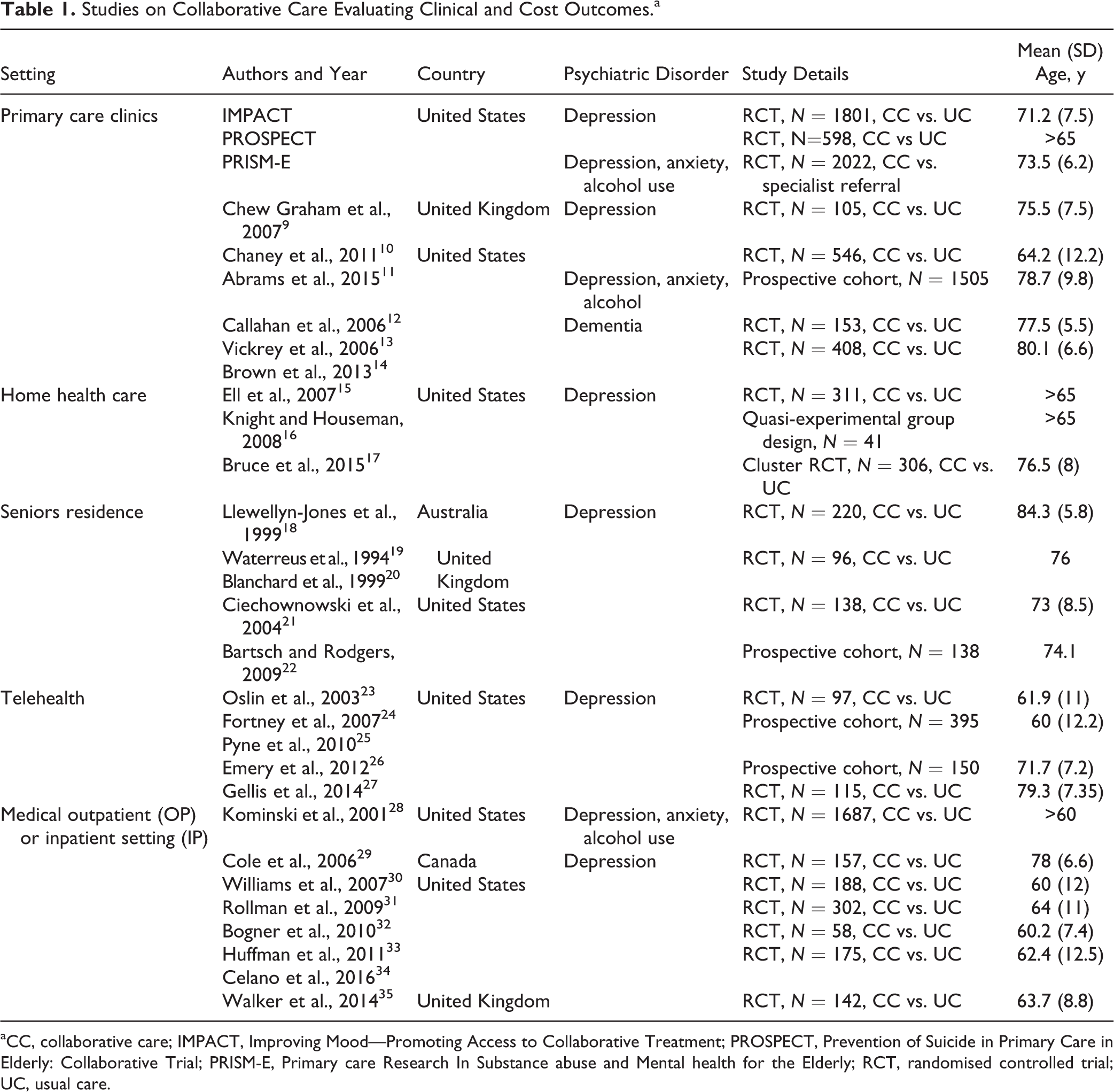
aCC, collaborative care; IMPACT, Improving Mood—Promoting Access to Collaborative Treatment; PROSPECT, Prevention of Suicide in Primary Care in Elderly: Collaborative Trial; PRISM-E, Primary care Research In Substance abuse and Mental health for the Elderly; RCT, randomised controlled trial; UC, usual care.
Studies Evaluating the Process of Implementation and Factors Influencing Uptake and Sustainability.
Our search identified 3 large RCTs (IMPACT, PROSPECT, and PRISM-E, Table 1) that generated 23 publications. Of these, 22 publications focused on clinical outcomes and cost analysis are clustered under their corresponding RCT. The other 27 publications on clinical outcomes and cost analysis are described individually and clustered by setting
IMPACT and PROSPECT studies on collaborative care in primary care for depression in the older population evaluated different aspects of collaborative care. Done in a large sample of 1801 and 598, respectively, they consistently showed significantly better outcomes for depression in collaborative care compared with usual care. 40 –42
In the IMPACT study, benefit was noted in depression care even in the presence of medical comorbidities such as arthritis 43,44 and diabetes 45 (Supplementary Table S1). Benefit was noted in the collaborative care compared with usual care in the presence of comorbid anxiety disorders such as panic disorder or posttraumatic stress disorder. 46 In the PROSPECT study, the benefit with collaborative care was noted even in the presence of medical comorbidities 47 and irrespective of cognitive deficits 48 (Supplementary Table S1). Ethnic differences did not influence the benefit with collaborative care compared with usual care 49,50 (Supplementary Table S1).
PRISM-E, with a sample size of 2022, showed that depression care integrated within primary care had better client engagement measured as number of visits with a mental health provider. 51 The outcomes in integrated care were similar to specialist referral and care 52 with no cost increment 53 (Supplementary Table S1). There was a reduction in alcohol use in terms of drinks per week and reduced episodes of binge drinking in both groups, with no significant difference based on the model of care 54 (Supplementary Table S1).
Three RCTs on collaborative care for depression in home health care 15 –18 did not show significant differences in depression outcome, although some benefit was noted at 12 months in moderately to severely depressed patients in one study 17 (Supplementary Table S1).
Three studies, two RCTs and another cohort study, within the community or community-based social service agencies showed improved outcomes for depression 19 –22 ( Supplementary Table S1). In one community study in the United Kingdom, improved outcome was noted at 3 months not sustained at 6 and 23 months. 19,20 Another RCT in public housing for seniors showed significantly greater response and remission in collaborative care compared with usual care. 21 Another cohort study showed significant improvement in the depression scores from baseline to discharge over 12 months. The treatment did not have a comparison group and hence it is difficult to assess if the benefit was because of collaborative interventions. 22
Three RCTs in which collaborative care for depression was integrated within primary care settings 9 –11 had variable outcomes as compared with the larger studies in primary care such as PROSPECT and IMPACT. In one study, at 16 weeks, the ratio of those being depressed was significantly lower. 9 In another study, there was no significant group difference in the depression scores at 6 months. The high variability was attributed to the uptake by primary care staff, which showed that at 24 weeks, change in depression scores from baseline in those with 2 case manager visit was significantly lower than those with 4 to 6 case manager visits10 (Supplementary Table S1).
Two RCTs 23,27 and 2 prospective cohort studies 24,26 used virtual modes of communication for collaborative care in depression. The 2 RCTs showed significantly better outcomes for depression compared with usual care, and benefit was noted compared with baseline, in the cohort studies (Supplementary Table S1).
Seven RCTs used collaborative care for depression in medical settings, 2 in general inpatient settings, 28,29 and 5 in specialty inpatient/outpatient clinics 30 –33,35 (Supplementary Table S1). Of these, all RCTs in specialty services showed significantly better outcomes for depression compared with usual care. Two of these RCTs also showed improved outcomes for diabetes and cardiac disease. 32,33
One RCT on collaborative care in dementia showed significantly improved neurobehavioral symptoms of dementia and caregiver stress. 12 Another RCT on collaborative care in dementia showed significantly greater adherence to dementia care guidelines, significantly greater confidence among caregivers in collaborative care compared with usual care, 13 and closed the disparity in dementia care quality between caregivers with less education and those with higher education 14 (Supplementary Table S1).
Two studies specifically focused on process of implementation and highlighted skill level, workload, and limited resources as important barriers to implementing collaborative care 37,38 (Supplementary Table S2). Qualitative analysis of the IMPACT study also revealed barriers such as organizational resistance and limited funding. The evaluation of sustainability 1 year after the end of funding found that it was sustained in 5 out of 7 sites in a modified manner. A few sites included it for adults aged more than 18 years, and all of them expanded it to other psychiatric disorders. They also modified the composition of the collaborative care team based on local resources. Sustainability was supported by effectiveness of the model, institutional support, and having trained staff 36 (Supplementary Table S2). An assessment of collaborative implementation of a memory clinic in primary care showed overall satisfaction among patients, caregivers, and physicians. One clinic that failed to be sustained was located in a resource-intense area with access to specialist care. 39
Discussion
This review broadens the scope of evaluation of collaborative care in older adults by including psychiatric disorders other than depression, settings beyond primary care, application in comorbid medical conditions, and various modes of implementation. It examines not only the outcome of the psychiatric disorder but also other outcomes such as quality of life, functioning, physical health, and cost-effectiveness. Lastly, it includes studies that evaluate factors affecting uptake and implementation.
Among the collaborative care studies for psychiatric disorders in adults, the numbers of studies in people aged 60 years and older are few. Using the broader criterion of mean sample age of 60 years and older in a previous review on depression and anxiety in primary care, only 15 RCTs were identified. 55 Applying similar criteria of collaborative care in all psychiatric disorders, we identified 29 studies. While chronic care models using an integrated approach are being evaluated for various medical conditions in frail elderly patients, 56 they do not often include mental health.
Most studies in this review focused on depression. There are 2 published studies on dementia. 12,13 At-risk alcohol use was included along with depression in the PRISM-E study. 51 One study targeted depression, anxiety, and alcohol abuse. 28 There are no studies on collaborative care for substance use disorders, psychotic disorders, mild cognitive impairment, or bipolar disorder in late life. In people older than 60 years, the prevalence of psychiatric disorders other than depression is significant and underidentified. 57 Comorbidity is common in this age group. 58 Substance use or misuse of prescription medication may be frequently associated with medical or psychiatric conditions. 59 Comorbidities often complicate treatments and delay recovery. 58 Hence, when collaborative care is evaluated and applied in older adults, it may need to target multiple psychiatric conditions along with medical conditions.
Collaborative Care Process Based on Settings
All elements in the collaborative care process are used across most studies. There were, however, some studies that did not include at least 1 element. 15,18,22 Lack of systematic follow-up and monitoring resulted in no benefit in some studies. 15,18,29 In fact, the physicians involved in the IMPACT study identified proactive follow-up as one of the most helpful components of collaborative care. 60 It is also emphasized as an important component for improved outcomes. 61
The settings included home health care, seniors community dwellings connected to social services, primary care, specialty care clinics, and hospital inpatient units. The mode of application varied depending on the setting. Most studies integrated the mental health care within the setting. They identified and trained existing staff to assist with coordination and collaboration. In primary care clinics and medical specialty clinics, specific case managers or nurses were trained in mental health to provide screening, education, psychotherapy, monitoring, and links between primary care/specialty care and mental health services. 9 –11,32,35 On inpatient units, the nurses helped with screening and identification. 28 –31,33 In home health care settings, the staff was trained to function as mental health case managers. 15 –18 In community dwellings connected to social services, staff of the social services were trained to screen and identify patients with depression and refer them for appropriate assessment and care. 21,37 Primary care physicians and members of the local community were trained in one study 22 to screen and identify patients with depression and refer to community mental health teams.
Screening and enhanced referral to psychiatry specialist clinics or community mental health teams was examined in 2 studies. 22,51 From the PRISM-E study, 52 there is evidence of better engagement when specialist care is collocated within primary care compared with referral to specialist services, and outcomes are similar to specialist referral and care. 51,52
Use of technology to enable the process of assessment or care provides insights into the unique ways of executing collaborative care. Telephone disease management to assess and monitor was used for depression 24,26,27 and in post–coronary bypass patients with depression. 31 One study used telepsychiatry to obtain specialist consultation, 24 apart from using telephone assessments. Another used virtual communication and electronic networking to coordinate input from the multidisciplinary team. 26 This is important, especially in remote areas where collaborations could be established even in the absence of local specialist services.
Treatment Outcomes
Treatment outcomes using collaborative care can be classified into various domains.
Treatment Rates
The collaborative approach helps to improve treatment initiation and possibly improved compliance. A number of studies found significantly higher treatment rates for depression intervention in terms of mental health contacts 15,40,51 and antidepressant use 10,12,40 or better adherence to antidepressant medications 24,32 compared with usual care (Supplementary Table S1). The impact on treatment rates among ethnic minorities is unclear. It was estimated at 60% to 70% of the treatment rates in the white population in the PROPECT study 49 but was no different from the white population in the IMPACT study. 50 In the dementia study, 14 there was greater adherence to dementia care guidelines and increased linkages to community resources in collaborative care versus usual care.
Treatment Outcomes for Psychiatric Disorder
Only a few studies showed lack of benefit for depression with collaborative care compared with usual care. 10,15,18,28,29 Also, the rate of response for depression was quicker 62 and remission rates significantly higher in the intervention group compared with usual care. 9,21,24,30,40,42
The negative studies are in populations with high disease burden in home health care settings 15,17 –19 or acute inpatient settings. 29,30 The authors have argued that the patients in the home health care setting have high medical morbidity and physical disability. Also, the time-based funding in home health care results in loss to follow-up and monitoring that may undermine the effectiveness of collaborative care. Two studies in the general acute inpatient setting did not show statistically significant benefit compared with usual care but showed reduced inpatient costs. 28,30 In the primary care setting, a nonsignificant outcome for depression was linked to poor uptake influenced by physician attitude and skills in one study. 10 Thus, acutely unwell patients and poor follow-up either due to high morbidity or lack of proactive engagement may weaken the benefits of collaborative care.
The IMPACT and PROSPECT studies also found that there was benefit with depression management even in the presence of medical comorbidities, 43 –45,47,63 comorbid anxiety disorders 46 irrespective of cognitive function, 48 and education or ethnic differences. 49,50 The response and remission of depression in the collaborative care group was similar to specialist psychiatry clinics in the PRISM-E study, 52 highlighting the effectiveness of collaborative care.
While the only study using collaborative care in dementia showed significant improvement in behavioral and psychological symptoms compared with treatment as usual, 12 this is the only study that evaluated clinical outcomes in patients with dementia, and thus, firm conclusions on its impact in dementia cannot be drawn.
Collaborative care models for psychiatric disorders other than depression have not been well studied, with existing studies having mixed results. For at-risk alcohol use included in the PRISM-E study, there was a reduction in alcohol use and binge-drinking episodes in both groups with integrated care and specialist referral. 52 No significant difference was noted in terms of outcomes for depression, anxiety, or alcohol use in the only study that evaluated collaborative care for 3 different conditions occurring on their own or in combination. 28 The reasons for this are unclear and could relate to lack of specific intervention for these conditions in the study or that tackling multiple psychiatric morbidities is challenging through collaborative care. This needs further investigation.
Secondary Outcomes (Suicidal Ideation, Quality of Life, Social Functioning, Physical Health, Long-term Mortality)
Collaborative care appears to have a positive impact on other aspects of care. Studies show reduction in suicidal ideation 62,64 and improved quality of life, functioning, and subjective distress. 9,21,24,35,40,41 In the study on dementia patients, it helped reduce caregiver distress 12 and improved caregiver confidence in providing care. 14
Only a few studies evaluated the impact on physical health status, of which the data from the IMPACT study showed significant improvement in pain scores in patients with arthritis, 43 while pain was found to influence treatment outcomes of depression in the PRISM-E study. 65 Long-term follow-up of participants in the PROSPECT study showed reduced mortality rates by 24% at 96 months in the intervention group compared with the comparison group (hazard ratio, 0.76; 95% confidence interval CI, 0.57 to 1.00; p = 0.05; Supplementary Table S1). 66 When collaborative care was incorporated into the management of medical illness, improvement was noted in diabetes control and cardiac care. 32,33 The impact on physical health status is, however, not consistent, with no benefit seen in some studies 15,21,22,26 (Supplementary Table S1). In post–coronary bypass and cancer patients with depression, the rates of hospital readmission or mortality were not affected by the collaborative care interventions 31,35 (Supplementary Table S1).
The improved outcome in areas other than primary psychiatric disorder could relate to the improvement in mental health or overall improvements in quality of care and monitoring associated with collaborative care.
Health Care Costs
Refer to Supplementary Table S1 for more details. Although there is an overall increased cost with the use of collaborative care, accounting for depression-free days and quality-adjusted life-years (QALYs), the studies suggest a cost benefit. The IMPACT study found that the total outpatient costs were USD $295 higher during the study period, but it was cost-effective after accounting for QALYs. 67,68 The PRISM-E study noted a cost benefit in Veterans Affairs settings. 53 Telemedicine, however, has higher costs per QALY than other studies on collaborative care (incremental cost of $85 637/QALY). 25 In cardiac patients, the cost of collaborative care was $175.27 higher per participant but was cost-effective because of depression-free days and improvement in QALYs (incremental cost-effectiveness of $3337.06/QALY). 34
Factors Influencing Uptake and Barriers to Implementation of Collaborative Care
There is a perceived need among various services for this model and a high degree of satisfaction. Effectiveness of the model, institutional support, and presence of trained staff were found to facilitate the process of collaboration and encourage sustainability. Some of the barriers identified are absence of staff skills and attitude, increased workload, and lack of organizational support or funding. 36 –38 There are only 2 studies evaluating sustainability. The IMPACT study showed that 5 out of 7 sites sustained the model after the funding ended but modified it to include other conditions and local staff members. 36 In the case of memory clinics within primary care, it was found that the clinic in a resource-intensive area with easy access to specialists could not be sustained. 55
Limitations
Most of the studies were focused on depression, with relatively few evaluating collaborative care in other psychiatric disorders. Hence, it is premature to draw conclusions about its impact in psychiatric disorders other than depression. In addition, nearly half of the publications reviewed were from 3 large RCTs, thus limiting the findings and interpretations. However, the results for collaborative care in depression are consistently positive, even in smaller studies across settings. A final limitation is that we included studies with a sample mean age of 60 years and older, which may not be truly representative of the older population.
Future Directions
We need studies on the impact of collaborative care in older adults for psychiatric conditions other than depression and co-occurring psychiatric disorders with and without medical illnesses. The role of proactive follow-up as well as attitudes and skills of primary care staff need specific focus in future studies since these may have undermined the collaborative care benefit in some situations. More studies are also needed on cost analysis and factors influencing uptake and sustainability, especially in settings other than primary care.
Conclusions
While evidence for the effectiveness of collaborative care in multiple psychiatric disorders with or without medical illnesses is poor and needs further evaluation, it is reasonable to conclude the following in the case of depression: It is feasible to implement collaborative care models in various settings. The means of implementation may vary depending on the available local resources. Further, the use of technology may help to overcome limitations without compromising benefits. There is compelling evidence for depression outcomes using collaborative care. Some of the implementation barriers identified are staff skills and attitude, workload in primary care, mobilization of resources, and organizational support.
Footnotes
Author Contributions
All authors were involved in the study concept and design. Pallavi Dham mainly worked on data acquisition and consolidation. All authors were involved with preparation of the manuscript. All authors have seen and approved the final version of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant received from the CAMH foundation and McMaster foundation as part of the collaborative care initiative. Carrie McAiney is supported in part by the grant received.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.