
Abstract
Objective:
The Psychotherapies for Chronic PTSD randomised trial found that three 14-week psychotherapies acutely benefitted patients with chronic posttraumatic stress disorder (PTSD). Previous research has reported sustained follow-up benefits for prolonged exposure (PE) and relaxation therapy (RT), but few comparable data exist for interpersonal psychotherapy (IPT). We describe 3-month follow-up for acute responders to all 3 treatments.
Method:
Acute responders, defined a priori as ≥30% improved from baseline, were reevaluated after 3-month no-treatment follow-up by independent evaluators using the Clinician-Administered PTSD Scale (CAPS).
Results:
Fifty of 110 initial study entrants met acute responder status at week 14. Forty-three (86%) responders entered follow-up: 23 remitters (CAPS ≤20) and 20 responders. At week 26, 27 had achieved remission status, 10 remained responders, and 6 had relapsed. Of week 14 remitters, 8 of 9 PE, all 8 IPT, and 4 of 6 RT patients remained remitted. Relapse rates were 7% (1/9) for PE, 10% (2/20) for IPT, and 33% (3/9) for RT. At week 26, PE showed greater improvement on CAPS than RT (P = 0.048) and a trend for superiority over IPT (P = 0.098), with no significant difference between IPT and RT. Depressive symptoms remained low during follow-up.
Conclusions:
These are the first systematic data on follow-up responder status and persistence of acute treatment benefits in patients receiving individual IPT for chronic PTSD. Patients generally maintained gains across treatments, fluctuating most in RT. Study limitations include small sample size and brief follow-up interval. PTSD research should employ response and remission criteria.
The first step in clinical outcome research is to show that treatments acutely alleviate symptoms. Having established this, the persistence of gains matters: do patients, once improved, stay better? We conducted a 14-week randomised trial of 3 psychotherapies 1 for unmedicated patients with chronic posttraumatic stress disorder (PTSD)—prolonged exposure (PE), 2 interpersonal psychotherapy (IPT), 3 and relaxation therapy (RT) 4 —and collected 3-month follow-up data on week 14 treatment responders at week 26. Whereas previous research on PTSD has evaluated follow-up of PE, other exposure therapies, and RT, almost no data address enduring effects of IPT for PTSD.
The literature indicates that patients with PTSD who respond to psychotherapy generally remain improved 5,6 unless they suffer further trauma. The extant research overwhelmingly comprises exposure therapies for PTSD. Two representative previous direct comparisons of exposure therapy and RT bear particular mention. Marks et al. 7 compared 4 randomly assigned 10-week treatments for 87 patients with PTSD: exposure alone, exposure with cognitive restructuring, cognitive restructuring alone, and RT. Exposure and cognitive restructuring, alone or combined, yielded greater acute improvement than RT on the Clinician-Administered PTSD Scale (CAPS), 8 and the treatments retained their relative gains at 6-month follow-up. Taylor and colleagues 9 treated 60 patients with PTSD in a randomised trial of 8 weekly sessions of PE, RT, or eye movement desensitisation and reprocessing. Forty-five patients completed treatment. Prolonged exposure produced larger acute reductions in reexperiencing and avoidance symptoms and had a larger proportion of patients who no longer met DSM-IV-TR PTSD criteria than did the other 2 treatments. Again, the treatments generally maintained acute gains at 3-month follow-up. 9
Few prior data address follow-up of individual IPT for PTSD, as ours was the first large trial of this affect-focused, nonexposure treatment. In a separate, preliminary 14-week pilot trial, 10 we openly treated 14 patients with chronic PTSD, finding large improvements on CAPS, Hamilton Depression Rating Scale (Ham-D), 11 and other measures. The six of these patients (43%) reassessed at 6-month follow-up showed persisting remission, defined by CAPS 8 score of <20. 1 Mean (standard deviation [SD]) CAPS score at follow-up was 16.8 (9.6), compared to 14.2 (9.8) at week 14. 1 Krupnick et al. 12 conducted a randomised trial comparing group IPT to a waiting list condition for 48 multiply traumatised socially disadvantaged women recruited from family planning and gynaecology clinics. Group IPT yielded greater improvement than the waiting list control: in the intention to treat sample, mean (SD) CAPS scores fell by 25.5 (16.9) in IPT and 5.8 (12.2) in the waitlist. Although only 81% of IPT and 63% of waiting list subjects attended 4-month follow-up ratings, gains generally persisted: 6/26 (23%) IPT versus 5/10 (50%) controls met criteria for PTSD, and 10 (38%) IPT and 7 (70%) control patients met criteria for major depression. 12
The current study provided the opportunity to retest the replicability of PE and RT follow-up outcomes while systematically assessing it in individual IPT for the first time. Does non-exposure-based therapy work as well as exposure therapy in maintaining acute treatment gains? We hypothesised that patients who had clinically responded when treatment concluded (week 14) would tend to maintain their gains 3 months later (week 26) in all 3 treatments. We assessed whether responders moved to remission status or relapsed but lacked power to find and did not anticipate significant differences in responder outcome.
Our primary outcome in the overall trial was acute (week 14) CAPS score. At that juncture, we offered patients who had met acute response criteria (defined a priori as ≥30% decrement from baseline CAPS score) entry into a 3-month, no-treatment follow-up phase. As it would be unethical to ask nonresponders to wait 3 months before receiving further treatment, they were offered no-cost crossover at week 14 to an alternative course of PTSD treatment. This ongoing treatment precluded their inclusion in the follow-up sample and is the key reason we did not report these follow-up data with the acute outcome analyses. 1 Follow-up of responders only is a standard strategy of pharmacotherapy trials. 13 Our basic question, however, remains. The acute outcome question asked whether IPT was no more than minimally inferior to PE. The follow-up question is the following: do the benefits of brief, PTSD-focused therapies, including IPT, persist after 3 months without further treatment?
Methods
Acute study details have been reported. 1 The study enrolled patients between April 2008 and November 2012 at New York State Psychiatric Institute in New York City. Individuals eligible after telephone screening signed informed consent for intake interviews to determine DSM-IV–defined trauma, PTSD as primary diagnosis, and exclusion criteria. Independent evaluators (PhDs) blind to treatment assignment established current and lifetime diagnoses using CAPS, 14 Structured Clinical Interview for DSM-IV, 15 and other measures. Eligible subjects signing institutional review board (IRB)–approved informed treatment study consent were randomly assigned to PE, IPT, or RT in a 4:4:3 ratio, stratified by presence of major depressive disorder (MDD; Structured Clinical Interview for DSM-IV diagnosis, 24-item Ham-D [10] score ≥20) and implemented in random-sized blocks (11 or 22).
The 3 study treatments differ considerably. PE, 2 the best tested of the various exposure-based treatments, comprised 10 weekly 90-minute sessions (900 minutes) spread over 14 weeks. It helps the patient reconstruct a coherent narrative of the trauma, presents a rationale for facing feared trauma reminders, helps the patient to construct a hierarchy of such fears, and then uses repeated imaginal and in vivo exposure to help patients habituate to and potentially extinguish them. IPT is a well-studied, time-limited, manualised treatment of demonstrated efficacy for mood and eating disorders that focuses on the link between feelings and interpersonal situations. 16 The first author adapted this approach to address the affective numbness and interpersonal hypervigilance typical of PTSD, stressing affective attunement as a means to assessing trust of others 3 in 14 weekly 50-minute sessions (700 minutes), and focuses not on past trauma but on its current interpersonal consequences, on patient numbness to affect, and on using affect as a guide to handling daily interpersonal encounters. It thus helps patients to determine whom they can trust, builds social support, and restores a sense of mastery of the environment. RT, 4 in 9 weekly 90-minute and a final 30-minute session (840 minutes) in which the therapist does most of the talking, induces progressive muscle and mental relaxation.
Patients 18 to 65 years old had a primary DSM-IV diagnosis of chronic PTSD and CAPS score ≥50 (i.e., at least moderately severe PTSD). Patients reported a variety of traumata, including 93% with interpersonal trauma, 62% physical trauma, and 35% sexual trauma. 17 Exclusion criteria comprised psychotic disorders; bipolar disorder; unstable medical conditions; substance dependence; active suicidal ideation; antisocial, schizotypal, borderline, or schizoid personality disorder; prior nonresponse to ≥8 weeks of a study therapy; and outside psychotherapy or pharmacotherapy. Response was defined a priori as ≥30% decrement from baseline CAPS score and remission as CAPS score <20. 8,18
All 3 treatments yielded overall acute gains (d = 1.32-1.88) in a sample of 110 unmedicated patients with chronic PTSD. At week 14, the primary outcome point, response rates were IPT 63%, PE 47%, and RT 38%; remission rates were PE 26%, IPT 23%, and RT 22%. IPT was statistically no more than minimally inferior to PE, and both treatments fared somewhat better than RT. 1 Following week 14 assessment, study patients who met response criteria (≥30% CAPS decrement) were invited to enter a 12-week observational follow-up without additional treatment, with assessment repeated at week 26. Although the follow-up was defined as treatment free, evaluators inquired about interval treatment history. Patients received $50 compensation for completing their final assessment.
Data Analysis
To determine whether the follow-up sample was representative of the original sample, patients participating in the follow-up were compared to all follow-up nonparticipants on baseline characteristics and clinical variables, using t tests for continuous measures and chi-square tests (or Fisher’s exact test, when appropriate) for categorical measures.
The PTSD treatment literature lacks consensus definitions for response and remission. Our follow-up strategy mirrored that of pharmacotherapy continuation studies, assessing change in response/remission status over time. 13 For each treatment group, we defined a priori 3 statuses at week 26 with frequencies and proportions: 1) responder, defined as ≥30% reduction from baseline CAPS score; 2) remitter, defined as CAPS score <208; and 3) relapse, defined as having <30% reduction from baseline CAPS score after having met response criteria at week 14. Group contrasts of CAPS score at week 26 and change in CAPS score from week 14 to week 26 were tested using a repeated-measures, mixed-effects model, with CAPS score as the response variable and treatment group, categorical time, and their interaction as predictors, adjusting for baseline CAPS score, with an unstructured covariance matrix. Cohen’s d effect sizes (d) for difference in CAPS scores between groups were calculated as mean differences divided by SD at baseline of the whole sample.
As this was a longitudinal exploratory analysis performed on a subsample of study participants, we made no correction for multiple comparisons. A power analysis revealed ≥80% power to detect only large effect sizes (Cohen’s d) of 1 SD or greater. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Fifty of 110 patients met responder criteria at week 14: IPT (n = 24), PE (n = 17), and RT (n = 9) (see Figure 1). Of those 50, 43 (86%) entered the follow-up assessment phase: IPT, 20 (83%); PE, 14 (82%); and RT, 9 (100%). The 7 eligible nonentrants generally requested further treatment (as CAPS response status does not imply symptomatic remission) or declined for other, nonspecific reasons. Study responders did not differ from acute treatment nonresponders by sex, race, education, or employment, although they expectedly differed in week 14 CAPS score and in Ham-D score (8.3 [SD = 7.3] vs. 20.5 [SD = 5.4] for acute treatment nonresponders). Nor, among responders, did follow-up participants significantly differ from eligible nonparticipants on demographic variables. Responders entering the follow-up phase did not differ from follow-up nonparticipants on baseline CAPS score (68.3 [SD = 13.4] vs. 68.7 [SD = 17.1]) but had a significantly greater CAPS decrease at week 14 than nonparticipants (70.0% [SD = 23.4] vs. 51.6% [SD = 21.2], t(53) = –2.45, P < 0.02). At week 14, follow-up patients had a mean (SD) CAPS score of 22.1 (19.1) and nonparticipants had a score of 32.8 (15.9) (P = 0.08), suggesting that nonparticipants, although having improved with study treatment, had greater reason to seek further treatment than follow-up entrants, whose mean score approached remission. 8 All follow-up entrants completed the phase.
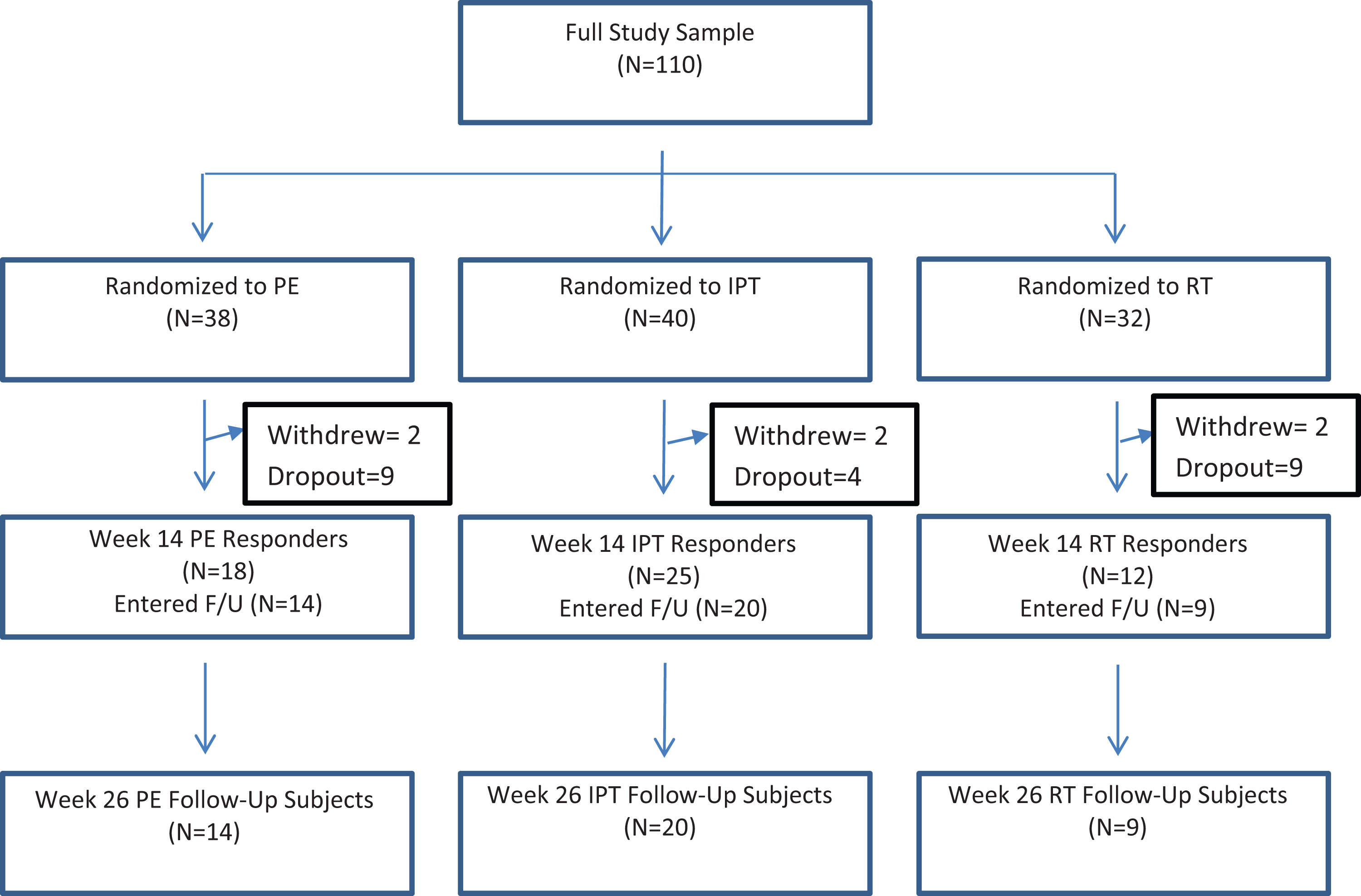
Study flowchart. F/U, follow-up; IPT, interpersonal psychotherapy; PE, prolonged exposure; RT, relaxation therapy.
Table 1 presents demographic data for the follow-up cohort, showing no differences across treatments aside from a trend (P = 0.07) for race, with IPT subjects more likely to report white race than RT subjects. The sample was 70% female; 60% white, 23% African American, 9% Asian, and 6% other, with 33% Hispanic ethnicity; 23% married or cohabitating; and 49% with full-time employment. Participants denied interval psychotherapy and psychopharmacotherapy. They reported a mean (SD) of 12.7 (12.7; median, 9) years of symptoms, in contrast to 14.1 (14.4) for the overall treatment sample.
Follow-up Sample Demographics and Clinical Characteristics.
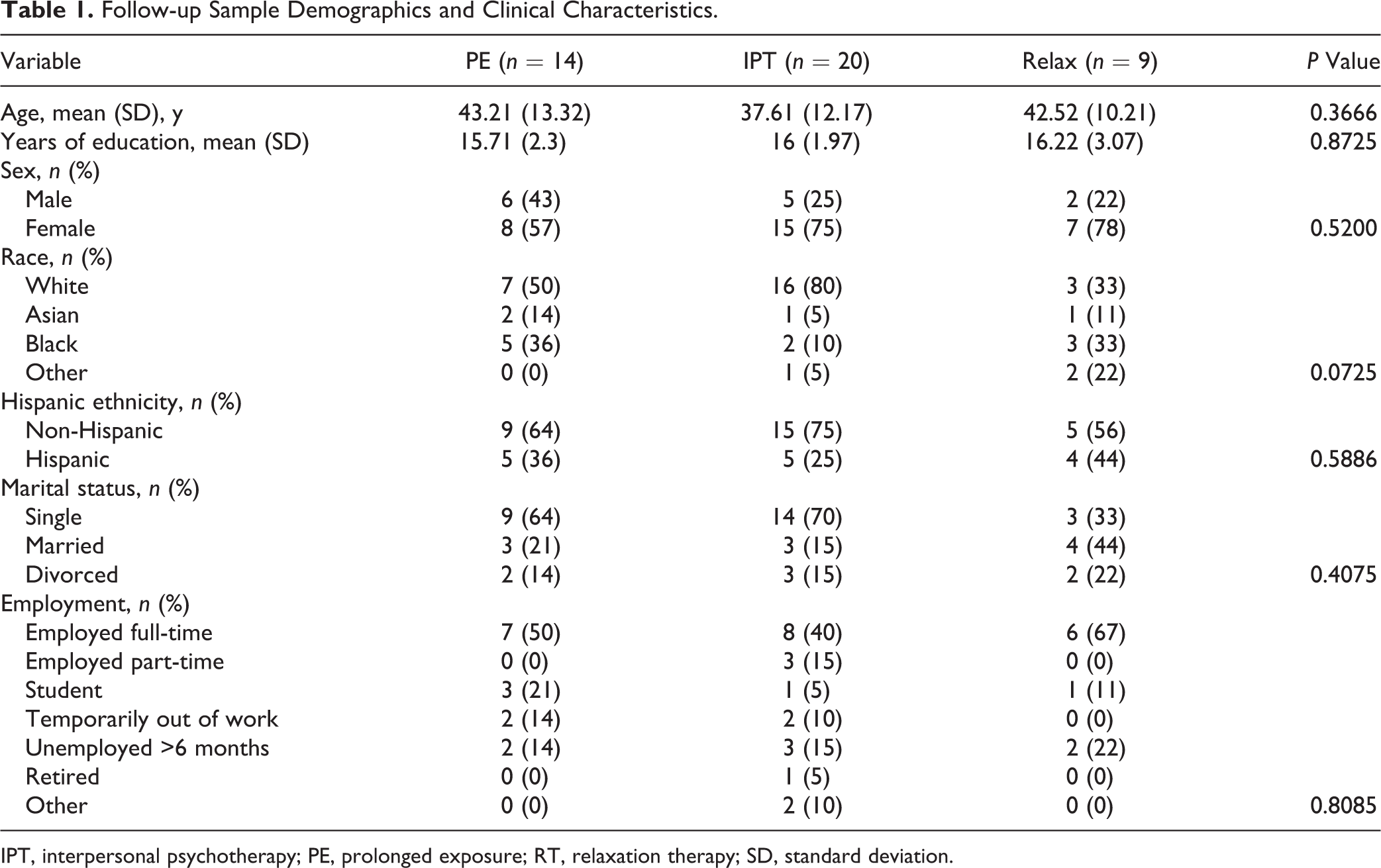
IPT, interpersonal psychotherapy; PE, prolonged exposure; RT, relaxation therapy; SD, standard deviation.
Forty-three patients entered the follow-up phase: 23 remitters and 20 responders. Three months later, 27 had achieved remission status, 10 had responder status, and 6 had relapsed (Figure 2). Table 2 dissects this by treatment. All 8 acute treatment IPT remitters maintained remission; of 12 responders, 3 became remitters, 7 remained responders, and 2 (2/20 = 10%) relapsed. Eight of 9 week 14 PE remitters maintained remission at week 26, with 1 slipping to responder status; of 5 acute responders, 3 attained remission, 1 remained a responder, and 1 (1/14 = 7%) relapsed. In RT, 4 of 6 acute remitters maintained remission, 1 became a responder, and 1 relapsed; among 3 responders, 1 remained remitted and 2 relapsed (overall 3/9 = 33% relapsed).
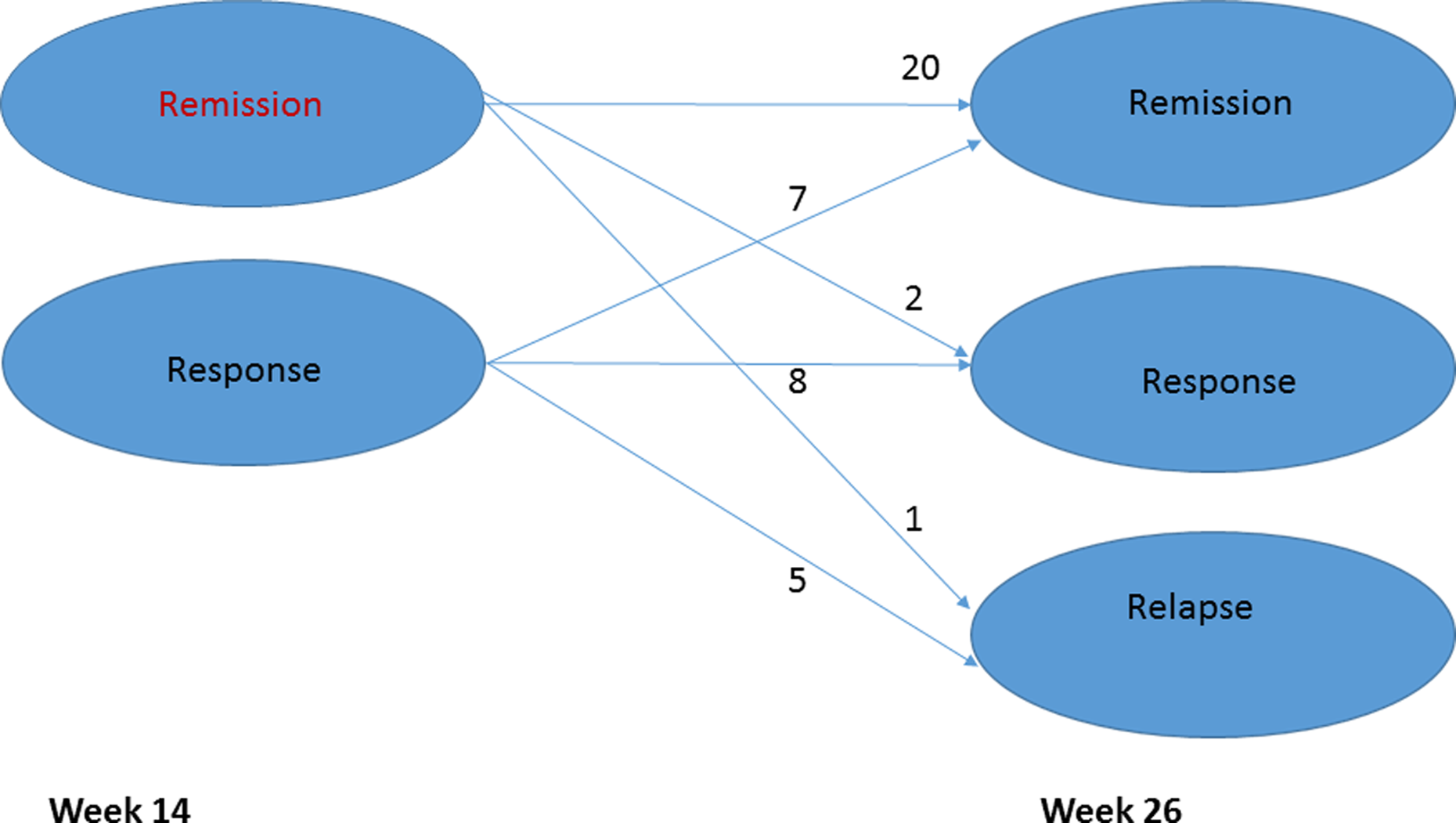
Status of patients after follow-up.
Treatment Remission, Response, and Relapse Status during Follow-up.
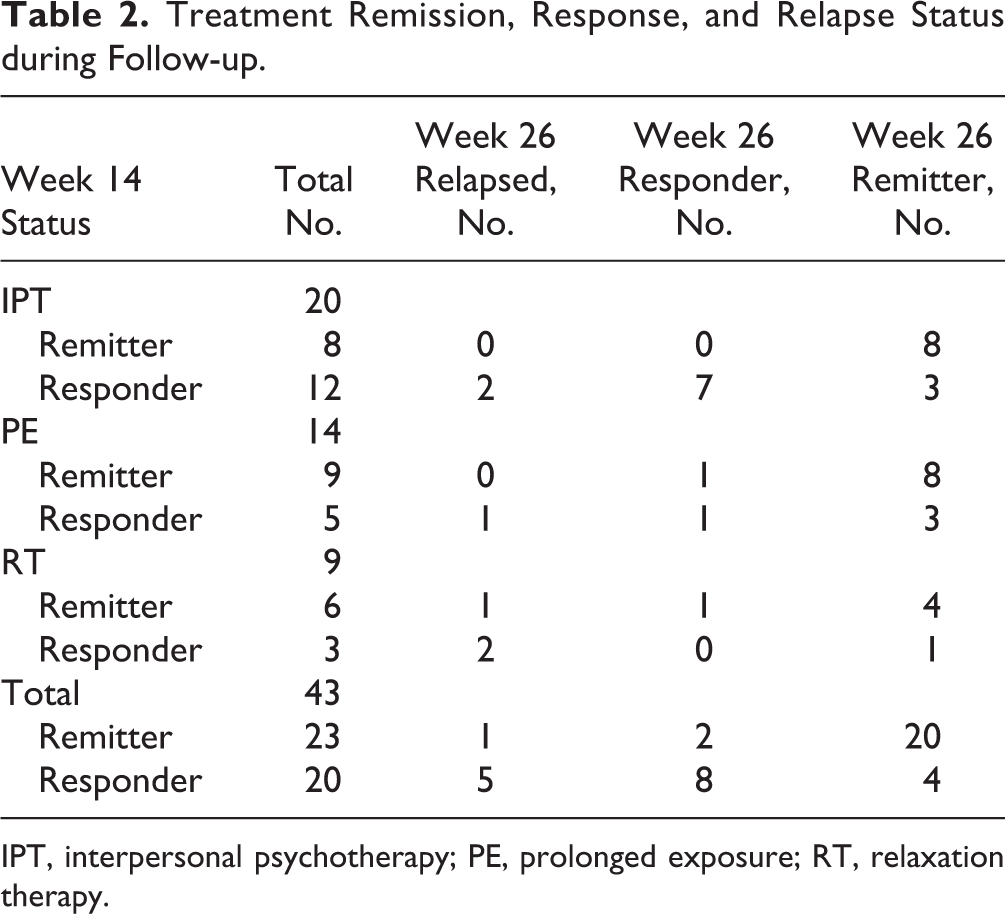
IPT, interpersonal psychotherapy; PE, prolonged exposure; RT, relaxation therapy.
As this study defined relapse as loss of response status (i.e., <30% improvement from baseline CAPS score), relapse might reflect barely crossing that threshold (e.g., 25% improvement) or further deterioration (0% or worse). Evaluating the scores of the 6 relapsing patients, we found that all but 1 still showed some, if more modest, treatment benefit relative to baseline PTSD severity on CAPS (Supplemental Table S1). A mixed-effects model comparing baseline CAPS scores to weeks 7, 14, and 26 showed significant improvement for each treatment, by week 14, without significant within-group change between weeks 14 and 26. The model found significant main effects for treatment (F 2,118 = 6.47, P = 0.0022), time (F 2,118 = 3.68, P = 0.0281), and baseline CAPS score (F 1,118 = 37.55, P < 0.0001) and a nonsignificant treatment-by-time interaction (F 4,118 = 1.58, P = 0.1853). Comparing outcomes at week 26, PE showed a statistically significantly greater improvement on CAPS relative to RT (d = 0.79, P = 0.048) and a trend for superiority over IPT (d = 0.78, P = 0.098), with no significant difference between IPT and RT.
Table 3 provides mean CAPS scores and Hamilton Depression Rating Scale (10) scores for the sample. Depressive symptoms did not differ across treatment groups at any time point.
Posttraumatic Stress Disorder and Depression Symptom Severity over Time.
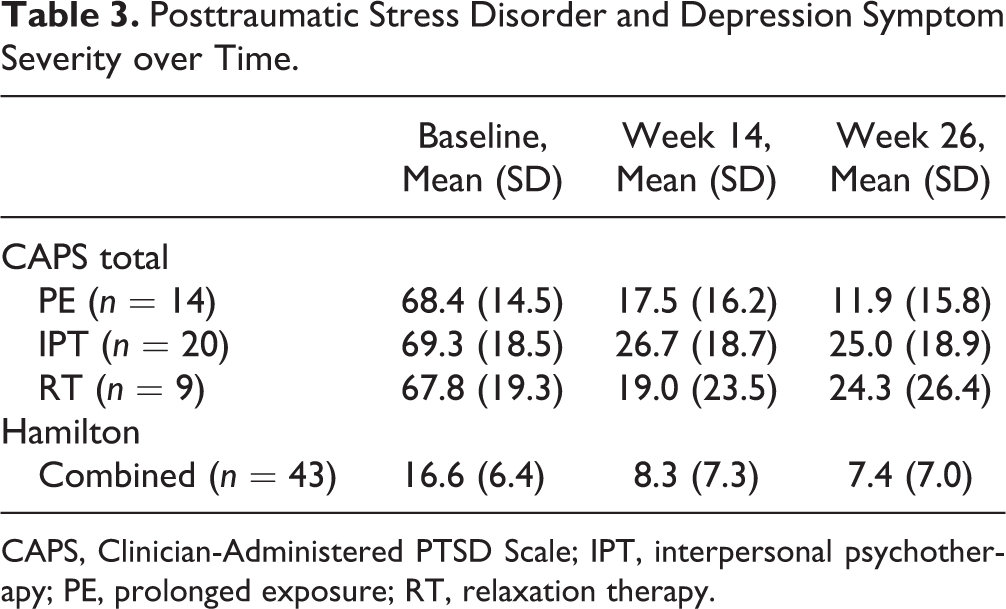
CAPS, Clinician-Administered PTSD Scale; IPT, interpersonal psychotherapy; PE, prolonged exposure; RT, relaxation therapy.
Discussion
As hypothesised, all treatments not only worked acutely but also continued to benefit most initially improved patients 3 months after treatment had ended. These findings of stability, previously demonstrated for exposure-based therapies and relaxation therapy, here applied to IPT as well. Patients treated with PE showed hints of continuing improvement in residual PTSD symptoms during the follow-up period, and the IPT patients remained generally stable, whereas the small subsample of RT patients showed some risk for deterioration. The subsample sizes are too small and the duration too limited to definitively judge, but the trends are intriguing. Although a small percentage of initial responders and remitters deteriorated (6/43 = 14%), most maintained their gains (remitters 20/23 = 87%; responders 15/20 = 75%), and 7 responders (7/20 = 35%) improved to remission status. Depression symptom severity remained low during the follow-up period. Perhaps because few studies have categorised remission and response in PTSD, we found no previous reports describing analogous changes in follow-up remission/response status.
One potential benefit of acute psychotherapy is that benefit may persist or increase after treatment has ended, 19 unlike pharmacotherapy, which requires ongoing prescription to maintain initial gains. Although the literature does not always clarify whether patients received interval treatment during follow-up periods, our patients reported none. This suggests potential cost-effectiveness for acute psychotherapy of PTSD relative to pharmacotherapy.
This is the first formal follow-up study of individual interpersonal psychotherapy for PTSD. Our acute outcome study found that IPT, a nonexposure treatment, worked essentially as well as PE, the best-tested exposure treatment. 1 The current findings indicate IPT continued to work equally well 3 months posttreatment. Limited follow-up data on IPT across psychiatric disorders exist aside from Krupnick et al.’s group IPT study for PTSD. 12 A few IPT studies followed up patients after acute treatment for major depression 20 –23 but provided maintenance IPT treatment. Talbot and colleagues 24 randomly assigned women with major depressive disorder and histories of sexual abuse, two-thirds of whom had comorbid PTSD, to either 16 sessions of IPT (n = 37) or usual-care psychotherapy (n = 33). Reassessments took place at 10, 24, and 36 weeks, but it is unclear whether the later stages constituted true follow-up, as treatment could be stretched over that duration. Fairburn and colleagues 25 found that IPT had slower acute onset than cognitive behaviour therapy (CBT) for bulimia nervosa, but that IPT caught up with CBT on follow-up. The National Institute of Mental Health (NIMH) Treatment of Depression Collaborative Research Program reported high relapse rates for acutely remitted major depression at 18-month follow-up of IPT (33%), CBT (36%), imipramine pharmacotherapy (50%), and placebo (33%). 26 More studies need to assess the enduring benefits of IPT for PTSD and for other disorders.
The study highlights the absence of consensus criteria for remission, recovery, and relapse in PTSD research, in contrast to those for the diagnosis of major depressive disorder. 27 Experts in PTSD outcome research should define these terms and use them in assessing outcome in acute and maintenance treatment studies. That the majority of this study’s patients did not respond to treatments indicates the need for further clinical research to enhance good outcomes.
Study limitations include its modest sample size and relatively brief duration of follow-up. The decision to enroll only unmedicated patients may be considered both a study strength and a limitation: it allowed clearer delineation of psychotherapy treatment effects but may have limited representativeness of the sample. The ethical responsibility to offer study nonresponders alternative treatment precluded their inclusion in the follow-up sample; moreover, follow-up of nonresponders would hold little interest. Because treatment-responsive patients entering the follow-up phase were no longer a random sample, this “sieve effect” 28 limits the validity of between-treatment comparisons. Small sample size limited statistical power to find all but very large between-group effects, which should be viewed cautiously: for example, although the differences between PE and RT and between IPT and RT were nearly identical (d = 0.79 vs. d = 0.78), only the former reached statistical significance. This may be a statistical finding without clinical significance. (IPT and PE maintained similar response rates at week 26, 90% and 93% respectively.) A different definition of response might have yielded different results. Study strengths include a rigorous design and careful assessment of interval treatment. The results, especially the between-group comparisons, should be considered preliminary and deserve attempts at replication.
Nonetheless, our within-group analyses provide the first data on the enduring effects of IPT in PTSD and encouragement that patients with chronic PTSD who improve in acute psychotherapy may maintain their gains, at least short term, in the absence of ongoing treatment. These data, while preliminary, have value: as the US National Institutes of Health no longer funds large clinical trials, replication of these early follow-up data may be unfortunately long in coming.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Markowitz receives research funding from the NIMH; salary support from the New York State Psychiatric Institute; modest book royalties relating to psychotherapy (including interpersonal psychotherapy) from American Psychiatric Publishing, Basic Books, and Oxford University Press; and an editorial stipend from Elsevier Press. Dr. Neria is an employee of the New York State Psychiatric Institute and has received royalties from Cambridge University Press and research support from the Mack Foundation, Stand for the Troops, and the New York Presbyterian Hospital. Mr. Choo reports no conflict of interest in the context of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by grant R01 MH079078 from the National Institute of Mental Health (Dr. Markowitz, PI) and salary support from the New York State Psychiatric Institute (Drs. Markowitz, Neria).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.