
Abstract
Objective:
A panel of experts, including researchers, clinicians and people with lived experience, was brought together to develop the new Canadian schizophrenia guidelines for the psychosocial treatment of children and youth with schizophrenia or psychotic disorders.
Method:
The ADAPTE process, which relies on adapting existing high-quality guidelines, was used. Existing guidelines for children and youth (mostly from the National Institute for Health and Care Excellence [NICE]), as well as CPA adult guidelines, were reviewed and discussed in terms of their adaptability to the Canadian context and their level of recommendation for children and youth. New treatments were also considered when recent meta-analyses suggested their usefulness.
Results:
The children and youth psychosocial guidelines include many cross-sectional recommendations in terms of clinical and interpersonal skills needed to work with this clientele, setting and collaboration issues and needed adaptations for specific subpopulations. In terms of specific treatments, the treatments most strongly recommended are family intervention and cognitive behavior therapy. Also recommended, although with different degrees of support, are supported employment/supported education programs, patient education, cognitive remediation, and social skills training. Novel and upcoming psychosocial treatments are also briefly discussed.
Conclusion:
These novel Canadian guidelines for the psychosocial treatment of children and youth with schizophrenia or psychotic disorders report evidence-based treatments as well as important considerations for providers who work with this clientele. More studies with children and youth with schizophrenia and psychotic disorders are warranted. If followed, these guidelines should facilitate the recovery of children and youth with schizophrenia or psychotic disorders as well as the recovery of their families.
The following guidelines have been developed to support clinicians in their delivery of psychosocial interventions to youth and children with schizophrenia spectrum or other psychotic disorders and their families. In the DSM-5, this category includes diagnoses of schizophrenia, schizoaffective disorder, schizophreniform disorder, brief psychotic disorder and delusional disorder. For the sake of concision, we will solely use the term schizophrenia when describing schizophrenia and other psychotic disorders. Numerous psychosocial interventions exist, although few have been empirically studied in youth and children with schizophrenia spectrum disorders. In fact, a recent meta-analysis recommended more studies on psychosocial interventions for youth and children with schizophrenia. 1 In developing our recommendations, the working group has primarily drawn upon the 2014 National Institute for Health and Care Excellence (NICE) 2 guidelines on the treatment and management of schizophrenia in youth and children. Given that psychosocial interventions have been extensively studied for adult populations with schizophrenia, we have also based our guidelines on the Treatment Guidelines on Psychosocial Treatment of Schizophrenia in Adults found in the Canadian Schizophrenia Guidelines. 3
Methods
The methods for the Canadian Schizophrenia Guidelines are described in brief here; please see the Introduction and Guideline Development Process article for an in-depth description. The guidelines were developed using the ADAPTE 4 process. Recognizing that the development of guidelines requires substantial resources, the ADAPTE process was created to take advantage of existing guidelines and reduce duplication of effort.
The first phase of ADAPTE, the set-up phase, involved preparing for the ADAPTE process. We assembled a national multidisciplinary panel from across Canada, including stakeholders with expertise in schizophrenia and mental health, health policy, patient advocacy and lived experience with schizophrenia. Endorsement bodies for the guidelines include the Canadian Psychiatric Association (CPA) and the Schizophrenia Society of Canada, which were also heavily involved in the dissemination and implementation strategy.
The second phase of the ADAPTE process, the adaptation phase, involves identifying specific health questions; searching for and retrieving guidelines; assessing guideline quality, currency, content, consistency and applicability; making decisions regarding adaptation; and preparing the draft adapted guideline. We searched for guidelines on schizophrenia in guideline clearinghouses and on the websites of well-established guideline developers for mental health disorders, including the National Institute for Health and Care Excellence (NICE), 2 the Scottish Intercollegiate Guidelines Network (SIGN), 5 the American Psychiatric Association, the American Academy of Child and Adolescent Psychiatry, and the European Psychiatric Association. A MEDLINE search was also performed using the terms guideline as publication type and schizophrenia as title or clinical topic. Inclusion criteria were that the guideline needed to be published after 2010, the guideline needed to be written in English, and recommendations had to be developed using a defined and systematic process. We identified 8 current guidelines that were potentially suitable for adaptation. These guidelines were reviewed and evaluated in duplicate using the AGREE II tool, 6 an instrument used to evaluate the methodological rigour and transparency with which a guideline is developed. Based on this evaluation, we determined that 6 guidelines were of suitable quality and content for adaptation (see Table 1). Recommendations from each guideline were extracted and divided based on content and were reviewed by the relevant working group. Following the ADAPTE process, working groups selected items from guidelines and recommendations to create an adapted guideline. Each working group carefully examined each recommendation, the evidence from which the recommendation was derived, and the acceptability and applicability of the recommendation to the Canadian context. For the current working group on the children and youth psychosocial guidelines, only the NICE guidelines were used. After reviewing the recommendations from the guidelines, the working groups decided which recommendations to accept and which to reject and which recommendations were acceptable but needed to be modified. Care was taken when modifying existing recommendations not to change the recommendations to such an extent that they were no longer in keeping with the evidence on which they were based. Please see Appendix 1 regarding how and why recommendations in this manuscript were modified from their original form.
Clinical Practice Guidelines Used for the Canadian Schizophrenia Guidelines.
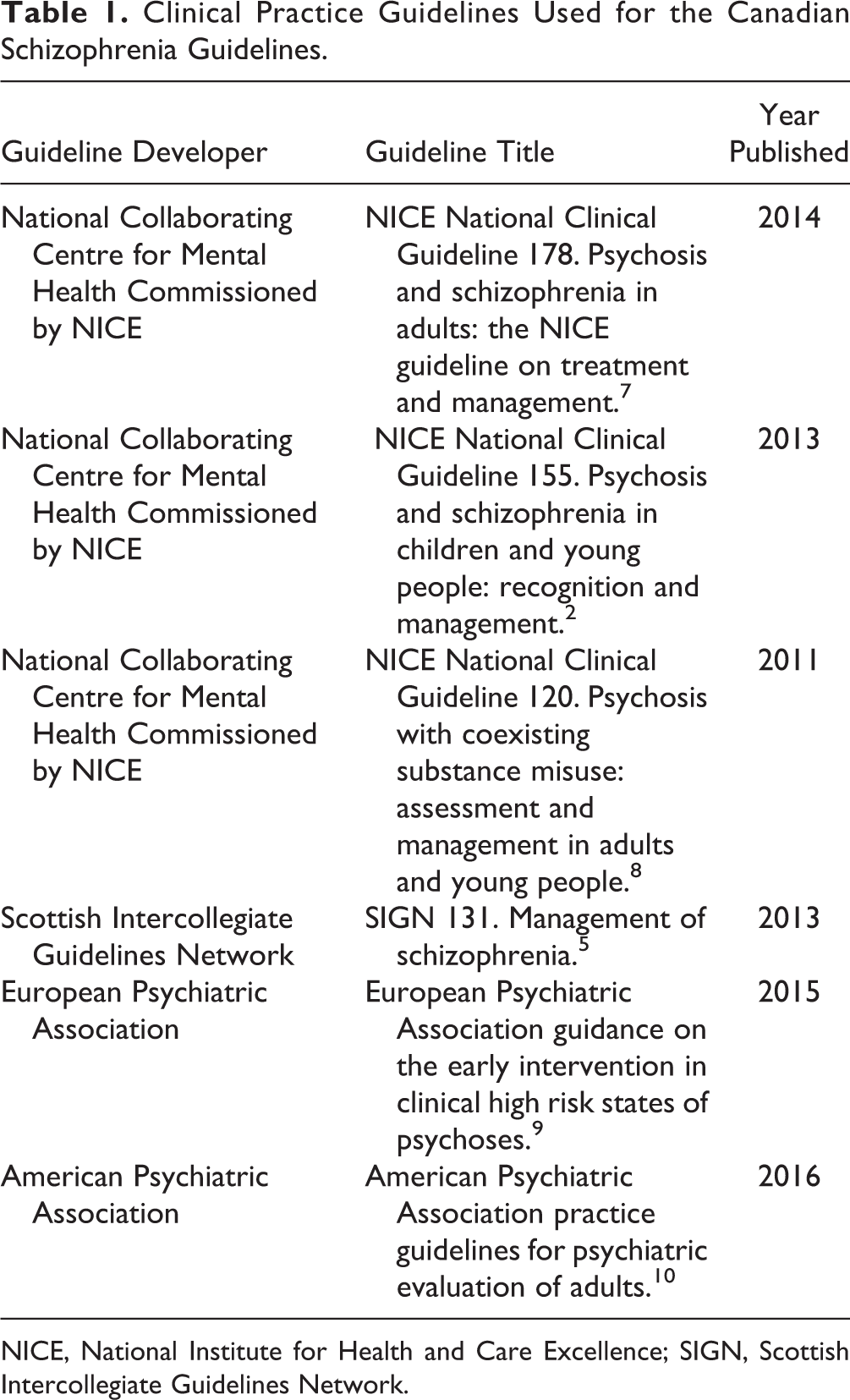
NICE, National Institute for Health and Care Excellence; SIGN, Scottish Intercollegiate Guidelines Network.
De novo recommendations were made in situations where it was believed that a recommendation was needed but none of the existing guidelines provided recommendations addressing the situation or topic. When de novo recommendations were created, the SIGN 5 method was followed for the levels of evidence and the grades of recommendation (see Table 2).
Grade/strength of recommendation classification systems for included guidelines.a
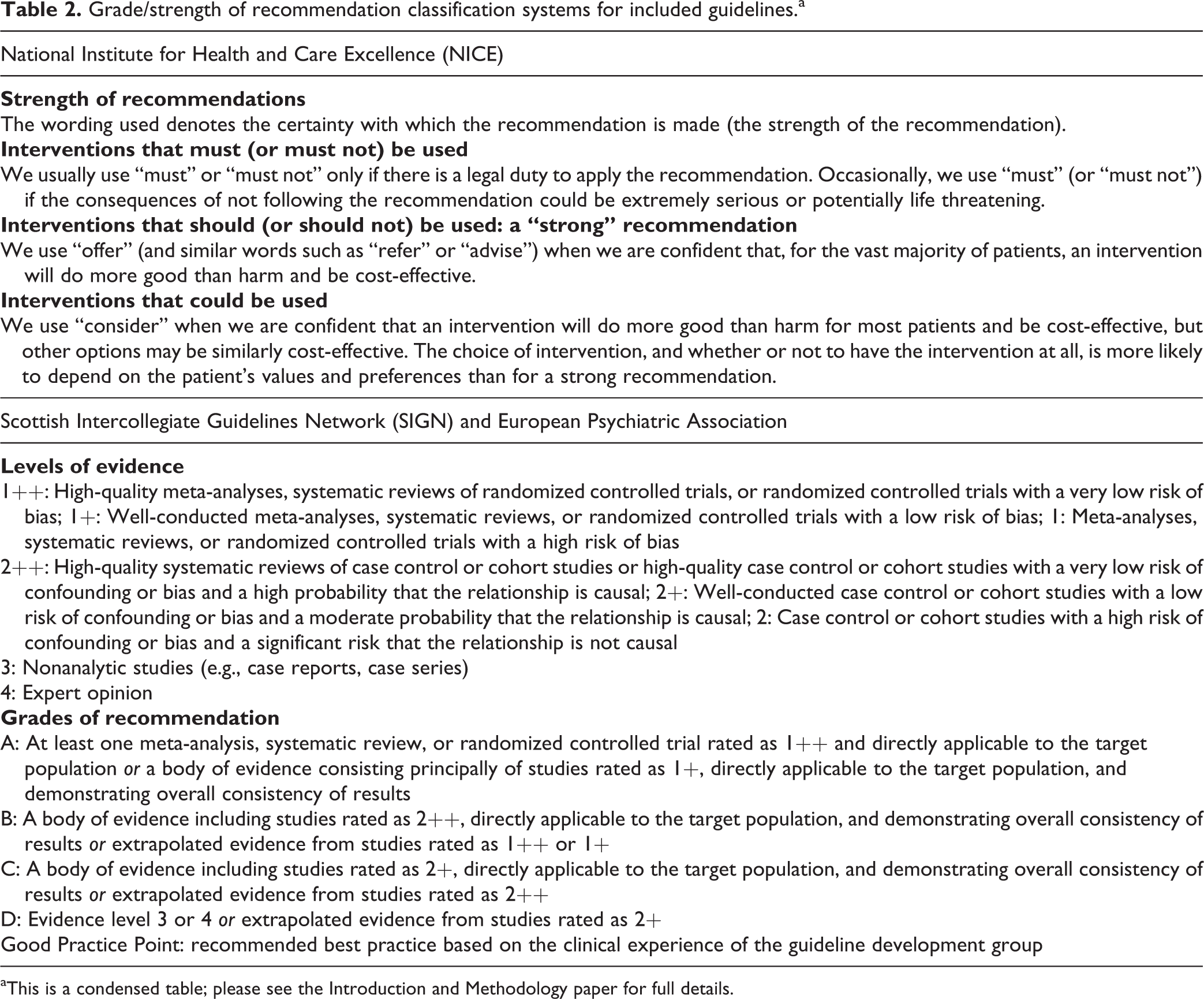
aThis is a condensed table; please see the Introduction and Methodology paper for full details.
Each working group developed a final list of recommendations from the included guidelines that was presented to the entire guideline panel at an in-person consensus meeting. Working group leaders presented each recommendation and its rationale to the panel. Anonymous voting by the entire panel using clicker technology was performed for each recommendation. Recommendations required agreement by 80% of the group to be included in the Canadian guidelines. If a recommendation did not receive 80% agreement, the group discussed the recommendation and whether minor modifications to the recommendation would alter the likelihood that the recommendation would pass. In these situations, recommendations were modified (as described above) and the group re-voted at a later date using an online anonymous survey. Whenever modifications in wording were made to original recommendations, the text “modified recommendation from” appears in the Canadian Schizophrenia Guidelines, and the source of each recommendation is written beside the recommendation statement. The strength or grade of the recommendation is provided in parentheses if applicable, using the system from which the recommendation was taken. The grades of recommendation for each reference guideline and their meaning are explained in brief in Table 2 (see Introduction and Guideline Development Process article for a more detailed description). Once the voting and consensus process was completed, each working group created a separate manuscript that contains all the recommendations adapted from the included guidelines, with accompanying text explaining the rationale for each recommendation.
During the finalization phase, the Canadian Schizophrenia Guidelines were externally reviewed by those who will be affected by their uptake: practitioners, policy makers, health administrators, patients and their families. The external reviewers asked questions about whether the users approved of the draft guidelines, strengths and weaknesses and suggested modifications. The process was facilitated through the Canadian Journal of Psychiatry and the Schizophrenia Society of Canada. The Canadian Psychiatric Association Clinical Practice Guidelines Committee reviewed and approved the guideline methodological process.
Recommendations
The guidelines are presented in bullet form, followed by the origin of the guideline and the level of recommendation (see Special Issue’s Introduction and Guideline Development Process article 11 ).
First, we describe recommendations that overarch psychosocial interventions and that are considered important in the care of youth and children with schizophrenia. For best practice, these guidelines must be used in conjunction with those specific to pharmacological treatment recommendations for children and youth with schizophrenia.
Recommendation 1
Clinicians should work in partnership with parents or carers, as well as children and young people with schizophrenia, while taking into consideration their developmental level, emotional maturity and cognitive capacity.
[NICE (Strong recommendation)]
Recommendation 2
Help, treatment and care should be offered in an atmosphere of hope and optimism, focusing on the child or youth’s recovery.
[NICE (Strong recommendation)]
Recommendation 3
Clinicians need to take time to build trusting, supportive, empathetic and nonjudgmental relationships as an essential part of care.
[NICE (Strong recommendation)]
Recommendation 4
Advise parents and carers about their right to an assessment of their own physical and mental health needs, and explain how to access this.
[NICE (Strong recommendation)]
Recommendation 5
Clinicians working with children and young people with schizophrenia need to be trained and skilled in working with families and need to know the legal and ethical considerations when working with youth and children (e.g., regarding confidentiality and information sharing).
[NICE (Strong recommendation)]
Recommendation 6
Clinicians should foster the child or youth’s autonomy, promote active participation in treatment decisions, support self-management and offer access to peer support (for children and young people of an appropriate developmental level, emotional maturity and cognitive capacity).
[Modified from NICE (Strong recommendation)]
Recommendation 7
Whenever possible, aim at maintaining continuity of individual therapeutic relationships.
[Modified from NICE (Strong recommendation)]
Recommendation 8
When working with children and young people with schizophrenia and their parents or carers, make sure everyone understands confidentiality and its limits. Ensure that the setting is therapeutic and that privacy, safety and dignity are respected.
[NICE (Strong recommendation)]
Recommendation 9
Depending on the young person’s developmental level, emotional maturity and cognitive capacity, a discussion should take place regarding how he or she wants parents or carers to be involved in his or her care. Such discussions need to be repeated at intervals to take account of any changes in circumstances, including developmental level.
[NICE (Strong recommendation)]
Recommendation 10
Clinicians need to make sure that they communicate clearly and verify that they are well understood by parents or carers and the child or young person. This means taking into account the person’s developmental level, emotional maturity and cognitive capacity including any learning disabilities, sight or hearing problems or delays in language development. It also means using plain language where possible, avoiding clinical jargon and using communication aids (such as pictures, symbols, large print, braille, different languages or sign language) if needed.
[Modified from NICE]
Recommendation 11
When working with children or young people and their parents or carers who have difficulties speaking or reading English or French, work with interpreters if possible and recommend educational resources that can provide English or French language teaching.
[Modified from NICE]
Recommendation 12
Clinicians need to gain cultural competence in order to appropriately assess skills and psychosocial needs and to understand culture-specific explanatory models of psychosis as well as culture-specific beliefs regarding psychosis or schizophrenia and related treatment expectations. Clinicians without appropriate cultural competence should seek advice or supervision from health care professionals who are experienced in working transculturally.
[Modified from NICE (Strong recommendation)]
With reference to each of the following recommendations targeting more specific psychosocial interventions, we provide a brief synopsis of the state of the current evidence for effectiveness, as well as some best practice guidelines endorsed by all members of the working group.
Family Intervention
Recommendation 13
Offer family intervention (delivered as set out below) to all families of children and young people with schizophrenia, particularly for preventing and reducing relapse. This can be started as soon as possible, either during the acute phase or later, including within inpatient settings.
[NICE (Strong recommendation)]
Recommendation 14
Family intervention should preferably include the child or young person with schizophrenia. It should be carried out for 3 months to 1 year and should include at least 10 planned sessions. It is important to take into account the whole family’s preference for either single-family intervention or multifamily group intervention. The family intervention should take into account the relationship between the parent or carer and the child or young person with schizophrenia and should encompass communication skills, problem solving and psychoeducation.
[Modified from NICE (Strong recommendation)]
Family members of children and youth with schizophrenia are closely involved in the young person’s care and can play an important role in facilitating treatment and recovery. 12 Family members or carers can experience great distress, which can at times manifest itself in detrimental interactions with the young person. 13 Family interventions that include the elements described above are among the most evidence-based psychosocial interventions, and they improve the recovery of not only the young person but the entire family as well. 14,15 The NICE guidelines describe evidence supporting the efficacy of family interventions (although there are few studies with youth and children) designed to help families deal with the challenges posed by having a close relative with a schizophrenia spectrum disorder. The interventions emphasize providing support and education for the family as well as tools to strengthen family members’ problem-solving and communication skills. It is also recommended to address issues related to crisis management and recovery.
We believe that family interventions should not focus only on the person with schizophrenia; the family needs to work on their recovery as a family.
Cognitive Behavioral Therapy
Recommendation 15
Offer cognitive behavioural therapy (CBT) (delivered as set out below) to assist in promoting recovery in children and young people with persisting positive and negative symptoms and for those in remission.
[NICE (Strong recommendation)]
Recommendation 16
CBT should be delivered by appropriately trained therapists following established, effective protocols, with regular supervision being available. It should be delivered in a collaborative manner and should include established principles of CBT, including teaching patients to monitor the relationships between thoughts, feelings, behaviors and symptoms; reevaluation of perceptions, beliefs and thought processes that contribute to symptoms; promotion of beneficial ways of coping with symptoms; protecting or improving self-esteem; reduction of stress; and improvement of functioning. The minimum dose of CBT should be regarded as 16 sessions.
[Modified from NICE (Strong recommendation)]
There are currently no randomized controlled trials on CBT that specifically target children or youth with schizophrenia. Most of the evidence reviewed by NICE pertains to adult studies and focuses on individual CBT. Studies with individuals described as “first episode of psychosis,” involving late-teens and young adults, have found strong benefits for CBT for psychosis. Although no studies to date have compared individual CBT to group CBT, the literature suggests that group CBT (rather than individual CBT) might be more beneficial for young individuals with psychosis. 16 –18 Given the paucity of evidence regarding the comparative benefits of CBT for psychosis delivered individually versus in a group format for children and youth, we recommend that the young person’s preferences be taken into account and that both formats be made available when possible.
Supported Employment and Supported Education Programs
Recommendation 17
Offer supported employment programs to young people with schizophrenia above compulsory school age who wish to find or return to work.
[NICE (Strong recommendation)]
Recommendation 18
Supported employment programs need to follow the following principles 19 : regular/competitive work is the goal; zero exclusion: anyone who wishes to work can receive supported employment; the mental health team needs to work together with the supported employment team; personal job preference is considered; counselling regarding social benefits is offered; rapid job search (no prevocational training needed); job specialist develops close ties with employers, negotiates accommodations and works at developing new positions; support is offered continuously and without a time-limit.
[Modified from NICE (Strong recommendation)]
Recommendation 19
For children and young people of compulsory school age, liaise with the child or young person’s school and educational authority, subject to consent, to ensure that ongoing education is provided.
[NICE (Strong recommendation)]
Recommendation 20
Consider supported education programs (described below) for children or young people who are of compulsory school age and wish to complete a degree, wish to obtain training prior to looking for employment, have special educational needs or need specific education-related accommodations.
[De novo recommendation (Level of evidence: 1; grade of recommendation, B)]
Recommendation 21
Supported education programs are modeled on supported employment programs and are often offered along with supported employment for young adults and youth. 20 The principles are the same but are transposed to the school environment: regular training/education settings are the goal; zero exclusion: anyone who wishes to study/train and needs support can receive supported education; the mental health team needs to work together with the supported education team; training/schooling preferences are considered; rapid return to school; education specialist develops close ties with schools (and negotiates accommodations when needed); support is offered continuously and without a time limit.
[De novo recommendation (Level of evidence: 1; grade of recommendation, B)]
Recommendation 22
When supported employment/education programs are not available, mental health services should work in partnership with local stakeholders, including those representing minority groups, to enable young people with schizophrenia to stay at work or school and to access new employment (including self-employment) and volunteer and educational opportunities.
[Modified from NICE (Strong recommendation)]
Employment and education are essential domains of one’s mental health recovery. Young people with schizophrenia need to be supported in completing their education and/or finding work in regular settings where they can meet their personal goals. NICE guidelines as well as multiple meta-analyses have shown that the supported employment model is the most effective vocational rehabilitation method for obtaining competitive employment. 19 Although the supported education model has been studied less extensively so far, it shows promise in terms of education or training goals being met. 20
The following psychosocial interventions have less empirical evidence compared with the previous recommendations but are important to mention because they either are in common practice or have promise in terms of empirical support.
Patient Education (or Psychoeducation)
Recommendation 23
Clinicians should give children and young people with schizophrenia, and their parents or carers, information regarding psychosis or schizophrenia. This should include comprehensive written information about the nature of interventions for schizophrenia, including biomedical and psychosocial perspectives on causes and treatment, in an appropriate language or format. Relevant information regarding local and national support groups, resources, and organizations, for children and young people with schizophrenia and their parents or carers, should be provided.
[Modified from NICE (Strong recommendation)]
NICE reports no empirical evidence for education about illness per se having a significant impact on critical outcomes such as symptoms, relapse/rehospitalization, adherence or insight. Nevertheless, NICE and the working group consider it important that education about the nature of psychosis and schizophrenia spectrum disorders be provided to young individuals as well as their families in order to facilitate their empowerment and ability to make informed decisions about illness management. This should include information about factors that contribute to illness onset, course of illness, treatment and recovery.
Cognitive Remediation
Recommendation 24
Cognitive remediation therapy may be considered for young individuals diagnosed with schizophrenia who have persisting problems associated with cognitive difficulties.
[De novo recommendation (Level of evidence, 1; grade of recommendation, B)]
Although the NICE guidelines suggest that cognitive remediation therapy has not yet gathered sufficient empirical evidence to be strongly recommended, recent meta-analyses have shown that cognitive remediation therapy can reduce cognitive deficits in basic cognitive processes such as attention, memory and problem-solving and can have an impact on social functioning. 21,22 A meta-analysis conducted with younger school-aged individuals with schizophrenia also suggested benefits with cognitive remediation, particularly when cognitive remediation was offered along with other psychosocial rehabilitation interventions and was offered in groups. 23
Social Skills Training
Recommendation 25
Social skills training should be available for young individuals who are having difficulty with or are experiencing stress and anxiety related to social interaction.
[De novo recommendation (Level of evidence, 1; grade of recommendation, B)]
NICE guidelines do not recommend systematically offering social skills training. However, mental illness during youth and childhood can negatively affect the acquisition of social skills, which in turn can lead to social awkwardness, isolation, and social anxiety. Social skills training uses basic learning principles to improve interpersonal skills related to social situations, such as conversational skills, making friends and assertiveness. Methods include instruction about the significance of verbal and nonverbal aspects of social behavior, modeling, role playing, behavioral rehearsal, corrective but supportive feedback and behavioral homework with practice to facilitate generalization to the individual’s social environment. A recent meta-analysis suggested that social skills training improves negative symptoms, 24 and another systematic review suggested that such training helps individuals learn to use the targeted skills in the community. 25 Given the importance of improving functional outcomes for children and young individuals with schizophrenia, and the prevalence of social anxiety and deficits in social functioning in this clinical population, we believe that having such interventions available is important. We therefore reiterated the relevant recommendation from the CPA 2005 guidelines.
New Developments
Several promising developments related to psychosocial interventions for schizophrenia could apply to children and youth and thus merit our attention, although more studies are warranted. These include third-wave therapies such as mindfulness interventions, 26 acceptance and commitment therapy 27 and compassion-focused therapy, 28 which aim to help individuals become less emotionally overwhelmed and to learn to distance their distress. Other novel therapies may include avatar therapy for voices, 29 social cognitive training or remediation (for deficits in social perception, emotion regulation and theory of mind) 30 and metacognitive training for cognitive biases linked to psychosis. 31 Youth in particular might be attracted to interventions using social media that help improve uptake of therapeutic skills. 32 An additional area of importance is the development and evaluation of interventions for common comorbidities found in people with schizophrenia, such as anxiety and depression. 33,34 Concurrent disorders related to substance use are addressed in another section of these guidelines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.