
Abstract
Objective:
To predict suicidal ideation in people with schizophrenia, certain studies have measured its relationship with the variables of defeat and entrapment. The relationships are positive, but their interactions remain undefined. To further their understanding, this research sought to measure the relationship between suicidal ideation with the variables of loss, entrapment, and humiliation.
Method:
The convenience sample included 30 patients with schizophrenia spectrum disorders. The study was prospective (3 measurement times) during a 6-month period. Results were analyzed by stepwise multiple regression.
Results:
The contribution of the 3 variables to the variance of suicidal ideation was not significant at any of the 3 times (T1: 16.2%, P = 0.056; T2: 19.9%, P = 0.117; T3: 11.2%, P = 0.109). Further analyses measured the relationship between the variables of stigmatization, perceived cognitive dysfunction, symptoms, depression, self-esteem, reason to live, spirituality, social provision, and suicidal ideation. Stepwise multiple regression demonstrated that the contribution of the variables of stigmatization and perceived cognitive dysfunction to the variance of suicidal ideation was significant at all 3 times (T1: 41.7.5%, P = 0.000; T2: 35.2%, P = 0.001; T3: 21.5%, P = 0.012). Yet, over time, the individual contribution of the variables changed: T1, stigmatization (β = 0.518; P = 0.002); T2, stigmatization (β = 0.394; P = 0.025) and perceived cognitive dysfunction (β = 0.349; P = 0.046). Then, at T3, only perceived cognitive dysfunction contributed significantly to suicidal ideation (β = 0.438; P = 0.016).
Conclusion:
The results highlight the importance of the contribution of the variables of perceived cognitive dysfunction and stigmatization in the onset of suicidal ideation in people with schizophrenia spectrum disorders.
Understanding psychosocial factors that can contribute to suicidality in schizophrenia is a central public health issue. Indeed, the risk of suicide in schizophrenia is 10 to 20 times higher than that of the general population. 1,2 Suicide is the source of 28% of the excess mortality in this group. 3 However, the process leading from suicidal ideation to suicide attempt is not yet well understood.
Between 40% and 80% of people with schizophrenia develop suicidal ideation during the course of their illness, and these ideations are very frequent during the first psychotic episode. 4 –8 Suicide attempts are present in 20% to 50% of persons having suicidal ideation, and 4% to 13% of people with schizophrenia actually die from suicide. 8
Suicidal ideation has attracted attention, as it is associated with an increased risk of suicide attempts, which usually take place before the first psychiatric consultation. 5,9,10 For this reason, suicidal ideation can be considered as an early sign of suicidal behavior. 11 –13
To better understand the development of suicidal ideation, biopsychosocial epidemiological studies 5,9,11,12,14 –31 have been conducted and cognitive models developed to attempt to analyze this development. More than 30 risk factors have been positively associated with suicidal ideation. Consequently, cognitive models have been proposed to better understand the relationships between risk factors and suicidal ideation. 32 –38
Some authors have proposed to conceptualize a psychotic episode as a life event requesting a response to cope with this event. This response depends on how the person appraises (understands and interprets) the psychotic episode. Also, the appraisal is based on the cognitive representation of the consequences of the psychotic episode for the person. What are the cognitive representations of the consequences?
Birchwood et al. 37 –43 developed a model that postulates that these 3 representations are the following: loss, entrapment, and humiliation. The first, loss, means that the psychotic episode limits interpersonal relations and self-fulfillment, resulting in a loss of the roles that the person values, so that he/she is now obliged to accept an inferior status. The second, entrapment, signifies that someone feels trapped because he/she believes that he/she has less and less opportunity to achieve his/her goals and fulfill himself/herself in socially valued roles. The person ends up believing that he/she is no longer able to use his/her skills to assert his/her identity or to experience a feeling of belonging in his/her familiar social environment. 44 The third, humiliation, stipulates that the person feels that his/her social rank has deteriorated due to social prejudices about mental illness that can be likened to stigmatization. However, these studies have focused on depression and have not examined suicidal ideation.
Taylor et al. 35,45 developed a model that applies to suicidal ideation. The model is based on the following assumption: to have suicidal ideation, the person must have the perception of being completely trapped and come to the conclusion that no other option exists. 35,36 To determine this phenomenological condition, the authors drew from concepts of loss (equivalent to defeat) and entrapment 46 identified by Birchwood et al 37 . One original aspect of this model is that certain psychosocial variables interact with defeat and entrapment to predict suicidal ideation. These variables are a) the ability to escape from a difficult situation, which is equivalent to problem-solving skills; b) access to rescue factors (social support); and c) perceived unlikeliness of relief in the future (despair).
Very few studies have examined the relationship between the variables of loss (defeat), entrapment, and humiliation with suicidal ideation. In a meta-analysis 47 of 40 studies, only one addressed these relationships. The findings indicated that the variables of defeat and entrapment explain 31% of the variance of suicidal ideation.
The goal of the current study was to verify if, following a psychotic episode, the 3 cognitive representations (loss, entrapment, humiliation) are related to suicidal ideation in people with schizophrenia spectrum disorders. This study also aimed to determine which other psychosocial variables are related to suicidal ideation.
Method
Study Design and Sample
A convenience sample of 45 participants was recruited from 3 hospitals shortly before being discharged (T1). An interview was completed at 3 months (T2) and 6 months (T3) after discharge. Participants were referred by a medical professional who would select only subjects whose condition allowed them to participate. He presented them with the project, and if they accepted, he informed the researcher who then contacted them. After answering their questions, a consent form was signed with the possibility of opting out at all times.
Each patient had received a diagnosis of a schizophrenia spectrum disorder (DSM-IV-TR criteria), which had to be in agreement by the 2 physicians in charge during intake and before discharge. Other inclusion criteria were being between 18 and 65 years old and being able to answer the questionnaires.
Only 30 of the 45 participants were retained for statistical analyses as explained below. The final convenience sample included 22 men and 8 women. Their mean age was 32.3 years (SD 9.62). Twenty-five participants were unmarried, widowed, or separated. The subjects had a mean of 12.10 years of schooling (SD 2.52). Twenty-six had not been employed at the time of their hospitalization. Their diagnoses according to the DSM-IV-TR were as follows: paranoid schizophrenia (n = 16), schizoaffective disorder (n = 11), and disorganized schizophrenia (n = 3). They had a mean of 4.07 (SD 4.16) previous hospitalizations prior to the current hospitalization. The antipsychotic medication was converted into chlorpromazine equivalents (mean 288.57 mg, SD 251.54 mg).
Instruments
The instruments used were self-administered questionnaires, scored with Likert-type scales. Unless otherwise indicated, the total scores were used for statistical purposes.
The dependent variable was suicidal ideation. The Scale for Suicidal Ideation 48 includes 19 items measuring the degree of severity. The validated French translation has a Cronbach alpha of 0.889. 49
The study included the 3 cognitive variables thought to be related to suicidal ideation and 8 additional variables.
The Personal Beliefs about Illness Questionnaire–Revised, 42 a 19-item instrument, measures the following 3 categories of appraisal/emotion: a) humiliation (6 items); b) entrapment (6 items); and c) loss of purpose, roles, and social status (7 items). It does not provide a total score. The internal consistency scores are 0.567 (humiliation), 0.743 (entrapment), and 0.705 (loss).
The Self-Esteem Scale 49,50 measures the overall perception that a person has of his/her own value. The French translation has been validated in 4 studies (Cronbach alpha scores range from 0.70 to 0.90). 51
The Reasons for Living Inventory 52,53 measures individual beliefs of justifying the choice to live (Cronbach alpha of French translation = 0.93).
Four questions determine the importance of spirituality, the meaning of life, and how spirituality helps one to understand and cope with the challenges of life (Cronbach alpha = 0.85). 54
The Subjective Scale to Investigate Cognition in Schizophrenia, assessing perceived cognitive dysfunction, was developed in French and validated by the authors. 55 It is a 21-item questionnaire measuring 4 domains of cognitive deficits: memory, attention, executive functions, and praxis (Cronbach alpha = 0.879).
The Positive and Negative Syndrome Scale 56 assesses the symptoms of schizophrenia. The internal consistency scores for the French translation 57 are the following: positive scale (0.78), negative scale (0.77), and psychopathological score (0.64).
The Calgary Depression Scale 58,59 measures depression in persons with schizophrenia (Cronbach alpha for French translation = 0.82).
The Stigmatization Scale 60 measures the perception of being socially stigmatized. It is a 21-item instrument. This study used the short form with 9 items (Cronbach alpha = 0.843).
The Social Provisions Scale 61,62 measures perceived social support (Cronbach alpha of French translation = 0.93).
Table 1 presents the mean, standard deviation, and Cronbach alpha for the pathological and social variables described above at the 3 measurement times.
Mean, standard deviation, and Cronbach alpha for pathological and social variables, evaluation variables, and suicidal ideation.
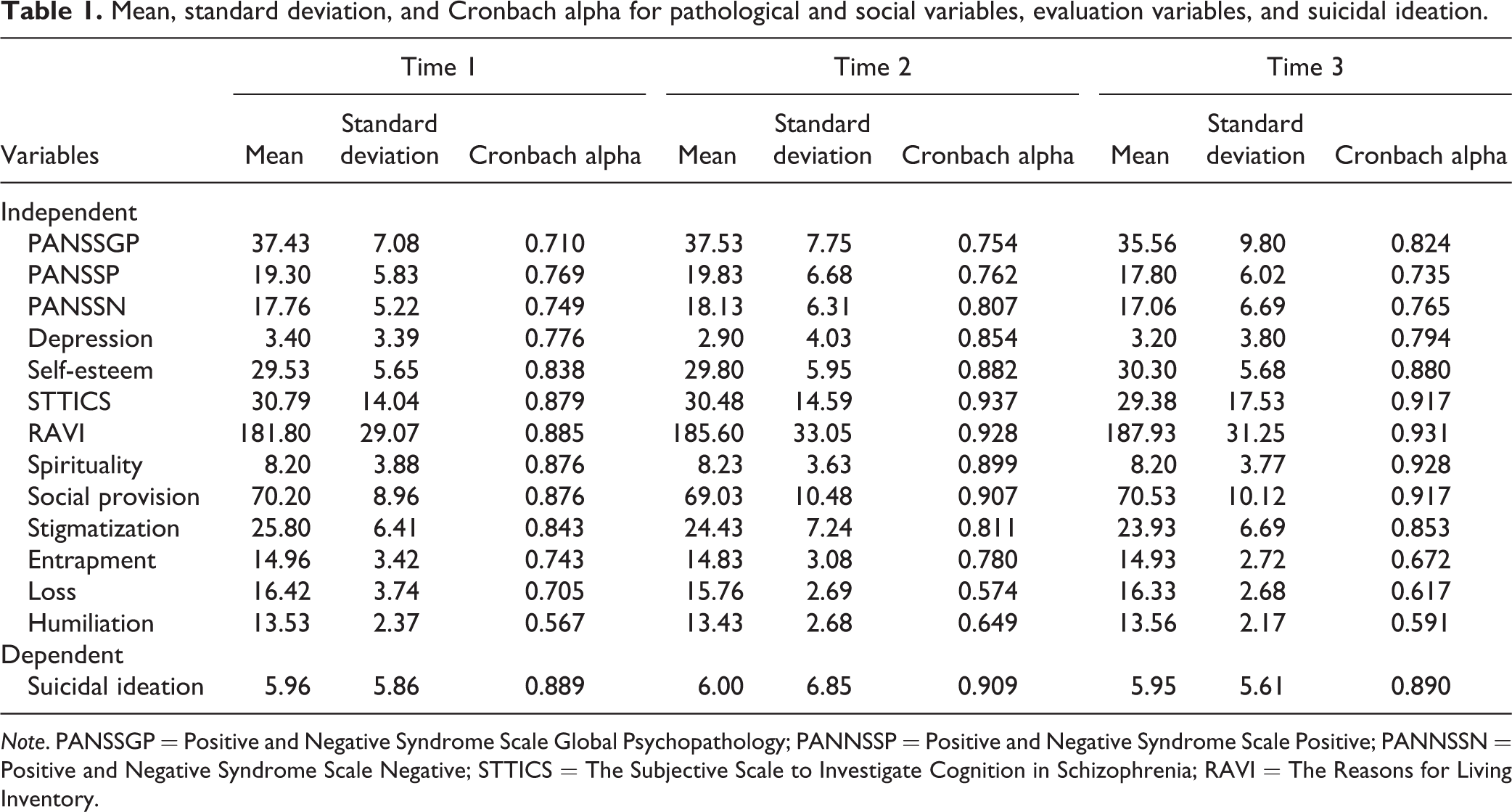
Note. PANSSGP = Positive and Negative Syndrome Scale Global Psychopathology; PANNSSP = Positive and Negative Syndrome Scale Positive; PANNSSN = Positive and Negative Syndrome Scale Negative; STTICS = The Subjective Scale to Investigate Cognition in Schizophrenia; RAVI = The Reasons for Living Inventory.
Statistical Analysis
Various statistical analyses were carried out. To measure internal consistency, Cronbach alpha was used, and univariate correlations were determined with the Pearson test. To measure the contribution of independent variables to the variance of suicidal ideation, multiple regression was used with a stepwise method.
Results
Before proceeding with statistical analyses, verification of the multiple regression hypotheses was completed. Analyses did not show any departure from the assumptions or multicollinearity for independent variables. Verification only highlighted that the dependent variable did not have a normal curve. Various corrective statistical measures were attempted to normalize the dependent variable but were unsuccessful except for the following: the exclusion of 15 of the 45 subjects with no suicidal thought at each measuring time. Hence, the sample was reduced to 30 subjects for statistical necessity.
Cognitive Representations (Loss, Humiliation, and Entrapment)
The analysis of the univariate relationship (Pearson R) between the 3 cognitive representations and suicidal ideation highlighted 3 findings: Mixed results. At T1, all 3 representations were significantly related to suicidal ideation. Yet, at T2, their significance varied. Entrapment was significantly associated with suicidal ideation at T2 and T3 and loss only at T2, while humiliation was not significant at either time (Table 2). Stability over time. The scores for suicidal ideation and the 3 representations remained stable over the 3 periods according to the Tukey honest significant difference test (suicidal ideation: P = 0.751; loss: P = 0.638; humiliation: P = 0.979; entrapment: P = 0.983) (Table 1). Contribution to Variance in Suicidal Ideation. The contribution of the 3 variables to the variance of suicidal ideation was not significant at any of the 3 times. Similarly, no individual variable contributed significantly to this variance (Table 2).
Multiple regression of 3 cognitive variables on suicidal ideation.
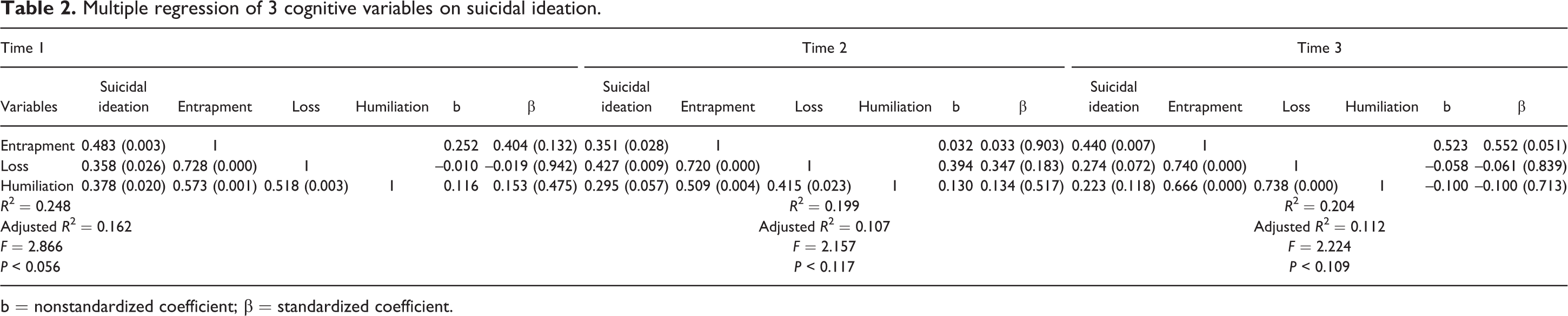
b = nonstandardized coefficient; β = standardized coefficient.
Perceived Cognitive Dysfunction and Stigmatization
Following these results, a regression equation was conducted to verify whether, in addition to the variables of entrapment, loss, and humiliation, the other 8 variables contributed to the variance of suicidal ideation. Of these 11 variables, we selected the 6 variables that were significantly correlated with suicidal ideation at T1: stigmatization (0.613; P = 0.000), perceived cognitive dysfunction (0.502; P = 0.005), entrapment (0.483; P = 0.003), humiliation (0.378; P = 0.020), spirituality (0.364; P = 0.048), and loss (0.358; P = 0.026).
A stepwise regression analysis of the 6 variables and suicidal ideation was then carried out. The 2 variables that contributed the most to the variance in suicidal ideation at T1 were perceived cognitive dysfunction and stigmatization. After verifying for assumptions and multicollinearity, multiple regression of these 2 variables (perceived cognitive dysfunction and stigmatization) on suicidal ideation at each measurement time was performed (Table 3).
Multiple regression of stigmatization and perceived cognitive dysfunction variables on suicidal ideation.
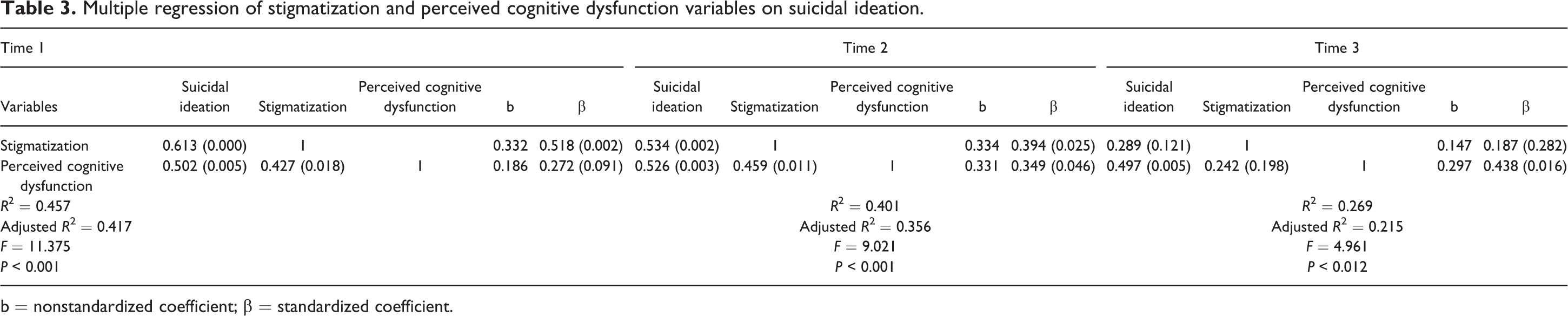
b = nonstandardized coefficient; β = standardized coefficient.
Two key results emerged: The contribution of perceived cognitive dysfunction and stigmatization to the variance of suicidal ideation was significant at all 3 times (T1: 41.7.5%, P = 0.000; T2: 35.2%, P = 0.001; T3: 21.5%, P = 0.012). At T1, only stigmatization contributed significantly to the variance of suicidal ideation (β = 0.518; P = 0.002). At T2, both variables contributed significantly: stigmatization (β = 0.394; P = 0.025) and perceived cognitive dysfunction (β = 0.349; P = 0.046). At T3, only perceived cognitive dysfunction contributed significantly to suicidal ideation (β = 0.438; P = 0.016).
Discussion
Appraisal (Entrapment, Loss, and Humiliation)
Contribution to the variance in suicidal ideation
Although all 3 representations were correlated with suicidal ideation, particularly at T1, they made no significant contribution to the variance of suicidal ideation. This result is not in accordance with previous studies, which concluded that the variables of defeat and entrapment mediated the association between positive symptoms and suicidal ideation. 45 Based on these findings and those of Birchwood et al. 37 –42 , it is plausible to suggest that the absence of significant results is due to a lack of statistical power. Moreover, because the probability is just above the threshold of 0.05 at T1, it seems difficult to reject the hypothesis of a relationship between the variables of loss, entrapment, and humiliation and suicidal ideation before replicating with a larger sample.
Individual correlations with suicidal ideation
Even though the scores of the measurement scales for the variables of entrapment, loss, and humiliation and suicidal ideation remained stable over time, there was a gradual decline in the strength of correlations between these variables. Various factors may account for this trend. As studies on coping have demonstrated, 63 patients may, in a situation where they have little or no influence, rely on cognitive strategies that do not modify the situation but diminishes its importance. Various coping strategies (emotion-oriented coping) allow them to control the stress related to schizophrenia spectrum disorders. 64 The patients would then be less affected or not affected by the situation.
Entrapment was the only variable that maintained a significant correlation over time. As mentioned previously, a person with a schizophrenia spectrum disorder enters a lifestyle marked by psychiatric care, relapses, and most often social contacts that are limited to other psychiatric patients. Employment opportunities are radically reduced and induce a feeling of being trapped by the illness. In other words, the social consequences of not being able to experience self-fulfillment and the gradual deterioration of skills, among others, reinforce the perception that he/she cannot escape the feeling of being trapped by his/her illness. 65 All these consequences are grouped together under “psychosis-related events,” 66 and patients are unable to change them possibly because of a lack of personal or social resources (coping) to escape from the situation.
Stability of scores over time
The mean scores of entrapment, loss, and humiliation and suicidal thoughts remained stable. T1 was when the hospitalization period ended. We assume that the participants were becoming aware of the consequences of their psychotic episode: life in the patient care unit, treatment, and comprehensive case management, among others. They experienced withdrawal from their social environment, loss of social status, prejudice, and a feeling of being trapped.
The patients could hope that being released from the hospital would mean leaving the medical setting and resuming independent life (context of T2 and T3). However, it appears that was not the case. When they left the hospital, the participants moved into a similar psychiatric environment characterized by daily drug therapy, the company of other psychiatric patients in specialized residences, and unemployment. The experience of not regaining their social status and being victims of social prejudice keeps them entrapped in their mental illness. It is therefore not surprising that the level of suicidal ideation remained high.
Variables of Perceived Cognitive Dysfunction and Stigmatization
Contribution to the variance in suicidal ideation
Perceived cognitive dysfunction and stigmatization had a direct and lasting contribution to the variance in suicidal ideation. Numerous studies have shown that stigmatization of mental illness and perceived cognitive dysfunction really exist, independently of patients’ perceptions. 67,68 In the same way for psychosis, these 2 variables constitute stressful events, needing to be coped with and leading to suicidal ideation when failing to deal with them.
Individual contributions of perceived cognitive dysfunction and stigmatization
Stigmatization contributed to the variance of suicidal ideation at T1 and T2, and perceived cognitive dysfunction did so at T2 and T3. We suggest that an interaction between the individual and the environment may account for this change. When patients leave the hospital, they are primarily concerned with negative reactions. They had experienced a complete disconnect from their social contacts during hospitalization. Diminished social interactions with others is widely considered the most stigmatizing aspect of the illness, accounting for more than 50% of the experience of stigmatization. 69 Gradually, as the months pass, it is possible that the support received following discharge becomes a good way to counter the impact of social prejudice. The patients may also develop coping strategies regarding stigmatization that diminish its impact. Some studies 64,70,71 have demonstrated that to cope, patients use cognitive strategies. For example, by devaluing areas such as work in which they perform less well, patients thus preserve their self-esteem. Social comparison to other patients is another strategy that leads them to believe that others may be experiencing an even worse situation.
After their discharge from the hospital, with regard to perceived cognitive dysfunction, patients may be less concerned with the satisfaction of their needs (affective, housing, etc.) because these are managed, for example, by alternative living environments in which they are housed. The patients are aware of their cognitive deficits, but because they have less need to make use of their cognitive skills after just leaving the hospital, the deficits’ contribution to suicidal ideation is lower. However, the contributive weighting increases with time as they gradually want or are invited to look after needs, a demand that makes them aware of their deficits.
An integrative cognitive model of suicidal ideation
Contrary to the cognitive models of Birchwood et al. 42 and Taylor et al. 35 centered on the appraisal of the event (psychotic episode), as evaluated by the 3 representations of loss (defeat), humiliation, and entrapment, this research illustrates the likely influence of a second appraisal. This suggestion is congruent with the transactional model of stress and coping, 72 which postulates that the impact of a stressor is mediated by primary and secondary appraisals. In the primary appraisal, the person evaluates whether the stressful event represents a threat, and if so, the person conducts a second appraisal about his/her coping strategies as to whether they are available and effective. If it is not the case, suicidal ideation may arise if the answer is no. This secondary appraisal of the ability to change the representations of the stressor is a more powerful determinant of suicidal ideation as it confirms to patients that it is impossible for them to get out of their situation (entrapment).
Conclusion
Despite the fact that further studies are needed to verify their validity and generalizability, the findings in the current research underscore the importance of promptly intervening with patients and their families. The results also highlight the need to widen the inventory of coping strategies for patients and to educate them on how to use these wisely. The results additionally strongly support actions to combat stigmatization around mental illness and facilitate the integration of patients into more welcoming housing and work environments.
Clinical Implications
This study suggests that further research should consider people’s personal and social capacities to handle events (which take concrete form as perceived cognitive dysfunction and stigmatization).
Our results highlight the fact that people with psychosis must cope with more than just one illness. They must also deal with the various realities associated with that illness.
Clinicians should integrate these realities into cognitive models of suicidal ideation in people with schizophrenia.
Limitations
The small number of subjects may have resulted in a statistical power issue. It also limits the possibility of measuring the hierarchical importance of the contribution of several predictors to the variance in suicidal ideation.
The limited number additionally restricts the generalizability of our results.
Another aspect is the correlational nature of this study, which means that we cannot measure the causality of the predictors. For this reason, we must analyze the hypothetical explanations of the results with caution.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was funded by the Social Sciences and Humanities Research Council of Canada (SSHRC) 410-2004-0185.