
Abstract
Objective:
To contribute to a better differential clinical categorisation of delusional disorder (DD) versus schizophrenia (SZ) and to add and complete evidence from previous clinical studies of DD compared to schizophrenia.
Methods:
A cross-sectional study using a clinical sample of 275 patients (132 patients with DD) was studied. Patients were consecutively attending public clinics located in urban and rural areas in both Andalusia and Catalonia (Spain). All participants met DSM-IV diagnostic criteria for either DD or SZ. Data were gathered on sociodemographics, illness duration, Barona-Index estimation of intelligence quotient (IQ), and global functioning, along with a thorough psychopathological assessment using the Positive and Negative Syndrome Scale (PANSS). Comparisons between both groups were calculated using χ2, Student t, and multivariate analysis of covariance tests.
Results:
Patients with DD were older (mean [SD], 50.3 [14.6] years vs. 36.6 [11.1] years; t = 8.597; P ≤ 0.0001), were more frequently married (45.4% vs. 10.8%; χ2 = 38.569; P ≤ 0.0001), and had a higher mean estimated premorbid IQ (111.4 vs. 105.4; t = 2.609; P ≤ 0.01). On the other hand, SZ patients were predominantly male (71.4% vs. 48.9%; χ2 = 14.433; P ≤ 0.0001) and had greater work-related disability than DD patients (20.5% vs. 50.3%; χ2 = 19.564; P ≤ 0.001). Overall, the DD group showed a less severe PANSS psychopathology than SZ group. Thus, total mean (SD) PANSS scores for schizophrenia and delusional disorder, respectively, were 76.2 (22.4) versus 54.1 (18.4) (t = –8.762; P ≤ 0.0001). Moreover, patients with DD showed a better global functioning than those with SZ (62.7 [13.2] vs. 51.9 [16.9]; F = 44.114; P ≤ 0.0001).
Conclusions:
DD is a milder and distinct disorder compared to SZ in terms of psychopathology and global functionality.
Historically, schizophrenia (SZ) has been a much better profiled category than delusional disorder (DD). In 1838, Esquirol made the first comprehensive description of paranoia, labelling it as a partial psychosis. 1 Later in 1863, Kahlbaum recovered the term paranoia, applying it to a disorder presenting delusions as main symptoms. According to him, ‘paranoia’ was a partial psychosis affecting only intellectual functions, preserving other areas of mental functioning and showing a persistent delusional behaviour. 2 However, for most of the 20th century, paranoia had been considered as some sort of mild version of SZ. The 1987 DSM-III-R 3 reintroduced the current concept of DD, which somewhat parallels that of paranoia from Emil Kraepelin, 4 who defined paranoia as a disorder characterised by chronic nonbizarre delusions and no evolution to defective states, unlike dementia praecox (schizophrenia). Currently, DD is well established as a psychosis characterised essentially by the presence of one or more delusions that persist for at least 1 5 or 3 months, 6 in which the presence of bizarre delusions or nonprominent hallucinations consistent with the delusional theme are now within its diagnostic criteria. 5 In addition, a relative preservation of psychosocial activity and absence of unusual or strange behaviour tends to occur. 5,6
To date, only a few comparative studies have approached the differences between DD and SZ assessing different clinical phenomena simultaneously. The lack of studies could be due to a low prevalence of the disorder 7 and/or DD clinical particularities, such as the combination of a relatively high functioning level along with a prominent lack of insight, which may have limited achievement of optimal sample sizes. 8 A general population-based sample study in Finland with 8028 subjects assessed the descriptive and predictive validity of DD and featured this as a disorder with a later age onset, absence of symptoms other than delusions, and a relatively good outcome. 9
Very recently, a comparison study 10 including 146 patients with DD has shown differences between disorders in 40 variables. This study featured DD as a distinct disorder compared to both paranoid SZ and nonparanoid SZ. DD patients tend to experience fewer, but more severe delusions than individuals with SZ. DD patients also tended to have higher prevalence of previous drug abuse, better premorbid sexual adjustment, later age of illness onset, higher level of affective disorder as depression or depressive symptoms and lack of insight, a poorer response to antipsychotics and a better functioning, including paid work. Predominance of somatic and jealousy delusions appeared confined to individuals with DD.
Similarly, previous studies suggest that patients with DD were more likely to be female 11 and married, 10 –12 present an older age of onset, 10 and have a higher proportion of immigrants than patients with SZ. 12 Moreover, the DD group showed relatively little occupational impairment and high psychiatric comorbidity as affective symptoms 13,14 and suicidal behaviour. 15 From a psychopathological perspective, the Halle Delusional Syndromes Study by Marneros et al. 16 (the HADES study) showed that DD appears to be milder than SZ. First-rank symptoms, relevant negative symptoms, and primary hallucinations did not occur in patients with DD. However, a recent study of first episodes has challenged this statement. 17 As for functionality, Marneros et al. 16 showed that patients with DD showed better functionality than subjects with paranoid SZ. Conversely, a recent study has denied the classical perception of a better global functioning for patients with DD. 17 We aimed at adding some new data (such as cognitive information) and replicating findings from previous attempts at confirming that DD is a distinct clinical category compared to SZ. The aim of this study is to contribute to a better differential clinical profiling of DD versus SZ using a relatively large cohort of well-characterised DD patients.
Methods
Sample
A cross-sectional clinical sample of 275 patients (132 patients with DD and 143 patients with SZ) was used. The sample was created by combining data from 3 independent studies using comparable assessment methods. Each study had a single interviewer for the clinical and psychopathological assessments who were all formally trained by the same senior trainer (J.A.C.). Thus, the sample was composed of individuals from 3 different studies: the GENIMS study 18 (DD/SZ = 23/76), the Paragnous study 19 (DD/SZ = 23/67), and the DELIREMP study 11 (DD/SZ = 86/0). To detect potential measurement bias in both Positive and Negative Syndrome Scale (PANSS) and Global Assessment of Functioning (GAF) evaluations made by different raters and across studies, we used intergroup 1-way analysis of variance (ANOVA) and calculated Cronbach’s alpha to analyse the internal consistency of the different PANSS dimensions. Thus, we tested whether internal consistency remained high despite the existence of different raters. PANSS dimensions had been previously validated using a large sample composed by patients with SZ, DD, and schizoaffective disorder (SAD). 18 In brief, such dimensions were the following: manic (excitement, hostility, anxiety, uncooperativeness, unusual thought content, poor impulse control), negative (blunted affect, emotional withdrawal, poor rapport, social withdrawal, difficulty in abstract thinking, motor retardation, disturbing of volition, active social avoidance), depression (somatic concern, guilt feelings, depression, preoccupation), positive (delusions, hallucinations, grandiosity, suspiciousness, lack of judgment and insight), and cognitive (conceptual disorganisation, stereotyped thinking, mannerism and posturing, disorientation, poor attention). That factor structure was very similar to another obtained by van der Gaag et al. 20 Participating patients were consecutive attendees to psychiatric outpatient clinics, and all were in a stable stage of their disorder and on antipsychotic medication in all cases. The clinical settings were public or private mental health services integrated or commissioned by the Spanish National Health Service located in Andalusia (GENIMS and Paragnous studies) and Barcelona, Catalonia (DELIREMP study). Patients belonging to the Paragnous study were recruited as consecutively attending 2 rural community mental health centres, 2 hospitals, and 3 urban community mental health centres from several locations from Andalusia. All were diagnosed by a clinical interview by a fully trained psychiatrist using DSM-IV criteria. Patients of the GENIMS study belong to 3 urban community mental health centres from Andalusia. They were recruited while consecutively attending mental health centres and were diagnosed using the Structured Clinical Interview for DSM-IV Axis I disorder (SCID-I). 21 Regarding patients of the DELIREMP study, all were randomly selected from a computerised DD case register from 5 urban community mental health centres in Barcelona. All were diagnosed using the SCID-I. 21
Inclusion criteria were as follows: 1) meet DSM-IV diagnostic criteria for SZ and DD, respectively; 2) be older than 18 years; and 3) agree to participate. Exclusion criteria were as follows: 1) mental retardation and 2) any type of dementia. All participants received a study instruction sheet giving sufficient information to enable them to sign the informed consent, which they returned a signed copy thereof. The study was performed in accordance with ethical standards of the 1964 Helsinki Declaration and was approved by the local ethical committees of every participating hospital.
Assessment
Sociodemographic and clinical variables such as sex, age, educational level, employment, marital status, and years after onset were recorded. To estimate each participant’s premorbid intelligence quotient (IQ), a Spanish version of the Barona index 22 was used. This formula uses the sociodemographic variables of age, sex, educational level, urbanicity, and geographical region to estimate the participant’s IQ.
The Spanish version of PANSS 23 was used to measure psychopathology, since PANSS is the standard scale valid and reliable for this purpose. 24 PANSS is a measurement instrument designed to evaluate positive and negative symptoms in SZ. It is composed of 30 items: 7 items for the positive scale, 7 items for the negative scale, and another 16 different items for general psychopathology. Item scores for increasing symptom intensity range from 1 to 7.
Global functioning was assessed using the GAF. 25 The GAF is a standard procedure to measure global outcomes in psychiatric patients within a continuum ranging from a state of total health to another of maximum illness. It is composed of only 1 item, ranging from 100 points (satisfactory performance on a whole array of activities and excellent evaluation of values and personal qualities by others) to 1 point (manifest death expectation).
Statistics
Descriptive statistics for age, sex, educational level, employment, Barona index, marital status, duration of the disorder (in years), GAF score, and PANSS score for the different diagnostic groups were calculated. As a proxy method to study the interrater reliability between the different studies, we used intergroup 1-way ANOVA and estimated Cronbach’s alpha to analyse the internal consistency of the different PANSS dimensions obtained, as explained above. Differences between both groups were evaluated using χ2 when qualitative variables were involved (sex, marital status, employment, and educational level) and Student t test for continuous variables such as age, Barona index, duration of disorder, or psychopathology. The analysis of covariance (ANCOVA) technique was done to control the impact of age, sex, marital status, and psychopathology over GAF scoring and to study the impact of age over PANSS scoring. In all cases, significance was assumed with P < 0.05. All calculations were performed with SPSS 20.0 (SPSS, Inc., an IBM Company, Chicago, IL, USA).
Results
Description of the Sample
Mean GAF scores were significantly higher in the DELIREMP study 11 (composed of DD patients only) than in the other 2 studies (GENIMS 18 and Paragnous 19 ), which were composed of a mix of patients with DD and SZ. In addition, the DELIREMP 11 study sample (composed of patients with DD only) showed lower mean scores on the PANSS than those from the GENIMS 18 and the Paragnous 19 studies (see Table 1). Cronbach’s alphas for PANSS dimensions were as follows: manic, 0.80; negative, 0.91; depression, 0.60; positive, 0.73; and cognition, 0.79.
Mean (SD) Values on the Clinical and Functioning Assessment for the 3 Different Studies.
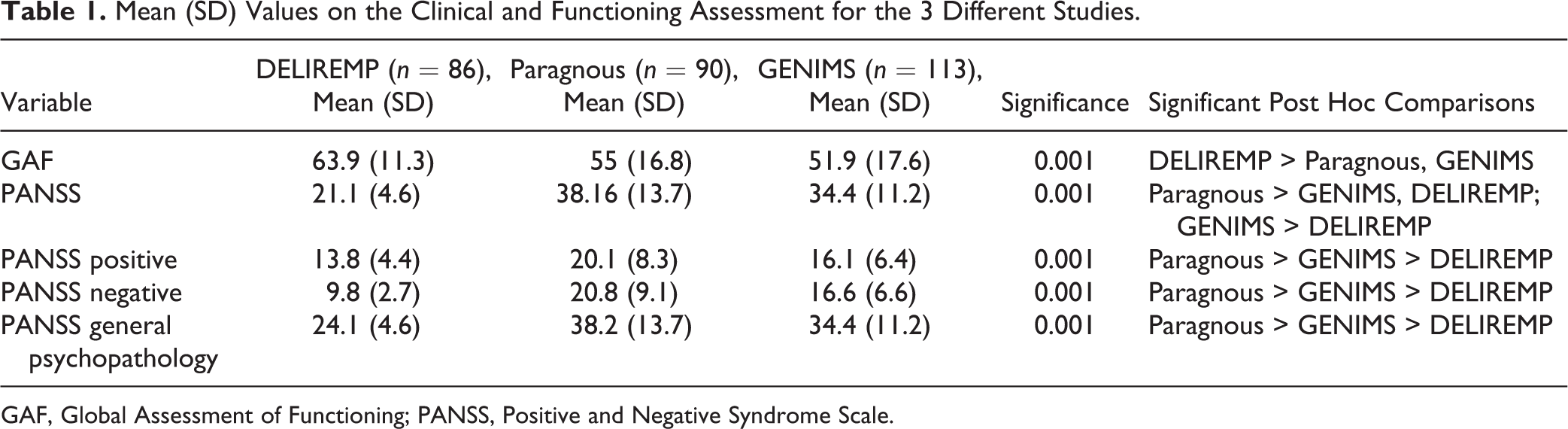
GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale.
Sociodemographics
Our aggregated sample included 275 patients (132 with DD and 143 with SZ). Main sample’s characteristics are described in Table 2. The mean (SD) age was 42.1 (14.6) years; 60.5% were men, 38.9% reached high school or university, 26.4% were married or living with a partner, and 42.2% were either unable to work or on sick leave. The mean (SD) number of years prior to the onset of the disorder was higher among DD patients (12.3 [11.9] vs. 6.4 [7.6] years; t = 3.951; P ≤ 0.0001) than among SZ patients.
Sociodemographic Characteristics of the Sample.
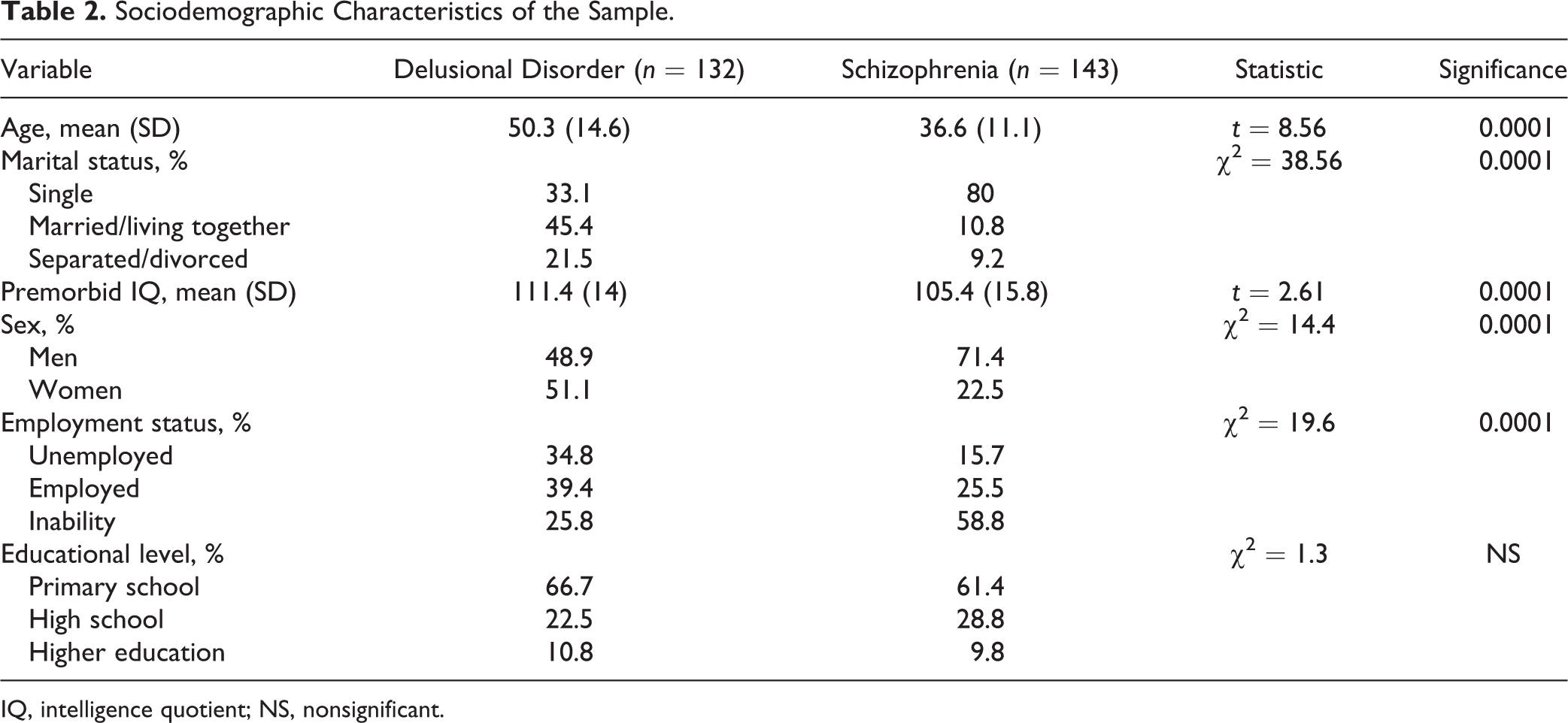
IQ, intelligence quotient; NS, nonsignificant.
Patients with DD were older (mean [SD], 50.3 [14.6] years vs. 36.6 [11.1] years; t = 8.597; P ≤ 0.0001), were more frequently married (45.4% vs. 10.8%; χ2 = 38.569; P ≤ 0.0001), and had a higher estimated IQ (111.4 vs. 105.4; t = 2.609; P ≤ 0.01). On the other hand, patients with SZ were predominantly males (71.4% vs. 48.9%; χ2 = 14.433; P ≤ 0.0001), had more inability to work, or were on sick leave compared to patients with DD (20.5% vs. 50.3%; χ2 = 19.564; P ≤ 0.001). There no were statistical significant differences in education level between both disorders.
Psychopathology
Overall, DD showed a less severe PANSS psychopathology than SZ. Thus, total mean (SD) PANSS scores for SZ and DD, respectively, were 76.2 (22.4) versus 54.1 (18.4) (t = –8.762; P ≤ 0.0001). As for PANSS subscales, results were as follows: positive symptoms, 18.9 (7.6) versus 14.9 (5.9) (t = –4.723; P ≤ 0.0001); negative symptoms, 20 (7.9) versus 11.6 (5.6) (t = –10.029; P ≤ 0.0001); and general symptoms, 37.3 (11.9) versus 27.6 (10) (t = –7.149; P ≤ 0.0001) (Table 3). We repeated these comparisons adjusting for age (given age differences among the SZ and DD groups), and including age did not alter the above results.
Assessment Psychopathology Scale by Clinical Group.
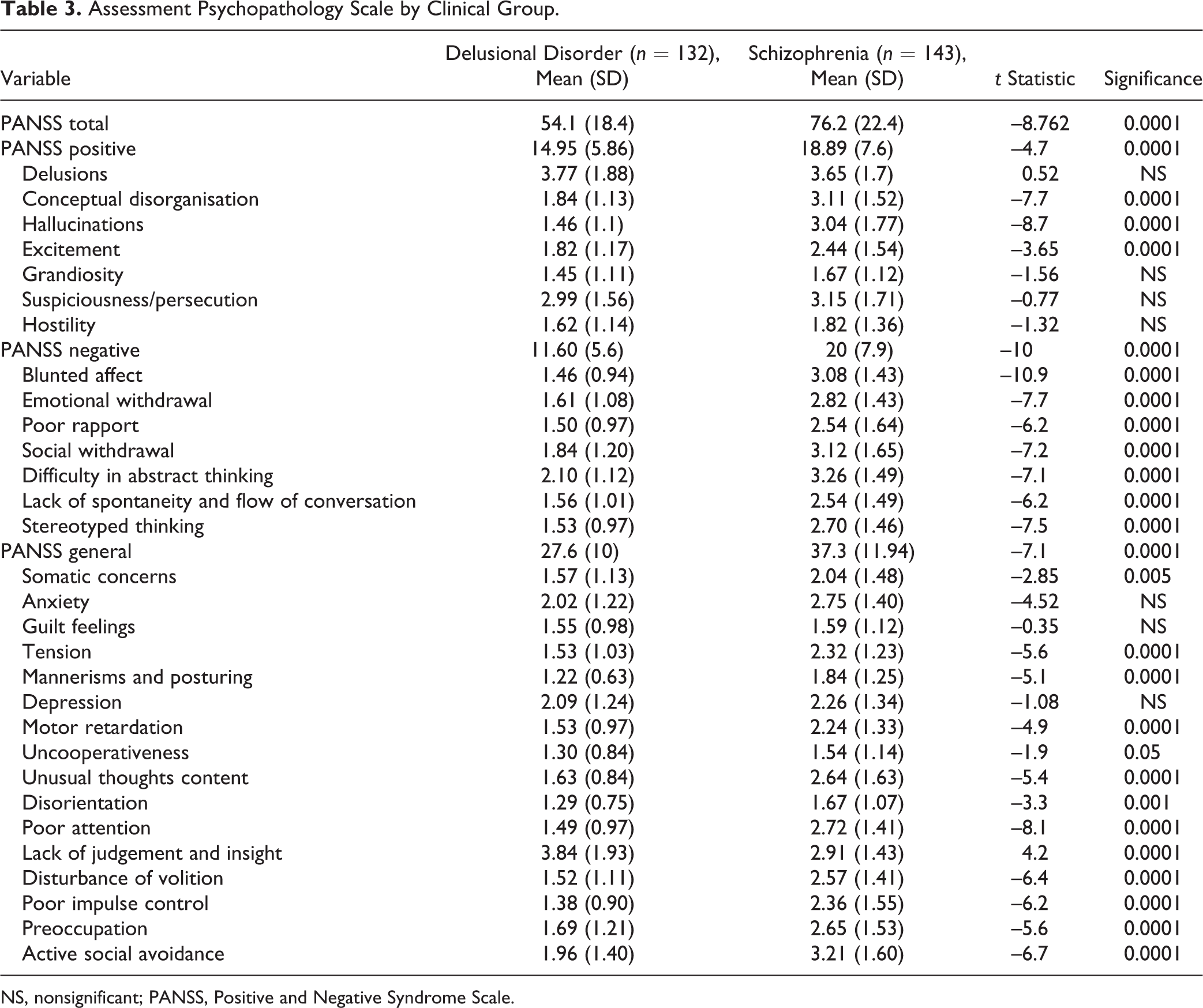
NS, nonsignificant; PANSS, Positive and Negative Syndrome Scale.
When we looked more thoroughly into DD core clinical symptoms, we found no significant statistical differences in delusion scores on the PANSS between both disorders (3.6 [1.7] for SZ vs. 3.8 [1.9] for DD; t = 0.517; P ≤ 0.605), but there were differences for hallucinations (1.5 [1.1] for DD vs. 3 [1.8] for SZ; t = –8.762; P ≤ 0.0001). Hallucinations were nearly nonexistent in DD. Negative symptoms were also much less intense among DD patients than in the SZ group, as PANSS negative subscale scores among SZ nearly doubled those found among DD patients.
The SZ group presented higher scores than the DD group on conceptual disorganisation, excitation, somatic concerns, tension, mannerism and posturing, motor retardation, uncooperativeness, unusual thoughts contents, disorientation, poor attention, disturbance of volition, poor impulse control, preoccupation, and active social avoidance but not on either lack of judgment or insight scores (Table 3).
From a functional viewpoint, patients with DD showed better global functioning than those with SZ both on crude analysis and also when it was adjusted by sex, age, marital status, and total PANSS scoring (62.7 [13.2] vs. 51.9 [16.9]; F = 44.114; P ≤ 0.0001).
Discussion
This is one of the few studies to compare psychopathology and other clinical features between DD and SZ, and it has a large sample of DD patients, similar to Peralta and Cuesta. 10 As a result, DD emerges as a distinct category from SZ. Patients with DD were older and showed more years of disease progression, had a higher premorbid IQ, got married more frequently, and experienced lower disability and less severe psychopathology than patients with SZ, except for lack of judgment and insight. From this perspective, overall, DD seems to be a milder psychotic disorder than SZ. Our study used one of the 2 largest existing samples reported to date, confirming that DD appears to be a distinct disorder from SZ from clinical, sociodemographic, and functional perspectives. Thus, our results clearly converge with more recent studies with a similarly large sample 10 and also with those reported earlier using smaller samples. 16 Conversely, they are not congruent with results from a Chinese study. 17 Marneros et al. 16 included a group of 43 patients with DD and 42 patients with SCZ as a control group. Hui et al., 17 on the other hand, followed a different methodology as they used an age-matched cohort of 71 patients with DD and 71 with SZ. However, introducing first episodes of both diseases has the handicap of a lack of diagnostic stability of some psychotic disorders, especially DD or a psychotic disorder other than SZ. 26 Our sample was composed of patients with a follow-up (9.1 years) that was long enough to avoid the inherent bias of diagnostic instability, and adjusting for age did not alter our results.
Sociodemographic Data
In our sample, there were no sex differences within the DD group, but there was an excess of men (71.4%) among the SZ patients. Although, in general, there seems to be a sex balance in SZ, 27 some systematic reviews pointed out an excess of men, with a median male/female rate ratio of around 1.40, 28,29 whereas other population studies reported no differences in sex. 30 A higher proportion of women in DD had been described in some studies, 12 –14,31,32 whereas others found a balanced sex distribution 33 ; finally, both Peralta and Cuesta 10 and Marneros et al. 16 claimed that sex difference is not clear. As expected, in comparing mean age between DD and SZ groups, we found that it was significantly higher among the DD group. This can be indicative of the known older age of onset reported for DD patients. Indeed, most studies have reported DD as a middle- to late-life psychotic disorder, 9,10,12,13,16,33,34 which is congruent with our findings. Finally, we did not find significant differences in educational level between both disorders, in line with other studies 16,17 and contrary to Peralta and Cuesta’s study finding that DD patients showed on average lower mean education years. 10
Psychopathology
The DD group showed less severity on PANSS scores than the SCZ group, including both global and subscale scores (i.e., positive symptoms, negative symptoms, and general psychopathology). Moreover, the DD and SCZ groups were clearly different on hallucination scores in that such scores were lower among the DD group. Indeed, hallucinations in DD were nearly nonexistent, in agreement with what was expected given the diagnostic criteria for both psychotic disorders and replicating previous studies 4 –6 as the dimensional profiling of DD by Serretti et al. 35 It is clear that, using current categorical diagnostic criteria, DD has sufficient entity to be regarded as a distinct psychotic disorder at least on hallucination intensity. We have posed earlier, however, that the use of common ‘pan-psychotic’ dimensions could be an alternative approach to profiling psychotic disorders with different categories varying in intensity across an array of common psychotic dimensions. 18 As for delusions scores, both disorders did not show major differences as they appeared to be similarly present. In contrast, Peralta and Cuesta’s study 10 found fewer, but more intense, delusions among the DD group. Furthermore, they postulate that predominance of jealousy and somatic delusions is specific of DD compared to subjects with SZ, who do not present these kinds of delusions in a predominant way. We infer that the occurrence of delusions, and not that of hallucinations, is one of the most important common features, hence justifying their common inclusion within the psychotic spectrum. Nevertheless, all these findings suggest the need for the study of psychotic disorders using a noncategorical, dimensional manner as reported earlier. 18 Although the DD group showed less negative symptoms than the SZ group, and clearly such difference is another distinction between the 2 categories, 5,6 the mere presence of these symptoms among DD patients goes against classical predetermined definitions of DD that exclude negative symptoms of its psychopathological constellation. Such a finding is also important as psychopathology, 36 particularly negative symptoms, can also be independent predictors of global functioning. 16,34,36,37 Hence, we report a less severe psychopathology among DD patients that would predict a better global functioning compared to SCZ patients. This notion is in line with previous findings of a milder psychopathological profile among DD patients, 16 even though no previous studies had reported the influence of such milder psychopathology in a better functional outcome.
Despite being a less severe disorder than SZ, both psychopathologically and functionally, DD is still severe enough as demonstrated by its very high psychiatric comorbity. 10,11 The frequent occurrence of depressive and affective symptoms in DD has been posed to indicate not mere comorbidity but, rather, a core symptomatic dimension of the disorder itself. 11,35,38 Another important finding is that of a higher lack of insight in patients with DD compared to patients with SZ, which could imply poorer adherence to treatment among the former, as also suggested previously by Peralta and Cuesta. 10 Indeed, this is supported by our recent finding that antidepressants might have a role in the treatment of DD. 39 It must be acknowledged, though, that the only study comparing first-episode DD and SZ patients 17 did not report psychopathology differences among them. However, as commented before, this report was heavily criticised on the grounds that its conclusions might emerge due to differential diagnostic stability when both disorders are looked at longitudinally. 40 Indeed, according to Heslin et al., 26 only 19% of patients with a DD diagnosis at baseline retained that diagnosis 10 years later, and 57% changed to SZ at follow-up. Given the importance of age when comparing disorders with a different onset of age and the fact that age is an important prognostic factor in SZ, 41,42 we reanalysed the above comparisons adjusted by age to detract the potential influence of such a potential confounding factor. In the event, we must say that adjusting for age rendered unaltered results.
Social, Premorbid IQ Estimate, and Global Functioning Outcomes
Patients with DD were more frequently married, were more frequently able to work, and tended to be older than those with SCZ. This is in complete agreement with earlier reports. 10,12,14,17 It is possible that since DD occurs at an older age and is a less severe disorder, patients with DD are more adaptive in establishing enduring relationships than patients with SZ. Data about premorbid IQ are lacking in all previous studies, to our knowledge. IQ is a predictor of cognitive performance. Our finding of a higher IQ among the DD group supports the hypothesis of a better premorbid performance in patients with DD. 10 This is also in line with other studies showing that patients with DD do have some cognitive deficits compared to healthy controls. 43 These deficits are similar to those found in SZ, 8 but our IQ finding is the first direct comparison reporting that cognitive capacity in DD is higher than in SZ, even though we merely estimated IQ using an indirect socio-demographic estimator. Finally, we replicate previous findings of a better global functioning among DD patients compared to SZ patients. 9,10 Such a result was to be expected, provided our above findings of better IQ, milder psychopathology, and better social and interpersonal adjustment among the DD group, all of which are elements contributing to better global functioning. 36
Limitations
A potential limitation of our study is that the sample, being relatively large, is composed of a group of patients researched across different studies by our group. Having said that, this is mitigated by the fact that all such studies used a similar methodology and diagnostic criteria, researchers were trained and directed by the same author, and proxy interrater reliabilities were tested and fairly high for all PANSS measures. Given that the sample comes from a clinical population rather than a community-based one, we must acknowledge the possibility of a degree of selection bias. In addition, we did not have precise data about medication, comorbidity, or family history of medical or mental illness. Although all patients were on an antipsychotic, we lack data on type and doses of medications across groups.
Clinical Implications
Despite these caveats, we trust that we provide substantial and key clinical information to further characterise DD using a relatively large cohort of DD patients. Our results suggest that keeping DD as a distinct disorder is herewith replicated; even when psychopathological differences between DD and SCZ come from predefinitions provided by nosological systems, we demonstrate that both disorders also differ on the grounds of myriad social, cognitive, and global functioning measures. Some of the most important studies, such as those by Marneros et al. 16 and Peralta and Cuesta, 10 used patients with paranoid SZ to be compared with DD patients, but the latter found that different SZ subtypes are more similar between them compared to DD, suggesting that future comparisons should use SZ as a whole rather than paranoid SZ. In addition, another work evaluating the clinical validity of DD and SZ found only a few clinical differences between paranoid SZ and undifferentiated SZ. 9 Moreover, our study contributes to complete contributions from genetics that suggest different genetic profiles between DD and SCZ, 44 even though Cardno and McGuffin 45 concluded that there is not a clear contribution of genetics to DD. Psychopathologically, though, the mere existence of negative and cognitive symptoms and correlates among DD patients also contributes to discounting the classical belief that such patients do not have such defectual symptomatology. It also suggests the potential for clinical use of common psychotic dimensions 18 rather than the current delusion-content classification when profiling DD subtypes. This can have implications for both accuracy of diagnosis and treatment specificity. The latter question is controversial because Peralta and Cuesta 10 found a worse response to treatment in DD patients compared to SZ patients. However, a comparison study specifically testing that did not find significant differences in antipsychotic response between both disorders. 46 Furthermore, a recent systematic review on DD treatment concluded that antipsychotics, particularly first-generation antipsychotics, were an effective treatment for DD, which also suggests a potential role for antidepressants in DD treatment. 39 Definitely a more profound comprehension, characterisation, and profiling of DD can contribute to finding adequate treatments as well as better management and clinical care of these patients.
Footnotes
Acknowledgements
We acknowledge and thank all the patients and their families who have participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.