
Abstract
Objective:
Homelessness has been identified as an important risk factor for suicide death, but there is limited research characterising homeless people who die by suicide. The goal of this study is to identify personal, clinical, and suicide method-related factors that distinguish homeless and precariously housed people who die from suicide from those who are not homeless at the time of suicide.
Methods:
Coroner records were reviewed for all suicide deaths in Toronto from 1998 to 2012. Data abstracted included housing status as well as other demographics, clinical variables such as the presence of mental illness, and suicide method.
Results:
Of 3319 suicide deaths, 60 (1.8%) were homeless and 230 (6.9%) were precariously housed. Homeless and precariously housed people were each younger than nonhomeless people (P < 0.0001). Compared with nonhomeless, homeless people were more likely to be male and less likely to be married, to have interpersonal conflict, or to leave a suicide note. Homeless people and precariously housed were more likely to have died by fall/jump than nonhomeless people (62%, 57%, and 29%, respectively).
Conclusions:
Homeless and precariously housed people are overrepresented among suicide deaths in a large urban center and differ demographically, clinically, and in their suicide method from nonhomeless people who die by suicide. Targeted suicide prevention strategies should aim to address factors specific to homeless people.
Homelessness carries a 2- to 6-fold increased risk of suicide compared to the general population. 1 –5 Despite this, research on suicide death in homeless people is limited and has been identified as an area of need. 1 Homeless people are more likely, compared to others who died by suicide, to be younger, unmarried, non-Indigenous, and unemployed; to use alcohol and/or drugs; to have stressful life events; and to be have physical illness and untreated mental illness. 1,6,7 Schizophrenia and mood, personality, and substance use disorders are all strongly associated with suicide in this population. 8 Acknowledging the challenges inherent to studying homeless people, it has nevertheless been argued that we need better, evidence-based estimates of suicide rates in homeless people and, in addition to the research that has characterised those with suicidal ideation and attempts, a clearer picture of those within this population who die by suicide. 4 We are not aware of any studies that have described suicide deaths across the spectrum of housing status in a North American setting. As Canada’s largest city, Toronto is home to a considerable number of homeless people with point-in-time counts suggesting that there are approximately 5000 at a given time, accounting for 0.2% of Toronto’s population. 9 The present analysis will draw from a larger study, using coroner records to examine all suicide deaths in Toronto from 1998 to 2012, to determine the proportion of deaths that occur in homeless and precariously housed people as well as to characterise these groups. A precariously housed group was included in addition to homeless and nonhomeless groups in recognition of the fact that homelessness lies on a continuum 10 and that tenuous housing status may affect suicide risk.
Method
This work is part of the larger Toronto Analysis of Suicide for Knowledge and Prevention (TASK-P) study, and the details and methods of data collection have been published previously. 11 Records from the Office of the Chief Coroner of Ontario (OCC) were reviewed for the 3319 deaths in the city of Toronto ruled as suicides from 1998 to 2012. Demographic, clinical, and suicide-specific data were collected from the coroner’s charts for all suicides by the primary investigator (MS) and 2 research assistants. Each chart contained a coroner’s investigation report, which included a determination of death, a pathology report, and commonly other sources of information such as police reports, letters from/interviews with family members or physicians, and copies of suicide notes. Housing status was defined according to OCC investigations of living circumstances, which are present in all charts: homeless was defined as having no fixed address and no last known residence or staying in emergency housing for the homeless such as a shelter; precariously housed was defined as having no fixed address and staying in a temporary location, including “couch-surfing,” a hotel, hospital, or jail.
Statistical analysis was performed using IBM SPSS Statistics 24 (SPSS, Inc., an IBM Company, Chicago, IL). Chi-square or Monte Carlo Fisher exact test analyses were conducted for bivariate comparisons on categorical variables. A 1-way analysis of variance (ANOVA) was conducted to test for significant differences in continuous variables with t tests for pairwise comparisons between groups. When indicated, the Welch-Satterthwaite method was conducted.
Results
Of 3319 suicide deaths in Toronto, 60 people (1.8%) were homeless, 230 (6.9%) were precariously housed, and 3029 (91.3%) were nonhomeless. Personal and clinical variables, as well as suicide methods for each group, are shown in Table 1. Homeless people were younger and more likely to be male than nonhomeless (38.9 ± 12.7 years vs. 47.7 ± 17.8 years, P < 0.0001; 83.3% vs. 70.0% male, P = 0.031). Homeless people were much less likely to be married or to have interpersonal conflict (both n < 5, exact numbers suppressed). Rates of any mental illness (72.7%), depression (54.8%), and identified comorbid medical conditions (35.2%) were highest in nonhomeless and lowest in homeless people (40.0%, 20.0%, and n < 5, respectively). Homeless people were least likely to leave a suicide note (n < 5). Homeless people were most likely to have been seen by an emergency department or outpatient psychiatrist in the week prior to suicide (15.0% compared with 7.7% of nonhomeless, P = 0.049).
Global and Pairwise Comparisons of Personal and Clinical Factors as Well as Suicide Methods among Homeless, Precariously Housed, and Nonhomeless Persons Who Died by Suicide in Toronto, Canada, 1998-2012.
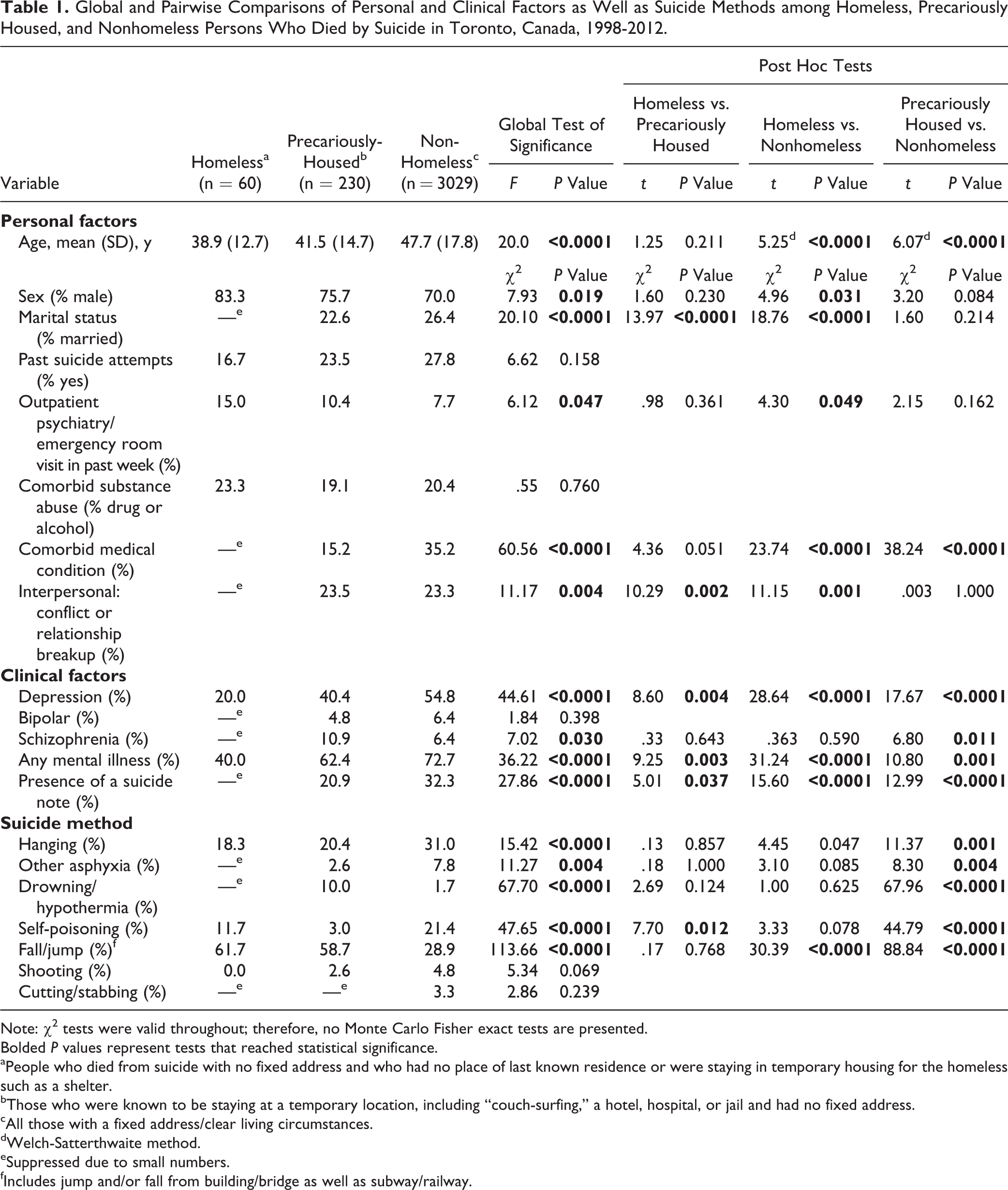
Note: χ2 tests were valid throughout; therefore, no Monte Carlo Fisher exact tests are presented.
Bolded P values represent tests that reached statistical significance.
aPeople who died from suicide with no fixed address and who had no place of last known residence or were staying in temporary housing for the homeless such as a shelter.
bThose who were known to be staying at a temporary location, including “couch-surfing,” a hotel, hospital, or jail and had no fixed address.
cAll those with a fixed address/clear living circumstances.
dWelch-Satterthwaite method.
eSuppressed due to small numbers.
fIncludes jump and/or fall from building/bridge as well as subway/railway.
Precariously housed people were younger than nonhomeless (41.5 ± 14.7 years vs 47.7 ± 17.8 years, P < .0001) and were most likely to have interpersonal conflict (23.5%). Schizophrenia was more prevalent in precariously housed (10.9%) compared to nonhomeless people (10.9% vs 6.4%, P = 0.01).
Homeless and precariously housed people were approximately twice as likely to have died by fall/jump than nonhomeless people (both P < 0.0001).
Discussion
The present study highlights the important contribution of homelessness to suicide deaths in North America’s fourth largest city by population. Homeless and precariously housed individuals accounted for 9% of all suicide deaths in Toronto over a 15-year period. They are therefore overrepresented in suicide death counts 10-fold, which is consistent with previous studies in other locations. 1 –3
We found that 83% of homeless people who died by suicide in Toronto were male, which is consistent with data from other countries. 1,7 Rates of being married and of interpersonal conflict and/or relationship breakups, which were low in homeless people, were notably similar between precariously housed and nonhomeless people. Relationship problems have been cited by recently homeless adults as a main pathway into homelessness; we speculate that this may be true for the precariously housed individuals who died by suicide in our sample, for whom relationship conflict may have contributed to their housing difficulties and to their suicides. 12 Both social connectivity and access to support services for the homeless have been shown to independently predict well-being. 13 Furthermore, a study that examined suicidal ideation longitudinally among homeless people with mental illness randomised to a housing and psychosocial intervention or treatment as usual found that suicidal ideation diminished over time in both groups. 14 In addition to regression to the mean, the authors also attributed these results to increased social connectivity mediated by interaction with the researchers, providing further suggestion that addressing social marginalisation and isolation has the potential to decrease suicide death in homeless people. We speculate that the finding that very few homeless people in the current study left suicide notes may at least partially reflect low social connectivity in this group. That is, many may have felt there was no one to leave a message for.
Differences in suicide methods likely relate to availability, with jumping in front of subways and from high places such as bridges accounting for the majority of deaths in homeless and precariously housed people. This highlights the need for restriction strategies, for example, barriers on subways and bridges, which have been shown to reduce suicide deaths 15 and may preferentially affect these groups. The fact that homeless people had a higher rate of physician contact in the week prior to suicide presents another potential opportunity for intervention in which providers could make greater efforts to improve social isolation and to connect homeless people to support services.
This study has important limitations. First, it relies on the coroner’s data, which are sometimes limited in clinical detail. Investigations of death in homeless people may be particularly vulnerable to missing data because they may be less likely to have next of kin to provide information or to have a regular physician to detect physical or mental disorders. 16 The lower rates of both mental and physical illness in homeless people, for example, should be interpreted with caution given that previous studies have reported the opposite relationship 1 and given that the overall rate of mental illness is approximately 20% lower than what has been observed in other large population studies 5 ; it should be assumed that the presence of mental disorders was underdetected in homeless people and reflects a need for improved surveillance of mental disorders in this population rather than the relative absence of them. While the coroner systematically collects data on last place of residence, in some cases, this information may fail to accurately capture a person’s living situation and may have led to the assignment of some deaths into the wrong group. Variable selection was also constrained by the data reported in the coroner’s records, and other salient factors could not be examined because they were not systematically available. These include previous/ongoing mental health care prior to the past week or a person’s social milieu beyond marital status. This study is also limited by the lack of a living control group. Therefore, while we present observational data to characterise homeless people who died from suicide, future studies should aim to identify which homeless people are at greatest risk. While it is not possible to determine whether results in Toronto may be generalizable to other cities and countries, as a large multicultural city that includes ethnic groups from around the world, we speculate that the findings here are likely to be applicable elsewhere.
This study examined a large number of suicide deaths in homeless and precariously housed people in a major urban center. The findings suggest that homeless and precariously housed people who die from suicide are distinct from one another and from nonhomeless people who die from suicide. In contrast to the general population, for whom older age is an established risk factor for suicide, our findings agree with previous literature that homeless people who die from suicide tend to be younger. 1,3,5 Precariously housed people also have some similarities to nonhomeless people in terms of marital status and interpersonal conflict as a proximate factor in suicide death, suggesting that attention should be paid to relationship difficulties in those who are precariously housed.
This study identifies a need for interventions in homeless and precariously housed populations for suicide prevention. Given that suicide deaths are overrepresented among homeless and precariously housed people, greater efforts at engagement and targeted prevention in these groups, including access to mental health services and programs focused on social connectedness, physician suicide risk assessment and suicide prevention barriers on bridges and subways are warranted.
Footnotes
Acknowledgements
We thank Dr. James Edwards (regional supervising coroner for Toronto East) and the entire staff at the Office of the Chief Coroner of Ontario, including Andrew Stephen, for making this research possible. We also thank Mr. Yasunori Nishikawa for his assistance with statistical analyses.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.S. reports that he has received grant support from the American Foundation for Suicide Prevention, the Physicians' Services Incorporated Foundation, the Dr. Brenda Smith Bipolar Fund, the University of Toronto Department of Psychiatry Excellence Fund, and the Innovation Fund of the Alternative Funding Plan from the Academic Health Sciences Centres of Ontario. N.K. reports that she has received funding from a Canadian Institutes of Health Research (CIHR) Fellowship and a NARSAD Young Investigator Award from the Brain & Behavior Research Foundation. C.R. has no conflicts to report. A.S. reports that he has received funding from the Ontario Mental Health Foundation, the American Foundation for Suicide Prevention, the Physicians' Services Incorporated Foundation, the Dr. Brenda Smith Bipolar Fund, the Ontario Ministry of Health and Long-Term Care, Sunovion, Otsuka, and Lundbeck.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Sunnybrook Health Sciences Centre research ethics board (ID 021-2011).