
Abstract
Objectives:
Schizophrenia and associated illnesses account for a large proportion of mental illness burden and health care expenditures, with the majority of expense involving inpatient care. To date, the literature exploring factors associated with length of stay (LOS) and functional improvement during inpatient care is underdeveloped. In response, this study examined the association between patient characteristics, LOS, and functional improvement using Ontario Mental Health Reporting System (OMHRS) data from 2005 to 2015.
Methods:
The associations of patient characteristics (including key demographics, psychosocial variables, reasons for admission, and service use history) and 2 outcome measures (LOS and Global Assessment of Functioning [GAF]) were analysed with generalised linear mixed modelling (GLMM). From 2005 to 2015, a total of 48,498 episodes for distinct patients from 18 psychiatric hospitals and 57 general hospitals in Ontario were included.
Results:
For psychiatric and general hospitals, mean LOS was 96.6 and 20.5 days, and mean GAF improvement was 14.8 and 16.1, respectively. The majority of associations probed demonstrated a high degree of significance with similar patterns across general and tertiary facility contexts. Older age and more recent readmission following a psychiatric discharge were associated with longer LOS and less GAF improvement. Recent experience of adverse life events and substance misuse were associated with shorter LOS.
Conclusions:
While the findings of this exploratory cross-sectional analysis will require further inquiry with respect to validity and reliability, they suggest that a different service pathway is likely required for individuals with greater psychosocial challenge and extensive service use histories.
The challenges that have attended the development of effective treatment and service approaches for schizophrenia are well documented, as are the extensive system costs attributed to the illness. 1 Of these costs, inpatient care is the largest contributor in most jurisdictions, 2 –4 with schizophrenia accounting for the longest lengths of stay (LOS). 5 Correlates of LOS in this population have included, along with illness severity, a range of demographic, social, and economic factors. 6,7 However, these findings have been inconsistent. For example, male gender has variably been unassociated 8 with LOS and associated with longer 4,9 and shorter LOS. 10 Such inconsistencies may partly be due to the methodological limitations. Many studies have used small samples, not controlled for the effects of repeated admissions, 8 and have not considered hospital effects. 4 This represents a problem at system and policy development levels as care models for schizophrenia are increasingly under scrutiny due to budgetary constraints and an emphasis upon community-based care. 11 Such planning needs to be informed by service utilisation data that are representative of Canadian contexts and populations. Systematic data collection through the Ontario Mental Health Reporting System (OMHRS) is the most comprehensive source of such information at a provincial level. Using data from OMHRS, this article aims to examine the association between patient characteristics and inpatient LOS and functional improvement of schizophrenia and other major psychotic illnesses. Attending to service utilisation and outcome trends as a function of these variables could allow for more informed mental health system and service planning. This study is among the most comprehensive to date internationally and the first such study undertaken with Canadian data.
Methods
Data Source
Data for this study were obtained from the OMHRS. Implemented in October 2005, OMHRS contains information on all hospital admissions for adults admitted to the approximately 5000 mental health beds in Ontario. OMHRS data are derived from the Resident Assessment Instrument–Mental Health (RAI-MH), which is a comprehensive, mandatory, and standardised assessment tool for inpatient psychiatry and includes information on patient demographics, socioeconomic status, diagnosis, substance use, psychiatric symptoms, cognition, and functioning. 12,13 The reliability and validity of the RAI-MH have been established in a number of previous studies. Specific domains include acceptable to high average interrater reliability based on kappa coefficients and percentage agreement between raters. 13
OMHRS records, purchased from the Canadian Institute for Health Information (CIHI), were obtained for all people admitted and discharged between October 1, 2005, and June 30, 2015, from a psychiatric bed in Ontario based on the OMHRS code for a primary diagnosis of schizophrenia and/or other psychoses (based on DSM-IV diagnostic category, including schizophrenia, schizoaffective disorder, schizophreniform disorder, delusional disorder, brief psychotic disorder, shared psychotic disorder, psychotic disorder due to medical conditions, substance-induced psychotic disorder, and psychotic disorder not otherwise specified). There is no specific category for ‘schizophrenia’ in isolation in this database. Patients without completed RAI-MH data, having a forensic status, or having an ‘unplanned discharge’ were excluded as confounds within the scope of this analysis. This study received approval from the Research Ethics Board of the Centre for Addiction and Mental Health (REB reference 093/2015).
Outcome Measures
Two outcome measures were included in this study: LOS (in days) and the functional improvement for each patient, measured as the difference of Global Assessment of Functioning (GAF) scores between discharge and admission. LOS is an important performance indicator for costing and hospital management and a key measure of efficiency of a health care system. 14 The LOS per episode was adjusted by excluding alternate level of care (ALC) days, which reflect systems considerations outside of the control of hospitals (e.g., housing, adequate case management). 15 GAF provides a global rating of severity across psychiatric diagnoses. It is used widely and captures psychiatric symptom severity and social and occupational functioning. 16 Scores range from 1 to 100, with 100 representing an absence of symptoms and superior functioning. While GAF has been found to be a reliable and valid measure for examining patient outcome and program performance, a shortcoming in this database is the possibility of different intake-discharge raters 17 and other concerns that might account for its removal from the DSM-5. 18
Patient Characteristic Variables
We extracted the following patient-level variables from the OMHRS data set: sex, age, language spoken, marital status, education level, employment, residential stability, number of previous psychiatric admissions, time since last psychiatric discharge, admission reasons, history of medication refusal, adverse life event experience, substance use, alcohol, and smoking.
For adverse life events, OMHRS has a variable for each of the following 8 major adverse life events categorised by recency: serious accident or physical impairment; death of a close family member or friend; major loss of income or serious economic hardship due to poverty; immigration, including refugee status; witness to severe accident, disaster, or act of terrorism; violence or abuse; victim of crime; sexual assault/abuse; and physical assault/abuse. In this study, we pooled major adverse life events into a single variable, adverse life events, and considered as a binary occurrence.
The data set has a variable for the following 6 substances: inhalants, hallucinogens, cocaine and crack, stimulants, opiates, and cannabis. We pooled the above substance use items into a single variable, substance use, with coding rules the same as coding adverse life events.
Data were also available on reasons for admissions. We focused on 2 variables—specifically, threat/danger to harm self or others and inability to care for self—which were binary coded.
Analysis
Data were analysed with SPSS (version 21; SPSS, Inc., an IBM Company, Chicago, IL). Descriptive analyses were conducted for all variables. To address the question of which patient variables are associated with LOS and GAF change, we employed generalised linear mixed models (GLMMs) to estimate the association between patient characteristics and LOS and GAF improvement. GLMM is a flexible statistical approach for analysing nonnormal data when random effects are present. 19 In this study, patient characteristics were set as independent variables, and possible hospital ‘block’ effects (e.g., policies, care culture) were set as random effects and controlled by the GLMM as hospital characteristics can influence patient LOS and outcome. 20 Estimated effects were reported as estimated marginal means (EMMs) and contrast estimates. The contrast estimate is the difference of EMM to the reference level of the variables. 21,22
Results
Descriptive Analysis
A total of 114,812 episodes were extracted from the data provided by CIHI. In total, 24,657 episodes were excluded from the study cohort due to forensic status or unplanned discharges. Another 1862 episodes, which were excluded due to missing GAF data either at admission or discharge, resulted in a total of 88,239 episodes included in this study. In total, 39,741 (45.0%) of 88,239 episodes were repeated admissions. The mean number of admissions per patient was 2.04 (SD = 1.99; median = 1; range, 1 to 43). To eliminate the weighted effects of patient characteristics from readmitted patients on outcome measures, 1 episode was randomly selected for each multiple-admission patient, leaving 48,498 episodes for distinct patients from 18 psychiatric hospitals (12,343) and 57 general hospitals (36,155).
For the psychiatric hospital subset, the average LOS was 96.6 days (SD = 205.1; median = 42.0; range, 1 to 3234) (Table 1), and the average GAF improvement at discharge relative to admission was 14.8 (SD = 16.1; median = 15.0; range, –90 to 85; note that negative values reflect a decline in admission to discharge change in scores) (Table 2). For the general hospital subset, the average LOS was 20.5 (SD = 25.4; median = 15.0; range, 1 to 1632), and the average GAF improvement was 16.1 (SD = 19.1; median = 19.0; range, –81 to 90).
Factors Associated with LOS in Patients with Schizophrenia in Ontario Psychiatric Hospitals: Descriptive Statistics and GLMM Analysis.
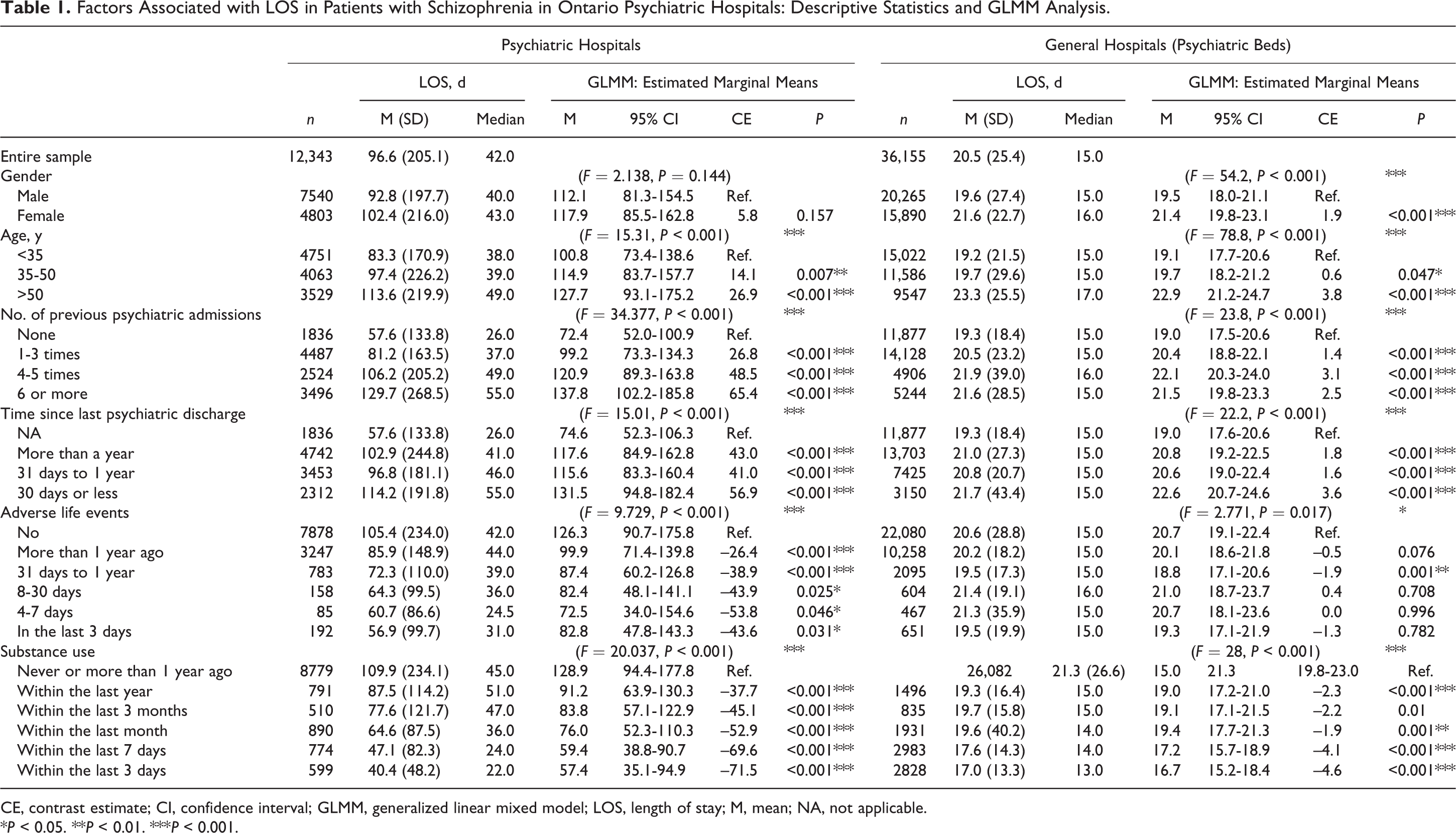
CE, contrast estimate; CI, confidence interval; GLMM, generalized linear mixed model; LOS, length of stay; M, mean; NA, not applicable.
*P < 0.05. **P < 0.01. ***P < 0.001.
Factors Associated with GAF Improvement for Schizophrenia Inpatient Stay in Ontario Psychiatric Hospitals: Descriptive Statistics and GLMM Analysis.
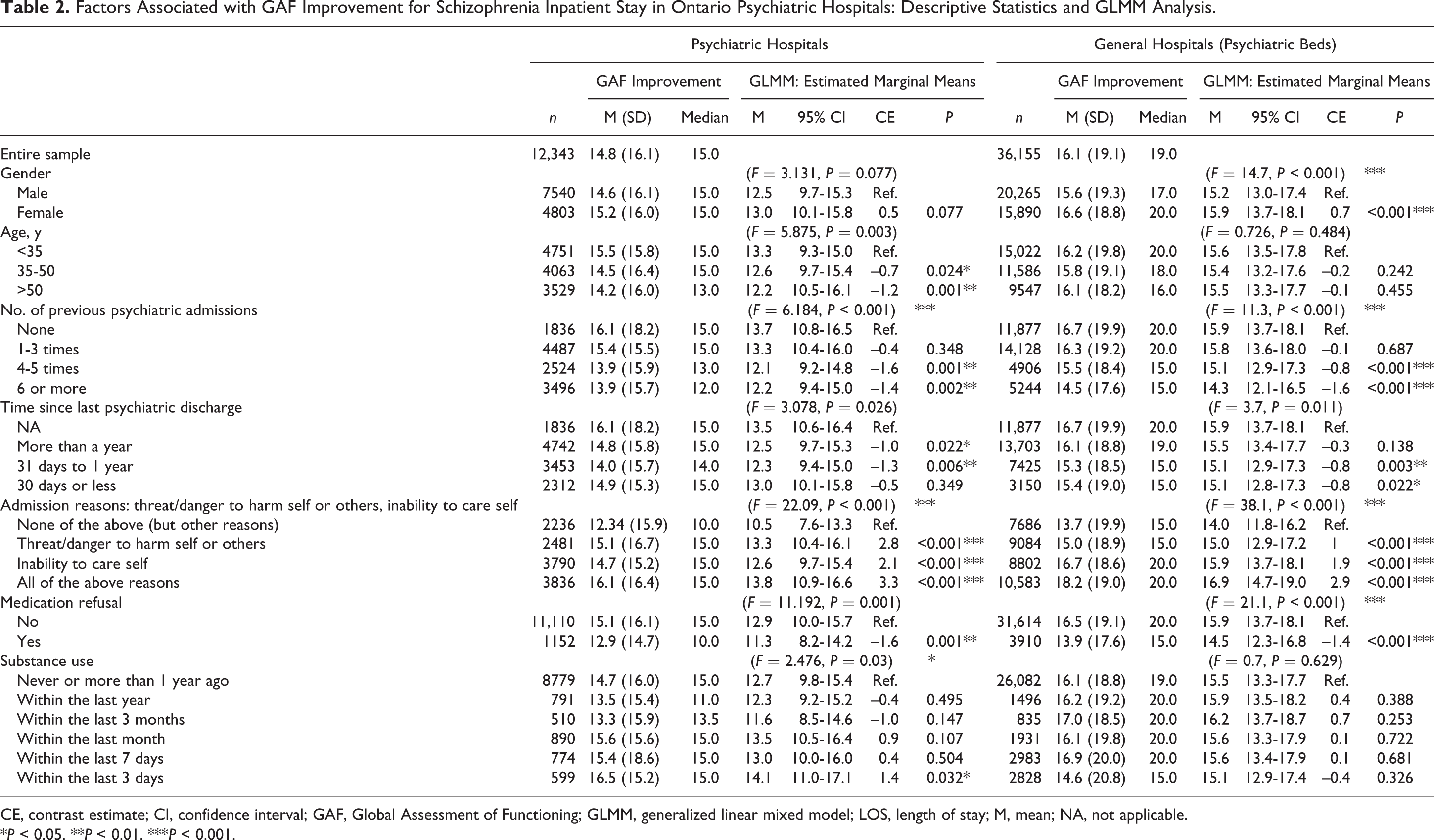
CE, contrast estimate; CI, confidence interval; GAF, Global Assessment of Functioning; GLMM, generalized linear mixed model; LOS, length of stay; M, mean; NA, not applicable.
*P < 0.05. **P < 0.01. ***P < 0.001.
GLMM Analysis and Estimation Results
The distributions of LOS for both the psychiatric hospital and the general hospital subsets were positively skewed (skew = 7.144 and 27.158 for psychiatric and general hospitals, respectively). With logarithmic transformation, the skew for the transformed LOS was 0.395 for the psychiatric subset and 0.438 for the general hospital subset. No significant skew was observed for GAF.
Patient characteristic variables were clustered into 4 groups: demographic factors, psychosocial factors, service factors, and challenges. Table 3 summarises the major findings of the study.
Summary of the Association between Patient Characteristic Factors and LOS and GAF Improvement.
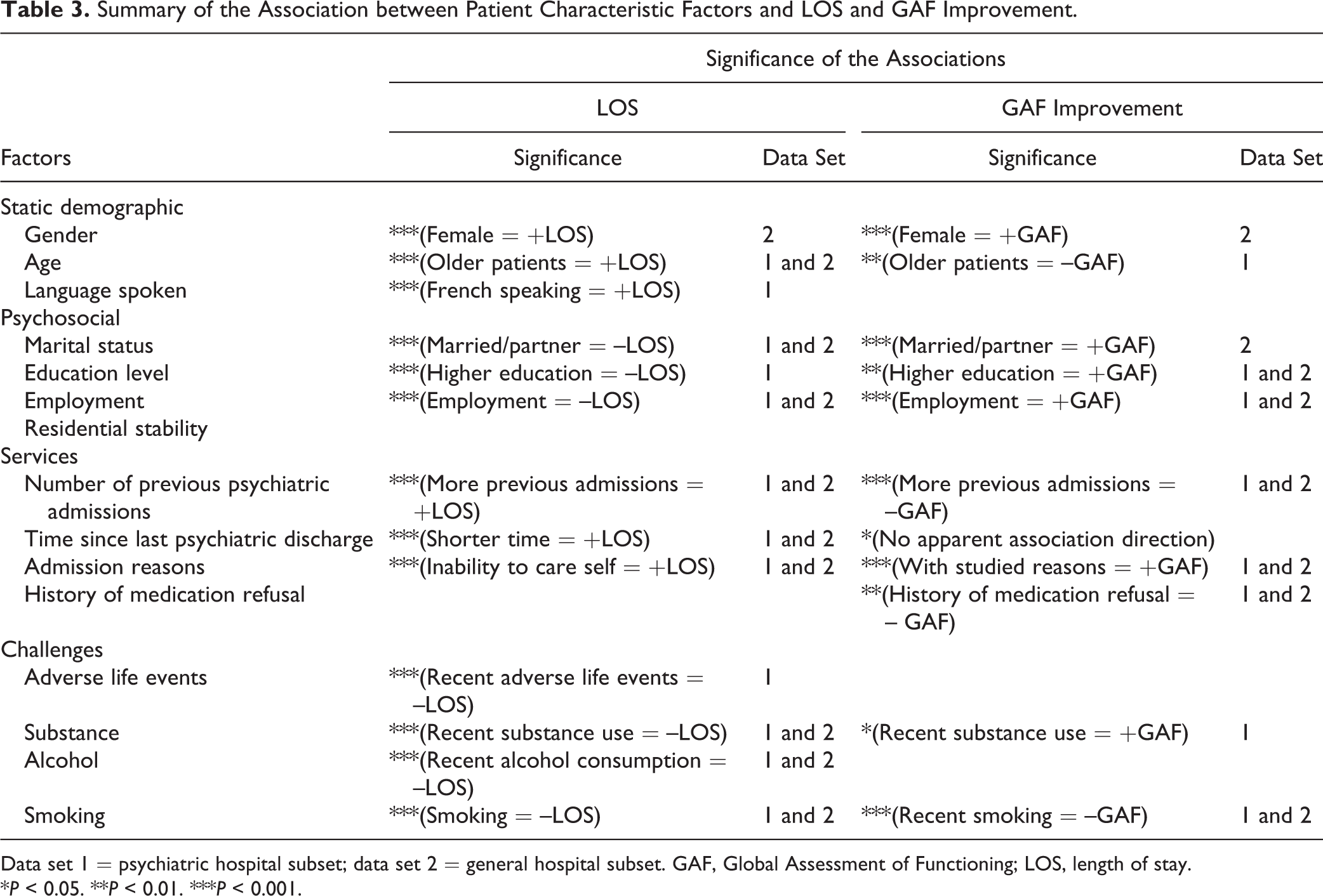
Data set 1 = psychiatric hospital subset; data set 2 = general hospital subset. GAF, Global Assessment of Functioning; LOS, length of stay.
*P < 0.05. **P < 0.01. ***P < 0.001.
Static Demographic Factors
We did not observe a significant association between patient sex and either LOS or GAF improvement for episodes in psychiatric hospitals (Tables 1 and 2). For general hospital episodes, there was a significant association for sex on both LOS and GAF improvement, with female patients being estimated (contrast estimate or CE) to stay 1.9 days longer and gain 0.7 more GAF points.
Age was significantly associated with LOS for episodes from both the psychiatric hospitals and general hospitals, with patients older than 50 years staying an average of 26.9 days longer in psychiatric hospitals and 3.8 days longer in general hospitals (Table 1). While not significant for general hospitals, in psychiatric hospitals, patients older than 50 years had 1.2 points less gain on the GAF (Table 2).
Language spoken was a significant contributor to LOS for psychiatric hospital episodes, with French-speaking patients estimated to have an LOS 65.9 days longer than English-speaking patients, although sample size was an issue in this analysis (Suppl. Table S1).
Psychosocial Factors
Patients who were married or had a partner were estimated to have a shorter LOS by 27.6 days (psychiatric) and 1.6 days (general) (Supplemental Table S1) and, in general hospitals, gain 1.1 points more on the GAF (Supplemental Table S2).
Patients with an education level of high school or above were estimated to have a shorter LOS by 29.2 days (psychiatric) and 0.6 days (general) (Suppl. Table S1) and gained 0.9 more points on the GAF in both psychiatric and general hospitals (Suppl. Table S2). Patients who were employed were estimated to stay 58.1 days (psychiatric) or 4.6 days (general) less (Suppl. Table S1) and gain 2.1 points (psychiatric) and 1.2 points (general) more on the GAF (Suppl. Table S2).
Service Use
Greater numbers of previous psychiatric admissions were associated with longer LOS (Table 1, Figure 1) and fewer gains on GAF in both hospital types (Table 2). Recency of readmission following a psychiatric discharge was associated with longer LOS (Table 1 and Figure 1) and less GAF improvement (Table 2). Patients who had a psychiatric discharge within 30 days were estimated to stay 56.9 days (psychiatric) or 3.6 days (general) longer (Table 1 and Figure 1).
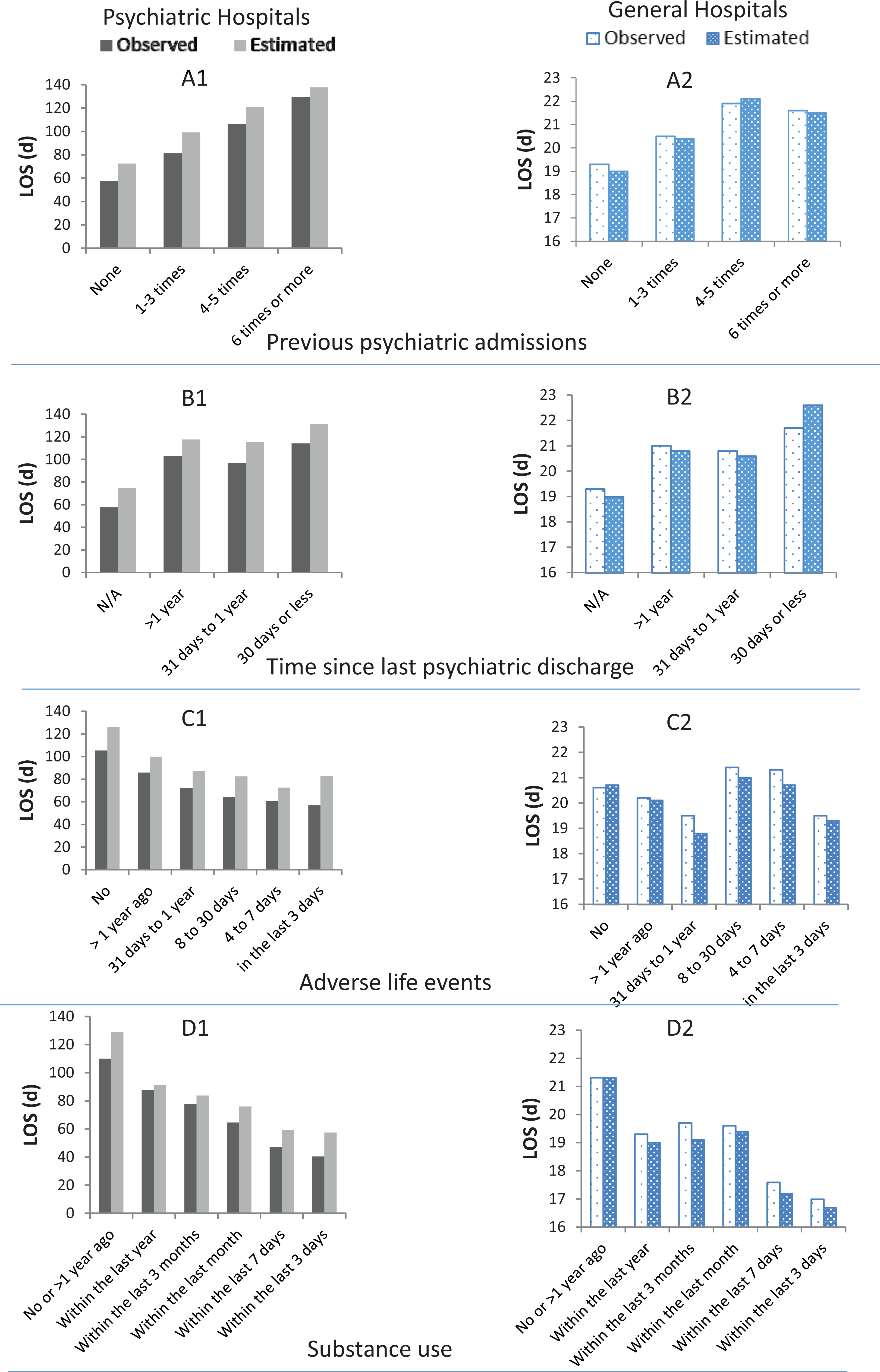
The impact of selected factors on observed and Global Assessment of Functioning (GLMM) estimated marginal mean length of stay (LOS).
Patients who were admitted because they demonstrated a threat/danger to harm self/others and inability to care for self were estimated to stay 43.7 days (psychiatric) or 3.4 days (general) longer (Suppl. Table S1) and gain 3.3 points (psychiatric) or 2.9 points (general) more in GAF scores (Table 2). Medication refusal while in hospital did not have a significant impact on LOS (Suppl. Table S1) but was associated with less changes in GAF in both psychiatric hospitals (1.6 points) and general hospitals (1.4 points) (Table 2).
Challenges
The more recently that patients experienced adverse life events, the shorter the LOS (Table 1 and Figure 1). Adverse life events were not associated with GAF change. With respect to substance use, the more recent the reported use, the shorter the LOS for both hospital types (Table 1 and Figure 1), and for psychiatric hospitals, those who used substances ‘within the last 3 days’ were estimated to gain 1.4 more GAF points than those who denied use in the past year (Table 2).
Alcohol consumption at any time in the 14 days prior to current admission was significantly associated with shorter LOS in both hospital types, with those reporting 5 or more drinks per sitting estimated to stay 49.5 days (psychiatric) or 4.0 days (general) less (Suppl. Table S1). No association with GAF was noted (Suppl. Table S2). Smoking was significantly associated with both LOS and GAF measures. Patients who smoked in the last 3 days prior to admission had lower LOS by 19.0 days (psychiatric) and 3.7 days (general) (Suppl. Table S1). Associations with GAF scores were less consistent (Suppl. Table S2).
Discussion
This article was intended to provide a descriptive profile of hospitalisation of individuals with schizophrenia and other psychotic disorders using a large provincial database. These findings indicated a median LOS that is longer (42 days for psychiatric hospitals and 15 for general hospitals) than previously reported national CIHI data from 2009 to 2010 (35 days for psychiatric hospitals and 13 days general hospitals), although a lower mean LOS (96.6 vs. 144.6 days for psychiatric hospitals and 20.5 vs. 23.4 days for general hospitals). 5 However, the meaning of these differences is difficult to interpret and, while possibly having implications regarding service utilisation (e.g., fewer very long stay patients hospitalised in Ontario), they could readily be a product of methodology. Key considerations include diagnostic parameters and how forensic patients, multiple admissions, and incomplete data were addressed, which might account for the differences observed. Both current and CIHI national data sets note markedly higher LOS among schizophrenia and psychosis populations compared with mean LOS findings across all mental illness and addictions diagnoses (CIHI mean of 80.5 days psychiatric; 18.3 days general). 5 More broadly, the results of the present study are comparable with findings in the United Kingdom (47.7 days, schizophrenia; 41.1 days, schizoaffective and other psychoses). 8 This observation might be a function of similar health care systems as the observed length of stay in Korea was found to be much longer for schizophrenia (217 days). 4
Comparative data are more difficult to generate regarding GAF improvement (mean of 14.8 points for psychiatric hospitals and 16.1 for general), but such a degree of improvement would seem modest given that crises typically prompt hospitalisation, the intensity of inpatient services, and lengthy LOS. Consistent with Jacobs et al., 8 for psychiatric hospitals, we did not observe a significant difference in LOS as a function of sex or GAF change. While, for psychiatric hospitals, this is suggestive of a lack of systemic difference in care as a function of sex, the longer lengths of stay with greater improvement for females in general hospitals are more difficult to interpret. The association between age, LOS, and GAF change matches what might be expected given the care complexities that attend aging and align with previous work in this area. 23 The finding of markedly longer LOS among French-speaking patients in psychiatric hospitals bears further analysis, although it aligns with previous research, which found that French-speaking patients were about one-third as likely to have daily contact with a psychiatrist in the first 3 days of admission. 24
The associations observed between psychosocial factors, LOS, and GAF improvement are consistent with other research on psychosocial determinants, suggesting better trajectories among individuals with greater social support (e.g., married) and better engagement with education and employment. 25,26
As proxy indicators of acuity, with implications for the adequacy of supports postdischarge, 27 the number of previous hospitalisations and recency of prior discharge suggest a pattern of individuals with more hospitalisations and more difficult community transitions having long LOS and making fewer gains. The finding that threat of harm and inability to care for self were associated with longer LOS would seem intuitive, and greater GAF change for such individuals might have occurred as a function of admission while in acute crisis and the range of potential gain being greater. Lastly, with respect to service-oriented indicators, the observation of medication refusal being associated with less gain could possibly be an indication of a subset of patients who are less engaged in care generally. 28,29
With respect to challenges, a picture emerged of the recency of adverse life events being linked with LOS in a linear fashion—an association that mirrors recent life adversity-psychosis severity findings. 30 This potentially suggests that acuity driven by environmental adversity might more readily be addressed in a shorter period than acuity driven by other factors (e.g., more biologically determined).
Similarly, with adverse life events, and consistent with previous literature, 8,31,32 we found that shorter LOS was associated with substance or alcohol misuse. This finding might suggest that they, as determinants of acuity, are more readily resolved in hospital following inpatient detoxification. Furthermore, such patients may be more likely to leave against medical advice (self-discharge) and are motivated to show improvement so they can leave to regain access to drugs or alcohol. Similarly, the association between smoking and lower LOS might indicate greater motivation to be discharged in contexts where access to tobacco is difficult.
With respect to implications, these findings support the utility of approaches such as assertive community treatment and intensive case management that focus on those demonstrating very difficult transitions to community and limited gains in hospital. 33,34 Also supported are implications for greater gains in shorter periods and interventions that might enhance such gains, in scenarios in which acuity is driven to a greater extent by environmental stressors and/or addictions. More broadly, systematic approaches are needed, such as integrated care pathways, 35 as it is clear that there are diverse service utilisation patterns that are predictable and likely require quite different approaches within the same diagnostic category. Initiatives to set standards for inpatient schizophrenia care such as those recently released by Health Quality Ontario are an important step in this direction. 36 Finally, it would be helpful from an equity perspective if race and ethnicity could be integrated into mandatory data collection given that this study indicated systematic differences as a function of language and sex.
Limitations
Limitations include the cross-sectional nature of the analysis, the use of data from a single Canadian province, complexities that attend transfers of patients from general to tertiary facilities, and the challenges that attend some of the metrics employed in clinical practice (e.g., GAF ratings). Additionally, the OMHRS does not have a specific variable for schizophrenia, which introduces variability attending other psychotic illnesses with diverse presentations and care trajectories, and it does not capture all the relevant parameters contributing to LOS, such as community services and social and family supports, which have dramatic impact on LOS. 37,38 Similarly, the OMHRS does not capture emergency room days, which might have resulted in lower LOS findings. Lastly, it would be beneficial if future analyses unpacked the possible differential impacts of individual types of adversity that preceded hospitalisation and considerations such as substance use type.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.