
Abstract
Background:
The Canadian Network for Mood and Anxiety Treatments (CANMAT) has revised its 2009 guidelines for the management of major depressive disorder (MDD) in adults by updating the evidence and recommendations. The target audiences for these 2016 guidelines are psychiatrists and other mental health professionals.
Methods:
Using the question-answer format, we conducted a systematic literature search focusing on systematic reviews and meta-analyses. Evidence was graded using CANMAT-defined criteria for level of evidence. Recommendations for lines of treatment were based on the quality of evidence and clinical expert consensus. “Psychological Treatments” is the second of six sections of the 2016 guidelines.
Results:
Evidence-informed responses were developed for 25 questions under 5 broad categories: 1) patient characteristics relevant to using psychological interventions; 2) therapist and health system characteristics associated with optimizing outcomes; 3) descriptions of major psychotherapies and their efficacy; 4) additional psychological interventions, such as peer interventions and computer- and technology-delivered interventions; and 5) combining and/or sequencing psychological and pharmacological interventions.
Conclusions:
First-line psychological treatment recommendations for acute MDD include cognitive-behavioural therapy (CBT), interpersonal therapy (IPT), and behavioural activation (BA). Second-line recommendations include computer-based and telephone-delivered psychotherapy. Where feasible, combining psychological treatment (CBT or IPT) with antidepressant treatment is recommended because combined treatment is superior to either treatment alone. First-line psychological treatments for maintenance include CBT and mindfulness-based cognitive therapy (MBCT). Patient preference, in combination with evidence-based treatments and clinician/system capacity, will yield the optimal treatment strategies for improving individual outcomes in MDD.
Keywords
In 2009, the Canadian Network for Mood and Anxiety Treatments (CANMAT), a not-for-profit scientific and educational organization, published a revision of evidence-based clinical guidelines for the treatment of depressive disorders. 1 CANMAT has updated these guidelines in 2016 to reflect new evidence in the field.
The scope of these guidelines remains the management of adults with unipolar major depressive disorder (MDD). CANMAT, in collaboration with the International Society for Bipolar Disorders, has published separate guidelines for bipolar disorder. 2 This section on Psychological Treatments is 1 of 6 CANMAT guidelines articles; other sections of the guidelines expand on burden and principles of care, pharmacological treatments, neurostimulation treatments, complementary and alternative medicine treatments, and special populations.
We use the term psychological treatment rather than psychotherapy as a broader term that involves treatment of psychiatric and behavioural disorders through a method of communicating that invokes a psychological model of illness. This method of communication begins with a patient who seeks alleviation of current symptoms or prevention of recurrence of symptoms. With the advent of computer, Internet, self-help, phone, and mobile apps, the relationship is now between the patient and the psychological model, with an implicit link to the “therapist” who designed the therapy. This guideline summarizes depression-specific psychotherapies as well as newer therapies that are promising and seeks to clarify the evidence and usefulness of each major treatment.
Psychological treatments for MDD share many common components: 1) the goal of treatment is alleviation of the core symptoms of depression; 2) there is careful attention to a specific method to deliver the therapy (typically a manual); 3) the psychotherapy focuses on the current problems of the patient; 4) high levels of activity are expected from both the therapist and the patient (who frequently has “homework”); 5) careful symptom monitoring, preferably with rating scales, is expected; 6) psychoeducation about the illness is a frequent component; and 7) the treatment is generally time-limited, often paralleling the time course for pharmacotherapy.
Furthermore, many of these therapies have been modified to be delivered in a group format. While a group approach may allow for integration of new techniques involving peer feedback and may be more cost-effective, the core of the psychotherapy remains unchanged, so group interventions are not evaluated in these guidelines as a separate “group therapy.” Similarly, context-specific therapies (such as marital therapy for MDD coinciding with a severe marital dispute) are not evaluated, since such therapies do not generalize to the average person with depression. Indications for a specific therapy, as well as the choice of either psychological treatment or pharmacotherapy alone or in combination, are reviewed in a number of the following questions, along with discussion of self-help approaches and peer support. The recommendations are presented as guidance for clinicians who should consider them in the context of individual patients and not as standards of care.
Methods
The full methods have been previously described, 3 but in summary, relevant studies in English published from January 1, 2009, to December 31, 2015, were identified using computerized searches of electronic databases (PubMed, PsychInfo, Cochrane Register of Clinical Trials), inspection of bibliographies, and review of other guidelines and major reports. Each recommendation includes the level of evidence for each graded line of treatment, using specified criteria (Table 1). The level of evidence criteria now reflect the primacy of meta-analysis because of its increasing use in the evaluation of evidence.
Criteria for Level of Evidence and Line of Treatment.
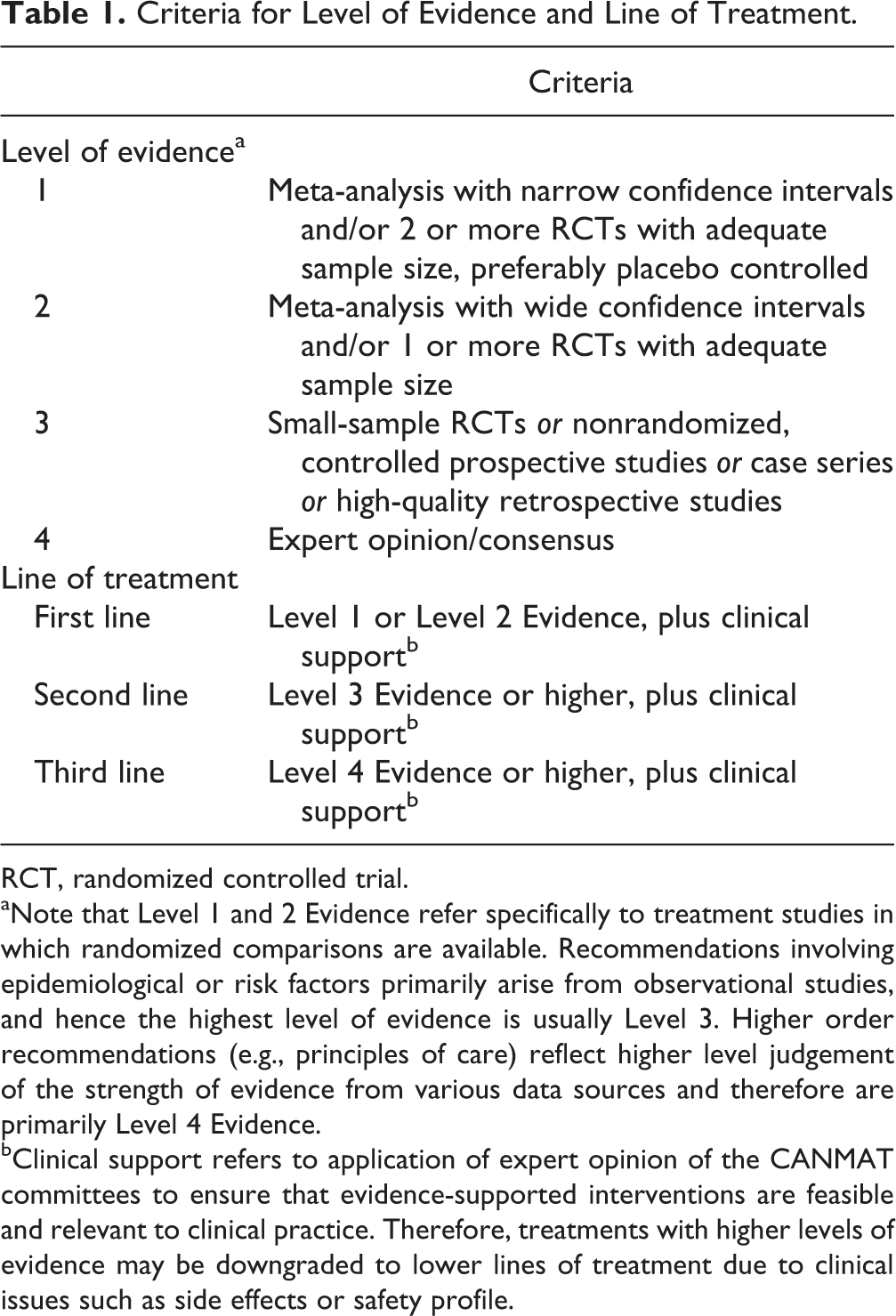
RCT, randomized controlled trial.
aNote that Level 1 and 2 Evidence refer specifically to treatment studies in which randomized comparisons are available. Recommendations involving epidemiological or risk factors primarily arise from observational studies, and hence the highest level of evidence is usually Level 3. Higher order recommendations (e.g., principles of care) reflect higher level judgement of the strength of evidence from various data sources and therefore are primarily Level 4 Evidence.
bClinical support refers to application of expert opinion of the CANMAT committees to ensure that evidence-supported interventions are feasible and relevant to clinical practice. Therefore, treatments with higher levels of evidence may be downgraded to lower lines of treatment due to clinical issues such as side effects or safety profile.
Because of the very large number of randomized-controlled trials (RCTs), this psychological treatments section will primarily focus on systematic reviews and individual and network meta-analyses. Although meta-analyses have advantages in summarizing data, they still have limitations that can lead to erroneous or conflicting results depending on the comprehensiveness of the review, criteria for study selection and quality and generalizability of the included studies, and various types of bias. 4 One additional limitation of both RCTs and subsequent meta-analyses needs to be highlighted: recruitment of individuals in standard MDD RCTs often excludes people with current suicidality, substance use, and other comorbidities. 5 This limits the generalizability of these studies. We have included separate sections on depression with various comorbidities to specifically highlight findings in those clinical conditions.
2.1. When Is Psychological Treatment Indicated?
In addition to patients’ attitudes and preferences, a clinician must consider the availability of high-quality evidence-based psychological treatment and the risk from delay in treatment initiation. In more severe and high-risk cases, it is imperative to start a treatment that is immediately available and to consider all treatment modalities, including neurostimulation. In moderately severe and low-risk cases, the choice of initial treatment between psychological treatment and antidepressants may be determined by the balance of patient preferences and availability of each treatment modality. In addition, special circumstances may need to be taken into account. For example, women who are planning to conceive or are pregnant may be preferentially considered for psychological treatment, because of concerns that use of antidepressants in pregnancy may affect the fetus. 6,7 On the other hand, psychological therapies are not indicated for individuals with psychotic depression, who require pharmacotherapy with antidepressants and antipsychotics 8 or electroconvulsive therapy.
2.2. Which Individuals with Depression Are Most Likely to Benefit from Psychological Treatment?
Demographic factors
Psychological treatments benefit men and women to the same extent; psychological treatments are equally suitable for individuals of all ages, levels of education, and cultural and ethnic backgrounds. 9 Psychological treatments in general and cognitive-behavioural therapy (CBT) in particular appear to be equally effective for different subtypes of depression, including atypical depression, melancholic depression, and anxious depression. 9,10 In addition, a large individual-level meta-analysis confirmed that men and women derive similar benefits from CBT and from antidepressants. 11 In persistent depressive disorder (PDD), medication treatment or combination of medication with psychological treatment provides more benefit than psychological treatment alone. 12,13
Severity
Early findings that CBT as a treatment for severe depression was less effective than medication 14 were followed by evidence of comparable efficacy for CBT and medication. 15 A subsequent meta-analysis confirmed that severity of depression does not differentially predict outcomes of treatment with antidepressants and CBT. 16 As in the case of antidepressant medication, the magnitude of benefit for psychological treatment appears to increase with increasing severity, 17 although there is evidence that psychological treatments are beneficial even for subthreshold depressive symptoms. 18 However, since the time course of improvement is typically faster with pharmacological than psychological treatment, 19 pharmacotherapy may still be preferred as the initial treatment in severe and high-risk cases.
2.3. How Do Co-occurring Psychiatric and Medical Conditions Affect the Efficacy of Psychological Treatments?
Psychiatric comorbidities
This question was addressed by a CANMAT task force in 201220 with individual studies on anxiety disorders, 21 attention-deficit/hyperactivity disorder (ADHD), 22 substance use disorders, 23 and personality disorders. 24 There is insufficient evidence to define formal treatment recommendations, so instead only evidence is summarized.
In summary, Level 2 Evidence supports a negative prognostic impact of comorbid personality disorder on treatment outcomes, including psychological treatments, in depression (Table 2). Insufficient evidence is available to support a positive or negative effect of anxiety symptoms or disorders on depression outcomes, but CBT may be more effective than other treatments. CBT is also effective for depressive symptoms in substance use disorders, and Level 2 Evidence supports integrated psychosocial treatment of alcohol misuse and depression. For ADHD, CBT can improve both depressive and ADHD symptoms.
Impact of Comorbid Psychiatric Disorders on Psychological Treatments in Major Depressive Disorder.
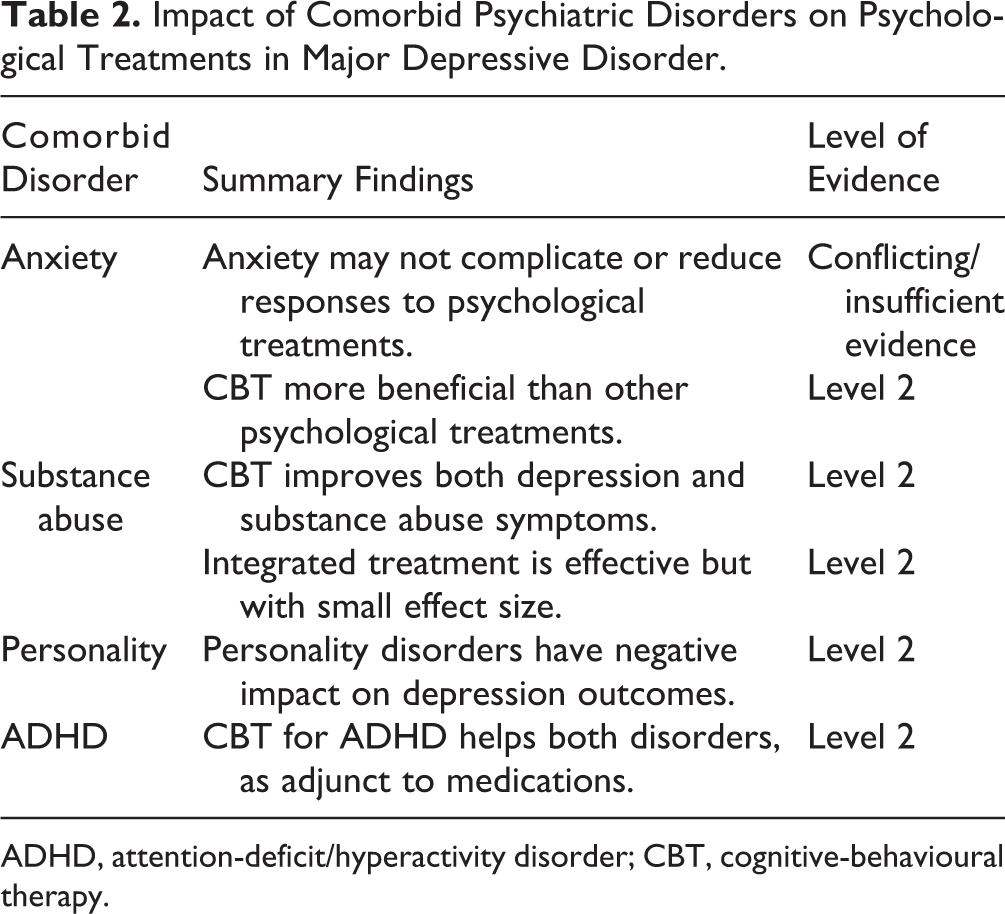
ADHD, attention-deficit/hyperactivity disorder; CBT, cognitive-behavioural therapy.
Medical comorbidities
The CANMAT task force also addressed the management of mood disorders and comorbid medical conditions. 20,25,26 There is insufficient evidence to define formal treatment recommendations, so instead only evidence is summarized.
Several key limitations exist in summarizing this literature: 1) the comorbid medical disorders themselves represent a variety of illnesses grouped according to organ system (e.g., cancer includes a variety of diseases), 2) the medical disorders themselves include patients at varying stages or severity of medical illness, and 3) most studies measure improvement in depressive symptoms as opposed to only improvement of those with a full diagnosis of MDD.
In summary, there is Level 2 Evidence for treatment of depression with co-occurring cardiovascular disease for CBT, interpersonal therapy (IPT), and problem-solving therapy (PST). 25,27 –29 Level 2 Evidence also exists for a variety of psychological treatments in cancer patients, but these are studied by cancer type and stage as noted in Table 3. 25,30 In the presence of human immunodeficiency virus (HIV), Level 1 Evidence supports a variety of psychological treatments, particularly CBT 31 and, importantly, improved adherence to medical interventions as well as improvement in depression. 32 For a variety of neurological disorders, psychological treatments (almost always CBT) have been tested for comorbid depression or depressive symptoms, with Level 2 Evidence of efficacy for multiple sclerosis and Parkinson’s disease, and Level 3 Evidence for epilepsy and migraines. 25,33,34 Finally, for the strikingly high rates of depression accompanying hepatitis C, only Level 3 Evidence exists for psychological treatments, based primarily on expert recommendations with a single trial using both CBT and IPT approaches. 25,35
Impact of Comorbid Medical Disorders on Psychological Treatments in Major Depressive Disorder.
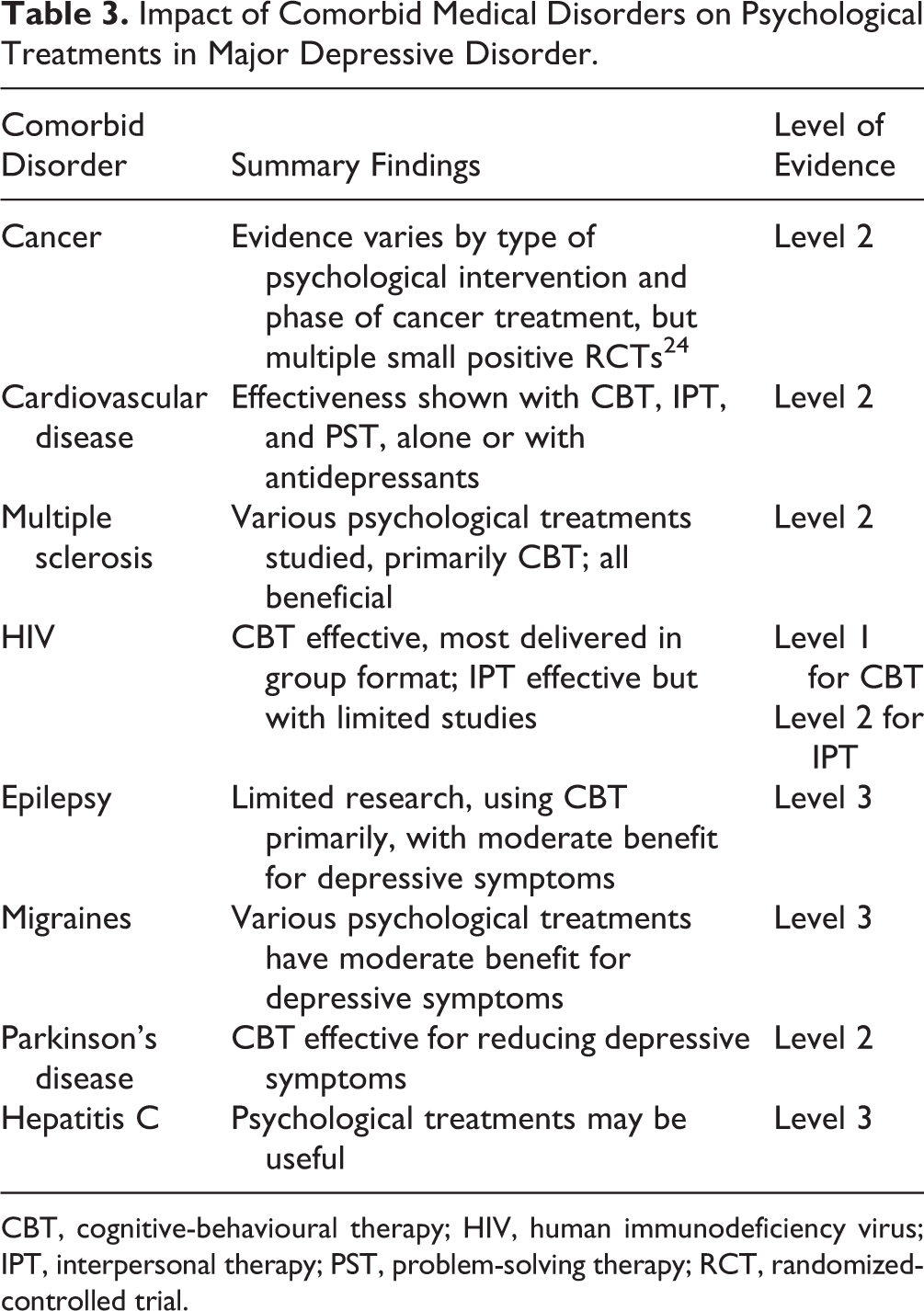
CBT, cognitive-behavioural therapy; HIV, human immunodeficiency virus; IPT, interpersonal therapy; PST, problem-solving therapy; RCT, randomized-controlled trial.
2.4. How Do Gender and Age Influence the Decision to Use Psychological Treatment?
More women than men prefer psychological treatment over medication treatment. 36 Considerations for women during childbearing years include exposure of the fetus during gestation or neonate during lactation. The scope of evidence for psychological treatment is broader for postpartum rather than during pregnancy, with Level 1 Evidence to support psychological treatment as first-line for perinatal women with mild to moderate depressive illness. 37 –40 Moreover, many pregnant women prefer psychological treatment and report fear of potential adverse effects of antidepressants on the developing fetus or on their newborn via lactation, general worries about a negative outcome, and fears of dependency as well as balancing concerns about their own health or the fetus. 41,42 Treatment for adolescents is addressed elsewhere; for further advice, see the American Academy of Child and Adolescent Psychiatry. 43 Similarly, psychological treatments may have increased relevance in the elderly, since older patients with depression are more vulnerable to medication side effects and drug interactions, as many may already be taking multiple medications for comorbid medical disorders. Treatment of depression in youth/adolescents, women, and those in late life is reviewed in Section 6. 44
2.5. What Are the Key Therapist Factors That Improve Clinical Outcomes?
Recommendations from the American Psychological Association Task Force on psychotherapy relationships 45 concluded that the best outcomes are likely to come from the concurrent use of evidence-based therapy relationships, not just evidence-based treatments. These conclusions were described as “demonstrably effective,” “probably effective,” and “promising, but insufficiently researched” (Table 4). 46,47 These recommendations are based on literature reviews and process research using secondary analyses, rather than experimental trials of the specific principles; thus, they are supported by Level 3 Evidence and are recommended as a first-line treatment practice. Three evidence-based common factors found to predict positive outcomes are establishing a strong therapeutic alliance, using empathy, and collecting client feedback (Table 4). 46 –49 Therapist characteristics that promote a therapeutic alliance include being genuinely respectful and interested in the well-being and safety of the patient, with empathy for subjective experience. 50 The collecting of patient feedback helps to track symptoms, experience of treatment, and functioning using validated scales (e.g., the Patient Health Questionnaire–9 [PHQ-9] 51 ) such that changes can be made if patients are not improving.
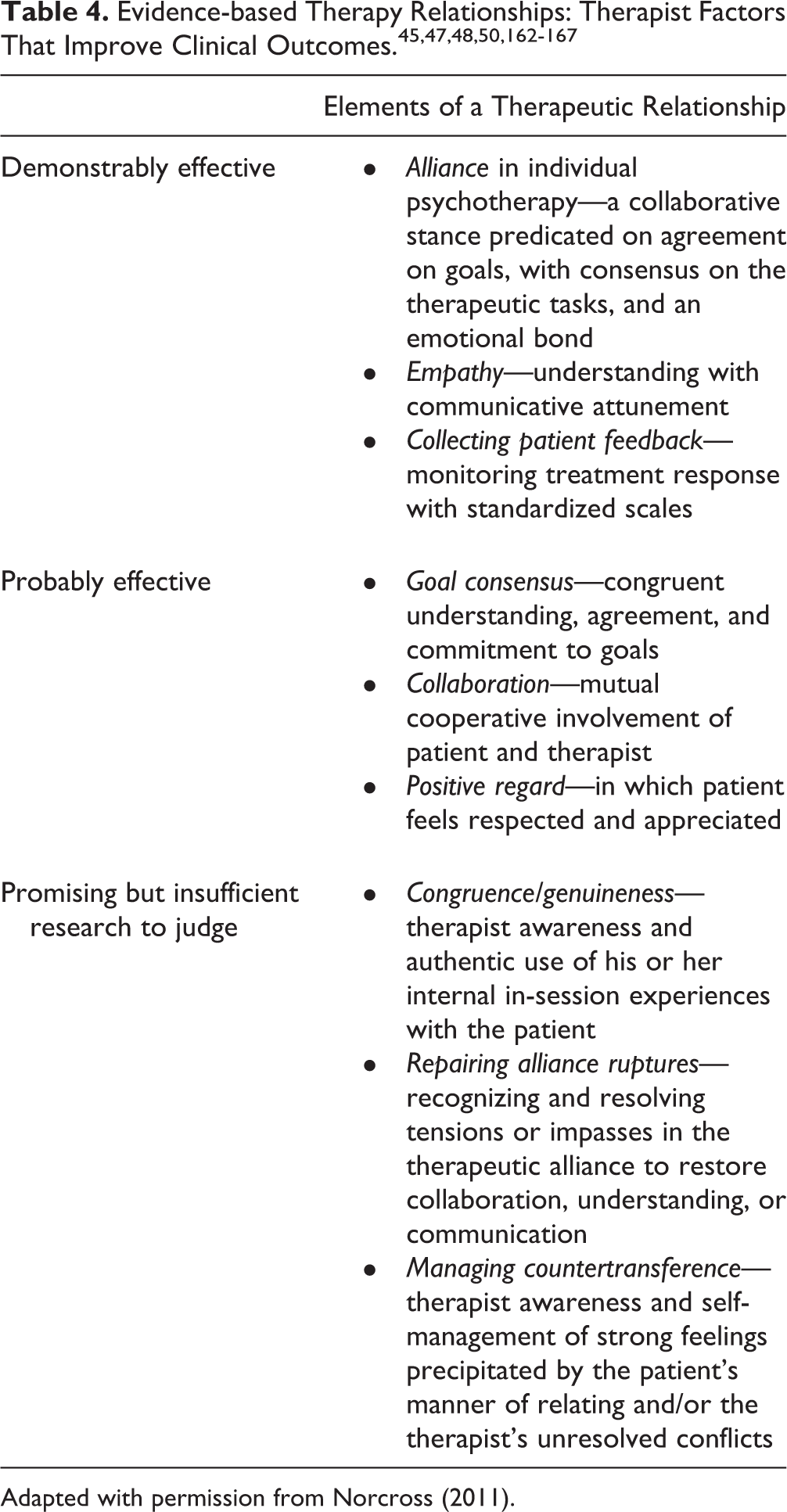
Adapted with permission from Norcross (2011).
Additionally, therapist supervision and feedback can improve patient outcomes, 52,53 although the research was not exclusively focused on patients with depression. Therapist experience, adherence, and ability to be responsive to individual patient differences are associated with better outcomes. 54,55 Most importantly, the evidence for psychological therapies for depression is based on studies with highly competent therapists, hence the second-line recommendation (Level 3 Evidence) that psychological therapies for depression should be delivered by trained and proficient therapists, although even less-trained therapists can have efficacy in treating depression and indeed may be the only source of treatment. 56
2.6. How Do You Choose a Psychological Treatment for MDD?
Choosing a specific type of psychological treatment should consider treatment efficacy, quality, and availability, as well as patient preference. Comparisons of different psychological treatments are fewer in number and quality, as well as complicated by methodological challenges, including lack of blinding and the effects of allegiance to a particular model.
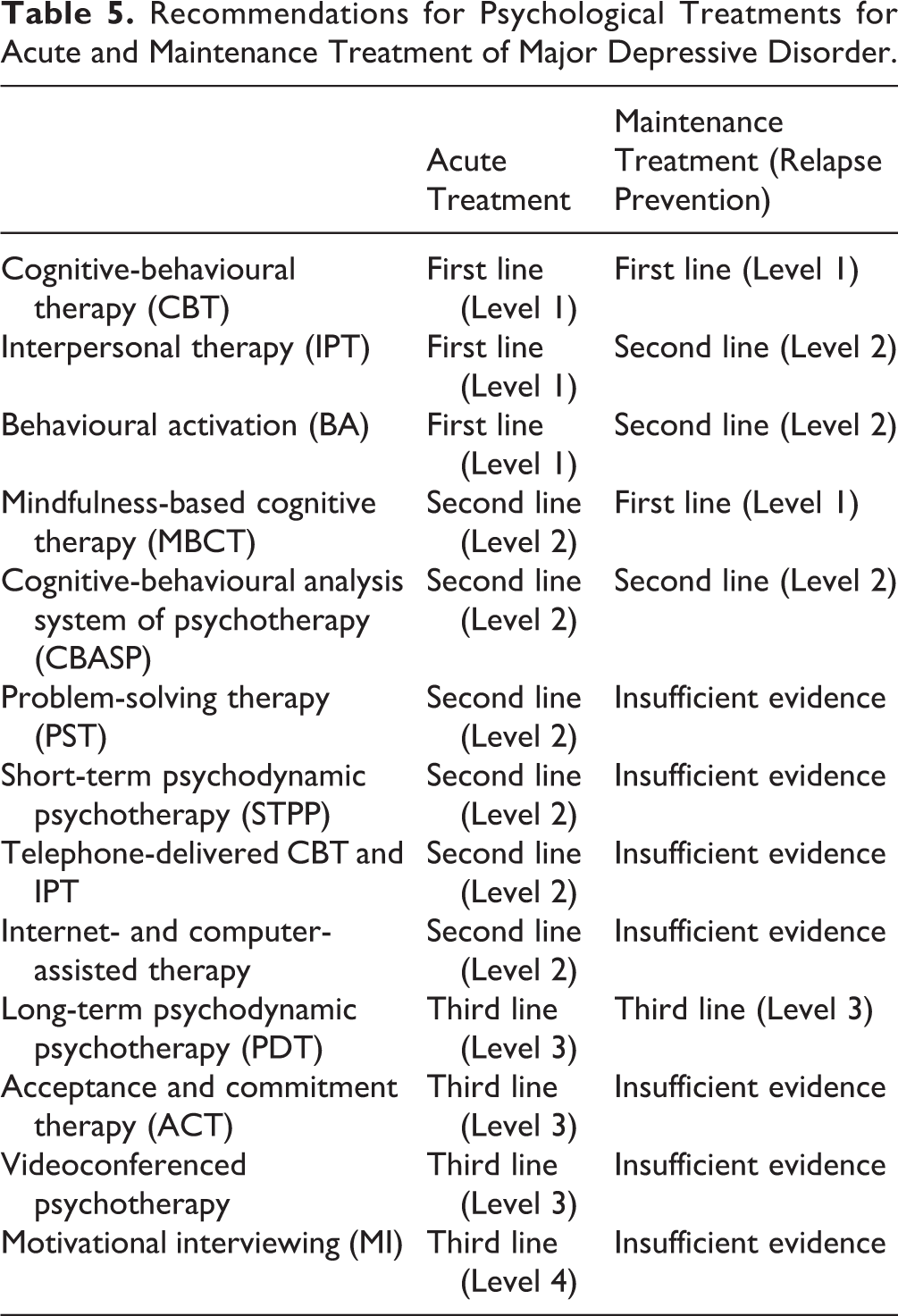
Table 5 lists recommendations for acute and maintenance psychological treatments (respectively) for depression, with the evidence level conveying the efficacy in comparison to control conditions, not to alternative psychological treatments. When choosing psychological treatment for a patient with depression, we recommend preferentially selecting from first-line treatments. Second-line treatments should be used if first-line treatments have failed or are unavailable. Third-line treatments should be reserved for use in specialist centres where first- and second-line treatments are also available. All high-quality evidence in psychotherapy research is based on studies where extensively trained therapists receive regular supervision and adhere to principles of the given therapeutic model with high fidelity. Therefore, the evidence-based recommendations do not extend to psychological treatments that eclectically use elements of different models.
Recommendations for Psychological Treatments for Acute and Maintenance Treatment of Major Depressive Disorder.
2.7. How Do Psychological Treatments for MDD Compare in Efficacy?
Some meta-analytic comparisons between specific models of psychological treatment have shown no significant differences in efficacy, 57 with others showing modest differences. 58 When only bona-fide therapies (defined as delivered by trained therapists, based on psychological principles, and designed to be a viable treatment) were considered, there were no differences between CBT and IPT, but CBT was more effective than other psychotherapies considered as a group 59 ; using a different definition of bona-fide therapy, supportive therapy was less effective than other types of therapy, with no differences between CBT, IPT, and psychodynamic psychotherapy (PDT). 60 Short-term psychodynamic psychotherapy (STPP) compared to other types of psychotherapies resulted in slightly worse outcomes on some measures of depression at the end of treatment. 61
Individual psychological treatments are discussed in more detail in the following, but in summary, CBT remains the most established evidence-based, first-line treatment for depression, both acute and maintenance. With more than 40 original reports and meta-analyses published on CBT for MDD or PDD since 2009, there is substantial evidence of efficacy even in severely affected individuals and in those who had not responded to treatment with antidepressants. 62,63 Similarly, there is evidence across populations (adult, adolescents, perinatal women) to support IPT as an alternative strong first-line treatment for acute MDD and second-line as a maintenance treatment. 64 –66 Mindfulness-based cognitive therapy (MBCT) has new evidence to qualify as a second-line acute treatment. With several meta-analyses demonstrating efficacy 67,68 and a large, high-quality RCT (N = 424) 69 demonstrating equal efficacy of MBCT to medication as maintenance treatment for recurrent MDD, MBCT has emerged as a first-line maintenance treatment adjunctive to medication.
While there are new studies using Internet- or smartphone-delivered treatment, a single additional face-to-face study together with a new meta-analysis including many older, small studies elevate behavioural activation (BA) to first-line treatment. 70,71 The evidence base for STPP has expanded with recent studies, including comparisons with CBT 72 and antidepressant medication 73 and a recently updated meta-analysis. 61 A key limitation of the STPP literature is the conflation of different models of psychodynamic therapy (PDT) into the broad term STPP, whereby no single model has a replicated large RCT with positive findings for MDD, unlike CBT and IPT. Consequently, STPP is recommended as a second-line therapy with Level 2 Evidence. While long-term PDT is not within the scope defined earlier of an acute treatment for depression, there is limited evidence of efficacy for acute MDD treatment. 74 Thus, the limited evidence base confines general PDT—as separate from specific STPP—as a third-line treatment. While the amount of evidence for the cognitive-behavioural analysis system of psychotherapy (CBASP) has increased, results of the most recent large trial (N = 491 in 3 conditions) are inconsistent with previous results and do not support the efficacy of CBASP. 75 Therefore, CBASP remains a second-line treatment for chronic depression. An updated meta-analysis of acceptance and commitment therapy (ACT) concluded that there is insufficient evidence of efficacy 76 ; therefore, ACT remains a third-line treatment. The evidence status for other types of psychotherapies has not changed significantly since the 2009 guidelines.
2.8. Does Group or Individual Format for Psychological Treatment Influence Outcome?
Meta-analyses that evaluated efficacy of group psychological therapy for depression concluded that it is more effective than treatment as usual. 77,78 However, group therapy was less effective than individual therapy at the end of treatment and had a higher dropout rate, although no differences were found at follow-up. 77 While efficacy evidence may slightly favour individual therapy, other factors, including availability, cost, and patient preference, are still important factors in choosing between group and individual treatments. Finally, given the gap between needed and available psychological treatments, group psychotherapy could improve access to treatment.
2.9. How Many Sessions of Psychological Treatment Are Required to Be Effective?
Recent research has examined shorter durations for various psychotherapies. Overall, there is Level 1 Evidence that brief interventions can be effective. A number of trials have demonstrated the efficacy of an 8-session CBT intervention. 79,80 A review of 4 small trials of an 8-session brief IPT intervention in depressed women also found efficacy, 81 while 2 other meta-analyses looking at brief (8 or fewer sessions) of CBT, MBCT, and PST noted significant efficacy in symptom reduction. 82,83 Studies comparing 8 versus 16 or more sessions are rare but suggestive of similar effectiveness. 84 –86
In the absence of definitive “dose-finding” trials, insufficient evidence exists to state a minimum dose; it is recommended that after selecting a first- or second-line psychological treatment, the specific treatment manual be followed. In several RCTs, 15,62,86,87 treatment was offered twice weekly for the first 2 to 8 weeks. Furthermore, in a recent analysis of 70 controlled studies (N = 5403), which account for natural recovery, there was no association between clinical improvement and the number of psychological treatment sessions or hours; however, a strong positive association was found for increased frequency of psychological treatment sessions per week and increased size of clinical improvement. 12 Thus, more frequent treatment sessions, particularly at the start of therapy, should be considered (Level 3 Evidence).
2.10. What Is Cognitive-Behavioural Therapy (CBT) and Its Efficacy in the Acute and Maintenance Phases of MDD Treatment?
CBT is an intensive, time-limited, symptom-focused psychological treatment built on the premise that depression is maintained by unhelpful behaviours and by inaccurate thoughts and beliefs about oneself, others, and the future. Behavioural interventions are aimed at increasing the patients’ participation in activities that promote a sense of pleasure and achievement and thus lift their mood. Patients also assess the impact of various behaviours on their mood. The cognitive techniques help patients evaluate the accuracy of their negative thoughts and beliefs. Practising the new skills outside the therapy room (i.e., homework) is crucial for the effectiveness of therapy.
Since 2009, several meta-analyses have been published 57,88,89 using the same database (www.evidencebasedpsychotherapies.com). The authors found that CBT is as effective as antidepressant medication, 88 and the combination of CBT and an antidepressant is more effective than either alone. 57,88,89 Results of a recent RCT 62 suggested that when both CBT and pharmacotherapy are of high quality, the addition of CBT to pharmacotherapy increases recovery rates. When participant characteristics were taken into account, this effect was limited to participants with severe nonchronic depression. CBT is also effective for people with treatment-resistant depression (i.e., those who did not respond to at least 2 adequate antidepressant trials). An RCT of 469 primary care patients with depression with poor response to medication found CBT improved response and remission, 63 with sustained effects at 3-year follow-up. 89 In summary, CBT has Level 1 Evidence of efficacy and continues to be recommended as a first-line treatment for acute treatment of MDD.
Regarding maintenance treatment, a meta-analysis of 9 RCTs comparing CBT and pharmacotherapy concluded that after 1 year, those who received CBT in the acute phase of depressive illness had a lower rate of relapse than those who discontinued medication. There was no difference, however, between the CBT group and those who continued pharmacotherapy at 1-year follow-up. 57 A meta-analysis of 10 trials demonstrated a reduction in the risk of relapse by 21% in the first year and by 28% in the first 2 years. 90 In a subsequent meta-analysis, which included more heterogeneous studies, CBT delivered during remission decreased the likelihood of relapse by 32%. The comparison with pharmacotherapy did not show a significant difference. 91 To prevent depressive relapse/recurrence, CBT versus pharmacotherapy delivered during the acute phase offers better protection. During maintenance phase treatment, CBT and pharmacotherapy provide comparable prevention of relapse. In summary, CBT has Level 1 Evidence and is recommended as a first-line maintenance therapy, whether the CBT is delivered either in the acute or maintenance phase of MDD.
2.11. What Is Mindfulness-Based Cognitive Therapy (MBCT) and Its Efficacy in the Acute and Maintenance Phases of MDD Treatment?
MBCT for MDD was formally developed as an 8-week group treatment designed to teach patients how to disengage from maladaptive cognitive processes through an integration of mindfulness meditation training and cognitive-behavioural techniques. 92 MBCT improves clinical outcomes via changes in mindfulness, rumination, worry, compassion, and meta-awareness, consistent with underlying theory. 93
MBCT was originally developed to prevent relapse in remitted patients. Clinical trials have supported its therapeutic value as an adjunct to treatment as usual 94,95 and its comparability to maintenance antidepressant medication 69,96 in this context. Of note, evidence has accrued to suggest that MBCT may only be efficacious or advantageous over other forms of aftercare for those patients with greater vulnerability, in the form of recurrent depression, 97,98 unstable remission, 99,100 or a history of childhood trauma 98 (although see also Geschwind et al. 101 ).
MBCT has been increasingly applied to treatment of residual depressive symptoms following treatment and more recently to depressive symptoms in the context of a full MDD, particularly in patients who have not responded to an earlier treatment. MBCT has exhibited efficacy as an augmentation to treatment as usual in a heterogeneous sample of both currently and remitted depressed outpatients, albeit with modest effect sizes. 102,103 MBCT has also exhibited superior efficacy to a psychoeducation control treatment 104 and comparable efficacy to group CBT, 105 although a brief follow-up period and small sample size, respectively, were notable in these studies.
In summary, MBCT is recommended as a second-line adjunctive treatment (Level 2 Evidence) for acute depression and as a first-line maintenance treatment (Level 1 Evidence).
2.12. What Is Interpersonal Therapy (IPT) and Its Efficacy in the Acute and Maintenance Phases of MDD Treatment?
IPT focuses on patients’ relational stressors involving losses, changes, disagreements, or interpersonal sensitivity, which are associated with the onset or perpetuation of present symptoms. The 4 focal interpersonal problem areas (i.e., bereavement, social role transitions, social deficits with interpersonal sensitivity, and disputes) each have a set of therapeutic guidelines. 106,107 The goals of IPT are to alleviate suffering, remit symptoms, and improve functioning.
A meta-analysis (16 RCTs, N = 1472) compared IPT to a control group for depression or depressive symptoms, with an effect size of 0.63. 65 A subsequent systematic review of comparative outcomes between IPT and other psychological treatments (8 studies, N = 1233) concluded that differences were small. 66 Finally, specific examination of IPT versus CBT for adults with MDD (7 trials, N = 741) found no differences between them. 64 In summary, Level 1 Evidence supports IPT as a first-line treatment for acute depression.
For maintenance treatment, a meta-analysis demonstrates that combined IPT with pharmacotherapy treatment was more effective than pharmacotherapy alone. 65 However, heterogeneity among the treatment formats (individualized vs. group) and small sample size in the studies reduce evidence to Level 2, and therefore IPT combined with medication is recommended as a second-line maintenance treatment for depression.
2.13. What Are Short-Term Psychodynamic Psychotherapy (STPP) and Long-Term Psychodynamic Therapy (PDT) and Their Efficacy in the Acute and Maintenance Phases of MDD Treatment?
Gunderson and Gabbard 108 have defined PDT as “a therapy that involves careful attention to the therapist/patient interaction with carefully timed interpretation of transference and resistance embedded in a sophisticated appreciation of the therapist’s contribution to the two-person field.” PDT has contributed deeply to understanding the importance of relationship/alliance issues (Table 4). Similarly, in the treatment of the depressed patient with comorbid personality disorder, PDT may have particular utility. 24 However, there is only weak evidence, and only after prolonged treatment, for efficacy of long-term PDT for acute treatment of MDD. 74,109 Hence, PDT is considered a third-line treatment for acute MDD.
For STPP, a meta-analysis identified 54 studies (33 RCTs). 61 STPP was significantly more effective than waitlist or treatment-as-usual control conditions, but some analyses indicated STPP was similar to other psychotherapies in outcomes while other findings noted STPP was significantly less effective on depressive symptoms than alternative psychotherapies at posttreatment. 61 Overall, the literature shows increasing evidence of a variety of improvements in outcomes related to STPP, but an absence of replication of specific models leaves evidence of efficacy at Level 2, and STPP models designed for depression should be considered second-line treatment. There is insufficient evidence to recommend STPP or PDT as a maintenance treatment for MDD.
2.14. What Is the Overall Level of Efficacy for Motivational Interviewing (MI) in the Acute and Maintenance Phases of MDD Treatment?
Motivational interviewing (MI) was originally designed for engaging and treating patients with substance use disorders 110 and takes the view that people approach change with ambivalence along a continuum of readiness. 111 There are no trials of MI as a stand-alone treatment for MDD; however, it has been used in conjunction with CBT, IPT, or medications to improve treatment engagement or adherence and for treatment of depression and comorbid substance misuse. For patients less likely to engage in or respond to unmodified treatments, it is worth considering integration of MI. 112 In the absence of specific MDD studies, evidence remains at Level 4 (expert opinion), and MI receives a third-line treatment recommendation.
2.15. What Is the Overall Level of Efficacy for Cognitive-Behavioural Analysis System of Psychotherapy (CBASP) in the Acute and Maintenance Phases of MDD Treatment?
CBASP was developed specifically for the treatment of chronic depression. 113 It involves cognitive, behavioural, and interpersonal strategies and is focused on helping patients to recognize how maladaptive cognitions and behaviours influence each other and lead to and perpetuate negative outcomes. Since the first CBASP trial published in 2000, 114 5 CBASP studies have been published that provide only mixed results supporting CBASP. 75,115 –118 Overall, Level 2 Evidence supports CBASP as a second-line monotherapy, or in combination with antidepressants, for partial-responding or nonresponding patients, in the treatment of PDD.
2.16. What Is Acceptance and Commitment Therapy (ACT) and Its Efficacy?
The aim of ACT is to mindfully increase acceptance of distressing experiences by taking an observer perspective and by clarifying and orienting behaviour towards valued directions, instead of struggling against or trying to control perceived suffering. 119 Since 2009, there have been 3 meta-analyses with a comparison of ACT to CBT. 120 –122 In 16 studies of various diagnoses, there was improvement in depressive symptoms and anxiety with ACT, although less than with CBT. ACT may also have particular value in the presence of comorbid medical conditions. 122 In the absence of specific large trials in MDD, evidence remains at Level 3 and ACT is recommended as a third-line treatment for MDD.
2.17. What Is Behavioural Activation (BA) for Depression and Its Efficacy?
The rationale for BA is that depression is caused and maintained by escape and avoidance of aversive emotions and stimuli that become self-reinforced and also prevents positive reinforcement of nondepressive behaviour, consequently causing longstanding patterns of inertia, avoidance, and social withdrawal. 123 Manuals are available to address techniques to be applied in BA. 124 –126
One meta-analysis (34 studies, N > 2000 patients with depressive symptoms, but not necessarily MDD) 127 found similar large effect sizes for BA and CBT compared to control conditions, as well as a similar effect to CBT. Subsequent clinical trials evaluating BA in MDD have almost exclusively involved Internet- or smartphone-delivered treatments as opposed to in-person therapy. 70,128,129 A subsequent meta-analysis (26 RCTs, N = 1524) that incorporated older studies, the Internet/smartphone studies, and 1 recent face-to-face trial reported a large effect size of BA compared to control conditions. 130,131 Overall, Level 1 Evidence supports BA as a first-line treatment for acute depression, with modest evidence that BA in acute depression provides protection against future relapse (Level 2), suggesting its role as a second-line treatment for maintenance.
2.18. What Are Peer Interventions and Their Efficacy for Depression?
Peer interventions for depression include self-help groups and peer-run organizations and services. 132 Peer support can be beneficial either alone or as a complement to clinical care. Guidelines from the Mental Health Commission of Canada provide direction to decision makers, program leaders, and the public about peer support training and practice. 133
An initial meta-analysis of peer support for depression was positive, but subsequent results are mixed. 134 –136 Given the general benefits of social and peer support, as well as the widespread availability of this resource, 137 peer interventions are recommended as a second-line adjunctive treatment for MDD (Level 2 Evidence).
2.19. What Is Problem-Solving Therapy (PST) and Its Efficacy?
PST is a structured brief, empirically tested intervention focusing on the adoption of adaptive problem-solving attitudes and skills to treat MDD. It has been shown to be more effective when training includes both positive problem orientation and problem-solving skills. 138
PST has been tested most extensively in primary care settings in individuals with a variety of depressive symptoms spanning subclinical depression, adjustment disorders, and MDD, with clear efficacy in reducing depressive symptoms. Both telephone-delivered and in-person PST were effective for treating MDD in low-income homebound older adults. 139 Two separate meta-analyses found that the use of PST as an acute treatment for late life depression resulted in a significant reduction of depressive symptoms as well as disability in comparison to control treatments. 138,140
Overall, since most studies include a focus on depressive symptoms rather than formal MDD, PST is recommended as a second-line acute treatment in primary care and geriatric depression (Level 2 Evidence); there is insufficient evidence to recommend PST as a maintenance treatment.
2.20. What Is Bibliotherapy and What Is Its Efficacy?
Bibliotherapy, the reading and use of self-help materials such as books to treat depression, has been tested in many older trials, particularly as RCTs involving a waitlist control compared to use of the book Feeling Good by David Burns. 141 With the expansion of computer/Internet approaches to self-help, very few bibliotherapy trials have been published since 2009. Although 1 RCT 142 highlighted the need for physician guidance to ensure active engagement, an RCT evaluating usual care versus prescription for Feeling Good found no difference in patient outcomes. 143 Overall, bibliotherapy has practical utility due to ease of use and low cost, may be useful for people waiting to be seen for clinical care, and remains a second-line treatment, either alone or as an adjunct to medication, ideally with clinician encouragement and monitoring.
2.21. How Effective Is Internet- and Computer-Delivered Therapy for Depression?
Meta-analyses and reviews of computer-based psychological treatment for the treatment of MDD, whether delivered over the Internet or as a stand-alone program, confirm efficacy. 144 –150 Internet- and computer-delivered therapy (I/CT) can also be helpful in relapse prevention. 151 I/CT studies usually use adaptations of CBT, but 1 trial compared updated versions of CBT and IPT with the established “MoodGym” online version of CBT with over 600 participants in each of the 3 groups; self-guided IPT was similar to the other treatments in reducing depressive symptoms. 152 When the Internet therapy is guided by a clinician, both adherence and efficacy are much more substantial. 88 Across psychiatric disorders, 1 meta-analysis 153 found that guided Internet CBT was no different in outcomes from face-to-face CBT, while a noninferiority study 154 specifically for depression also found no differences between the 2 approaches. I/CT remains a second-line treatment for depression, with improved efficacy if the I/CT is actively guided by a clinician.
2.22. How Effective Is Remote Interactive Psychological Treatment for Depression (Phone, Video, Internet) Compared to Face-to-Face Therapy?
Psychological treatments with a live therapist are being increasingly mediated by technology, whether by phone, videoconferencing, or live interaction over the Internet. In addition to CBT, a significant number of studies have evaluated other methods of telephone-delivered support and disease management.
Telephone-delivered psychological treatment remains the most studied model. In one of the first large trials (600 patients starting antidepressants in primary care offices), both 8-session CBT and disease management by phone improved clinical efficacy and satisfaction, compared to medication alone. 79 The same 8-session CBT phone intervention added to an antidepressant improved work performance and satisfaction compared to antidepressant alone. 80 Collectively, telephone-delivered CBT has Level 1 Evidence, while other therapies have Level 2 Evidence, positioning telephone-delivered therapy as a second-line treatment.
Videoconferencing approaches to psychological treatment may include use of traditional videoconference suites with television cameras in 2 different locations or, more recently, Internet technologies on personal computing devices, including Skype, Medeo, FaceTime, and many others. The broader application of such technologies to psychiatry has been extensively reviewed and found to be acceptable and generally equivalent to face-to-face care for many psychiatric conditions. 155,156 Relatively few studies have been done using videoconferencing for MDD, but there is limited evidence of efficacy in several small RCTs, 156 –158 suggesting that videoconferenced psychological treatment for depression may be considered a promising third-line treatment.
2.23. Is Combined Psychological Treatment with Medication Superior to Psychological Treatment Alone?
Accumulated evidence shows that combined psychological and antidepressant treatment is more effective than psychological treatment alone or psychological treatment with placebo. 159,160 The evidence is mostly based on studies where either CBT or IPT was delivered alone and combined with selective serotonin reuptake inhibitors (SSRIs) or tricyclic antidepressants (TCAs). There was a trend for SSRIs and IPT to be less effective in combinations than TCAs, CBT, and other psychotherapies. The small to moderate effect size of the differences suggests that combined treatment should be offered to individuals with moderate to severe depression based on a consideration of benefit-burden balance and preferences of a given patient.
2.24. Is Combined Psychological Treatment with Medication Superior to Medication Alone?
A recent meta-analysis shows that psychological treatment combined with antidepressants is more effective than antidepressants alone. 159 The evidence is primarily based on studies where individual CBT or IPT was combined with SSRIs or TCAs. The effect size of the difference was moderate, suggesting that combined treatment should be offered in preference to antidepressants alone to individuals with moderate to severe depression.
2.25. Is Sequential Treatment Superior to Monotherapy?
A meta-analysis of 8 studies found that psychological treatment after antidepressant treatment reduces the likelihood of relapse by 20%, compared to treatment as usual, which included discontinuation of antidepressants. 161 Although the meta-analysis aimed to examine the effect of any type of psychological treatment, the evidence was limited to CBT and MBCT. 161 In addition, a large pragmatic trial found that a course of up to 18 sessions of face-to-face individual CBT significantly reduced depressive symptoms and increased the likelihood of therapeutic response to antidepressants in treatment-resistant depression. 63 Another large primary care trial compared the effects of group MBCT and maintenance antidepressant therapy on time to relapse; while there were no significant differences between the 2 conditions, the risk of relapse was greater in those who had prematurely discontinued antidepressant treatment. 69 In contrast, PDT (up to 60 sessions over 18 months) did not significantly increase the likelihood of remission. 74
In summary, CBT or MBCT is recommended as sequential first-line treatment (Level 1 Evidence) after a course of antidepressants, and MBCT is recommended as a second-line alternative to long-term maintenance antidepressant treatment (Level 2 Evidence).
Footnotes
Disclosures
The guidelines process and publication were funded entirely by internal CANMAT funds; no external support was sought or received. No honoraria were paid to authors and no professional editorial assistance was used. All members of the CANMAT Depression Work Group disclosed potential conflicts of interest (available at ![]() ). CANMAT is a project-driven organization governed by a volunteer, unpaid advisory board, with no permanent staff or dedicated offices. CANMAT has a conflict of interest policy that includes disclosures by all participants, and all continuing professional development (CPD) projects are accredited by academic institutions. CANMAT has diverse funding, but in the past 5 years (2011-2015), sources of CANMAT revenue (excluding CIHR and research funding) included national/international scientific conferences (28% of revenue), publications (26%), industry-supported CPD projects (26%), and academic projects (18%).
). CANMAT is a project-driven organization governed by a volunteer, unpaid advisory board, with no permanent staff or dedicated offices. CANMAT has a conflict of interest policy that includes disclosures by all participants, and all continuing professional development (CPD) projects are accredited by academic institutions. CANMAT has diverse funding, but in the past 5 years (2011-2015), sources of CANMAT revenue (excluding CIHR and research funding) included national/international scientific conferences (28% of revenue), publications (26%), industry-supported CPD projects (26%), and academic projects (18%).
The CANMAT guidelines are not officially endorsed by the Canadian Psychiatric Association.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
SVP has been a consultant to Bristol Myers Squibb, Lundbeck, and Takeda; has had a research contract with Assurex; and has equity in Mensante.
LCQ, PR, BP, VV, and RU have nothing to disclose.
MR received honoraria from AstraZeneca, Bristol-Myers Squibb, Canadian Psychiatric Association, Eli Lilly, Lundbeck, Otsuka, Pfizer, and Sunovion.
SG has received honoraria as a consultant, member of an advisory committee, or for lectures from Actavis, Bristol Myers Squibb, Eli Lilly Canada, and Pfizer, as well as research grant support from Canadian Institutes of Health Research, CR Younger Foundation, Ontario Mental Health Foundation, and Ontario Ministry of Health and Long-Term Care.
SHK has received honoraria for ad hoc speaking or advising/consulting or received research funds from Allergan, Brain Canada, Bristol-Myers Squibb, Canadian Institutes of Health Research, Janssen, Lundbeck, Ontario Brain Institute, Pfizer, St. Jude Medical, Servier, and Sunovion.
RWL has received honoraria for ad hoc speaking or advising/consulting or received research funds from Asia-Pacific Economic Cooperation, AstraZeneca, Brain Canada, Bristol-Myers Squibb, Canadian Institutes of Health Research, Canadian Depression Research and Intervention Network, Canadian Network for Mood and Anxiety Treatments, Canadian Psychiatric Association, Coast Capital Savings, Johnson & Johnson, Lundbeck, Lundbeck Institute, Medscape, Pfizer, St. Jude Medical, Takeda, University Health Network Foundation, and Vancouver Coastal Health Research Institute.
GMM has been on advisory board or speaker for Janssen, Lilly, Lundbeck, and Pfizer.
RVM has received speaker and consultant honoraria or research funds from Allergan, Bristol-Myers Squibb, Canadian Institutes of Health Research, Canadian Network for Mood and Anxiety Treatments, Canadian Psychiatric Association, Eli Lilly, Johnson & Johnson, Lallemand, Lundbeck, Merck, Ontario Brain Institute, Ontario Mental Health Foundation, Otsuka, Paladin, Pfizer, Queen’s University, Sunovion, Takeda, the University Health Network Foundation, and Valeant.
AVR has received speaker and consultant honoraria or research funds from Bristol-Myers Squibb, Canadian Depression Research and Intervention Network, Canadian Foundation for Innovation and the Ministry of Economic Development and Innovation, Canadian Institutes of Health Research, Grand Challenges Canada, Janssen, Lundbeck, Ontario Mental Health Foundation, Pfizer, and Sunovion.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.