
Abstract
Objective:
To explore the effects of baseline psychological and antidepressant medication treatment in a trial of lay telephone coaching in a low-intensity, supported depression self-care intervention.
Method:
A single blind, individually randomised, pragmatic trial was conducted among primary care adults with chronic physical conditions and comorbid depressive symptoms. Eligible subjects were randomised to receive a depression self-care toolkit with (intervention group) or without (control group) telephone coaching provided by trained lay coaches. For this brief communication, a secondary analysis of the trial data focused on the effects of baseline psychological and antidepressant treatments on mental health outcomes (Patient Health Questionnaire 9 [PHQ-9], SF-12 Mental Component Summary [MCS], Generalized Anxiety Disorder 7 [GAD-7]) and satisfaction with the intervention.
Results:
In total, 223 patients were randomised, and 165 (74.0%) completed both 3- and 6-month follow-ups. There were 2 significant interactions of baseline treatment and study group for 6-month mental health outcomes. A significant benefit of coaching on 6-month PHQ-9 was seen only among participants who were not receiving baseline psychological treatment. A smaller interaction was found for baseline antidepressant medications and 6-month mental health. There was a significant main effect for baseline psychological treatment and lower 6-month satisfaction.
Conclusions:
Depressed patients receiving baseline psychological treatment may not benefit from lay coaching offered as part of a low-intensity depression self-care intervention.
We recently reported the results of a single blind, individually randomised, pragmatic trial that compared 2 active treatments varying in intensity: a depression self-care toolkit with or without lay telephone coaching among primary care adults with comorbid chronic physical conditions and comorbid depressive symptoms. 1 The intervention group received the toolkit and was offered coaching; the control group received the toolkit only. We had hypothesized that coaching would be associated with improved depressive symptoms at 6 months (the primary outcome) with an effect size of at least 0.4. 2 We found that coaching was indeed effective in reducing the severity of depressive symptoms at 3 months (effect size, 0.44; 95% confidence interval, 0.16 to 0.72) but not at 6 months postrandomisation (effect size, 0.24; 95% confidence interval, –.01 to 0.60).
The purpose of this secondary analysis is to explore the effects of baseline depression treatment on mental health outcomes and potential interactions of coaching with these treatments. Due to the pragmatic intent of the trial, we did not exclude patients receiving baseline antidepressant medication or psychological treatment other than cognitive-behavioral therapy (CBT); those receiving CBT at baseline were excluded due to the similar approach used in the study intervention. As part of our preplanned analyses, we analyzed 5 primary outcomes and 15 secondary potential intervention modifiers, 2 and we found that only baseline Patient Health Questionnaire 9 (PHQ-9) and self-efficacy interacted significantly (P < 0.1) with the intervention. 1 Patients with mild and severe depression symptoms (PHQ-9 of <10 and 20+, respectively) at baseline and those with lower self-efficacy for depression self-care at baseline did not appear to benefit from the coaching intervention. Because the current analysis was not preplanned but suggested during analyses of adherence to the intervention, 3 it should be considered exploratory.
Methods
Design and Participants
The methods have been reported in detail elsewhere. 1 Eligible participants were not suicidal, had at most mild cognitive impairment, 4,5 and had no visual, hearing, or other physical impairment that would prevent them from using the toolkit or participating in telephone interviews. As the goal was to assess the effectiveness of the intervention under usual primary care conditions, we did not exclude patients who were taking antidepressant medications or were receiving psychological treatment. However, because the intervention was based on principles of CBT, we excluded patients who were receiving CBT at baseline. Following written informed consent, participants were randomised and a baseline interview was conducted.
Interventions
Immediately after randomisation, all participants received the toolkit, described elsewhere. 1 Participants randomised to the intervention group were also assigned a trained lay coach. After the first 2 telephone contacts in which the toolkit was introduced, patients were offered weekly calls for up to 3 months, followed by monthly calls up to 6 months postrandomisation.
Measures
The severity of depression was measured with the PHQ-9 at 3 and 6 months after randomisation, administered by a telephone interviewer who was blinded to the randomisation assignment. The 6-month PHQ-9 score was the primary outcome. 6,7 Secondary outcomes included satisfaction with the intervention, 1 severity of anxiety (Generalized Anxiety Disorder 7 [GAD-7]), 8 and the SF-12 Mental Component Summary (MCS) score. 9
Treatment measures at baseline included current antidepressant medication (coded from self-reports of medication prescriptions used in the week before baseline) and non-CBT psychological treatment. Sociodemographic variables included age, sex, and educational attainment. Coach contacts were recorded by coaches in coaching logs.
Data Analysis
We used linear regression for continuous outcomes (PHQ-9, GAD-7, and MCS) and logistic regression for the binary outcome (satisfaction). 9,10 For modeling and for subgroup analysis, we used strategies similar to those in our previous report. 1 We assessed the effects of baseline antidepressant medication treatment, non-CBT psychological treatment, and study group on each outcome, with adjustment for baseline variables with potentially important differences by study group and the baseline value of the outcome (if appropriate). To each model, we added interaction terms between study group and each type of treatment; in addition, analyses were performed for each outcome by including the 2 interaction terms. In a further analysis, we revisited our previous results, 1 in which the 6-month PHQ-9 was found to be significantly affected by the interaction of the intervention with 2 baseline variables, each comprising 4 categories: PHQ-9 (3 interaction terms) and self-efficacy (3 interaction terms). To test whether these findings remain significant (P < 0.1), we fitted in our study sample (n = 165) the interaction terms for PHQ-9 and self-efficacy while adding the interaction term between intervention and non-CBT counseling.
All the analyses were conducted at a 0.05 level of significance; 95% confidence intervals of the estimate (beta or odds ratio) were computed from the model; interaction terms with P < 0.1 (as recommended in a similar context) 11 were explored further with stratified analyses using the 0.05 level of significance. To explore possible differences in coaching associated with treatment, the t test was used to compare the number of coach contacts by treatment in the intervention group. SAS version 9.4 (SAS Institute, Cary, NC) was used to conduct all the analyses.
Results
Among 407 eligible patients screened for the study, 223 (55%) consented to participate and were randomised; of these, 165 (74.0%) completed both 3- and 6-month follow-up, with similar rates in the 2 study groups. Overall, 39.6% and 22.4% of participants were receiving baseline antidepressant medication and non-CBT psychological treatment, respectively (Table 1). There were no statistically significant differences by study group at baseline, but baseline differences in education, PHQ-9, and both types of treatment were judged potentially important. Education and PHQ-9 were added to all regression models as covariates (both treatment types were systematically included). We found 2 significant interactions (P < .10) of baseline treatment with study group: with baseline psychological treatment for 6-month PHQ-9 and with antidepressant treatment for 6-month MCS (Table 2). In both cases, a benefit of coaching was seen only among those not receiving treatment at baseline: for 6-month PHQ-9, this benefit was statistically significant, while for MCS, the benefit was small and nonsignificant (Table 2).
Baseline Characteristics of Participants and Baseline and 6-Month Treatments, by Study Group (n = 165).
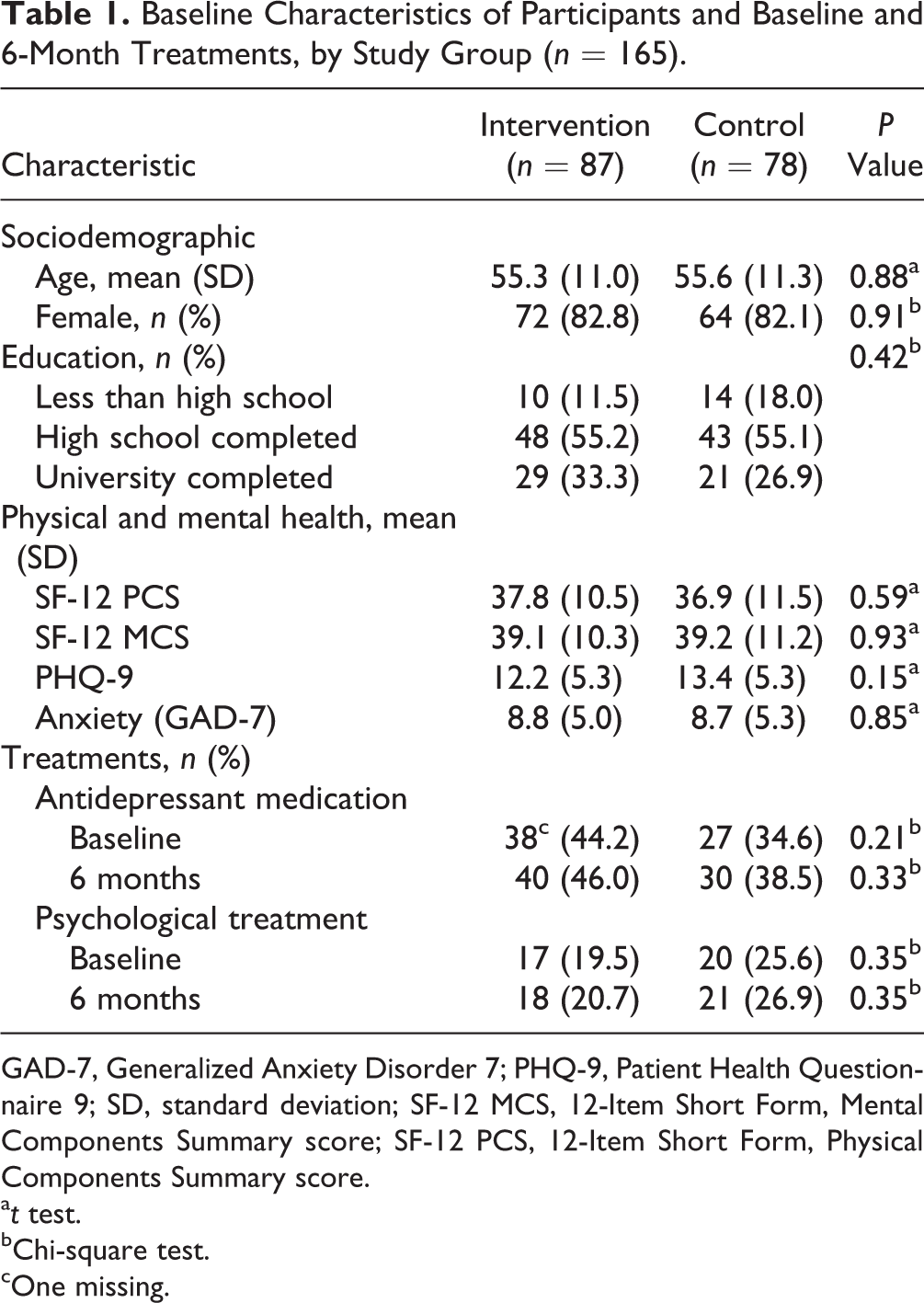
GAD-7, Generalized Anxiety Disorder 7; PHQ-9, Patient Health Questionnaire 9; SD, standard deviation; SF-12 MCS, 12-Item Short Form, Mental Components Summary score; SF-12 PCS, 12-Item Short Form, Physical Components Summary score.
a t test.
bChi-square test.
cOne missing.
Effects of Baseline Treatments on Study Outcomes (n = 165).
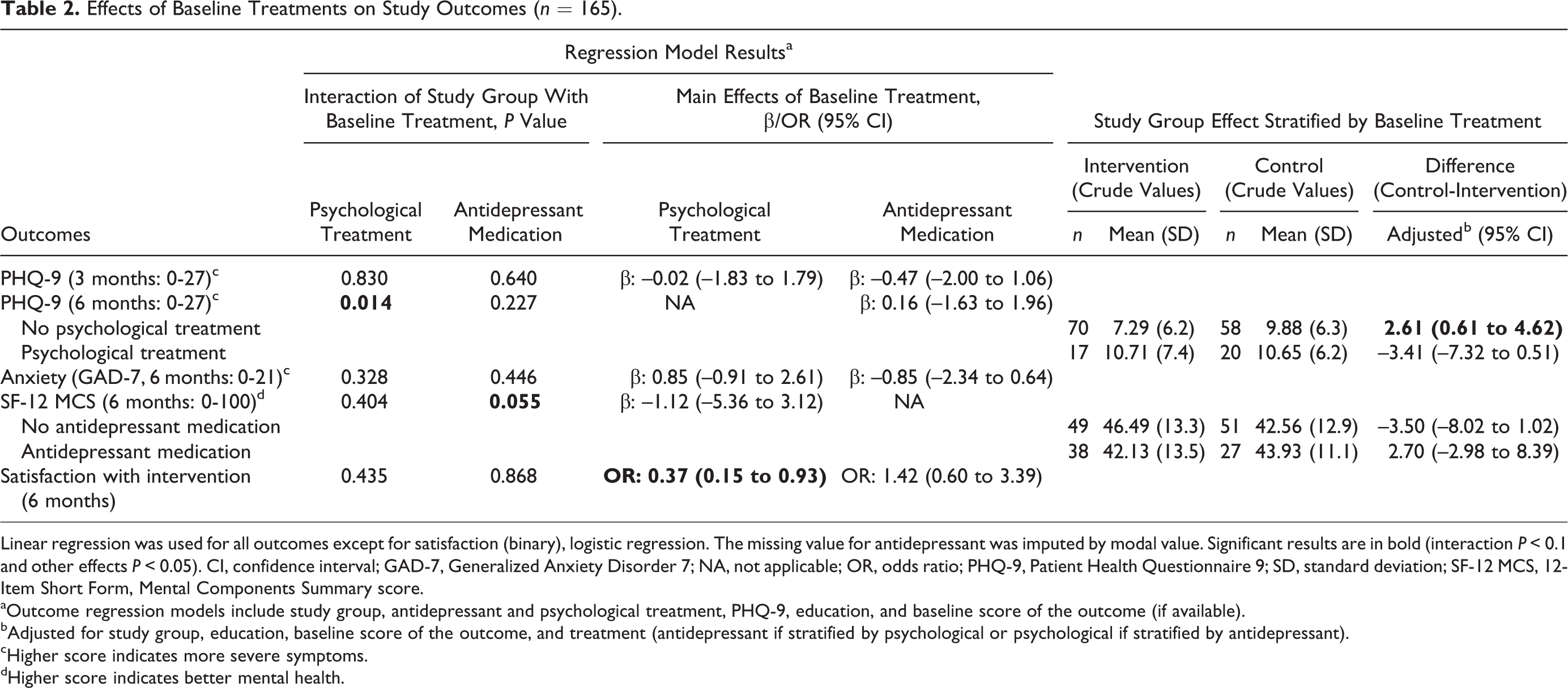
Linear regression was used for all outcomes except for satisfaction (binary), logistic regression. The missing value for antidepressant was imputed by modal value. Significant results are in bold (interaction P < 0.1 and other effects P < 0.05). CI, confidence interval; GAD-7, Generalized Anxiety Disorder 7; NA, not applicable; OR, odds ratio; PHQ-9, Patient Health Questionnaire 9; SD, standard deviation; SF-12 MCS, 12-Item Short Form, Mental Components Summary score.
aOutcome regression models include study group, antidepressant and psychological treatment, PHQ-9, education, and baseline score of the outcome (if available).
bAdjusted for study group, education, baseline score of the outcome, and treatment (antidepressant if stratified by psychological or psychological if stratified by antidepressant).
cHigher score indicates more severe symptoms.
dHigher score indicates better mental health.
The interaction of the intervention with baseline non-CBT psychological treatment is shown graphically in Figure 1. For those without baseline psychological treatment, mean PHQ-9 scores remained lower at 6 months in the intervention versus the control group. For those with baseline non-CBT counseling, members of the control group had higher mean PHQ-9 scores at baseline than intervention group members but similar mean scores at 6-month follow-up. In fact, mean PHQ-9 scores in the intervention group with baseline non-CBT psychological treatment improved at 3 months but returned to the baseline level at 6 months. For the PHQ-9 6-month outcome, 2 additional models were developed from the model containing the interaction between intervention and baseline non-CBT psychological treatment. For the first model, the interaction terms between intervention and baseline PHQ-9 were added: the previously significant interaction for those with baseline PHQ-9 of 20+ (P = 0.083) 1 became nonsignificant (P = 0.186). For the second model, the interaction terms between intervention and baseline self-efficacy were added: the interaction remained significant for the highest self-efficacy group (score, 9-12; P = 0.044).
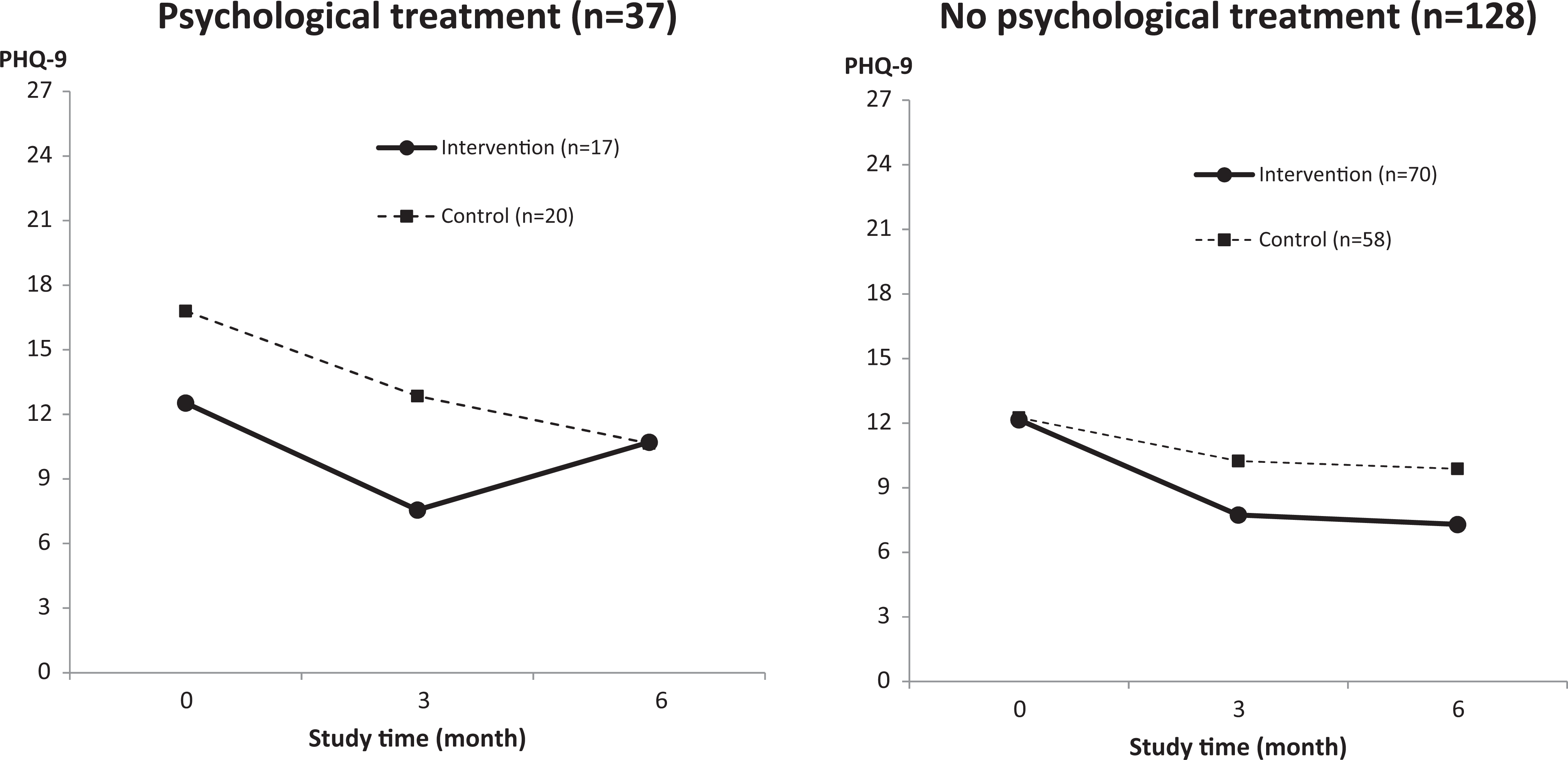
Mean Patient Health Questionnaire 9 (PHQ-9) scores at baseline, 3 months, and 6 months by study group, stratified by baseline psychological treatment without cognitive-behavioral therapy (n = 165).
There was also a significant effect of treatment on satisfaction: participants receiving baseline non-CBT psychological treatment were significantly less satisfied with the intervention (Table 2). There was no effect of treatment on anxiety.
For patients who received the coaching intervention, neither type of treatment was significantly associated with the number of completed coach calls (range, 0-15 calls). For those with versus without treatment, respectively, we found the following means and standard deviations for number of coach calls: 11.2 (4.1) versus 10.6 (4.4), P = 0.57, for psychological treatment and 11.3 (4.3) versus 10.3 (4.4), P = 0.32, for antidepressant medication.
Discussion
In exploratory analyses, we found that baseline non-CBT psychological treatment was an important modifier of the effect of lay telephone coaching of a depression self-care intervention. The hypothesized beneficial effect of lay coaching on the primary outcome (effect size of 0.4 for the PHQ-9 at 6 months) was limited to most patients who were not receiving psychological treatment at baseline. The weaker overall effectiveness of the intervention reported previously 1 was thus diluted by the inclusion of patients receiving non-CBT psychological treatment; these patients had a positive effect of weekly coaching at 3 months but a subsequent relapse at 6 months after the frequency of coaching was reduced to monthly. Interestingly, the interaction with baseline non-CBT psychological treatment also appears to explain the interaction we previously reported with baseline PHQ-9. We previously found that participants with severe depression symptoms at baseline (PHQ-9 of 20+) did not benefit from coaching. This effect appears to be explained by those participants receiving baseline non-CBT psychological treatment (whose PHQ-9 scores tended to be high).
Two potential mechanisms for this effect might be considered. First, patients who have previously sought psychological treatment for their depression but continue to experience symptoms may be more resistant to a self-care intervention that is likely to be less intense than face-to-face therapy. They may improve initially with weekly coaching but then relapse when coaching is less frequent. Second, the content of the coaching may conflict in some way with the face-to-face therapy. The lower satisfaction with the intervention reported by participants who were receiving baseline non-CBT psychological treatment is consistent with both of these potential mechanisms. The effect does not appear to be explained by the number of coaching sessions received.
Antidepressant medication was a weak modifier of the coaching effect but may be clinically unimportant. 12 This finding is inconsistent with research that has found a synergistic relationship of antidepressant and psychological treatments on depression outcomes. 13
These results should be interpreted with caution as they were based on exploratory analyses and not on testing a priori hypotheses. The analysis does not meet conventional criteria for the validity of subgroup analyses, including statistical power 14 and evidence for the validity of patient reports of current treatment. 15 Nevertheless, it is recommended that exploratory analyses of potential modifiers should be included in meta-analyses. 15 Despite these limitations, it may be prudent either to exclude participants receiving psychological treatment from future trials of coached mental health self-care interventions or to carefully monitor other concurrent treatments and conduct analyses of their effects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.