
Abstract
Objective:
Burnout is a serious problem for health care providers that has implications for clinical practice and personal health. While burnout is known to affect residents, no studies have examined the prevalence or impact of burnout among Canadian psychiatry residents.
Method:
Residents in all Canadian psychiatry training programs were surveyed between May 1, 2014, and July 1, 2014. The survey included a well-validated, single-item measure to assess symptoms of burnout, several demographic questions, and Likert-scale items to assess residents’ appraisals of empathic functioning and strategies for coping with stress from patient encounters.
Results:
Responses were obtained from 400 residents, for a response rate of 48%. Twenty-one percent (N = 84) of residents reported symptoms of burnout. Burnout was reported more frequently by residents in postgraduate year 2 than by those in other years and was associated with engagement in personal psychotherapy during residency. No association was found between burnout and age, gender, or location of residency program. Residents who endorsed symptoms of burnout reported higher levels of compromised empathic functioning, were less likely to consult with supervisors about stressful clinical experiences, and were more likely to engage in unhealthy coping strategies.
Conclusions:
Symptoms of burnout affect one-fifth of Canadian psychiatry residents. The associations between burnout symptoms and problematic clinical and personal functioning suggest areas of concern for those involved in the training of Canadian psychiatry residents.
Clinical Implications
Symptoms of burnout are prevalent among psychiatry residents and are associated with reduced empathy and problematic strategies for coping with patient-related stress. Psychiatry training programs should implement strategies to address and prevent burnout.
Limitations
A single-item burnout measure is not inclusive of a wider range of burnout symptoms. The cross-sectional nature of the survey does not reveal the direction of associations.
Burnout is an occupational syndrome characterized by emotional exhaustion, feelings of cynicism and detachment toward patients, and a reduced sense of personal accomplishment. 1 Among health care providers, burnout is a serious problem associated with increased medical errors, decreased capacity for empathy, and deviation from best practice guidelines. 1 –6 Burnout is also harmful to practitioners; it is often linked with anxiety, depression, substance use, and suicidal ideation. 1,6,7
Psychiatry residency training is a transitional period that warrants particular attention to the issue of burnout. The combination of long work hours, on-call obligations, financial strain, and increased clinical responsibility can place a heavy burden on residents as they learn the complexities of psychiatric practice. Moreover, psychiatry residents are exposed to emotionally taxing experiences such as violent patients and patient suicide. 8 –10 Attention to burnout during residency is also important given the potential to implement proactive preventive and management strategies early in physicians’ careers. 11 Surprisingly, few studies have systematically examined the prevalence of burnout among psychiatry residents, and none have looked at the prevalence across multiple institutes. A small U.S. study found that 40% of psychiatry residents endorse burnout—less than residents in other medical and surgical specialties but more than those in family practice. 12 Another U.S. study found lower rates of burnout among residents in psychiatry compared with family medicine (incidence of burnout was not reported). 13 A study in the Netherlands, however, found the 29% incidence of burnout among psychiatry residents to be the highest of 6 specialties studied. 14 These incongruent data suggest that the impact of training may be quite variable across nations and thus of limited generalizability to Canadian residents. To our knowledge, no study to date has evaluated the rate and implications of burnout among Canadian psychiatry residents.
The present study was designed to determine the prevalence and associated features of burnout symptoms among Canadian psychiatry residents. As part of a larger study on residents’ engagement in personal psychotherapy, 15 we surveyed residents across all training programs in Canada about their experience of burnout symptoms as well as their appraisal of their current empathic functioning and strategies for coping with stressful patient encounters.
Methods
The survey items in this study were included in a 43-item questionnaire on personal psychotherapy that was distributed to all of the 839 active psychiatry residents in Canada between May 1, 2014, and July 1, 2014. 15 The survey was pilot-tested by resident representatives and reviewed by the Coordinators of Psychiatric Education (COPE) before electronic distribution through each program’s resident COPE representative. A raffle to win a $1000 gift certificate was offered to incentivize participation. The survey was anonymous, and residents’ contact information could not be linked to their responses. The study was approved by the University of British Columbia Research Ethics Board.
The present study inquired about residents’ (a) basic demographic information; (b) use of personal psychotherapy; (c) levels of burnout symptoms; (d) appraisal of empathic functioning; and (e) strategies for coping with stress from patient encounters. In the interest of brevity and increased response rates, symptoms of burnout were assessed with a single item (see Table 1) that has been validated in previous studies as being highly correlated with the Maslach Burnout Inventory emotional exhaustion scale. 16,17 Likert-scale items were used to assess residents’ appraisals of empathic functioning and coping strategies.
Demographic information and responses to burnout survey among Canadian psychiatry residents, N = 400.
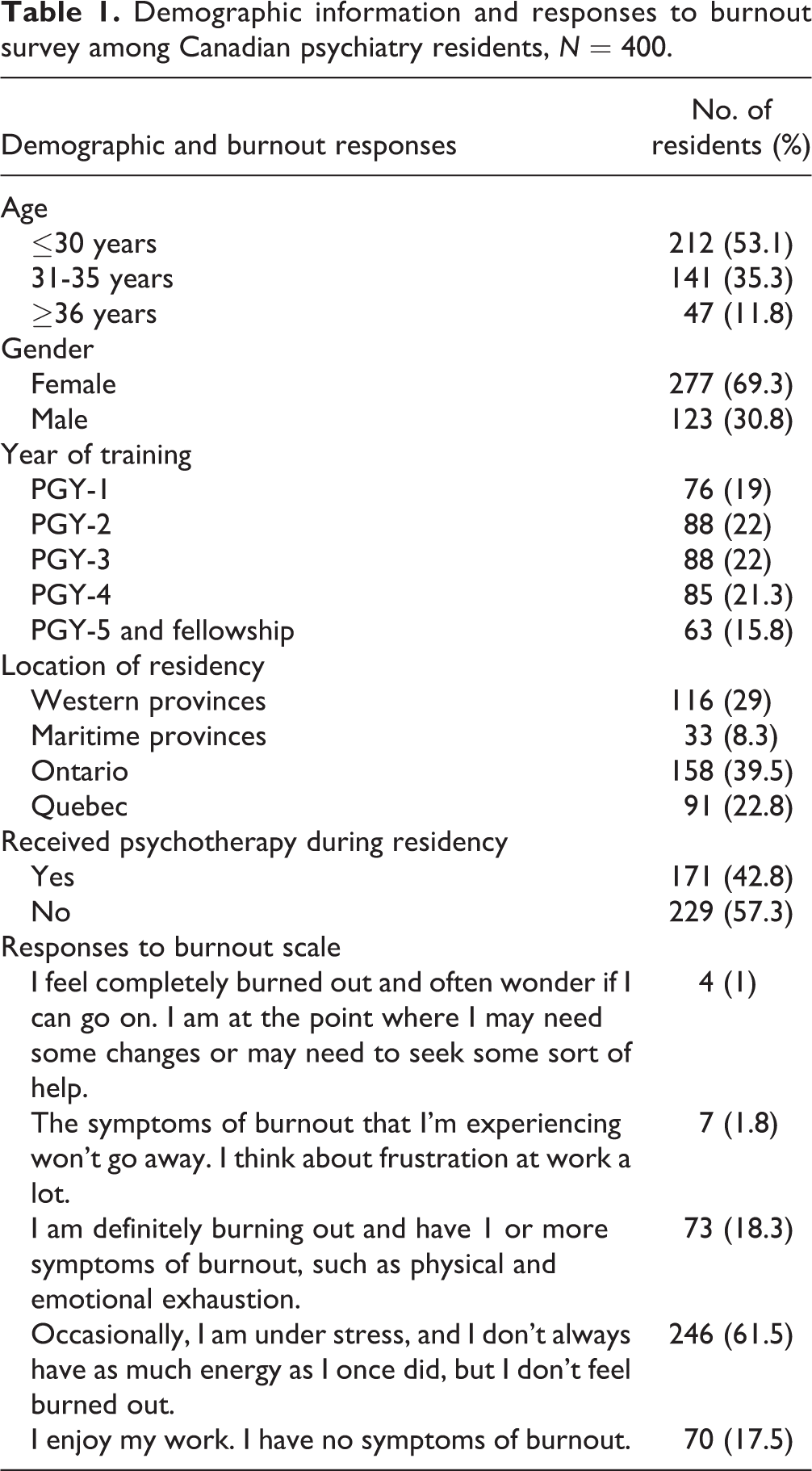
Standard descriptive statistics were used to characterize the sample. Consistent with previous research, 17 the burnout item was dichotomized, with scores on the lower 2 categories indicating no symptoms of burnout and scores on the higher 3 categories affirming at least 1 symptom of burnout. Associations between burnout symptoms and categorical variables were assessed using chi-square tests. Mann-Whitney U tests were used to compare between residents who endorsed burnout and those without burnout symptoms with regard to the Likert-scale items (significance set at P < 0.01 to adjust for multiple tests).
Results
A total of 400 residents returned the survey, with responses from every program across Canada, yielding a response rate of 48%. Demographic data and responses to our burnout scale are reported in Table 1. Respondents’ gender distribution was similar to that of Canadian residents generally (64.3% female). Twenty-one percent (N = 84) of residents reported symptoms of burnout. Chi-square tests found no association between burnout symptoms and age, gender, or location of residency program. A significant association was noted between burnout symptoms and year of training (χ 2 = 12.22, df = 4, P = 0.016), with symptoms of burnout reported more frequently by postgraduate year (PGY)-2 residents at 31%, followed by PGY-3 at 27%, PGY-4 at 18%, PGY-5 at 16%, and PGY-1 at 8%. An association was also found between personal psychotherapy during residency and symptoms of burnout (χ 2 = 5.09, df = 1, P = 0.024); of those who reported burnout symptoms, 54% had undertaken personal psychotherapy during residency. Mean scores for Likert-scale items regarding empathic functioning and coping strategies are reported in Table 2 according to residents’ endorsement of burnout symptoms. Analysis with Mann-Whitney U tests found significant differences between residents who reported symptoms of burnout and those who did not with regard to empathic functioning, consultation with supervisors, and use of unhealthy coping mechanisms. Residents endorsing burnout symptoms were more likely to appraise their current capacity for clinical empathy to be compromised and were significantly less likely to consult with supervisors regarding stressful patient encounters. These residents were also more likely to engage in unhealthy coping mechanisms such as alcohol use, excessive shopping, or unhealthy eating.
Psychiatry residents’ appraisal of empathic functioning and reported strategies for coping with work-related stress, N = 400a.
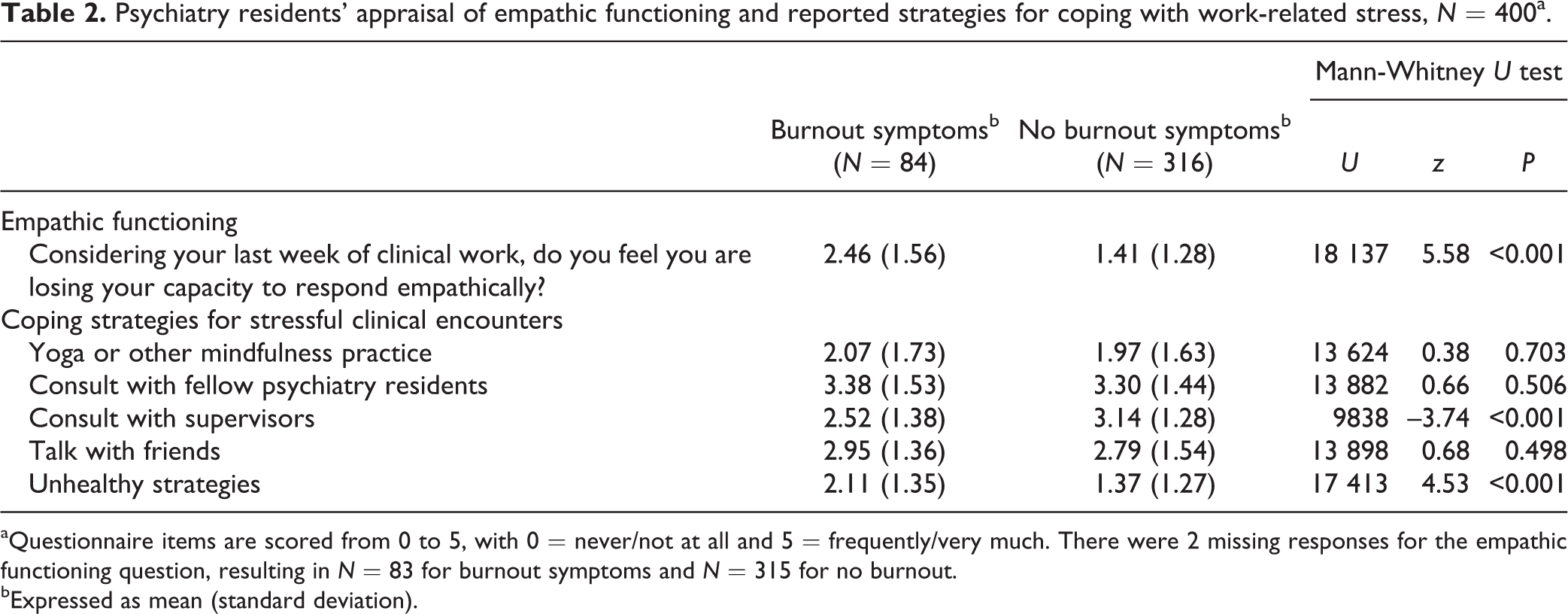
aQuestionnaire items are scored from 0 to 5, with 0 = never/not at all and 5 = frequently/very much. There were 2 missing responses for the empathic functioning question, resulting in N = 83 for burnout symptoms and N = 315 for no burnout.
bExpressed as mean (standard deviation).
Discussion
This is the first study to examine the prevalence of burnout symptoms among residents in psychiatry training programs across Canada. The endorsement of burnout symptoms by one-fifth of residents was considerably lower than that reported by U.S. psychiatry residents, 12 although this may be a consequence of methodological differences. The incidence of burnout symptoms revealed by our survey is cause for concern for Canadian psychiatric educators, given the pathway to compromised practice and physician health that burnout signals. Indeed, the residents we surveyed who reported symptoms of burnout rated themselves as having significantly reduced empathic functioning compared with those without symptoms of burnout. Whether this represents an actual decline in clinical competence is impossible to determine from our survey; it is conceivable that residents endorsing burnout may be underestimating their ability to connect with patients. Strategies to prevent burnout and bolster empathic functioning are nevertheless important to implement, particularly given the encouraging evidence for interventions in preventing burnout. 18
It appears optimal to raise the issue of burnout during or prior to PGY-2, since burnout symptoms were most frequently reported at this stage of training. The PGY-2 year requires a significant role and identity transition as residents begin their immersion in psychiatry. This involves the pressure of rapid skill acquisition in assessment, diagnosis, psychopharmacology, and psychotherapy while being exposed for the first time to acutely ill psychiatric patients in emergency, inpatient, and outpatient settings. Including education about burnout over the course of resident training, coupled with information about prevention and self-care, would be a valuable accompaniment to PGY-1 and PGY-2 curricula, to prepare residents for the psychological disruption that may occur in training.
Interestingly, we found a positive association between burnout and personal psychotherapy during residency. Given that we also found a significantly positive impact of personal therapy on residents’ personal lives and professional development in our larger survey—no resident reported a negative impact from personal therapy during residency 15 —it is unlikely that personal therapy contributes directly to burnout. Rather, it may be that psychotherapy, through fostering personal awareness, primes residents to recognize and acknowledge potentially troublesome symptoms. Alternatively, residents who experience burnout may be motivated to pursue personal therapy.
The finding that residents with burnout symptoms were less likely to consult supervisors is concerning, as is the greater likelihood that these residents will use less adaptive coping strategies. Resident-supervisor interactions have tremendous potential in mitigating the development of burnout, given residents’ positive attitudes toward this relationship. 19 Supervisors should consider residents’ reluctance to disclose difficulties due to concerns about anticipated negative evaluation or shame 20 and may need to actively foster trust and acceptance while modelling a level of comfort with mistakes. 21
This study’s limitations must be noted. Despite a favourable response rate, the potential for nonresponse bias cannot be ruled out. Distressed residents—especially those who may have been on leave—may have been less motivated to participate, despite our $1000 raffle incentive. Another limitation concerns our use of a single-item burnout question: Although this has been well-validated to capture emotional exhaustion, our survey may have neglected to include residents with primarily dissociative burnout symptoms. Additionally, the cross-sectional nature of the survey precludes inferences about the directions of associations found in our study. Further research is needed to investigate clinical and personal difficulties associated with burnout among psychiatry residents.
Notwithstanding these limitations, the incidence of burnout symptoms among one-fifth of Canadian psychiatry residents warrants the attention of psychiatric educators, program directors, and residents themselves. Residency is an opportune time to implement prevention, supervisory, and self-care strategies. Doing so at this stage may help reduce vulnerability to burnout among Canada’s future psychiatrists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by the Department of Psychiatry at the University of British Columbia through a start-up grant awarded to Dr. Hadjipavlou.