
Abstract
Introduction:
The epidemiology of attempted suicide has not been well characterized because of lack of national data or an International Classification of Diseases (ICD) code for suicide attempts. We conducted a retrospective chart review in 2 adult general hospitals (tertiary and community) in Montreal, Canada, in 2009-2010 to 1) describe the characteristics of men and women who presented to the emergency department (ED) and/or were hospitalized following a suicide attempt, 2) identify factors associated with attempts requiring hospitalizations, and 3) validate the use of International Classification of Diseases, 10th Revision (ICD-10) codes for “intentional self-harm” as a method to detect suicide attempts from hospital abstract summary records.
Method:
All potential suicide attempts were identified from hospital abstract summary records and ED nursing triage file using ICD-10 codes and keywords suggestive of suicide attempts. All identified charts were examined, and those with confirmed suicide attempts were fully reviewed.
Results:
Of the 5746 identified charts, 369 were fully reviewed. Of these, 176 were for suicide attempters treated in the ED and 193 for hospitalized attempters, of whom 46% had an ICD-10 code for intentional self-harm. Poisoning (46%) was the most frequent method of suicide used. Half of attempters were younger than 34 years, 53% were female, and 75% had a history of mental disorders.
Conclusion:
About half of individuals who seek medical care for attempted suicide are admitted to hospital. About half of attempters use poisoning as a method of suicide, and a quarter do not have a history of mental disorders. Intentional self-harm codes capture only about half of hospitalized attempters.
Clinical Implications
One-fourth of suicide attempts do not occur in the context of mental health disorder. Further clinical description of this clinical group may be warranted.
Young women and women with children may be a more vulnerable group. Further clinical description of this group may be warranted.
Only half of hospitalized suicide attempts are coded as intentional self-harm. Improved coding will enhance treated suicide attempt data quality.
Limitations
The study is based on chart review; some variables may have been miscoded or missed.
The study was conducted at 2 general hospitals in Montreal. Generalizability to the whole province and to other centres should be done with caution.
The method used for chart selection resulted in a large number of charts, only 7% of which were true suicide attempts; more effective searching strategies should be explored.
Suicide attempts are a major public health problem with enormous emotional and financial burden to individuals, families, society, and the health care system. 1 –7 In Quebec, about 24,000 persons (0.3%) attempt suicide each year. 8 The World Health Organization (WHO) estimates that a prior suicide attempt is the single most important risk factor for suicide in the general population. 9 Additionally, individuals who survive an attempt are 40 to 100 times more likely to reattempt and complete suicide compared to the general population. 10,11 Over 1 million individuals die by suicide worldwide each year. 1,9 In 2009, approximately 3890 Canadians took their own lives; 1146 were from Quebec. 12,13
The epidemiology of attempted suicide has not been well characterized because of lack of national data and International Classification of Diseases (ICD) code for suicide attempts. Published studies addressing the epidemiology of attempted suicide have mostly relied on population surveys or health services administrative databases. 9,12 –19 Survey data are limited by participation and self-report bias, 9,12 as well as inconsistent definitions (or interpretation by survey responders) of suicidal attempts (often including suicidal ideation, planning, and attempts). 14,15 Published studies using health services administrative databases have used the ICD codes for intentional self-harm to identify suicide attempts, although some have also used unintentional poisoning codes. While these databases cover the entire population and have the advantage of large samples and easy to use data, they lack important sociocultural, clinical, and psychiatric information. In addition, codes for self-harm may miss over half of the suicide attempts. 19 –21 Some studies have also used direct data collection or registries to assess suicidal behaviour in adults. These studies have collected detailed sociocultural, clinical, and psychiatric data but have been limited by small sample sizes and/or selected populations such as the adolescents, the elderly, those suffering from mental disorders, and those with a specific occupation. 22 –25
Despite these limitations, studies have found suicidal behaviours to be more frequent among women, younger individuals, those with a lower education and lower income, unmarried and unemployed individuals, those with a family history of suicidal behaviour, and those with psychiatric disorders and history of suicidal behaviours. 3,4,15,19,26 –34 In addition, occupational stress, 25,35 –42 chronic or terminal illness, 43 and lack of social support have also been associated with a higher risk of suicidal behaviour. 44
We conducted a retrospective chart review in 2 adult general hospitals (tertiary and community) in Montreal, Canada, in 2009-2010 to 1) describe the characteristics of men and women who presented to the emergency department (ED) and/or were hospitalized following a suicide attempt, 2) identify factors associated with attempts requiring hospitalizations, and 3) validate the use of International Classification of Diseases, 10th Revision (ICD-10) codes for “intentional self-harm” as a method to detect suicide attempts from hospital abstract summary records.
Methods
Study Design and Sample
This was a cross-sectional study using retrospective chart review. All potential cases of attempted suicide among all individuals who presented to the ED and/or were hospitalized in the study hospitals (1 tertiary trauma McGill university teaching hospital and 1 community hospital affiliated with McGill University) between January 1, 2009, and March 31, 2010, were identified from the hospital abstract summary records and the ED nursing triage file. The study period included a full calendar year (to account for seasonality) and went up to the time of the request for ethics approval.
Study Procedure
Case selection for chart review was done in 2 steps as follows: 1) hospitalized cases were identified from the hospital abstract summary records using ICD-10 codes, and 2) cases treated in the ED were identified from the ED nursing triage file. We did not use ED nursing triage to identify hospitalized patients because individuals who arrive in a critical condition do not go through triage, and some attempts may be missed by the triage nurse.
Case selection for chart review from the hospital abstract summary records involved 1) creating a list of probable ICD-10 codes indicating suspicious injury or behaviour (Table 1) and 2) asking Medical Records to identify patients who received at least 1 ICD-10 code from the list as principal or secondary diagnosis or external cause of hospitalization on their hospital abstract summary record. In addition to the ICD-10 codes for intentional self- harm (X60-X84 and Y87.0), most often used to identify suicide attempts from administrative databases, 19 –21 the list also included “poisoning by drugs, medications and biological substances and toxic effects of substances chiefly nonmedicinal as to source” (T36-T65) 21 and other suspicious injury and behaviour such as neck injury, reaction to severe stress, and adjustment disorders (Table 1). We used a much broader range of codes than that used in the literature to maximize the likelihood of capturing all suicide attempts at the expense of reviewing more negative charts.
International Classification of Diseases, 10th Revision (ICD-10) Codes and Keywords Used for Chart Selection: Number of Chartsa Selected and Number of Cases of Suicide Attemptsb Identified.
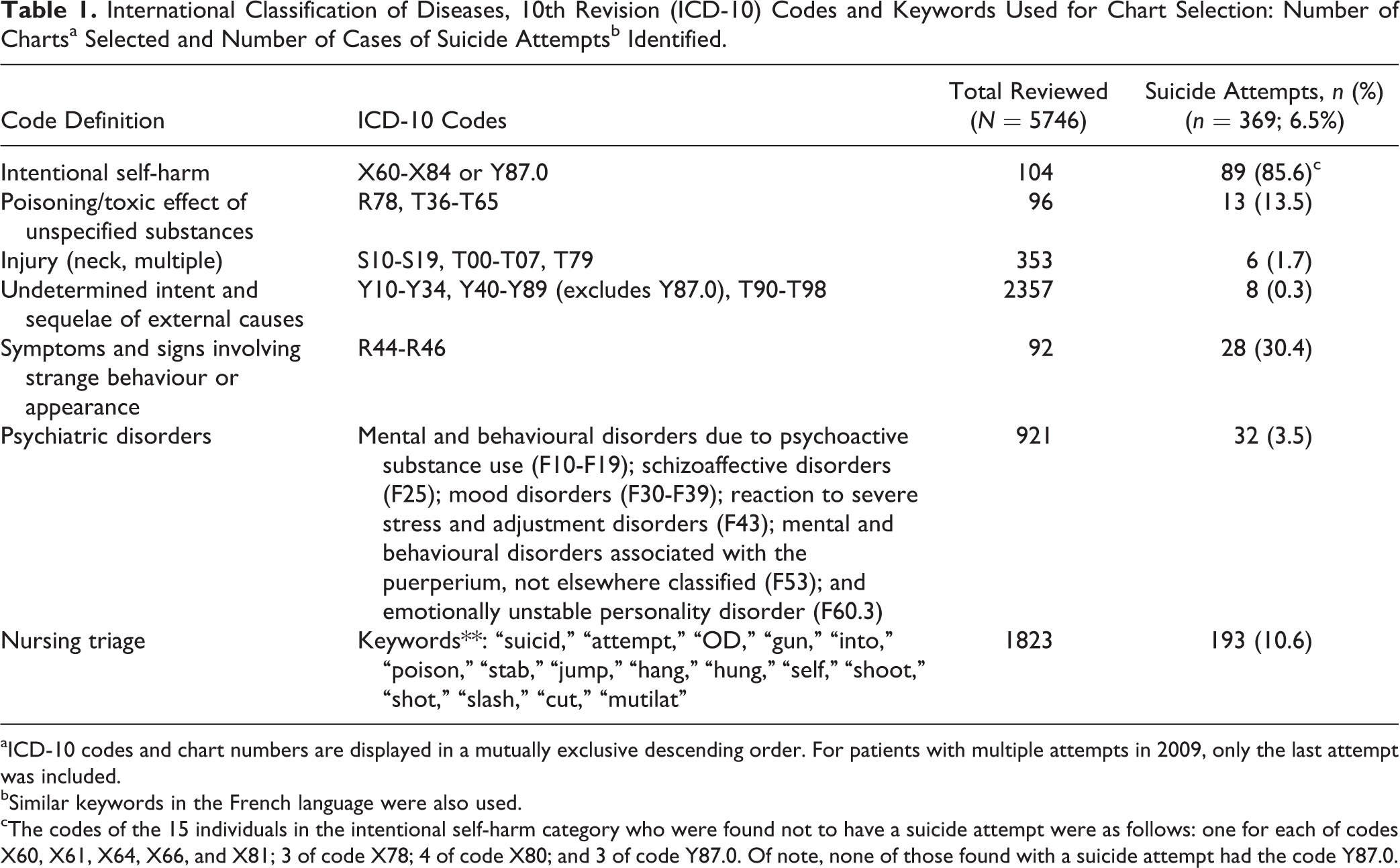
aICD-10 codes and chart numbers are displayed in a mutually exclusive descending order. For patients with multiple attempts in 2009, only the last attempt was included.
bSimilar keywords in the French language were also used.
cThe codes of the 15 individuals in the intentional self-harm category who were found not to have a suicide attempt were as follows: one for each of codes X60, X61, X64, X66, and X81; 3 of code X78; 4 of code X80; and 3 of code Y87.0. Of note, none of those found with a suicide attempt had the code Y87.0.
Case selection for chart review from the ED nursing triage file involved using the electronic ED triage file to identify all patients who had an indication of suicidality or self-harm at ED presentation using keywords selected by 2 nurses, 1 triage and 1 psychiatric, and approved by our team (Table 1).
In all Quebec hospitals, patients who arrive to the ED undergo a triage assessment to determine the priority of their needs. According to ED management guidelines, triage is conducted by an experienced nurse and follows the Canadian Emergency Department Triage and Acuity Scale (CTAS) 45 ; the ED triage nurse is trained to recognize suicidal patients and is present in the ED at all times. A suicide management protocol is followed for the evaluation, treatment, management, and follow-up of suicidal patients. Software accredited by the Ministry of Health is used for ED triage. 46 All triage files and medical records during the study period were searched as described above. If any of the codes were found in the medical record or a keyword found in the triage file, the chart was retrieved.
Chart Review: Identifying Suicide Attempt and Patient Characteristics
Chart review was conducted by 2 physicians and coordinated by a psychiatric nurse. An Access program was used to standardize data entry, and a codebook was created that described all the fields in the Access program and provided guidance for ambiguous situations that the reviewer may have encountered. The reviewer was encouraged to consult with the psychiatric nurse and report the case to the team at any time. The first 5 cases identified were discussed by the reviewers and authors who agreed on an objective suicide attempt definition: an explicit documentation of attempted suicide recorded by at least 2 different health care professionals during the episode of care (ED visit for those discharged from the ED or hospitalization for those admitted to hospital). Subsequent charts were reviewed by both the psychiatric nurse and the reviewers, and the first 10 cases identified were audited by our team. Complete agreement on suicide attempt identification was found. In addition, 30 cases reviewed by one of the reviewers were selected at random and reviewed by the second reviewer independently and recorded variables were compared. Some slight disagreement was found in sociocultural variables such as education, employment, and ethnicity. As these variables were grouped into categories in this study, these differences disappeared. For example, a student working part time was recorded as “student” by 1 reviewer and “employed part time” by the second in the variable “working status.” However, in the current study, we categorized this variable into “unemployed” (yes/no), which was in perfect agreement between reviewers.
Variables collected from each chart reviewed included sociodemographic and sociocultural factors (age, sex, employment status, education level attained, presence of social support, country of birth, family history of mental disorders, family history of suicidal behaviour), time of suicide attempt (January-April, May-August, September-December), suicide methods used in the attempt (poisoning, laceration, injury [collision, jump, fire burns, and firearm], hanging/strangulation, and other), history of mental disorders (major depressive episode, bipolar disorder, schizophrenia, panic disorder, generalized anxiety disorder, antisocial personality disorder, borderline personality disorder, alcohol/drug abuse), previous suicide attempts, comorbidities (grouped by the order of most frequent: cardiovascular, cancer, respiratory, chronic pain, and others as recorded in the chart), number of days in-hospital, and mortality during that episode of care. Ethics approval from the Ethics Boards of the study hospitals and permission from the Director of Professional Services (DPS) were obtained for the triage assessment and chart review. Patient informed consent is not required for retrospective chart review and was not sought.
Statistical Analyses
Descriptive statistics (means, medians, and proportions as appropriate) were used to summarize patient characteristics at ED presentation. Characteristics were assessed by sex and admission to hospital. Logistic regression models were used to compare patient characteristics between hospital type (tertiary and community). Separate logistic regression models were also used to compare patient characteristics between men and women and between those treated in the ED and those admitted to hospital. Logistic regression models were also used to identify factors associated with attempting suicide requiring shorter (≤8 days) and longer (>8 days) hospital stays versus not hospitalized. Patient characteristics listed above were considered in the models if statistically significant in the univariate analyses at the 25% level (P < 0.25) and were kept in the model if statistically significant at the 5% level (P < 0.05). 47 The Schwarz information criterion was used to select the final models. The main analyses were conducted with missing data imputed using multiple imputation techniques. 48 Secondary analyses were also conducted using complete data. The sensitivity of intentional self-harm codes (X60-X84 or Y87.0) to identify hospitalized suicide attempts was calculated as the proportion of those with a code for intentional self-harm among those hospitalized. The positive predictive value (PPV) of intentional self-harm was defined as the proportion of individuals with hospitalized suicide attempts among those with a code for intentional self-harm. All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC) for Linux.
Results
A total of 5746 charts were retrieved (3923 patients were identified from the hospital abstract summary records and an additional 1823 patients by the triage file). In total, 369 patients with suicide attempts were identified. Table 1 displays the number of suicide attempts identified through each of the ICD-10 categories used as well as those identified exclusively through the nursing triage file. Among the 193 patients exclusively identified by the triage file (i.e., no ICD-10 codes from our list), 17 were considered as admitted to hospital (explicit indication for admission was present for 2 patients admitted to the intensive care unit, 2 to the medical ward, and 4 to the psychiatric ward; the additional 9 patients did not have an explicit indication for admission, but their hospital stay was between 3 and 6 days). Therefore, 193 study patients were hospitalized and 176 were treated in the ED.
The sensitivity of intentional self-harm (ICD-10 codes X60-X84 or Y87.0) in detecting cases of hospitalized suicide attempts was poor (46%; 89/193) while its PPV was high (86%; 89/104) (Table 1).
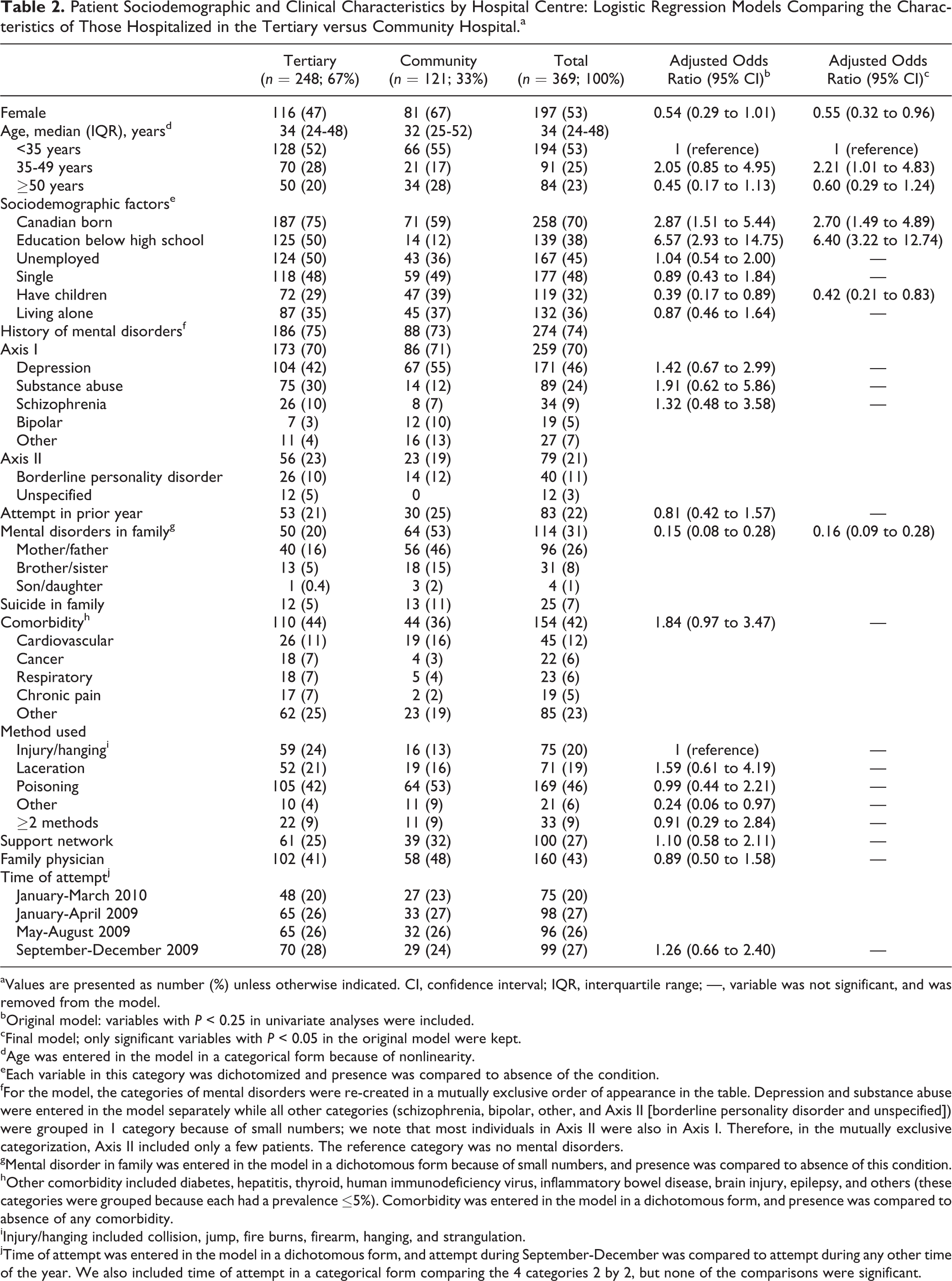
Poisoning was the most frequent method used by study patients. Of study patients, about half were males, three-fourths were younger than 48 years, three-fourths had a history of mental disorder, and a third had a mental disorder in the family, mostly in the mother. In terms of sociocultural characteristics, over a third of study patients did not complete high school, almost half were unemployed, a third had children, less than a third had a supporting family/social network, and only about half had a family physician (Table 2).
Patient Sociodemographic and Clinical Characteristics by Hospital Centre: Logistic Regression Models Comparing the Characteristics of Those Hospitalized in the Tertiary versus Community Hospital.a
aValues are presented as number (%) unless otherwise indicated. CI, confidence interval; IQR, interquartile range; —, variable was not significant, and was removed from the model.
bOriginal model: variables with P < 0.25 in univariate analyses were included.
cFinal model; only significant variables with P < 0.05 in the original model were kept.
dAge was entered in the model in a categorical form because of nonlinearity.
eEach variable in this category was dichotomized and presence was compared to absence of the condition.
fFor the model, the categories of mental disorders were re-created in a mutually exclusive order of appearance in the table. Depression and substance abuse were entered in the model separately while all other categories (schizophrenia, bipolar, other, and Axis II [borderline personality disorder and unspecified]) were grouped in 1 category because of small numbers; we note that most individuals in Axis II were also in Axis I. Therefore, in the mutually exclusive categorization, Axis II included only a few patients. The reference category was no mental disorders.
gMental disorder in family was entered in the model in a dichotomous form because of small numbers, and presence was compared to absence of this condition.
hOther comorbidity included diabetes, hepatitis, thyroid, human immunodeficiency virus, inflammatory bowel disease, brain injury, epilepsy, and others (these categories were grouped because each had a prevalence ≤5%). Comorbidity was entered in the model in a dichotomous form, and presence was compared to absence of any comorbidity.
iInjury/hanging included collision, jump, fire burns, firearm, hanging, and strangulation.
jTime of attempt was entered in the model in a dichotomous form, and attempt during September-December was compared to attempt during any other time of the year. We also included time of attempt in a categorical form comparing the 4 categories 2 by 2, but none of the comparisons were significant.
Patient characteristics of suicide attempters differed by study hospital type (Table 2). Individuals aged 35 to 49 years (but not over 50 years) compared to those younger than 35 years were more likely to be hospitalized in the tertiary centre. Those born in a foreign country and those who did not finish high school were also more likely to be hospitalized in the tertiary centre, while those who had children and those who had a family history of mental disorders were less likely (Table 2).
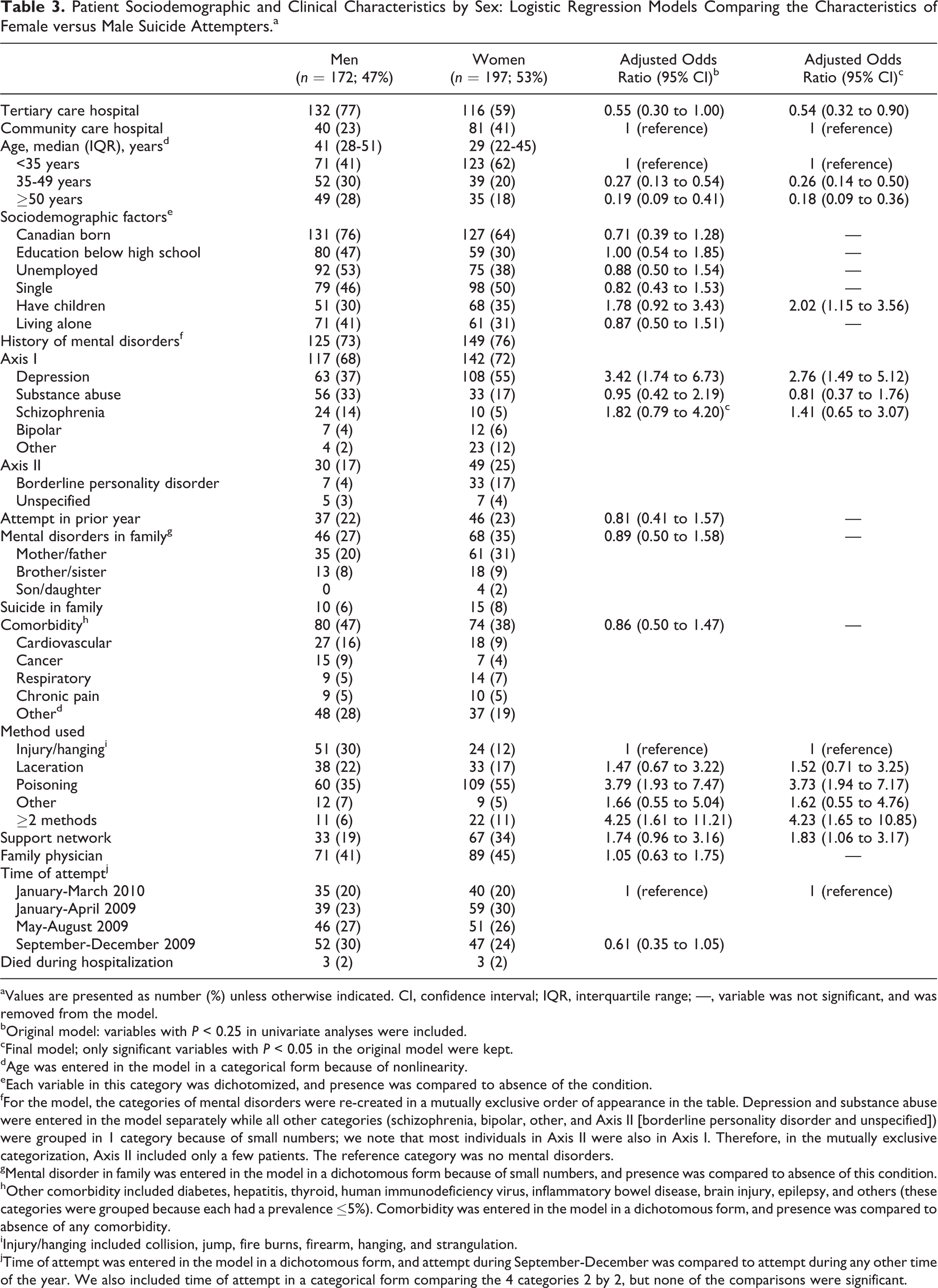
Women were younger than men, less likely to be hospitalized in the tertiary versus community hospital, about 3 times more likely to have depression, about 4 times more likely to have used poisoning or 2 methods concomitantly versus injury (collision, jump, fire burns, and firearm) or hanging/strangulation, nearly 2-fold more likely to have a family/social support network, and 2-fold more likely to have children (Table 3).
Patient Sociodemographic and Clinical Characteristics by Sex: Logistic Regression Models Comparing the Characteristics of Female versus Male Suicide Attempters.a
aValues are presented as number (%) unless otherwise indicated. CI, confidence interval; IQR, interquartile range; —, variable was not significant, and was removed from the model.
bOriginal model: variables with P < 0.25 in univariate analyses were included.
cFinal model; only significant variables with P < 0.05 in the original model were kept.
dAge was entered in the model in a categorical form because of nonlinearity.
eEach variable in this category was dichotomized, and presence was compared to absence of the condition.
fFor the model, the categories of mental disorders were re-created in a mutually exclusive order of appearance in the table. Depression and substance abuse were entered in the model separately while all other categories (schizophrenia, bipolar, other, and Axis II [borderline personality disorder and unspecified]) were grouped in 1 category because of small numbers; we note that most individuals in Axis II were also in Axis I. Therefore, in the mutually exclusive categorization, Axis II included only a few patients. The reference category was no mental disorders.
gMental disorder in family was entered in the model in a dichotomous form because of small numbers, and presence was compared to absence of this condition.
hOther comorbidity included diabetes, hepatitis, thyroid, human immunodeficiency virus, inflammatory bowel disease, brain injury, epilepsy, and others (these categories were grouped because each had a prevalence ≤5%). Comorbidity was entered in the model in a dichotomous form, and presence was compared to absence of any comorbidity.
iInjury/hanging included collision, jump, fire burns, firearm, hanging, and strangulation.
jTime of attempt was entered in the model in a dichotomous form, and attempt during September-December was compared to attempt during any other time of the year. We also included time of attempt in a categorical form comparing the 4 categories 2 by 2, but none of the comparisons were significant.
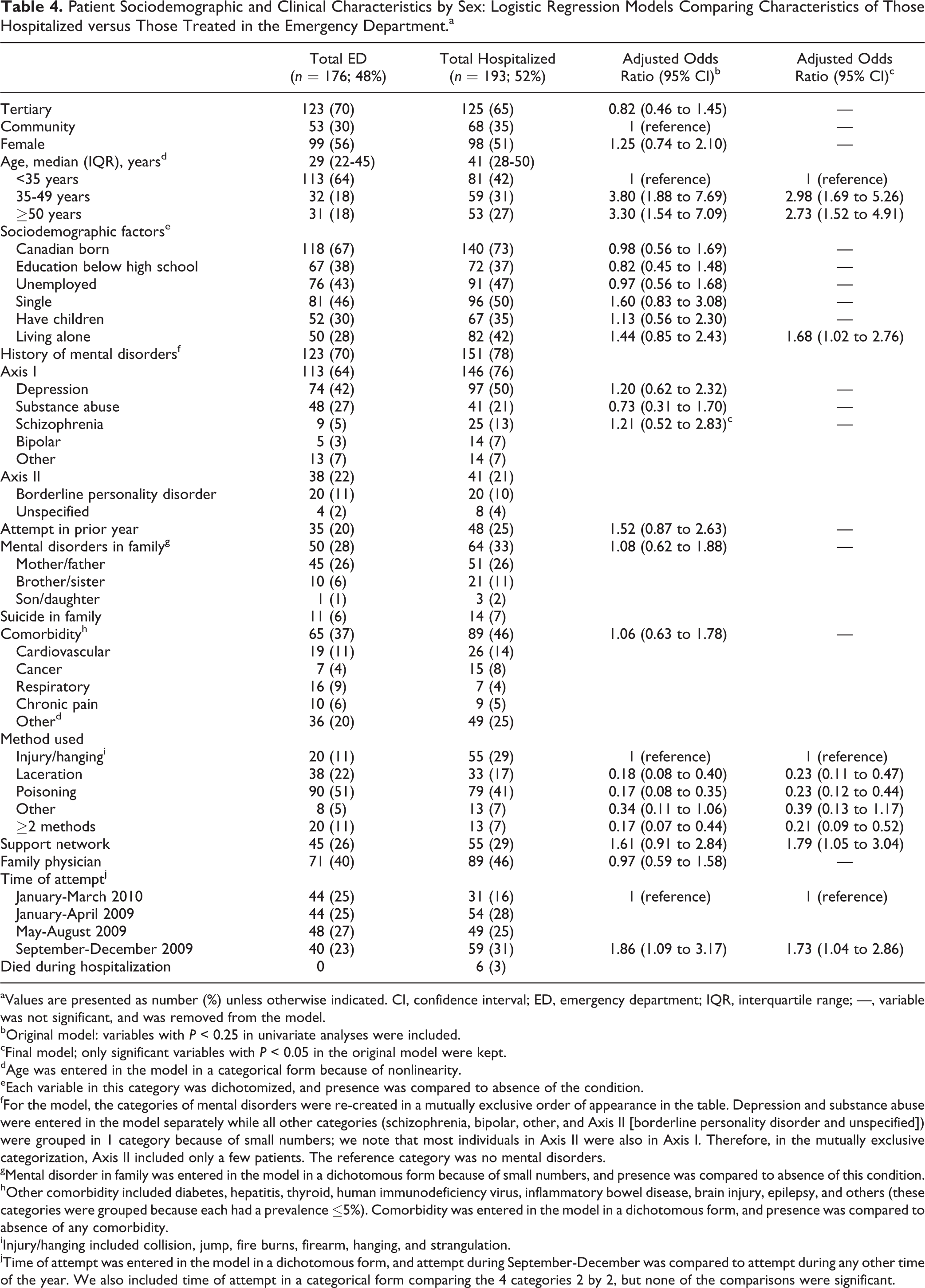
Hospitalized patients were older than those treated in the ED, more likely to have attempted suicide in September to December compared to other times of the year, and more likely to have used a method classified as injury or hanging (collision, jump, fire burns, firearm, hanging, or strangulation). Hospitalized patients were also more likely to be living alone and to have a family/social supporting network (Table 4). Overall, a quarter of attempters were hospitalized for over 8 days (median days, 2; interquartile range [IQR], 1-8). Longer hospitalizations were more likely in older individuals and more likely among those who used injury or hanging as a method in the suicide attempt (data not shown).
Patient Sociodemographic and Clinical Characteristics by Sex: Logistic Regression Models Comparing Characteristics of Those Hospitalized versus Those Treated in the Emergency Department.a
aValues are presented as number (%) unless otherwise indicated. CI, confidence interval; ED, emergency department; IQR, interquartile range; —, variable was not significant, and was removed from the model.
bOriginal model: variables with P < 0.25 in univariate analyses were included.
cFinal model; only significant variables with P < 0.05 in the original model were kept.
dAge was entered in the model in a categorical form because of nonlinearity.
eEach variable in this category was dichotomized, and presence was compared to absence of the condition.
fFor the model, the categories of mental disorders were re-created in a mutually exclusive order of appearance in the table. Depression and substance abuse were entered in the model separately while all other categories (schizophrenia, bipolar, other, and Axis II [borderline personality disorder and unspecified]) were grouped in 1 category because of small numbers; we note that most individuals in Axis II were also in Axis I. Therefore, in the mutually exclusive categorization, Axis II included only a few patients. The reference category was no mental disorders.
gMental disorder in family was entered in the model in a dichotomous form because of small numbers, and presence was compared to absence of this condition.
hOther comorbidity included diabetes, hepatitis, thyroid, human immunodeficiency virus, inflammatory bowel disease, brain injury, epilepsy, and others (these categories were grouped because each had a prevalence ≤5%). Comorbidity was entered in the model in a dichotomous form, and presence was compared to absence of any comorbidity.
iInjury/hanging included collision, jump, fire burns, firearm, hanging, and strangulation.
jTime of attempt was entered in the model in a dichotomous form, and attempt during September-December was compared to attempt during any other time of the year. We also included time of attempt in a categorical form comparing the 4 categories 2 by 2, but none of the comparisons were significant.
The proportion of patients with missing data was low (less than 5%) for most key variables. In secondary analyses, models with complete data showed similar results (data not shown).
Discussion
Our study was designed to include all individuals who attempted suicide and presented to the ED and/or were admitted at 2 general hospitals (1 tertiary trauma hospital and 1 community hospital) affiliated with McGill University in 2009-2010. A relatively large number of suicide attempters was found (n = 369), 52% of whom were hospitalized and 48% were treated in the ED. The proportion of hospitalized patients in our study was lower than that reported in a study conducted in Alberta in 1998-2000 based on data from the Ambulatory Care Classification System (64%) of individuals discharged from the ED among those presenting with a self-inflicted injury. 19 Differences in suicide attempt identification method and data used may explain this difference in proportions.
Published studies addressing the epidemiology of attempted suicide using national and international surveys found suicide attempts to be more frequent in women and in those with younger age, lower education, and lower income; those who were unmarried and unemployed; and those with psychiatric disorders, family history of mental disorders, and history of suicidal behaviours. 9,12 –15 While our study did not include a control group and cannot be directly compared to population-based survey studies, it did find higher proportions of individuals with similar risk factors, and as reported by published studies, our study patients were mostly young and most frequently used poisoning as the method of suicide attempt.
In our study, women attempters were younger than men, and more had a history of depression. More women than men used poisoning as the method of suicide, more had children, and more had a family/social support network. A study conducted in Ontario in 2001-2002 among individuals 12 years and older using data from the National Ambulatory Care Reporting System also found age differences between men and women who presented to the ED with medicinal self-poisoning. 49 Another study conducted in Alberta using the Ambulatory Care Classification System in 1998-2000 found higher rates of self-inflicted injury in females and in younger patients. As in our study, poisoning was the most frequent method of suicide used, and males were more likely to use more lethal methods. The rate of self-inflicted injury was lowest from November to February in that study, while in our study, such seasonal differences were not detected. 19 However, we did observe higher rates of hospitalizations for suicide attempts during the period from September to December compared to the rest of the year.
Our study used both Medical Records and ED triage files to identify suicide attempts. It showed that the use of the ED triage file to identify those treated in the ED is a good strategy to capture most suicide attempts. In Quebec, triage nurses are trained to recognize suicidal cases, and an ED suicidal patient management protocol is in place in all hospitals. 46 Our study also showed that patient charts are a good source of suicide attempts data because attempters who present to the ED receive a comprehensive suicide evaluation and a detailed psychiatric evaluation that are recorded in the chart; missing data were minimal, not exceeding 5% for most key variables. However, our study required the review of a large number of charts (5746) to identify 369 suicide attempts. Although both identification strategies (hospital abstract summary data and nursing triage file) were necessary for our study, future efforts should be deployed to refine our list of codes and construct a more efficient algorithm for suicide attempt identification. In fact, of the 369 suicide attempts found in our study, only 281 were found by the triage method. Possible reasons for missing 81 hospitalized suicide attempts by the triage method include the following: patient critical condition on arrival, absence of explicit signs of suicidal behaviour, or missing important keywords in our triage selection list. Gaps in the coordination between specialists in mental health, addiction, and ED services have been identified in almost half of suicide cases in 1 Canadian province and may be a reason why suicide attempt was not recorded as such in the triage file for some complex patients. 50 In addition, our study demonstrates that intentional self-harm records cannot be solely used to detect hospitalized suicide attempts. Indeed, while the PPV of these codes was high at 86%, their sensitivity was poor at 48%. Therefore, cases of suicide attempts identified from hospital abstract databases using diagnoses for intentional self-harm are likely to be true cases, but they are not representative of all suicide attempts. One Canadian study of hospital databases confirmed good reliability of the self-injury codes when present 20 and found that 63% of deliberate self-poisonings identified in medical chart review were also identified by the self-harm codes. 20 A literature review of studies conducted in the United States and Canada reported a wide range for the sensitivity (14% to 65%) and PPV (4% to 100%) for international self-harm codes. 51 Some studies have used additional codes to those for self-harm to identify suicide attempts from administrative databases. One such study conducted in Ontario demonstrated an added value for the use of the codes for injury with undetermined intention, 18 while a study conducted in Manitoba used the following ICD-10 (and corresponding ICD-9) codes: T39, T40, T42.3, T42.4, T42.7, T43, T50.9, T58, Y10 to Y12, and Y16 to Y17, in addition to the codes for self-harm. On examination of our data, 66 charts were identified by these additional codes in our study, among which 37 were suicide attempts (24/37 were also detected by the self-harm codes). 21
Surveillance data published by the Canadian Institute of Health Information (CIHI) based on ICD codes for intentional self-harm reveal that in 2013, population rates of suicide attempts were between 50 and 85 per 100,000 inhabitants—a fourth of what is usually reported in surveys. 52 However, in our study, the majority of hospitalized cases of suicide attempts did not receive codes for intentional self-harm, and about half of suicide attempters who presented to the ED were not hospitalized. Our case findings imply that the true rates of suicide attempts may be 3-fold higher than the figures published by CIHI but remain lower than the 0.3% figure reported in surveys. 8 Discrepancy between our study finding and survey figures may be explained by the number of individuals who attempt suicide but do not seek medical help and by those survey responders who confuse suicide attempts with suicide ideations.
The strengths of our study include the inclusion of all patients who attempted suicide and were treated in 2 general hospitals (tertiary trauma hospital and community hospital). The study provided comprehensive information on adult men and women for a range of sociodemographic characteristics and suicide risk factors, such as methods of suicide used and personal and family history of mental disorders. The use of a systematic method based on electronic files and a much broader range of ICD-10 codes than previously used in the literature, complemented by keywords applied to the triage file, reduced the likelihood of selection and related reporting bias in our study. In our study, we used data from Medical Records that are regularly submitted to the provincial administrative database holder. Therefore, the reported sensitivity and PPV of the “intentional self-harm” code highlight the limitations of studies of suicide attempts relying on such data and codes alone. The relatively large cohort that we assembled allowed robust comparisons of characteristics of men and women and of those hospitalized (vs. discharged from ED), which has rarely been examined and is also a strength. The inclusion in our study of patients treated in 2 general hospitals of different missions (a trauma tertiary care centre and a community centre) provided the possibility for data comparison between these 2 types of hospitals and possible insight concerning differences found in the literature in single-centre studies.
Our study has also some limitations. Although our search strategy aimed to capture all suicide attempts treated at the study hospitals during the study period, some cases of suicide attempts may have been missed because they did not receive one of the selected ICD-10 codes or one of the keywords used in the triage file. Second, data obtained from hospital paper-based chart review may suffer from missing information. However, missing information in this study was limited to less than 5% for most key variables and did not affect the final results as shown in secondary analyses that used complete data to address this issue. Third, our study was conducted at 2 hospitals in Montreal. Although it is reasonable to believe that patient charts do not differ greatly between these hospitals and the remaining hospitals in Quebec of the same missions, this assumption cannot be verified. Fourth, the definition of a suicide attempt in our study required 2 notes indicating “suicide” from 2 different health professionals. Two notes were thought to limit the risk of false positives because patients who self-injure and are agitated on ED presentation may receive a note for a suicide attempt, although they had never intended to kill themselves. Since it is required that all suicide attempters get a psychiatric and suicide risk assessment, we believe that suicide attempters had a wide opportunity to receive a second note in the chart indicating a suicide attempt (by the social worker, psychiatrist, or other health professional). We acknowledge that some suicide attempts may have received only 1 note indicating suicide and may have been missed by our definition. Future studies should compare the 2 suicide definitions (2 vs. 1 note for suicide attempt). Finally, as previously mentioned, we had to review a large number of charts to identify study individuals. Better case identification from administrative databases would enhance our ability to assess the quality of suicide management and risk of recurrence that requires case audit and health services utilisation assessments. 53,54
In conclusion, our study showed that about half of individuals who seek medical care for attempted suicide are admitted to hospital. About half of attempters use poisoning as a method of suicide, and a quarter do not have a history of mental disorders. Our study also showed that intentional self-harm codes capture only about half of hospitalized attempters. Our study highlights the value of nursing triage systems to identify cases of suicide attempters not captured by the currently available Canadian surveillance system because either patients are not admitted or because the ICD codes of intentional self-harm are not recorded. If such nursing triage systems in place in most hospitals could be linked to the other provincial hospital health record systems, this would allow better surveillance and quality monitoring of care for suicide attempters.
Footnotes
Acknowledgment
The authors thank Jivko Jelev, MD, and Elena Molchynska, MD, for chart review and data collection, as well as Angelina Perillo and Helene Racine for their contribution to the questionnaire used in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Quebec Network on Suicide, Mood Disorders and Related Disorders (RQSHA).