
Abstract
Objective:
Medical residency programs are traditionally known for long working hours, which can be associated with a poor quality of sleep and daytime sleepiness. However, few studies have focused on this theme. Our objective was to investigate sleep quality, daytime sleepiness, and their relation with anxiety, social phobia, and depressive symptoms.
Methods:
This cross-sectional observational study involved 59 psychiatry residents. The Pittsburgh Sleep Quality Index (PSQI) and the Epworth Sleepiness Scale (ESS) were used to measure the quality of sleep and excessive daytime sleepiness ([EDS] and ESS > 10), respectively.
Results:
Among the 59 psychiatry residents, 59.3% had poor sleep quality (PSQI > 5) and 28.8% had EDS. Poor sleep quality was associated with higher EDS (P = 0.03) and the year of residency program (P = 0.03). Only 20% of residents with poor sleep had consulted at least once for sleep problems; 54.2% had used medications for sleep; and 16.9% were using medications at the time of interview. Only 30% obtained medication during medical consultations. Poor sleep was associated with irregular sleep hours (P = 0.001) and long periods lying down without sleep (P = 0.03). Poor sleep quality was also associated with high scores of anxiety symptoms (P < 0.001) and social phobia symptoms (P = 0.02).
Conclusion:
Psychiatry residents frequently have poor sleep quality and EDS. Considering that sleep disorders can affect quality of life, predispose to metabolic syndrome, and be associated with worse performance at work, attention to this clinical problem is needed.
Occupations associated with great demand and stress or with night or alternating shifts are commonly associated with an increased risk for sleep disorders. 1,2 Since college, medical students are subjected to a stressful routine. They establish arduous study schemes to achieve an appropriate academic performance. Beyond the curricular activities, which require great effort, many of them submit to several other activities to improve their training, such as courses, academic leagues, tutoring, research projects, and internships. These activities contribute to increased stress levels and result in irregular working hours. 3
Medical residency programs are traditionally known for long work hours. In the 1990s, residents of surgical specialties used to devote more than 100 hours per week to specialization courses. 4 This was associated with symptoms of fatigue, daytime sleepiness, anxiety, depression, and burnout syndrome. 5,6 It is reasonable to say that sleep quality and daytime sleepiness in medical residents has profound implications for their health and for the care of their patients.
In this context, several organizations began pressuring educational institutions to limit working hours for the purpose of providing a better quality of life for residents and indirect benefits for patients. 7,8 Although residents of many medical specialties have been well studied about the quality of sleep and its repercussions, psychiatry residency does not have consistent studies on the subject.
Psychiatry residency programs vary widely around the world. In Brazil, where this study was conducted, its duration is 3 years, with a workload of 60 hours per week. It is recommended that a minimum of 10% of time dedicated to theoretical activities; and 80% to 90% for practical training. The first year of residence consists mainly of service training in general psychiatry (clinics and wards). The second and third year focus on more specialized services. There is an optional fourth year for residents who want to specialize in 4 areas: child and adolescent psychiatry, geriatric psychiatry, psychotherapy, or forensic psychiatry. This differs from other residency programs, such as Canada, where its duration is 5 years. The residents also receive a scholarship, with a lower value compared with other countries, about US$1100 monthly. In our institutions, residents in first or second year of residency are on call 12 hours every 2 weeks. In the third and fourth year of residence, they are not on call in the residence.
Our study aims to investigate sleep quality and daytime sleepiness and their relation with anxiety, social phobia, and depressive symptoms.
Methods
This cross-sectional study was conducted from December 2013 to July 2014. Psychiatry residents were informed about the study. Participation was voluntary and all participants signed an informed consent form. Questionnaires and self-administered scales were applied.
All psychiatry residents (n = 62) of 4 institutions located in Northeastern Brazil were invited to participate in the study. One refused to sign the informed consent, 2 could not be contacted, and 59 participated in the study. Therefore, the response rate was high (95.2%). Eligibility criteria included admission to a residency program for at least a month. Vacation or licenses due to illness in the last month were exclusion criteria.
A structured questionnaire with sociodemographic and professional information was created. It contained information on sex, age, marital status, number of children, and year of medical residency. In addition, the questionnaire contained specific questions about sleep, such as medical consultations about sleep problems, use of hypnotics, and sleep hygiene habits.
Regarding sleep hygiene, residents determined the frequency of the following habits: irregularity of sleep times, use of bedroom as a study or recreation place, use of television or computer before bed, physical activity at night, excessive nighttime eating, nighttime use of stimulant drinks, and staying for long periods lying down without sleep. Each was classified into 2 categories: frequent and rare or occasional.
The Pittsburgh Sleep Quality Index (PSQI) and Epworth Sleepiness Scale (ESS) were used to measure quality of sleep and excessive daytime sleepiness (EDS), respectively.
The PSQI consists of 24 questions. They are divided into 7 categories: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disorders, use of sleep medication, and daytime dysfunction. Each one is scored as follows: 0 (very good), 1 (good), 2 (poor), to 3 (very bad). The sum of scores varies between 0 and 21 and determines the PSQI. A score higher than 5 suggests a poor quality of sleep.
The ESS scores from 0 to 3 the probability of falling asleep in 8 everyday situations. The sum of scores equal to or greater than 10 reflects EDS.
Further, the Beck Depression Inventory-II (BDI-II), the Beck Anxiety Inventory (BAI), and the Social Phobia Inventory (SPIN) were used to evaluate depressive, anxious, and social phobia symptoms, respectively. In our study, the following cut-off scores were used: 7 for BAI; 10 for BDI-II; and 19 for SPIN.
We performed a descriptive analysis to assess the sleep of residents. The mean score of the PSQI and the ESS were calculated. Comparisons between sleep quality and characteristics and habits of residents were carried out using the Fisher exact test. Statistical significance was considered a P value of less than 0.05. All the statistical analyses were performed using the SPSS version 17.0 program package (IBM SPSS Inc, Armonk, NY).
The research was approved by a local Ethics Committee and authorized by the institutions where it was performed.
Results
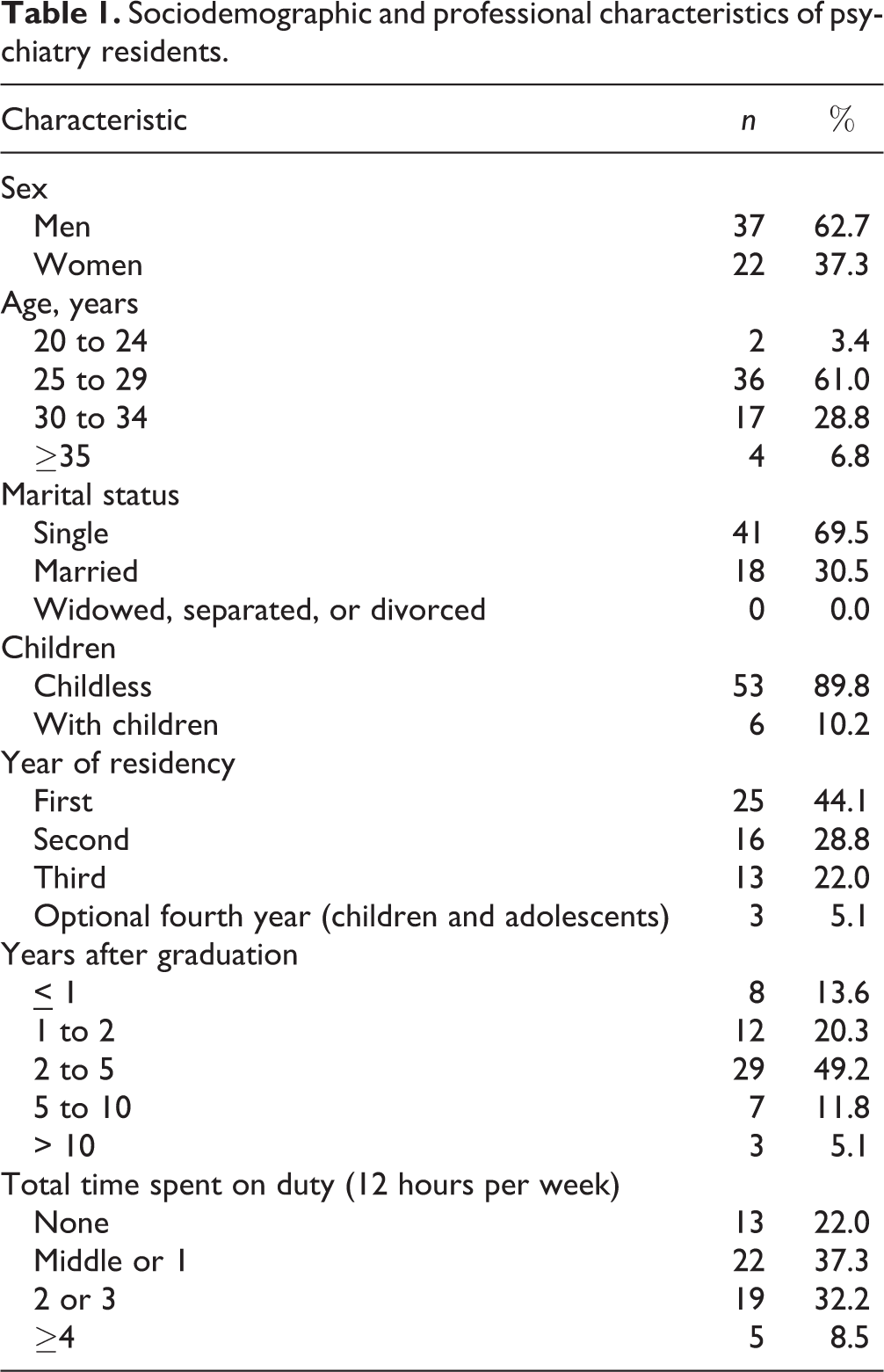
Table 1 shows the sociodemographic and professional profile of residents. Most were male (61.4%), single (68.4%), and childless (89.5%). Most of them had less than 5 years after graduation (81.3%) and were less than 2 times on duty per week (59.3%).
Sociodemographic and professional characteristics of psychiatry residents.
Sleep Quality
Table 2 presents sleep patterns of psychiatry residents. Among the 59 residents, 35 of them (59.3%) had a poor quality of sleep, as per the PSQI. According to the ESS, 17 residents (28.8%) had EDS. An association between poor sleep quality and EDS (P = 0.03) was observed.
Sleep patterns of psychiatry residents.
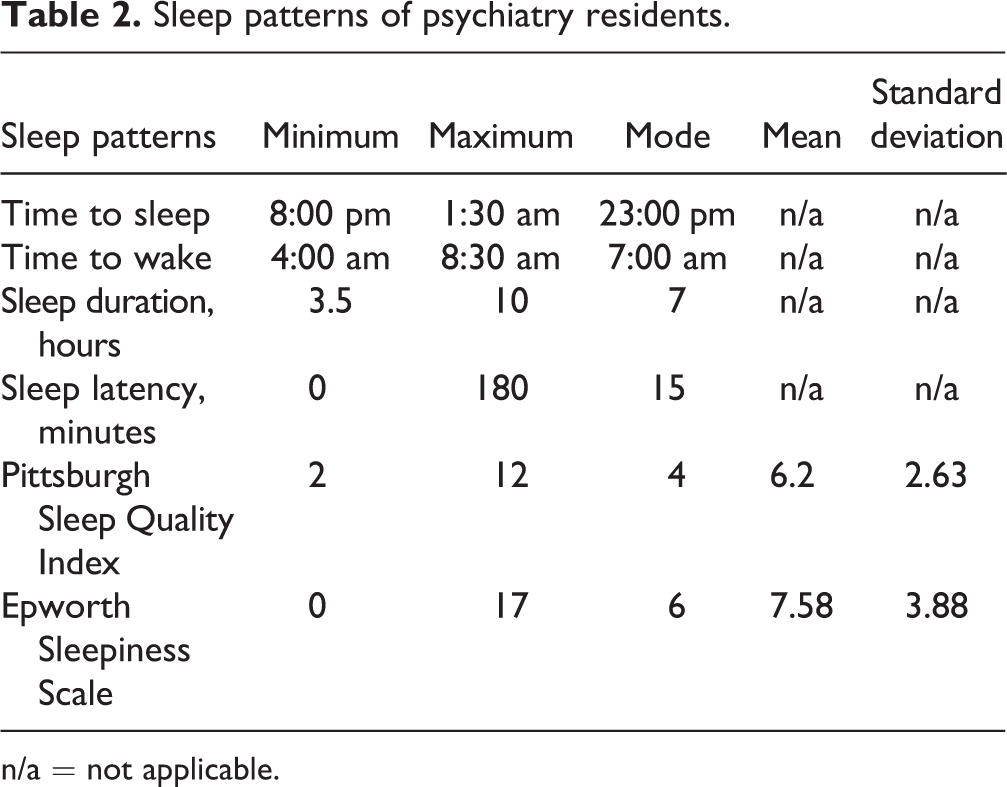
n/a = not applicable.
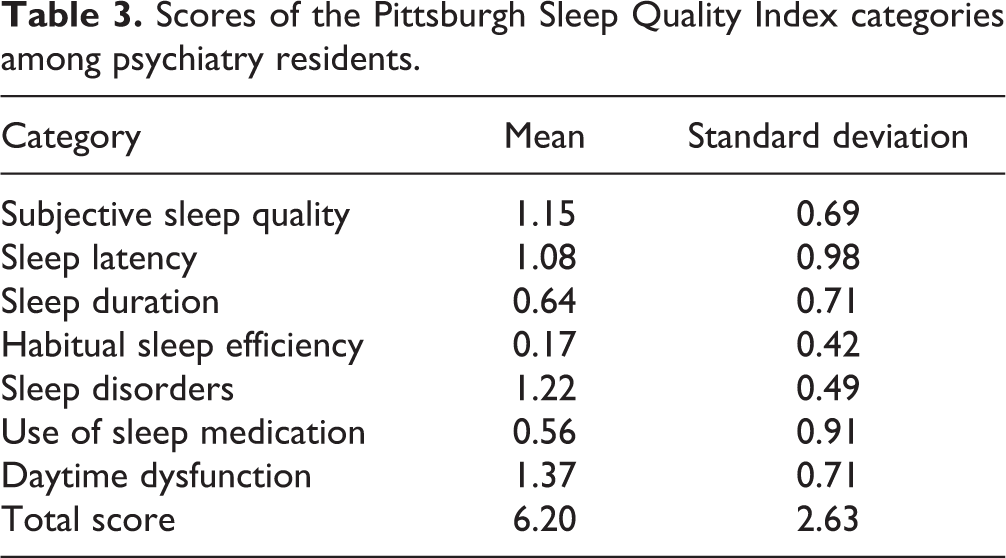
Table 3 displays scores of the 7 categories of the PSQI. Areas with higher scores were daytime dysfunction (1.37), sleep disorders (1.22), and subjective sleep quality (1.15).
Scores of the Pittsburgh Sleep Quality Index categories among psychiatry residents.
Residents in their third year had worse sleep quality than first and second year residents (P = 0.03). Poor quality of sleep was not associated with sex (P = 0.59), age (P = 0.56), marital status (P = 0.39), time after graduation (P = 0.53), total time spent on duty (P = 0.53), and residence performance (P = 0.76).
Poor sleep quality was associated with anxiety symptoms (P < 0.001) and social phobia (P = 0.02), but not with depressive symptoms (P = 0.17).
Searching for Medical Care and Treatment
Among psychiatry residents, 32 (54.2%) had used sleeping medications, and 10 (16.9%) were on use at the time of the interview. Among residents in use of these medications, 30% obtained them in medical consultations, and 70% practiced self-medication. Ninety per cent had a poor quality of sleep. Specific reported medications were benzodiazepines (40%), zolpidem (30%), and antidepressants (20%); 10% did not report the type of sedative or hypnotic.
Nine residents (15.3%) reported previous use of medication to stay awake, and 3 (7.3%) still used them at the time of the interview. Only 1 (33.3%) of them admmitted that this medication was prescribed by other physicians, and the other 2 admitted self-medication. Two residents reported current use of psychostimulants and one did not identify the medication in use. One resident reported using both sleep medication as drugs to stay awake.
Considering only the 35 residents with poor sleep, 80% never sought consultation by sleep problems; and 25.7% used medication regularly at the time of the interview.
Sleep Hygiene
Regarding sleep hygiene of the 59 residents, 37.3% did not have regular hours of sleep; 66.1% used the bedroom for study or recreation; 79.7% often used television or a computer before bedtime; 37.3% routinely practiced physical activities in the evening; 33.9% ate excessively at night; 16.9% often ingested stimulant drinks in the evening; and 16.9% reported increased time lying in down in the absence of sleep (Table 2).
Table 4 shows the relation between sleep hygiene and sleep quality. A poor sleep was associated with irregular sleep hours (P = 0.001) and with long periods lying down without sleep (P = 0.03).
Relation between sleep hygiene and sleep quality of residents.
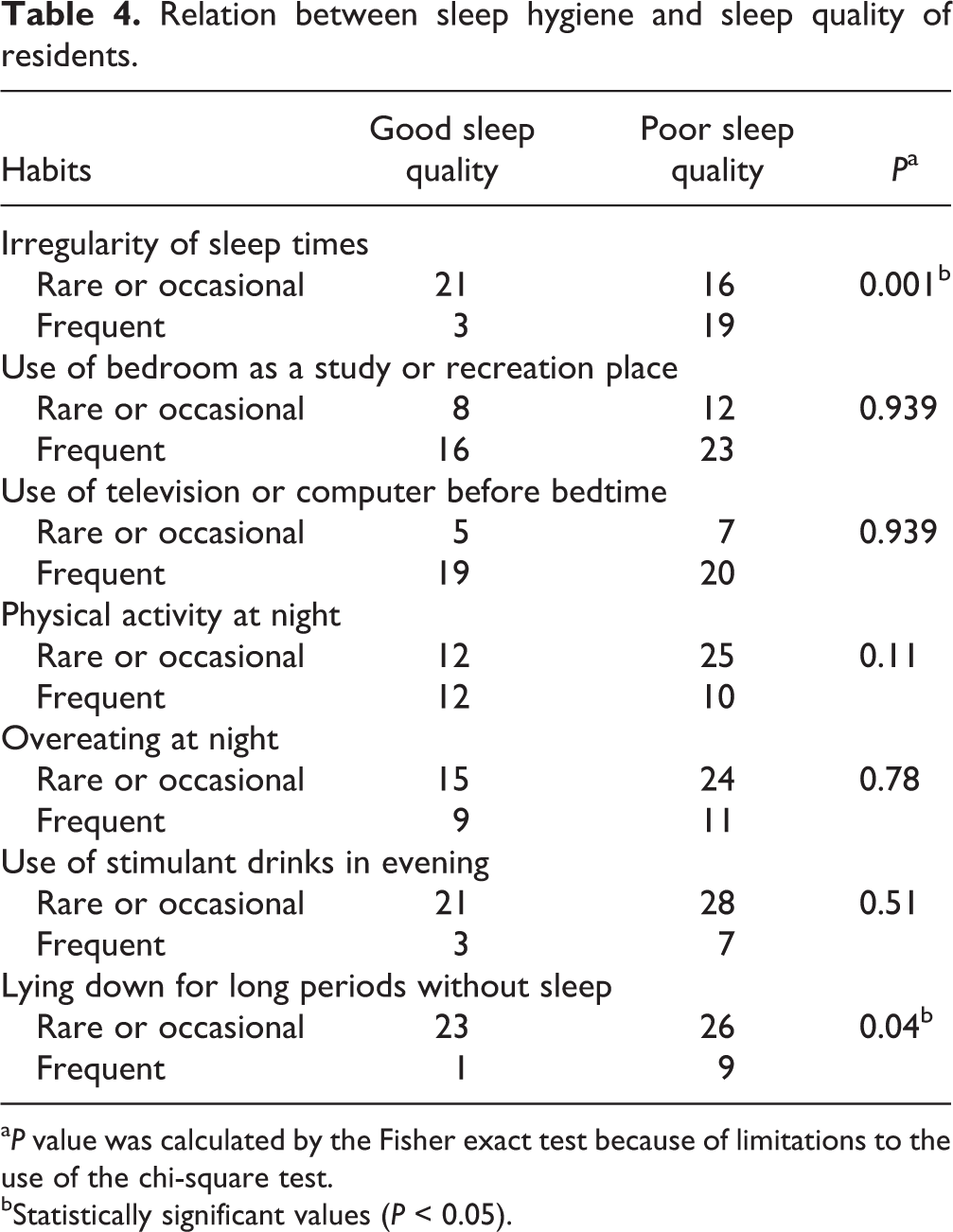
a P value was calculated by the Fisher exact test because of limitations to the use of the chi-square test.
bStatistically significant values (P < 0.05).
Discussion
Ours was the first study evaluating sleep quality and daytime sleepiness specifically in psychiatry residents. Our findings show that poor sleep quality is frequent in this population and associated with anxiety and social phobia symptoms. More importantly, bad sleep hygiene and use of hypnotics were common.
More than one-half of the residents had poor sleep quality; and nearly one-third had, EDS. As can be expected, an association between sleep quality and daytime sleepiness was found. Previous studies indicate that 7% to 30% of medical students are unhappy with their sleep. 9,10 Objective measures show altered sleep in 50.9% and EDS in 30.6% of medical students. 11,12 These values are similar to those found in psychiatry residents.
Interestingly, the third year residents had poorer sleep quality than the first and second. This is in agreement with other studies reporting worsening of sleep quality with time evolution throughout medical school. 3,13 Moreover, sleep quality is found to be worse in residents, than in medical students. Residents seem to accumulate a double stress because at the same time they are physicians (with great professional responsibility) and students, under training. 3 It is largely accepted that psychological stress is closely related to sleep problems. 1,14 This association may be explained by dysregulation of the levels of corticosteroid-induced stress which results in the loss of sleep. 15,16
Our findings show that 80% of psychiatry residents with poor sleep quality never consulted a professional for this reason. It is worrying for the high prevalence of poor sleep quality and for the significant possible impacts related. This highlights the need for awareness about this problem. The potential role of sleep deprivation on metabolic syndrome and cognitive performance are only part of the problem. Sleep disorders are connected to several systemic diseases, such as hypertension, diabetes, obesity, stroke, headaches, chronic pain, infections, and cardiac, respiratory, renal, and urological diseases. More importantly, sleep deprivation is related to mortality by any cause. 17 Further, insomnia is associated with poor academic and occupational performance, increased risk of accidents at work or driving and high public expenses. 18,19
The high use of hypnotics is also noteworthy, especially when one considers that 70% of residents use it without medical consultation. Other studies show a high prevalence of self-medication, including psychoactives. 20,21 The attempt to avoid assuming the sick role, the easy access to drugs, and the pressure to perform at work, contribute to the high rates of self-medication. However, there are various risks, such as increased misdiagnosis, incorrect doses, adverse reactions, and drug interactions, abuse, and dependency. 22 This shows a need for awareness about a change of habits, behaviour therapy, and sleep hygiene measures.
Among the medications to sleep, the most used are benzodiazepines. This is worrying for the high risk of abuse and dependence, especially in people who have easy access to them, as is the case of physicians, especially those who work with mental health. 23 Besides the risk of addiction, chronic benzodiazepine use can result in cognitive effects, such as sedation and drowsiness, mental slowing, and anterograde amnesia. Further, it can impair driving and working performance and cause accidents. 24
Poor sleep was associated with an irregularity of hours of sleep and lying down for long periods without sleep. Other studies have shown a relation between sleep hygiene and sleep quality. 11,25 However, our study was the first to observe this relation in psychiatry residents. Inadequate sleep hygiene has been related to sleep problems that became a diagnostic category in the International Classification of Sleep Disorders. 26 Although a recognized and commonly used treatment option, there is no absolute consensus about sleep hygiene treatment. 27,28
This study showed an association between sleep quality, anxiety, and social phobia symptoms. This finding is in agreement with other studies that showed a relation between anxiety disorders, social phobia, and poor sleep quality. 29,30 However, this finding is unprecedented among physicians and medical students. It is widely known that sleep problems are associated with various psychiatric disorders. 31 –33 In 90% of severe mental disorders, there are reports of chronic insomnia. 32 In some cases, insomnia is considered the main complaint, instead of other psychiatric symptoms. The relation between sleep and anxiety is well established, and a feedback cycle has been suggested. Generalized anxiety disorder and social anxiety disorder seem most related to poor sleep quality. 18,19
One explanation for the poor sleep quality in psychiatry residents is working time. Beyond the regular hours devoted to the residency, some activities (such as preparing lectures, writing clinical cases, or reading scientific papers) are conducted outside of the official time of residency. This is a common practice in many medical residencies around the world. Maybe saving part of the residency time for these activities could increase the sleep time and leisure, and minimize the problem of poor sleep quality.
In addition, the low value of the scholarship in some countries (around US$1100) stimulates residents to work in their free time, increasing the workload and reducing sleep time and leisure. Thus, the creation of an exclusive dedication regiment for medical residency with better pay and better working conditions could be an attempt to minimize the problem.
Some limitations to our study must be acknowledged. Our findings are based on self-report scales. Thus, the personality of the resident and his mood at the time of the interview may influence the evaluation and impair the reliability of data. Comparisons with medical residents in other countries or with other specialties provide new and important conclusions. Differences between the medical residency programs around the world may limit the external validity of these data. However, it does not diminish the importance of our findings. This is the first study about sleep of psychiatry residents and offers important conclusions. New studies in other locations are suggested to compare the results.
Conclusion
In summary, our findings indicate that poor sleep, daytime sleepiness, and hypnotics use are frequent among psychiatry residents. Despite the magnitude of the problem, the search for medical care was small. More attention to this clinical problem is needed, considering that sleep disorders can affect quality of life, predispose a person to metabolic syndrome, and be associated with poor work performance.
Footnotes
Acknowledgements
We thank all of the psychiatry residents for their participation in our study. Melo conceived and designed the study, and collected and analyzed the data. Daher, Medeiros, and Sales de Bruin contributed to the conception and design of the study. Santana and Lima contributed to data collection and analysis. All authors contributed to the drafting and revisions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and (or) publication of this article. The authors are responsible for the content and writing of the paper.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and (or) publication of this article. The authors do not have a financial relation with a commercial entity that has an interest in the subject of this paper.