
Abstract
This article provides a narrative account of a small research study run with a grant from the Institute of Group Analysis (IGA) Legacy Fund. It discusses the challenges and opportunities of engaging in research involving interdisciplinary collaboration between trainee cognitive behaviour therapists working in the NHS and group analysts/groupwork practitioners. It makes the case for building on the results of this study by developing a protocol for a pre-post pilot study using a mixed methods approach to explore whether IGA-led groupwork in CBT training has any effect on patient outcomes and service key performance indicators.
Keywords
Background and rationale 1
The project was set at a university in Northeast England. It involved testing the feasibility of implementing and evaluating a version of SP/SR groupwork delivered by facilitators from the Institute of Group Analysis (IGA) in the training of cognitive behaviour therapists based in Improving Access to Psychological Therapies (IAPT) services.
Training in Cognitive Behaviour Therapy (CBT) is funded by Health Education England (HEE) as part of the IAPT programme, now called NHS Talking Therapies. The training is at postgraduate diploma level and courses last for between 12–18 months. To be eligible to apply for high intensity training (HIT) in CBT, candidates must have at least two years relevant experience of working in mental healthcare settings. Most candidates are psychological wellbeing practitioners who offer guided self-help and psychoeducational groups in IAPT. Other professional groups who apply for HIT training include mental health nurses, occupational therapists, counsellors, social workers, for example.
Compared to the training of a group analyst or a groupwork practitioner, the CBT course is relatively brief. The Psychological Professions Workforce Plan for England (Health Education England, 2021) aims to increase the supply of psychological professionals to meet increasing demand. Shorter trainings are necessary if we want to extend the reach of psychotherapeutic interventions and make them more accessible. Psychotherapists with extensive and specialist training such as group analysts have a role in training, supervision, consultation, and support of other practitioners (Health Education England, 2021).
Personal and professional development
Like all psychotherapists, cognitive behaviour therapists need to cultivate qualities such as non-defensive curiosity, courage, openness, and humility to constantly question whether their practice is ethical, effective, and efficient. These qualities are vital in the identification and modification of their therapy-interfering beliefs and behaviours (Waller, 2009). Clinical supervision plays a role in these processes. However, challenging personal and interpersonal schema in supervision often evokes discomfort or distress because these domains are more ‘emotionally sensitive, more personally felt’ (Bennett-Levy and Thwaites, 2007: 264). Collusion often occurs when CBT supervisors do not want to upset their supervisees (Milne et al., 2009).
Another way of cultivating the qualities required and of questioning oneself is for therapists to undergo personal therapy during training. This is not required as part of CBT training, and cognitive behaviour therapists experience ‘considerable internal conflict’ if they engage in ‘relationally oriented’ personal therapy which makes it more difficult for them to use a protocolized CBT approach in practice (Noble and Rizq, 2020: 29). A proxy for personal therapy in CBT is Self-practice/Self-reflection (SP/SR) (Bennett-Levy, 2006) which involves engaging in a process of experiential learning and reflection perhaps with a peer as in co-therapy or facilitated by an independent person in a group of peers or as a process of self-reflection and mindfulness (Bennett-Levy, 2019; Bennett-Levy et al., 2003).
Self-practice / Self-reflection
Self-practice/Self-reflection (SP/SR) (Bennett-Levy, 2006) is frequently used in CBT training programmes, and groupwork is a key component. It is built on the Declarative-Procedural-Reflective (DPR) model which is a conceptual framework explaining how trainees develop competence in CBT and how therapists develop expertise in CBT (Bennett-Levy, 2006). According to the DPR model, competence as a cognitive behaviour therapist comes about through the acquisition of declarative knowledge (i.e., theory of CBT) and procedural skills (i.e., practice of CBT). This requires development of the ‘personal self’ and the ‘therapist self’ (Chigwedere et al., 2019) through two interrelated processes called ‘self-practice’ and ‘self-reflection’ whereby the practitioner practises CBT techniques on themselves and then reflects on this experience (Bennett-Levy et al., 2014). In addition, a process of deeper reflection is required as a ‘bridge’ between rational-technical competence and emotional-relational competence, so that knowledge and skills are sensitively applied to meet individual patient’s needs in a real-world clinical setting (Bennett-Levy, 2019).
The tripartite model used in the training of psychoanalytic psychotherapists is somewhat like the DPR model as it requires an integration of learning from three different but interrelated spheres: personal therapy (self-practice/self-reflection), practice placement and close clinical supervision (procedural skills), and theoretical lectures (declarative knowledge). So, whilst the theory and philosophy of cognitive-behavioural and psychoanalytic approaches are in many ways incommensurable, it is possible that there are some potentially useful translations of interdisciplinary collaboration in terms of practice.
How does SP/SR work?
The DPR model proposes that SP/SR works in part by enhancing self-awareness (or insight). Self-awareness is a core component of the model because it provides feedback to therapists about their inner world of thoughts and feelings, and how these might translate into helpful or unhelpful behaviour within their clinical work. The DPR model has been further elaborated to explain the clinical decision-making process at the micro-level to show how patient communications evoke ‘sophisticated, flexible, and responsive’ therapist communications (Bennett-Levy and Thwaites, 2007: 258). Another hypothetical mechanism by which SP/SR works is by enhancing interpersonal awareness (or outsight) because it ‘allows therapists to put themselves into their patients’ shoes . . . [and] as a result, this experience is reported to increase therapists’ empathy for their patients’ (Gale and Schröder, 2014: 388). This process aims to transform textbook knowledge into true understanding through a ‘deeper sense of knowing’ about oneself and how patients might experience CBT, positively and negatively (Bennett-Levy et al., 2001: 201). Ultimately, the main purpose of SP/SR is not self-practice for its own sake but for helping the trainee (or practitioner) to become a better therapist.
The DPR model has since been expanded to conceptualize ‘the nature and function of therapeutic empathy’ (Thwaites and Bennett-Levy, 2007: 592). As Thwaites and Bennett-Levy (2007: 592) point out, ‘When cognitive behaviour therapists ask patients to engage in difficult and emotionally challenging tasks, therapeutic empathy becomes even more important’. Finally, another mechanism by which SP/SR might work is by a shift in trainees’ identity or self-schema (Haarhoff, 2008). Engaging in SP/SR during training can lead to either assimilation i.e., ‘an increasingly nuanced and deeper sense of self’, or accommodation i.e., ‘a new sense of self’ (Freeston et al., 2019: 3). The most sustainable benefits accrue when trainees engage fully with the process which integrates the ‘therapist self’ and ‘personal self’ schema (Chaddock et al., 2014).
Why use SP/SR to develop emotional-relational skills in CBT trainees?
The effects of incorporating SP/SR into CBT training has been evaluated empirically (e.g., Thwaites et al., 2017; Davis et al., 2015), and a mixed-method review of 10 published studies found an improvement in self-reported technical skills, self-awareness, interpersonal, perceptual, and relational skills, empathy for patients, and understanding of discomfort associated with self-disclosure, although confidence in these findings were undermined by inconsistencies and methodological weaknesses (McGillivray et al., 2015). Other studies claim that SP/SR is acceptable to trainees (Chigwedere et al., 2021), to have several positive effects on trainees (Scott et al., 2021), although not every trainee is likely to benefit (Chaddock et al., 2014; Spendelow and Butler, 2016).
SP/SR has been called the engine of lifelong learning (Bennett-Levy et al., 2009: 119) because it promotes a habit of ongoing ‘reflection-in-action’ and ‘reflection-on-action’ (Haarhoff and Thwaites, 2016: 9). Once qualified, therapists (and supervisors) are at risk of professional stagnation and decay of skills without ongoing reflection (Rønnestad et al., 2019). Therefore, participating in the SP/SR process as a trainee is important because is likely to influence the trajectory of therapists’ personal and professional development throughout their career.
Problems reported by trainees when engaging in self-experiential work
Introspection is one aspect of SP/SR that can make trainees feel uncomfortable and unsettled (Fraser and Wilson, 2010; Sutton et al., 2007), confused, frustrated, irritated, or bored (Haarhoff et al., 2011). SP/SR can be perceived as threatening (Bennett-Levy and Lee, 2014) with some practitioners worrying about opening a Pandora’s box of uncontrollable thoughts and feelings which might interfere with their clinical work (Sanders and Bennett-Levy, 2010: 463). Other negative effects reported by trainees when practising CBT techniques include ‘going too deep, too soon’, over-analysing and ruminating on what they had uncovered (Spendelow and Butler, 2016: 607), which may cause exhaustion and mood swings (Hahn et al., 2023). This suggests that training in group facilitation is essential.
SP/SR groupwork
Sharing one’s reflections is a key component of the SP/SR process and group delivery of SP/SR is recommended because ‘reading or hearing about other group members’ experiences enables participants to normalize their experience and/or compare and contrast it with others’ (Bennett-Levy and Lee, 2014: 60). In CBT training programmes, SP/SR may be delivered in groups facilitated by clinical educators, lecturers and/or supervisors, and the groups may be synchronous face-to-face (Bennett-Levy et al., 2014) or online (Jona et al., 2022), or asynchronous via an online blog (Spafford and Haarhoff, 2015). However, facilitation of SP/SR groupwork requires a different skillset from teaching or supervising (Bennett-Levy et al., 2014). Facilitators may need specialist training to create a supportive and enriching group culture (Bennett-Levy et al., 2014) which is crucial to achieving positive outcomes for trainees.
Problems reported by trainees when engaging in groupwork
Groupwork in SP/SR is another factor that can be anxiety-provoking (Schneider and Rees, 2012; Haarhoff and Stenhouse, 2004). Group discussion involves a degree of self-disclosure and peer feedback which helps in the consolidation and application of learning (Freeston et al., 2019). However, trainees and therapists sometimes find groupwork demanding and destabilizing, especially when no explanation has been given as to why SP/SR is being conducted in the group (Maaß et al., 2022). Whilst the group process might enhance some trainees’ engagement in the SP/SR process, they may be inhibited if the group includes work colleagues (Bennett-Levy and Lee, 2014). Shared reflection carries some risks such as fear of rejection or judgement, feelings of self-consciousness or embarrassment (Freeston et al., 2019), concerns that it could be exposing (Spendelow and Butler, 2016), as well as uncomfortable power issues and emotional intensity (Maaß et al., 2022). Some practitioners worry that their privacy will be invaded if expected to ‘share [their reflections] on a public noticeboard’ (Haarhoff et al., 2015: 325) or that their confidentiality might be breached (Spendelow and Butler, 2016).
Likewise, mixed effects were reported by counsellors and psychologists during and after their training courses of attending ‘personal development groups’, with both positive and negative effects being attributed to the group facilitation skills of the person running the group (Smith and Burr, 2022; McMahon and Rodillas, 2020; Bledin, 2019; Moller and Rance, 2013; Fairhurst, 2011; Knight et al., 2010; Robson and Robson, 2008; Lennie, 2007). This suggests that training in group facilitation is essential.
IGA-facilitated SP/SR groupwork
To the best of our knowledge, this aspect of SP/SR has never previously been undertaken by group facilitators trained by the Institute of Group Analysis (IGA). Bennett-Levy and Lee (2014: 58) acknowledge that group facilitators need to be able to increase engagement and intensify the experience ‘by offering alternative perspectives and allowing the reflection process to operate at different depths’. Skilful facilitation helps group members to trust each other, which subsequently makes sharing a lot easier and allows for a true ‘learning community’ to be created (Bennett-Levy et al., 2014: 28).
IGA training programme
The IGA offer intensive educational programmes drawing upon psychoanalytic theory, social science, and systems theory in its understanding of the human experience. To qualify, group analysts undertake a long-term specialist training in group psychotherapy and groupwork practitioners undertake a medium-term non-specialist training in groupwork. Successful completion of the IGA diploma course confers eligibility to join the IGA as a groupwork practitioner and associate membership, and successful completion of the qualifying course confers eligibility to join the IGA as a group analyst and full clinical membership. The IGA training is based on a model of group facilitation which stresses the ‘meeting of minds’ i.e., sharing of thoughts and feelings (Behr and Hearst, 2008), and aims to equip facilitators with the knowledge and skills to create a group culture that is safe but not too safe (Berman, 2019), and this is important because group discussion often requires a degree of risk-taking. Moreover, many IGA-trained group facilitators also run reflective practice groups (Einhorn, 2019) and staff support groups (Hartley and Kennard, 2009; Novakovic and Vincent, 2019), and their skills are likely to be transferable in the delivery of SP/SR groupwork.
Using IGA-trained group facilitators for SP/SR could prove to be highly beneficial. Firstly, their extensive and intensive training in groupwork equips them to contain the ‘strong emotional reactions’ that may be evoked when trainees use SP/SR to question themselves as a person and as a therapist (Freeston et al., 2019). So, whilst a degree of personal exploration is encouraged, skilful facilitation will ensure that the ‘boundaries are more contained’ (Bennett-Levy and Lee, 2014). Secondly, trainees get more out of SP/SR when the group process is working effectively (Bennett-Levy and Lee, 2014). IGA-trained group facilitators have expertise in ‘oiling the wheels’ of group interaction, i.e., encouraging self-disclosure and peer feedback (Bennett-Levy and Lee, 2014: 50). This helps to promote group cohesion and fostering participation, both of which are associated with positive experiences (Maaß et al., 2022). Thirdly, IGA-trained group facilitators have expertise in focusing on feelings, both expressed and unexpressed, in the group. This skill will help them to attend ‘both to what [trainees] verbalize and to their non-verbal communication’ which creates ‘a feeling of safety’ in SP/SR groupwork (Mackenzie and O’Mahony, 2021: 13). Finally, observation of IGA-trained facilitators in action may prompt trainees to internalize some emotional-relational skills such as empathic attunement, resonance, abstinence, silence, and containment of distress (Barwick and Weegmann, 2017).
Whilst there are other UK-based trainings in group facilitation, they tend to be relatively short courses e.g., 3–9 days and competence is not assessed. What makes the IGA training unique is that qualified groupwork practitioners and group analysts are required to participate in experiential groupwork and personal therapy in a group over a relatively long period i.e., two to four years respectively. To pass the course, they must demonstrate that they are knowledgeable about group dynamics and the stages of small group development and that they are skilful in maximizing the positive effects of group interaction and minimising the negative effects (Bacha, 2005).
There may of course be some drawbacks to involving group analysts and groupwork practitioners in SP/SR groupwork. Unless they are dual trained in group facilitation and CBT, they may not be able to fulfil the vital ‘linking and synthesizing’ function of a CBT-trained facilitator (Freeston et al., 2019: 8). In any further research, this issue could be addressed by offering an intensive training workshop to equip facilitators with a basic understanding of CBT principles and techniques.
Summary
Overall, the potential advantages outweigh the potential disadvantages of involving IGA-trained facilitators in the delivery of SP/SR groupwork due to their knowledge and skills in facilitating groups developed through the training described above. The recommendation for experiential learning and reflection in revised curriculum for CBT training (Health Education England, 2022) is both a challenge and an opportunity for the IGA. This study represents the beginning of a research cycle that has the potential to demonstrate with clear evidence that groupwork facilitated by IGA-trained facilitators in CBT training is effective across a range of measures such as patient outcome measures, staff satisfaction, and service key performance indicators, such as patient completion of treatment and retention of staff.
Research study
Aims of the study
Primary aim
To investigate whether the implementation and evaluation of SP/SR groupwork is feasible when using IGA-trained group facilitators in a HIT training programme.
Secondary objectives
- To report on i) participant recruitment; ii) characteristics of the resulting sample; iii) rates of retention / attrition, iv) utility of outcome measures and data collection methods; and v) estimated costs of delivering the intervention.
- To report on the interim benefits of the intervention to participants.
- To use the data generated on the difference in outcomes (effect sizes) to inform a power calculation for sample size in any future study.
Design, methods, and analysis
The University’s Health Research Ethics Sub-Committee authorized and indemnified the study. The protocol and the results of the SP/SR groupwork project are reported elsewhere (under review). Briefly, there are several stages of the research process in health and social sciences which usually starts testing the research design and methods. Our study is a Phase I feasibility study which aims to find out if the study can be done easily and conveniently i.e., whether the research design and methods are doable and practical.
Recruiting participants
The methods began with recruiting a convenience sample of 30 CBT trainees from a cohort of 33. All students were working within local IAPT services and were treating patients under close supervision. Students are seen as a ‘vulnerable’ population because they might believe that not giving consent could affect their grading when the researcher is also their lecturer. Therefore students require special protections and safeguards when participating in university-based research. The use of coercion when recruiting students is a serious issue which calls into question the overall validity of the findings since participants may provide answers on questionnaires that are not true (Leentjens and Levenson, 2013; Dugosh et al., 2010). All procedures must be perceived as acceptable and fair, especially when participation is required or when incentives are offered. In our study, to emphasize that participation was voluntary, written consent was obtained without any overt or covert pressure put on trainees. We reduced the risk of coercion with trainees being able to opt in by signing the form in their own time and at home with time to consider and to consult with others about whether to take part or not. Participants were able to withdraw consent at any time up to the commencement of the data analysis stage i.e., 18 months from the start of the project.
Engaging group facilitators
The next step was engaging qualified group analysts or groupwork practitioners through the Institute of Group Analysis (IGA). Information about SP/SR was sent to anyone interested in finding out about the project. Evidence about their experience and expertise in groupwork was collected by submission of a CV and reference. Four group analysts and four groupwork practitioners were engaged. They were not part of the study team (i.e., they were external, employed on a casual contract). Their contract included a section on the limits of confidentiality and outlined the responsibilities of a SP/SR groupwork facilitator and their remuneration. An online orientation session designed to introduce them to the project and to answer any questions they have about it lasted two hours. Since some of the group facilitators were not trained in CBT, the orientation session involved basic training in how SP/SR is designed to help trainees acquire CBT concepts and skills, and how group facilitators can enhance this process. There were five main instructions regarding the conducting of the SP/SR groupwork: 1) To encourage dialogue between all group members; 2) To help group members focus on each trainee’s thoughts, feelings, and behaviours, not the trainee’s patient’s thoughts, feelings, and behaviours. In other words, to be clear that the group was a ‘self-reflective’ group and not a ‘reflective practice’ group; 3) To support group members to manage their discussions and disagreements in a constructive manner; 4) To divert discussion of extremely upsetting personal issues which may be better addressed in personal therapy or counselling; and 5) To use ordinary language and no psychoanalytic terminology.
One week before each SP/SR group, facilitators were sent the relevant chapter from the workbook (Bennett-Levy et al., 2014) so that they could familiarise themselves, only if desired, with the relevant CBT concepts and skills covered in that module. Facilitators were invited to contact a member of the research team, who are all accredited cognitive behaviour therapists, if they had any questions or concerns.
SP/SR groupwork
There were eight group facilitators (A–H). Each group had four to five trainees with one facilitator (See Table 1). They met six times over 12 months from May 2022 to January 2023.
SP/SR Facilitators and Groups.
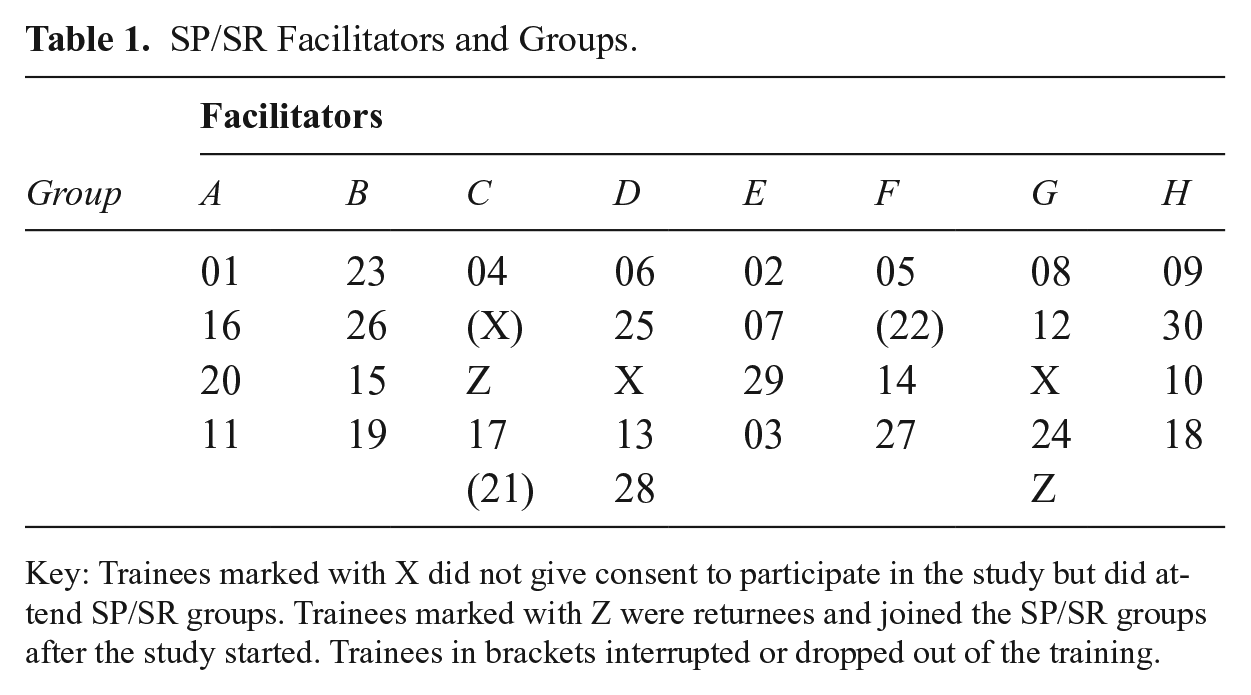
Key: Trainees marked with X did not give consent to participate in the study but did attend SP/SR groups. Trainees marked with Z were returnees and joined the SP/SR groups after the study started. Trainees in brackets interrupted or dropped out of the training.
The groups were online and ran for one and a quarter hours with one and a quarter hours’ preparation beforehand for the trainee to complete the CBT exercise during a timetabled teaching session. Confidentiality was stressed to maintain safe psychological boundaries and to minimize the potential risks of sharing personal information in group sessions. Furthermore, all trainees were asked to agree to group ground rules such as not to discuss issues raised by another trainee outside of sessions without that person’s clear consent. The ground rules clarified how SP/SR differentiates process from content and the difference between SP/SR and personal therapy or counselling. Trainees were advised that they may feel more comfortable at times to share only how they found doing the exercise (i.e., process) and not the details (i.e., content) as illustrated in the following example (Figure 1).

Example of differentiation between process and content.
Trainees were advised that the focus of SP/SR is a ‘challenging problem’ rather than a ‘major negative life event’ such as divorce, bereavement, abuse, and that SP/SR can support them ‘in dealing with personal difficulties only insofar as it also helps to improve professional behaviour and promotes a deeper understanding’ of their clients’ experiences of CBT (Maaß et al., 2022: 29).
The contract outlined the facilitators’ duties and responsibilities. This included an obligation to break confidentiality should any trainee disclose that they or others are at risk of harm with a section on the limits of confidentiality. Likewise, the contract asked the facilitator to inform the lead researcher/s of any inappropriate behaviour or concerns about a trainee’s capability to work ethically and effectively. In these circumstances, the lead researcher/s who would take appropriate action to safeguard trainees, clients, or others.
Results
This article reports our interim findings with the final quantitative results to be reported elsewhere. On that basis, this study shows it is feasible to implement a new version of SP/SR groupwork delivered by facilitators from the Institute of Group Analysis (IGA) in the training of high intensity cognitive behaviour therapists. It is also feasible to evaluate this intervention using the instruments chosen. Analysis of data derived from repeated self-report measures from baseline to 12 weeks follow up evidenced significant and positive changes on self-reported self-awareness, confidence in using emotional-relational skills in practice, and perceived stress. Analysis of data derived from independent assessment of trainees’ emotional-relational skills in pre- and post-intervention role plays evidenced significant improvement in the group as a whole but with wide variation in competence at baseline and at the end of training. Finally, approximately 59% of trainees expressed overall satisfaction with the teaching programme. The cost of the study was approximately £10,000. No adverse events were recorded.
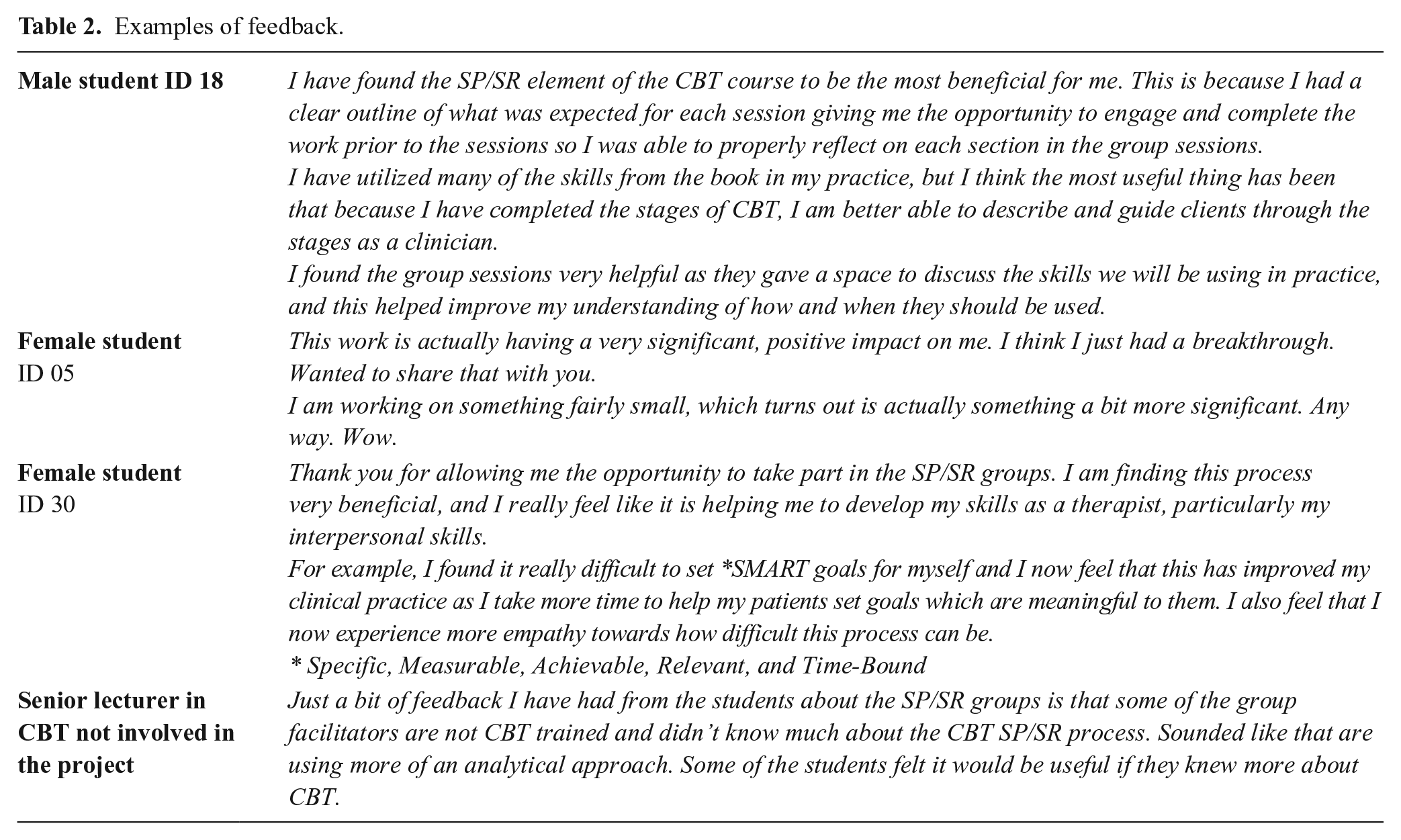
Written feedback was invited from participants by email after each SP/SR group. Feedback was also received from a senior lecturer in CBT (See Table 2).
Examples of feedback.
Discussion
The study clearly demonstrates that pragmatic research and interdisciplinary collaboration between group analysts/groupwork practitioners and cognitive behaviour therapists is possible, and potentially transformative. Otherwise, what has been learned so far is limited by the nature of a feasibility study. Thus, it is not possible to say whether the trainees actually engaged with self-practice or self-reflection, or what IGA-trained facilitators actually did. In future, it would be desirable to collect and analyse process data so that we could investigate what happened during the SP/SR teaching sessions in several ways.
Firstly, measurement of adherence to the self-practice component could be achieved by asking trainees to submit an example of their thought diary or activity schedule for example, prior to the SP/SR group. Secondly, measurement of adherence to the self-reflection component could be achieved by video recording the online sessions and using a strategy such as discourse or conversational analysis of observational data to pinpoint mechanisms of change in IGA-led SP/SR groups. Thirdly, measurement of fidelity of implementation would require an operational definition of what each group analyst or groupwork practitioner says and does to facilitate an SP/SR group. Our facilitators shared their experiences, views, and perspectives in the debrief session but because they were not participants in the study, we are unable to report this ethically. Our facilitators were given a fairly free reign in running the SP/SR groups, with some using a structured approach and some using a more free-floating discussion approach. In future, it would be important to capture how the differences in approach influenced trainees’ engagement and learning. Usually, a degree of standardization is necessary in research for the replication of the intervention and generalization of findings. This often requires a process of ‘manualization’ as ‘a way of ensuring that the method remains consistent whoever is implementing it’ (Dalal, 2017: 49). Whilst Dalal (2017: 49) worries that what is delivered would be ‘unrecognizable’ as group analysis which has an ‘open, improvizational nature’, systemization means that fidelity to a specified model can be measured (Cassullo and Keller, 2015). The existing group analytic literature has already investigated and categorized what group analysts say and do (Lorentzen, 2020; Brown et al., 2012; Lo Coco et al., 2004; Kennard et al., 2000; Sandahl et al., 2000). These descriptions are not prescriptive but may help to identify the ‘unity and diversity of the broad church of group analysis’ (Hopper et al., 2017: 80) and what constitutes good practice in using a group analytic approach (Maratos and Bledin, 2022). Lastly, transcripts of semi-structured interviews or focus groups could be analysed using qualitative methods to gain a deeper insight into the experiences of both trainees and facilitators.
Further research is needed to determine whether the theory underpinning SP/SR is empirically supported or not. At present, there is some support for the DPR model because research studies suggest that CBT patient outcomes are influenced by their therapists’ interpersonal skills more that their technical and conceptual skills (Scott et al., 2021; Chaddock et al., 2014; Haarhoff, 2008). The accumulating evidence leads Bennett-Levy and Thwaites (2007: 278) to ‘the inescapable conclusion that interpersonal skills are intimately related to our personal (self-schema) development and capacity to reflect on our experience’. These two problems might be responsible for the high dropout rates in IAPT (NHS Digital, 2023) and further research may be able to show that IGA-led SP/SR groupwork is effective in improving both emotional-relational skills and reflective ability.
The next step for us will be a pilot quasi-experimental study investigating the impact of SP/SR groupwork delivered by IGA-trained facilitators (i.e., the ‘intervention’) on IAPT patients as well as practitioners. This study would require ethical approval from the NHS.
If the results of the pilot quasi-experimental study are promising e.g., showing a potential positive impact on patient retention, then there would be strong grounds for applying for research funding for a Phase II randomized controlled trial (RCT) across two or more sites with a much larger sample. This would help to establish whether IGA-led SP/SR groups are more effective in terms of direct outcomes for trainees and indirect outcomes for their patients compared to SP/SR groups delivered as online blogs for example (Freeston et al., 2019; Farrand et al., 2010). The protocol for an RCT will have to set out the number of therapists and patients per therapist to ensure sufficient statistical power (i.e., 0.8) to detect difference between trainees (Schiefele et al., 2017).
Limitations
This small feasibility study aimed to gather data on recruitment rate, participant characteristics, rates of retention/attrition, utility of outcome measures and data collection methods, and costs. It was therefore designed to assess whether implementation and evaluation of the IGA-led SP/SR intervention was possible and did not seek to measure its effectiveness, which would require an RCT.
Sources of potential bias should be noted. Firstly, although all the instruments used to assess the secondary outcomes are well validated, they are self-reported and are therefore subject to response, recall, or social desirability bias for example. Secondly, our sample is a convenience sample of an intake of trainees onto the course and is therefore subject to recruitment bias.
Conclusion
This article has reported results from a small study which shows that it is feasible to implement Group SP/SR delivered by IGA-trained facilitators and is it feasible to evaluate it.