
Abstract
We present a 55-year-old male patient with right renal carcinoma with long inferior vena cava (IVC) tumor thrombus who underwent robot-assisted laparoscopic radical nephrectomy with extensive IVC resection and left renal vein ligation. The patient had a history of hematuria only prior to admission. Our case involved resection of the entire abdominal segment of the IVC and left renal vein without reconstruction. Unfortunately, the patient passed away over a year after the surgery due to brain metastasis.
Keywords
Introduction
Renal carcinoma exhibits venous extension, with an estimated 4%–10% patients eventually developing tumor thrombi.1–3 To achieve R0 resection, complete resection of the involved vein is performed.4–6 However, subsequent inferior vena cava (IVC) reconstruction presents challenges such as the need for long-term anticoagulation, low long-term vascular patency rates, and a substantially increased risk of complications such as infection.6,7 We present a case of robot-assisted laparoscopic resection of the abdominal segment of the IVC and the left renal vein without reconstruction in a patient with renal carcinoma and concomitant IVC tumor thrombus. With the patient’s consent, we present this case to offer new insights into the management of IVC involvement in cancer.
Case report
We present the case of a 55-year-old male who presented with painless hematuria for 10 days before admission. He did not report any other symptoms. Physical examination uncovered a palpable and firm mass in the right abdomen the size of an infant’s head. Computed tomography and magnetic resonance imaging revealed a space-occupying lesion in the right kidney (approximately 89 × 97 × 74 mm) with tumor thrombus formation in the IVC and bilateral renal veins, accompanied by the formation of collateral circulation (Figure 1). Moreover, ultrasonography confirmed the presence of a tumor thrombus in the IVC (Mayo II) extending from 6.1 cm below the opening of the right renal vein to 6.5 cm above the opening. The patient underwent robot-assisted laparoscopic radical right nephrectomy, extensive segment IVC resection, and left renal vein ligation. Preoperative imaging data. A–C: MRI shows a massive space occupying lesion in the right kidney (about 89*97*74 mm) with tumor thrombus formation in the IVC and bilateral renal veins. D–F: Well-developed collateral circulation, including three lumbar and vertebral veins, with venous drainage through the azygous and hemiazygos veins.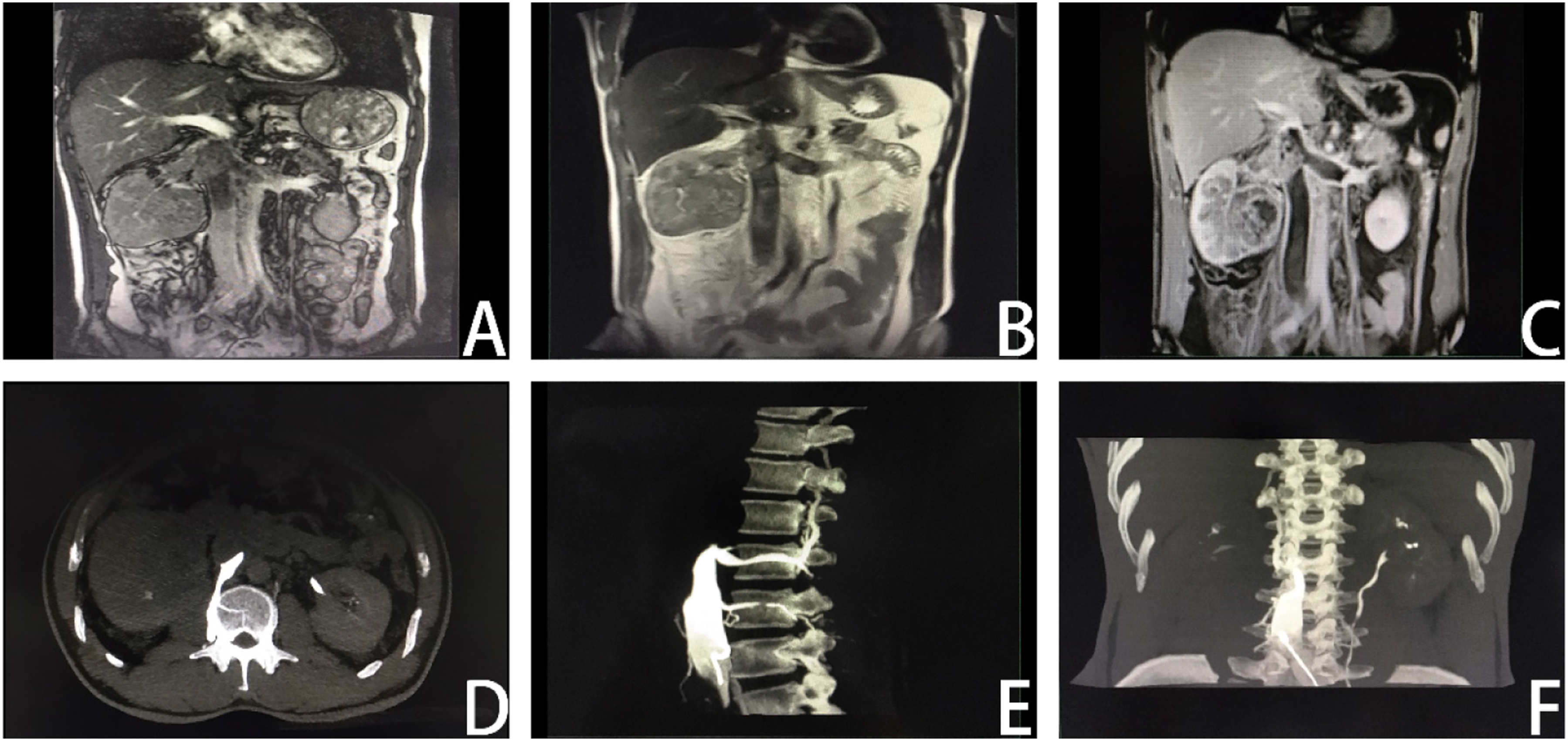
Surgical procedure: Using a B-mode ultrasound laparoscope probe, thrombi were found extending from the upper end to the second hepatic hilum and from the distal end to the level of the bifurcation of the left and right common iliac veins. Furthermore, there was evidence of tumor embolism in the left renal vein. Sequentially clamped at the distal bifurcation of common iliac veins, the distal end of the left renal vein tumor thrombus, and the proximal IVC near the second porta hepatis using vessel loops to extract the tumor embolus. We discovered that the IVC was completely obstructed by cancer thrombus and associated thrombus, with local invasion of the IVC wall, precluding the possibility of surgical thrombectomy. Therefore, the entire segment of the IVC within this range was resected along with the distal portion of the left renal vein containing the tumor embolus. The right kidney and adrenal gland were completely excised (Figure 2). IVC Surgical procedure of IVC resection combined with left renal vein ligation. A: Ligation of the right renal artery B: Ligation of the distal IVC C: Ligation of the left renal vein D: Ligation of the proximal IVC E: Tumor thrombus and thrombosis F: IVC resection without reconstruction.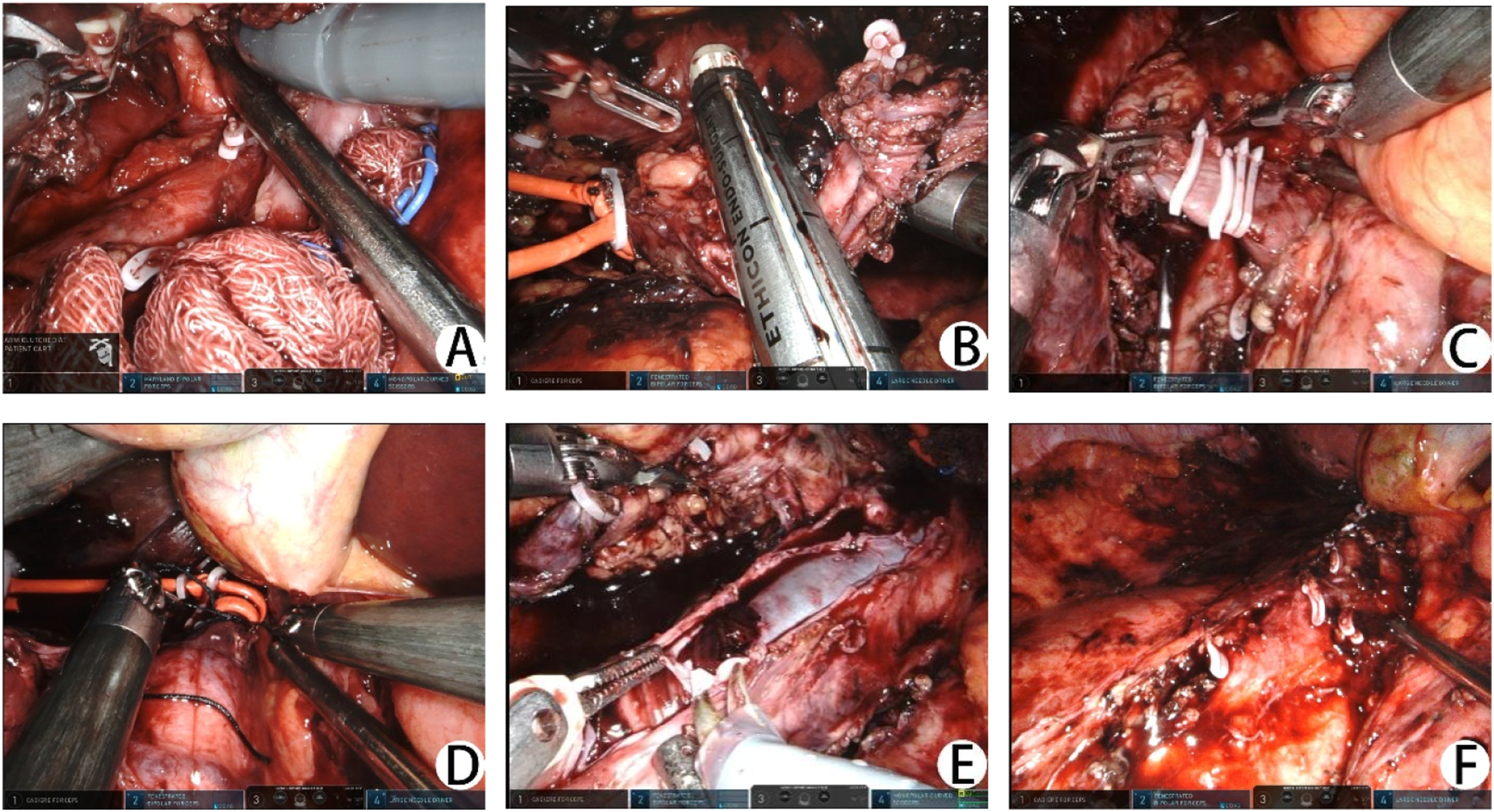
Complete resection of the tumor and tumor emboli was achieved, with an operation time of approximately 350 min and intraoperative blood loss of approximately 100 mL. Following the surgery, liver and kidney function were continuously monitored (Figure 3). Three days post-surgery, there was a sharp elevation in liver enzymes, with alanine aminotransferase (ALT) peaking at 5720 U/L and aspartate aminotransferase (AST)peaking at 11,590 U/L. The peak postoperative creatinine level was 543 μmol/L, and on the fifth day postoperatively, oliguria and notable edema in the lower extremities and scrotum were observed. Within 3 weeks postoperatively, continuous renal replacement therapy (CRRT)and intermittent hemodialysis (IHD)were sequentially administered. With symptomatic supportive treatment, liver and kidney function gradually improved and returned to preoperative levels. Changes in postoperative indexes. A: Changes in serum creatinine and hemodialysis treatment B: Changes in liver enzymes.
The edema in both lower limbs completely subsided, liver function returned to normal, and renal function approached the preoperative level, indicating a favorable recovery during the follow-up period. The postoperative pathology report revealed that the tumor tissue invaded the renal sinus fat without breaking through the renal capsule. Additionally, the tumor tissue involvement was observed within the IVC, accompanied by infiltration into the IVC wall. No metastatic cancer was detected in the lymph nodes. On a follow-up phone call, we learned that the patient passed away 1 year later owing to cerebral metastasis.
Discussion
There is limited research on IVC resection without reconstruction, particularly in cases involving extensive IVC resection. More than 50% of patients without IVC reconstruction reported lower limb edema, which was generally well tolerated. 8 The overall incidence rate of acute renal failure is below 40%. 9 Renal failure typically resolved spontaneously, and some patients regained renal function after dialysis, consistent with several studies.9–11 The liver is susceptible to ischemia and hypoxia, and liver ischemia-reperfusion injury resulting from decreased venous return and hilar occlusion is directly associated with acute liver failure. Although our patient did not undergo porta hepatis occlusion during the operation, a certain degree of liver function impairment still occurred postoperatively. Further analysis is warranted to understand the specific etiological mechanism in such cases. Even in patients with adequate collateral circulation, these complications can still occur owing to the trauma associated with extensive IVC resection and the inevitable disruption of the original collateral vessels intraoperatively, leading to insufficient venous return. 12 As collateral circulation gradually forms, these complications diminish.
IVC reconstruction, however, presents challenges such as the need for long-term anticoagulation, low long-term vascular patency rates, and a substantially increased risk of complications such as infection.6,7 Multiple studies on IVC reconstruction have reported an average graft patency rate of approximately 54%. 13 Furthermore, the incidence of venous thromboembolism after reconstruction and anticoagulation therapy ranged from 7% to 22%.14,15 Moreover, 1%–6% of prosthetic graft infections eventually require graft removal in 85% of instances. 16 Therefore, for patients with well-developed collateral circulation, IVC resection without reconstruction is considered a safe, feasible, and well-tolerated option. 8 This approach can reduce operative time and minimize complications associated with artificial vascular replacement. 17 Even if postoperative complications arise, symptomatic treatments such as dialysis can allow time for the establishment of collateral circulation. Thus, we are inclined to favor the surgical strategy of simple IVC resection without reconstruction to minimize associated long-term complications.
In our case, the tumor thrombus extended into the infrarenal IVC and left renal vein in a retrograde venous reflux direction, which is uncommon in clinical practice. Such patients often have highly malignant tumors that easily adhere to surrounding tissues and are prone to distal thrombosis, resulting in a worse prognosis. 6 During the surgery, we observed that the thrombus was notably longer than what was indicated in the preoperative imaging, and we speculated that this discrepancy might be related to the IVC angiography. Thrombosis caused by IVC angiography is rarely reported. This type of renal cancer involving IVC invasion is likely to possess increased immunogenicity, 9 which can lead to enhanced immune monitoring and a hypercoagulable state. 18 Simultaneously, the cancer thrombus completely obstructs the IVC, impeding the normal passage and elimination of contrast agents and resulting in their excessive accumulation. Additionally, the high viscosity and hypertonicity of contrast agents contribute to slow blood flow and vascular endothelial damage, thereby activating endogenous and exogenous clotting pathways, ultimately leading to the formation of a long thrombus. 19
Conclusion
In conclusion, we demonstrate the feasibility of performing abdominal segment resection of the IVC combined with left renal vein ligation without the need for vascular reconstruction in carefully selected patients. 20
Footnotes
Contributors
Kun Shang contributed to the drafting, interpretation, and writing of manuscript. Changjiu Li, Jun Chen and Ning Li contributed to the literature research. Huadong He contributed to the literature research, supervision, and conception of manuscript. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Zhejiang Medical Science and Technology Project, grant number 2022507093, 2021435142 and 2024KY230, and Health and Technology Project of Hangzhou, grant number ZD20210043 and A20210162.