
Abstract
Pediatric cardiac surgeries involving aortic arch reconstruction are complex and require long cardiopulmonary bypass (CPB) times with deep hypothermic circulatory arrest (DHCA). Selective perfusion techniques have been developed to prevent the deleterious consequences of DHCA associated hypoperfusion. The effectivity of low body perfusion through cannulation of the femoral artery with an arterial sheath remains to be elucidated. We compared perfusion and inflammation in patients receiving selective antegrade cerebral perfusion (ACP) only to low body perfusion (LBP) in addition to ACP during DHCA for aortic arch reconstruction surgery. There was no difference in patient characteristics, cardiac pathologies, or performed procedures between ACP and LBP groups. Lactate levels increased after cardiac arrest in both groups. However, lactate levels were lower after 1 h reperfusion, at the end of extracorporeal circulation (ECC), and after surgery in LBP group compared to ACP only. Furthermore, creatinine was increased in ACP group on postoperative day 1 compared to LBP group but no acute kidney injury was observed in any group. IL-6 concentration increased in ACP group, while remained unchanged in LBP group compared to pre surgical values and were significantly lower compared to ACP group on postoperative days 1 and 2. LBP via an arterial sheath during cardiac arrest for aortic arch reconstruction surgery in addition to ACP, improves post ECC tissue perfusion as indicated by lower lactate levels and reduces creatinine levels suggesting milder kidney injury. LBP seems to prevent postoperative inflammation through a reduction in procedural duration or enhanced perfusion and thereby improves the outcome after aortic arch reconstruction surgery.
Keywords
Introduction
Congenital heart defects (CHDs) affect 1% of live births, are associated with lifelong comorbidity, and frequently require repeated cardiac surgery procedures.1–3 Pediatric cardiac surgeries are complex and established only at specialized centers in each country. 4 Perioperative mortality and morbidity including neurological consequences have always been a concern for pediatric cardiac procedures and are related to post interventional hypoperfusion including low cardiac output syndrome, inflammation, and end-organ dysfunction.2,5
Anesthesia management and cardiopulmonary bypass (CPB) techniques during congenital cardiac surgeries differ between institutions to a significant extent. 6 With increases in pathophysiological knowledge and technological development in extracorporeal circulation (ECC), more sophisticated perfusion strategies and procedures have been developed, resulting in improved perioperative outcomes in this special group of patients.7–10 Hereby, surgeries requiring deep hypothermic circulatory arrest (DHCA) have mostly disappeared, apart from procedures involving reconstruction of the aorta.
Surgeries involving aortic arch reconstruction are complex, require long CPB times with DHCA, resulting in increased lactate levels and release of inflammatory mediators, thus leading to intra- and postoperative complications including neurological and end-organ dysfunction. Therefore, these complex interventions are representing a particular challenge for the entire team including the surgeon, the anesthesiologist, the perfusionist, and the intensivist after the surgical procedure.
Various selective perfusion techniques have been developed to prevent the deleterious consequences of DHCA-associated hypoperfusion including selective antegrade cerebral perfusion (ACP) in order to improve neurological outcomes.5–9 In addition to brain protection, ACP has been shown to decrease lactate levels, reduce the need for inotropic support and intensive care therapy, and prevent acute postoperative kidney injury after pediatric cardiac surgeries requiring DHCA.11–14
Hypothermia, inflammation, decreased renal and non-pulsatile blood flow are all present during CPB and may cause acute kidney injury (AKI), a common complication after pediatric cardiac surgery.15,16 Recently, in addition to ACP low body perfusion strategies have been described to prevent the deleterious consequences of DHCA on end-organ dysfunction. The results of improved perfusion seems to reduce lactate levels and incidence of kidney damage, potentially preventing intestine and kidney from the deleterious consequences of DHCA-associated hypoperfusion.5,17,18
However, low body perfusion techniques differ substantially between centers and include intraoperative aortic cannulation through the anastomosis or infradiaphragmatic cannulation of the abdominal aorta. Recently, Boburg et al. 19 reported a sufficient and save low body perfusion strategy through the insertion of an arterial sheath into the femoral artery during aortic arch reconstruction.
CPB is associated with an expression of inflammatory mediators, including interleukin-6 (IL-6), potentially resulting in systemic inflammatory response syndrome (SIRS) including vascular damage, increased endothelial permeability, edema, impaired oxygenation, and finally multiple organ dysfunction.20–23 Systemic inflammation in newborns during the crucial time of developmental placidity is highly relevant, potentially leading to persistent neurological, cardiovascular, and pulmonary consequences.24–26 Although CPB is inducing an increase in inflammatory mediators through exposure of the blood to the bypass circuit and non-pulsatile flow, ECC has been shown to reduce the increase in inflammatory mediators through improved perfusion and gas exchange accordingly. 27
However, the effectivity of low body perfusion through an arterial sheath cannulation, potentially improving abdominal tissue and organ perfusion, resulting in a reduction of inflammation, protecting abdominal organs, remains to be elucidated. Therefore, the present retrospective analysis aimed to compare the effectiveness of low body perfusion through cannulation of the femoral artery to selective ACP alone in preventing hypoperfusion post DHCA.
Patients and methods
Groups
After approval form the Ethics Committee at the University Hospital Bonn, Germany (No. 201/17, Chair Professor Kurth Racke), and in accordance to the Declaration of Helsinki and §15 of the Medical Association Nordrheins’ professional code of conduct, we performed a retrospective analysis of all pediatric cardiac surgeries involving aortic arch reconstruction using cardiopulmonary bypass at the University Medical Center Bonn, Germany, between March 2013 and May 2017. Perfusion technic for 14 patients that were treated between Mach 2013 and November 2016 was selective antegrade cerebral perfusion (ACP) during deep hypothermic cardiac arrest. Ten patients that were treated between December 2016 and May 2017 received low body perfusion (LBP) using femoral artery cannulation in addition to ACP during deep hypothermic circulatory arrest. All surgeries were performed by the same team of pediatric cardiac surgeons, perfusionists, pediatric cardiac anesthesiologists, and pediatric cardiac intensivists.
Anesthesia
After applying standard monitoring, including electrocardiography, blood oxygen saturation (SpO2), and blood pressure, anesthesia was induced using sufentanil, etomidate, and rocuronium. Subsequently, patients were intubated using a protex tube and ventilated. Cerebral oxygenation (rScO2) was monitored using near-infrared spectroscopy (NIRS) (Medtronic/Covidien INVOS™ and cerebral electric activity was assessed using a bisprectral index (BIS) monitor (Version XP, BIS version 4.0, Medtronic Inc, Dublin, Ireland). Anesthesia was maintained with sufentanil and sevoflurane. Subsequently, a central line was inserted via ultrasound visualization through the right central jugular vein and the right radial artery was cannulated for invasive blood pressure measurement. During cardiopulmonary bypass sevoflurane was administered through the extracorporeal circulation according to recommendations from the German society of anesthesiology. Arterial blood gases (blood gas analysis (BGA)) were analyzed throughout the surgery and at changes of perfusion strategies.
Selective antegrade cerebral perfusion (ACP)
After induction of anesthesia and thoracotomy the arterial perfusion cannula was inserted into the truncus brachiocephalicus or ascending aorta if feasible, while the venous canula was inserted through the right atrium into the vena cava inferior. ECC was established starting at a perfusion rate of 2.8 l/m2 body surface area (BSA) and patients were cooled to a temperature of 18°C −20°C. Subsequently, the aorta was cross-clamped and Bretschneider cardioplegic solution administered through an aortic needle vent. During DHCA the perfusion rate of the extracorporeal circulation was reduced and continuous ACP was achieved during reconstruction starting at a perfusion rate of 0.42–0.56 l/m2 BSA/min. ACP was monitored through the right radial arterial cannulation and 50 mmHg blood pressure was targeted, while the target value for cerebral oxygenation was less than 20% reduction of pre-anesthesia rScO2 values.
Low body perfusion (LBP)
After induction of anesthesia, an additional arterial sheath was percutaneously inserted into the femoral artery under sterile conditions and via ultrasound visualization. In addition to regional cerebral oxygenation, a NIRS electrode was placed over the right kidney to assess regional splanchnic tissue oxygenation. After arterial and venous cannulation for ECC the femoral arterial line was connected through a high-flow three-way stopcock to achieve low body perfusion (LBP) throughout cardiac arrest. Perfusion was established starting at a perfusion rate of 2.8 l/m2 body surface area (BSA). Subsequently, patients were cooled to a temperature of 26°C. After cross-clamping and administration of Bretschneider solution to induce cardiac arrest, the ECC was reduced and combined ACP via the perfusion cannula and LBP via the arterial line was achieved during reconstruction starting at a perfusion rate of 0.42–0.56 l/m2 BSA/min. ACP was monitored through the right radial arterial cannulation and 50 mmHg blood pressure was targeted, while the target value for cerebral oxygenation were less than 20% reduction of pre-anesthesia rScO2 values. LBP pressure was monitored via a three-way stopcock prior to the arterial cannulation. The target value for regional splanchnic oxygenation were pre-anesthesia rScO2 values. Perfusion was directed from ACP to LBP using a clamp on the arterial cannula. Lactate levels were closely monitored to determine if low body perfusion was effective.
After reconstruction of the aortic arch, whole body perfusion was resumed through a switch of the aortic cannula from aortic root or truncus brachocephalicus to the enlarged aortic arch. Lactate as well as creatinine levels were monitored post-surgery and during the ICU treatment as markers of splanchnic and renal ischemia. Furthermore, IL-6 was assessed during ICU treatment to evaluate systemic inflammation post CPB. After the surgery, lower extremities were examined and compared for signs of potential ischemia caused by the arterial sheath. Surrogate parameters for tissue perfusion, like re-capillarization, tibial and fibular artery pulse, and skin color did not differ between legs while the cannula still was inserted.
The sheath was removed during the first 6 h upon ICU admission and patients were examined at least three times a day for clinical signs of mal-perfusion (re-capillarization, tibial and fibular artery pulse, and skin color).
Statistical analysis
Statistical analyses were performed using the Prizm 8 (GraphPad Software, La Jolla, CA). The chi-square test was used to compare distributions between groups and normal distribution was confirmed using the Kolmogorov–Smirnov test. Data were analyzed using unpaired t test or restricted maximum likelihood model (REML) for time courses. Data are presented as mean ± standard deviation. No power analysis has been performed due to the retrospective nature of the study.
Results
Patient cohort
The present retrospective study included a total of 24 children who underwent pediatric cardiac surgery for aortic arch reconstruction using cardiopulmonary bypass at the University Hospital Bonn, Germany. Perfusion technic for 14 patients was antegrade cerebral perfusion (ACP) during deep hypothermia circulatory (DHCA) arrest only. The remaining 10 patients received low body perfusion during circulatory arrest via an arterial sheath through the femoral artery in addition to ACP during aortic arch reconstruction surgery.
Patient characteristics
Patient characteristics including age, weight, height, BSA, and gender were compared between ACP and LBP groups. Statistical analyses indicated that age, weight, height, and BSA were not different between ACP and LBP groups (Table 1). Furthermore, presurgical cardiac pathologies included hypoplastic or aplastic aortic arch, hypoplastic left heart syndrome, transposition of the great arteries, atrial, and ventricle septum defects. Statistical analyses indicated that distribution of pathologies was not different between ACP and LBP groups (Table 1).
Patient characteristics, diagnoses, and surgeries. Baseline demographics.

Surgeries and CPB settings
Patients from both groups received aortic arch reconstruction surgery, either as the main surgery or within a complex procedure. Performed procedures included Norwood type surgery, aortic arch reconstruction, and transposition of the great arteries with aortic arch reconstruction. Statistical analyses indicated no difference in performed procedures between ACP and LBP groups (Table 2).
Patient characteristics, diagnoses, and surgeries. Intraoperative variables.

Durations of cardio-pulmonary-bypass (CPB), aortic cross-clamping (AoX), circulatory arrest (CA), reperfusion, and (ACP) were retrieved from the operative records. AoX, CPB, CA, and ACP durations were all significantly shorter in the LBP group, compared to ACP group. Temperature during circulatory arrest was lower in ACP, compared to LBP group according to the respective perfusion protocol. Reperfusion times were not different between groups (Table 2).
Metabolism and inflammation
Perioperative lactate concentrations were assessed after induction of anesthesia, at specific timepoints during surgery, and during ICU treatment. Statistical analyzes indicated no difference in pre surgical lactate concentrations before or after CA. However, lactate levels were significantly higher in ACP group after 1 h reperfusion, after ECC, and post-surgery compared to LBP group (Figure 1).

Patients receiving low body perfusion (LBP) via an arterial sheath in addition to antegrade cerebral perfusion (ACP) during aortic arch reconstruction surgery in circulatory arrest exhibited lower arterial lactate concentrations after 1 h reperfusion, at the end of extracorporeal circulation (ECC), and after surgery (post OP), compared to ACP only. n = 10 LBP, n = 14 ACP.
Creatinine and IL-6 levels were assessed the day before surgery, upon ICU admission, and during ICU treatment. Statistical analyses indicated no difference in creatinine levels between groups in the pre- and early postoperative phase. Nevertheless, creatinine levels were significantly higher at postoperative day 1 in ACP compared to LBP group (Figure 2). However, Urine output per body weight was not different between groups and no patient had renal failure requiring dialysis.

Creatinine concentration was lower in patients receiving low body perfusion (LBP) via an arterial sheath in addition to antegrade cerebral perfusion (ACP) during aortic arch reconstruction surgery in circulatory arrest 1 day after surgery, compared to ACP only. n = 10 LBP, n = 14 ACP.
IL-6 levels were also not different between groups in the pre- and early postoperative phase. However, IL-6 level significantly increased at days 1 and 2 in ACP group compared to pre-surgical concentration. In contrast, IL-6 concentration remained unchanged after surgery in LPB group and were significantly lower compared to ACP group on postoperative days 1 and 2 (Figure 3). Neither creatinine, not IL-6 levels were different 3 days after surgery between groups.
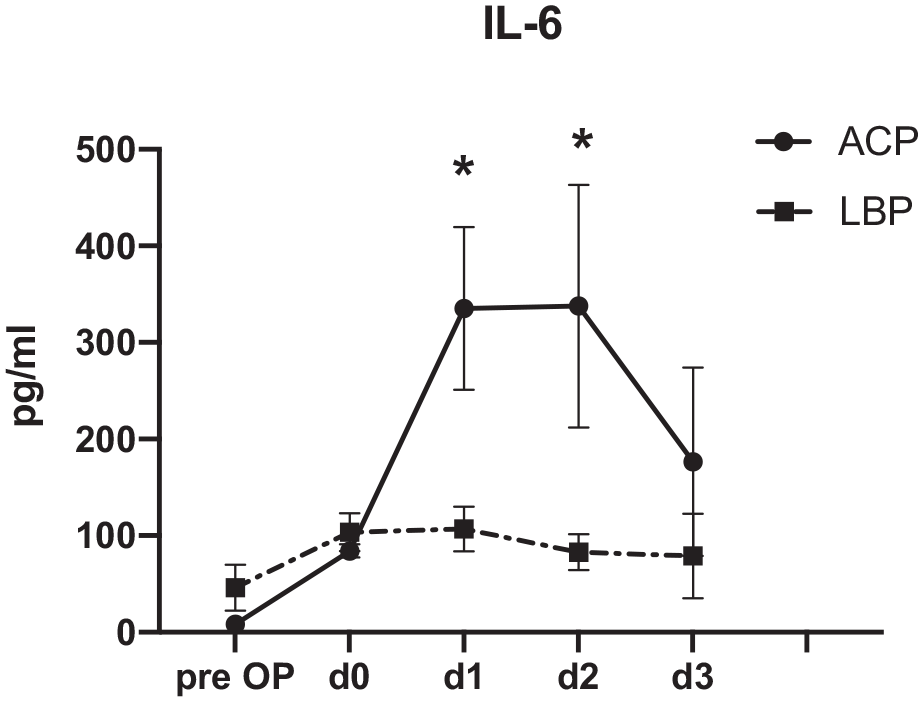
Patients receiving Low-Body-Perfusion (LBP) via an arterial sheath in addition to antegrade cerebral perfusion (ACP) during deep circulatory arrest for aortic arch reconstruction surgery exhibited lower IL6 serum concentration postoperative days 1 and 2 compared to antegrade cerebral perfusion only. n = 10 LBP, n = 13 ACP.
Discussion
The hemodynamic management and perfusion strategies for surgeries involving reconstruction of the aortic arch, have been modified over the last years to avoid the potential deleterious consequences of deep hypothermic circulatory arrest (DHCA) and improve outcomes.7–9,28 Selective ACP during DHCA has become the standard perfusion regime to prevent deleterious cerebral consequences and improved neurologic outcomes after pediatric cardiac surgeries requiring DHCA.
Boburg et al. 19 described the safety of lower body perfusion via an arterial sheath through the femoral artery. In accordance with the initial report of this technique we have not seen any complication after removal of the sheath in the context of vessel injury or hematoma, confirming that low body perfusion can safely be performed via an arterial sheath that is percutaneously inserted into the femoral artery under sterile conditions and ultrasound visualization.
Although cerebral perfusion techniques have improved neurological outcomes, hypoperfusion is still present for a substantial part of the body during the surgery as seen through elevated lactate levels during reperfusion and early postoperative recovery. Lactate is a commonly used biomarkers to detect poor organ perfusion 29 and various studies indicated that lactate levels correlate with prognosis in critically ill patients. 30 To evaluate LBP associated improved perfusion, we assessed procedural lactate levels. Our data show that lactate levels were increased in patients that received ACP and LBP during CA. However, lactate levels were significantly lower in LPB group compared to ACP group 1 h after begin of reperfusion, at the end of CPB, and at the end of the surgery, compared to ACP group, suggesting that LBP through an arterial sheath sufficiently improves lower body perfusion during aortic arch reconstruction performed in CA.
Elevated creatinine levels are commonly seen after aortic arch reconstruction surgery indicative of hypotension associated kidney injury and the prevention of acute kidney injury has improved survival after pediatric cardiac surgery.31,32 Our data indicate that creatinine levels were lower in patients that received LBP in addition to ACP during CA for aortic arch reconstruction surgery, suggesting that LBP via an arterial sheath sufficiently improved kidney perfusion, potentially improving postoperative outcomes.
Inflammation is a major concern after ECC and IL-6 concentrations correlate with length of surgery and hospital stay after open heart surgery. 33 The present study shows that ECC duration and IL-6 levels were lower in patients that received LPB in addition to ACP during cardiac arrest, potentially improving outcomes after aortic arch reconstruction surgery. However, it remains unclear whether reduction in IL-6 is caused by improved lower body perfusion or secondary to a reduction in procedure times.
There are several limitations including the retrospective nature, a low patient number, and comparing two different treatments with data not being powered for have to be considered interpreting our results. Also, a treatment change with selective antegrade cerebral perfusion (ACP) only being the standard procedure during the first part to low body perfusion (LBP) in addition to ACP during DHCA being the standard treatment during the subsequent part of the observational period.
Conclusion
In summary, our data support that LBP during deep circulatory arrest for aortic arch reconstruction surgery in addition to ACP, improves post ECC tissue perfusion as indicated by lower lactate levels, reduces creatinine levels suggesting milder kidney injury, and prevents post procedural inflammation through a reduction in procedural duration or enhanced perfusion, all potentially improving outcomes after aortic arch reconstruction surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Anesthesiology, University Hospital Bonn, Germany.
Ethics approval
Ethical approval for this study was obtained from Ethics Committee at the University Hospital Bonn No 201/17.
Informed consent
Has been waived from the Ethics Committee due to the retrospective nature.
Trial registration
This randomized clinical trial was not registered due to the retrospective nature.