
Abstract
Background
Dermatomyositis (DM) is an idiopathic immune-mediated myopathy, and may involve many organs, including muscles, skin and lungs. Myositis-specific autoantibodies (MSAs) are a useful aid in diagnosis DM and identifying its clinical subtype. During the COVID-19 pandemic, several studies found clinical similarities regarding lung involvement in both COVID-19 and DM. Such similarities have prompted speculation of a common pathogenetic mechanism. Indeed, viral infections are well-known triggers of autoimmune diseases. This prompted us to investigate whether circulating MSAs could be markers of the severity of lung involvement and of clinical outcome in COVID-19 patients. Moreover, we investigated the presence of cutaneous signs of DM in COVID-19 patients.
Methods
We conducted a retrospective cohort study on 178 hospitalized patients affected by COVID-19. The diagnosis was confirmed by naso-pharyngeal swab positivity for SARS-CoV-2. The severity of lung involvement was assessed by assigning to each patient a radiological score ranging from 1 to 4, based on chest imaging (chest X-rays or CT scans). Serum samples were tested for MSAs.
Results
Anti-PL-7 antibodies were detected in 10.1% of patients and were found to be associated with an increased risk of severe pulmonary involvement (p = 0.019) and a worse prognosis in COVID-19 patients. Cutaneous lesions were observed in 26.4% of patients. However, none were cutaneous manifestations of DM.
Conclusions
The detection of anti-PL7 antibodies might predict severe pulmonary involvement and a worse prognosis in COVID-19 patients.
Keywords
Introduction
Dermatomyositis (DM) is an immune-mediated idiopathic inflammatory myopathy (IIM). IIM is a group of rare and clinically heterogenous connective tissue diseases that are characterized by the inflammation of many organs and tissues, including muscles, skin and lungs. 1 Dermatological signs of DM comprise: periorbital heliotrope rash, purplish papules and plaques in the dorsal region of the metacarpo-phalangeal or interphalangeal joints (Gottron's papules), fissured palmar fingertips (mechanic's hands), and erythema of the face, chest (V-sign) and back (shawl sign). 1 By contrast, skin manifestations of Coronavirus Disease 2019 (COVID-19) include chilblain-like lesions, maculo-papular eruptions, urticarial eruptions, vesicular eruptions, erythema multiforme (EM)-like lesions, livedo and necrosis. 2 Other skin findings in COVID-19 patients have been described in association with a multisystem inflammatory syndrome in children (MIS-C) and, rarely, with a multisystem inflammatory syndrome in adults (MIS-A). 2 Other manifestations, such as pityriasis rosea or shingles, have also been reported.2,3 Similar cutaneous manifestations have also been reported after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccination.4,5 Typically, in DM the proximal muscles of the upper and lower limbs are affected. In some cases, pulmonary involvement may lead to nonspecific interstitial pneumonia (NSIP). 6
Myositis-specific autoantibodies (MSAs) are useful tools for the diagnosis and classification of DM. Indeed, various MSAs are described in association with specific clinical phenotypes of DM. 6 Specifically, anti-melanoma differentiation-associated gene 5 (anti-MDA5) antibodies are associated with more aggressive and rapidly progressive lung involvement, higher mortality and the absence of myopathy. 1 Other specific MSAs, including anti-synthetase antibodies, anti-histidyl-tRNA synthetase antibody (anti-Jo1), anti-threonyl-tRNA synthetase (anti-PL7), anti-alanyl-tRNA synthetase (anti-PL12), anti-isoleucyl-tRNA synthetase (anti-OJ) and anti-glycyl-tRNA synthetase (anti-EJ), are associated with the anti-synthetase antibody syndrome, which is characterized by severe interstitial lung involvement, high fever, myositis, polyarthritis and absence of cutaneous signs. 7
During the COVID-19 pandemic, cases of overlap between COVID-19 and DM were described in several case reports.8–15 Moreover, a recent retrospective study revealed a strong temporal relationship between DM symptoms and COVID-19 infection or vaccination in patients with DM evaluated in a rheumatology clinic during the pandemic. 16 Cases of DM following COVID-19 or COVID-19 vaccination have been reported.17,18 Notably, lung involvement in SARS-CoV2 pneumonia may resemble the interstitial pneumonia and the ground glass opacifications found in patients affected by DM with circulating anti-MDA5 antibodies. 19 Similar features of pulmonary involvement in these two diseases have prompted speculation that they share a common pathogenetic mechanism. Although the pathogenesis of DM is still unclear, it is likely to be associated to abnormal complement activation and excessive type-I interferon (IFN) release. Indeed, it has been found that the cytokine cascade in COVID-19 is similar to that observed in DM, and that it involves various cytokines, including interferon-gamma (INF-γ), interleukin 8 (IL-8) and monocyte chemoattractant protein-1 (MCP-1). 20 Furthermore, IFN has proved to be involved in organ damage in COVID-19 patients, and also to play a major role in damage to muscle fibers in DM. 21 Megremis et al. identified three immunogenic linear epitopes with high sequence identity to SARS-CoV-2 proteins in patients with autoimmune DM. 22 It can therefore be speculated that exposure to SARS-CoV-2 may trigger the development of DM.
The prevalence of circulating MSAs in COVID-19 patients has not yet been thoroughly investigated. Since specific types of MSAs are associated to lung involvement in patients affected by DM, given the similarities of pneumonia in COVID-19 patients and DM patients, and considering the reported cases of DM following COVID-19 or SARS-CoV-2 vaccination, we decided to investigate whether circulating MSAs and myositis-associated antibodies (MAAs) could be markers of the severity of lung involvement and of clinical outcome in COVID-19 patients. Moreover, we investigated whether these patients presented cutaneous signs of dermatomyositis.
Methods
Study population
We conducted a retrospective cohort study on patients affected by COVID-19 who were hospitalized between March and May 2020 at the Ospedale Policlinico San Martino IRCCS, in Genoa, Italy. All patients tested positive for SARS-CoV-2 on nasopharyngeal swab samples and clinically presented full-blown COVID-19. No other specific inclusion or exclusion criteria were adopted in selecting the sample. Demographics, pre-existing comorbidities and the course of the disease during hospitalization were studied by retrospectively analyzing clinical records. All patients were investigated for cutaneous manifestations of DM and COVID-19. Local ethics committee approval was obtained (N. CER Liguria 521/2020). Since the study was conducted during the COVID-19 global pandemic and was retrospective, we encountered difficulties in collecting written informed consent from all patients. Our study complied with the “Standards for reporting qualitative research (SRQS)” guidelines. 23
Radiological assessment
The patients’ pulmonary involvement was assessed by means of either chest X-rays or computed tomography (CT) scans, performed during hospitalization. Chest CT scan images of all patients were not available, as only chest X-rays were mainly performed at the beginning of the pandemic, owing to the simplicity and rapidity of the method. In order to evaluate the severity of lung involvement, we created an ad hoc radiological severity score based on the literature24–28; this was used to evaluate both X-rays and CT scans.
The radiological score ranged from 1 to 4, as follows (Table 2): • 1: No focal parenchymal lesions • 2: Nuanced parenchymal thickening • 3: Extensive bilateral lung parenchymal thickening • 4: Ground glass opacities
Laboratory analysis
Frozen serum samples, which were used for MSA and MAA titration, were obtained within the first 10 days of the patients’ hospitalization. Other abnormalities in laboratory parameters were also evaluated on the same serum samples. Line blot assay (EUROLINE Profile Autoimmune Inflammatory Myopathies 16 Ag (IgG); Euroimmun Mediziniske Labordiagnostika, Germany) was used to detect MSAs [anti-OJ, anti-EJ, anti-PL-12, anti-PL-7, anti-signal recognition particle (anti-SRP), anti-Jo-1, anti-small ubiquitin-like modifier activating enzyme 1 (anti-SAE1), anti-nuclear matrix protein 2 (anti-NXP2), anti-MDA5, anti-transcriptional intermediary factor 1-γ (anti-TIF1-γ), anti-Mi-2β and Mi-2α antibodies] and MAAs (anti-Ro-52, anti-Ku, anti-polymyositis/Scl (PM-Scl) 75 and anti-PM-Scl-100) The line blot assay for MSA detection has proved valid for MSA in several unrelated studies.29–32 The specificity of this test ranges between 97% and 100%. 32
Results were expressed as arbitrary units, with a cut-off positivity according to the manufacturer’s instructions.
Statistical analysis
Continuous variables were summarized as mean values with standard deviation and median values with range. Categorical data were expressed as frequencies and percentages. The radiological score was categorized as “normal” or “mild” if both lungs had a radiological score <4, and as “severe” if the radiological score was ≥4. Univariate and a subsequent logistic regression model were run to identify autoantibodies that predicted worse radiological scores, after adjusting for age and sex.
Results
Baseline and clinical characteristics.

Results are reported as mean ± standard deviation and median with range or frequency and percentage.
Univariate and multivariate binary logistic regression model for identifying autoantibodies predicting severe radiological score.

Results are reported as count with frequency and percentage. The analysis has been adjusted for age and sex.
Score Legend: 1- No focal parenchymal lesions; 2 - Nuanced parenchymal thickening; 3-Extensive bilateral lung parenchymal thickening; 4- Ground glass opacities.
Anti-OJ: anti-isoleucyl-tRNA synthetase; Anti-EJ: anti-glycyl-tRNA synthetase; Anti-PL-12: anti-alanyl-tRNA synthetase; Anti-PL-7: anti-threonyl-tRNA synthetase; Anti-SRP: anti-signal recognition particle; Anti-Jo-1: anti-histidyl-tRNA synthetase antibody; Anti-SAE1: anti-small ubiquitin-like modifier activating enzyme 1, Anti-NXP2: anti-nuclear matrix protein 2; Anti-MDA5: anti-melanoma differentiation-associated gene 5; Anti-TIF-1γ: anti-transcriptional intermediary factor 1-γ, Anti-PM-Scl-75: anti- polymyositis/Scl 75, Anti-PM-Scl-100: anti- polymyositis/Scl 100.

Anti-PL-7 antibody is the only myositis-specific autoantibody associated with an increased risk of a severe lung involvement. Anti-PL-7: anti-threonyl-tRNA synthetase.
Cutaneous manifestations in 178 patients.
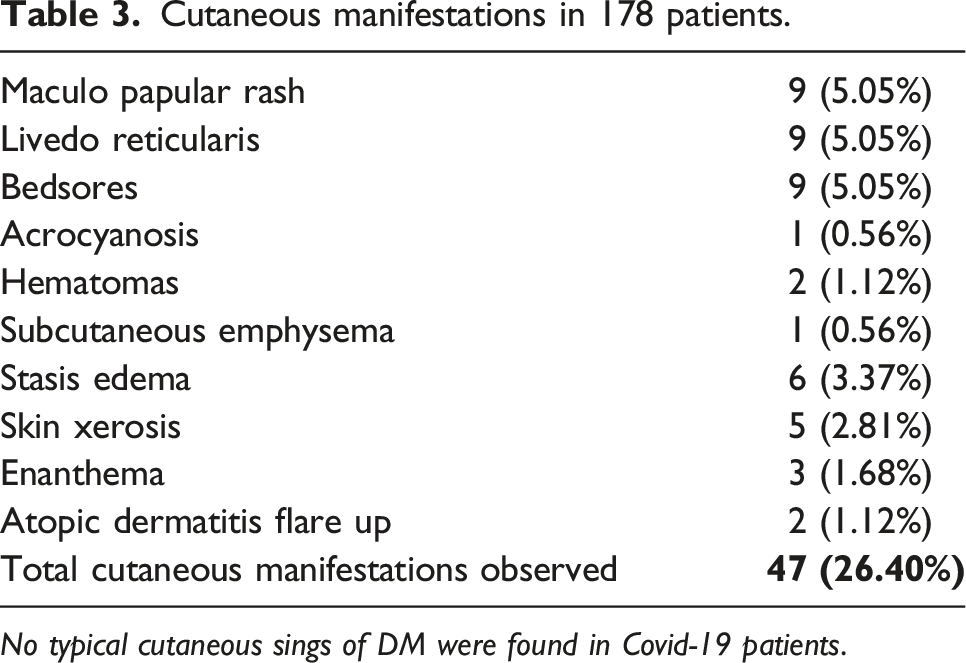
No typical cutaneous sings of DM were found in Covid-19 patients.
Discussion
The possible link between SARS-CoV-2 infection and autoimmunity has been reported in the literature. It is, indeed, well known that environmental factors, such as viral, bacterial and parasitic infections, may trigger or exacerbate autoimmune diseases, especially in genetically susceptible individuals. 33 In particular, autoimmunity can be induced by viruses in many ways: via molecular mimicry, epitope spreading, bystander activation and immortalization of infected B cells. For example, in chronic Epstein-Barr virus infection, the reactivation of the virus may be associated with the onset of various autoimmune diseases, including DM. 34
Furthermore, vaccination against SARS-CoV-2 has also been reported to trigger the onset of autoimmune conditions, including myocarditis, IgA vasculitis and autoimmune liver diseases. 35 Moreover, epidemiological data have shown that DM is mostly diagnosed at specific times of the year, with seasonal clustering, which suggests that viral or bacterial infections might be common triggers for DM. 36
In our study, we found several COVID-19 patients with positivity to MSAs. However, we did not observe skin manifestations typical of DM nor severe muscle involvement. On the other hand, the pulmonary involvement we observed in our patients hospitalized for SARS-CoV-2 pneumonia was very similar to that described in patients with DM, with a typical interstitial pattern.
Recently, cases of DM with anti-MDA5-associated autoantibodies and lung injury have been described in association with SARS-CoV-2 infection or vaccination.36–38 Anti-MDA5 autoantibodies are typically associated with an amyopathic or hypomyopathic form of DM, extensive and rapid lung involvement and a poor prognosis.1,39 Moreover, a few cases of anti-synthetase antibody syndrome with severe pulmonary involvement following SARS-CoV-2 infection have also been reported.40,41 A recent case series collected 12 cases of middle-aged women affected by anti-synthetase syndrome, in whom SARS-CoV-2 infection triggered a flare of their underlying autoimmune condition. 42 Three of the 12 patients had circulating anti-PL-7 autoantibodies and radiological sings of NSIP and ground glass opacities. 41 A case of anti-synthetase syndrome that occurred after SARS-CoV-2 infection was also reported a in a 62-year-old man with positive anti-Jo1 autoantibodies. 40 Recently, in patients referred to an immunology department for IIM, Garcia-Bravo et al. observed a higher prevalence of MSAs during the COVID-19 pandemic and the SARS-CoV-2 vaccination period than in the three years prior to the pandemic. 43 MSAs were associated to the HLA DRB1* risk allele. 38 Differential profiles of MSA specificity were observed: mainly anti-MDA5 in 2020 and anti-RNA-synthetases in 2021. Thus, the authors also hypothesized that the increased cases of anti-MDA5 positivity observed in 2020 could be attributed to recognition of the coronavirus through RNA sensors, inducing an antiviral response by producing INFs and TNF. By contrast, in 2021, the increased incidence of detection of anti-PL-7 and anti-PL12 antibodies could suggest that SARS-CoV-2 vaccination might induce a reaction against Spike 1 proteins and other tissue antigens. 43 However, the possible association between a specific antibody positivity and the severity of the COVID-19 patient’s prognosis had not yet been investigated.
Our study documented a close link between positivity for the myositis-specific antibody anti-PL-7, the severity of pulmonary involvement in COVID-19 patients and their poor prognosis. Indeed, not only was anti-PL7 the most commonly detected MSA (18/178 patients); it was also associated with a much higher risk of severe lung injury. By contrast, no association was found between other MSAs and an increased risk of severe lung injury.
Severe cases of SARS-CoV-2 pneumonia are associated to a massive inflammatory cascade.20,44 It is possible that the inflammatory cascade induced in severe cases might also non-specifically trigger autoimmunity, which can result in full-blown DM or, in some cases, in a subclinical epiphenomenon of circulating autoantibodies. This hypothesis could possibly justify our findings.
The cutaneous manifestations we observed in 26.40% of patients mainly consisted of maculo-papular rashes, livedo reticularis, bedsores and acrocyanosis. These skin signs were probably attributable to nonspecific manifestations of vasculopathy in the context of a systemic viral infection, rather than to autoimmune processes. 45
Limitations
The main limitation of the present study was the absence of a control group of healthy individuals. Another limitation concerned the different types of radiological imaging analyzed. Indeed, owing to health emergency issues, not all patients underwent a chest CT scan. Furthermore, no data on previous autoimmune pathology or serology of our patients were available. Lastly, no sample size/power analysis was performed in this study, owing to its retrospective design and the low number of available sera collected during the pandemic.
Conclusion
On the basis of our findings, MSAs are not associated to cutaneous manifestations of DM in COVID-19 patients. However, positivity for anti-PL-7 antibodies were found to be associated to more severe pulmonary involvement and a worse prognosis in COVID-19 patients. It might be useful in the future to evaluate anti-PL7 antibody positivity in COVID-19 patients when making a prognosis. It would also be interesting to investigate other possible associations between dermatomyositis, autoimmune diseases and SARS-CoV-2 infection.
Footnotes
Author contributions
G.A.O.: conceived of the presented idea, contributed to the analysis of the results and to the writing of the manuscript. P.C.: carried out the line blot assays; E.C.C.: supervised and directed the project. G. G.: contributed to the analysis of the results and to the writing of the manuscript. A. G.: developed the radiological score and evaluated the chest X-rays and CT-scans; L. R.: developed the radiological score and evaluated the chest X-rays and CT-scans; I. S.: performed the statistical analysis. A.P.: supervised and directed the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.