
Abstract
Primary prostate lymphoma (PPL) is rare. This article reports a case of PPL by retrospective analysis of the clinical data and review of the literature, in an attempt to explore the diagnosis, treatment, and prognosis of this rare disease. The present case involves a male patient who came to our hospital for medical consultation of dysuria. Serum prostate-specific antigen (PSA) was not remarkable. Pelvic computed tomography (CT) scan suggested obvious enlargement of the prostate and a tumor in the prostate, but the tumor was not significantly enhanced on contrast-enhanced CT scan. Ultrasound suggested obvious enlargement of the prostate with multiple local low-density echoes and rich blood flow signals inside. Histopathology of prostate biopsy suggested prostate diffuse large B-cell lymphoma (DLBCL). The patient refused chemotherapy but agreed to receive radiotherapy. After radiotherapy, the tumor became smaller and the International Prostate Symptom Score (IPSS) score was reduced. Our experience, together with literature review, suggests that prostate puncture biopsy is an important method for the diagnosis of PPL, and imaging examination can assist the diagnosis. Radiotherapy is able to reduce the tumor volume and relieve the symptoms of urinary tract obstruction, and chemotherapy can help achieve a better therapeutic outcome.
Introduction
Lymphoma is defined as a group of malignant tumors originating from lymph nodes or lymphatic tissues. Pathologically, lymphoma is classified as Hodgkin’s disease (HD) and non-Hodgkin’s lymphoma (NHL), with the latter more frequently seen. Prostate lymphoma is rarely seen in the urogenital tract. Researchers in other countries reported that most cases of prostate lymphoma are NHL, accounting for about 0.1%. 1 According to tumor origin, prostate lymphoma is classified as primary and secondary, with the former even more rarely seen. 2 Large B-cell lymphoma is the main pathologic type of primary prostate lymphoma (PPL). 3 Most related cases reported in the literature were individual case reports, 3 and therefore, there is a lack of systematic and comprehensive study on the clinical characteristics, imaging diagnosis, treatment, and prognosis of PPL. This article reports a case of PPL by retrospective analysis of the clinical data and imaging findings in the context of literature review in an attempt to explore the diagnosis, treatment, and prognosis of this rare disease.
Case report
An 80-year-old male patient was admitted in March 2010 because of urine frequency, urgency, and dysuria. He had been healthy without underlying diseases, hepatosplenomegaly, anemia, or other systemic symptoms and signs. Digital rectal examination (DRE) suggested third-degree prostate hyperplasia, with the central fissure disappearing. No nodule was palpated. Ultrasound showed bilateral enlarged cervical, supraclavicular, axillary, and inguinal lymph nodes but no deep ones. Specially, the ratio of lymphocytes in the peripheral blood was decreased. Serum prostate-specific antigen (PSA) was higher than 4 ng/mL. In November 2011, transurethral resection of the prostate (TURP) was performed, and the bilateral lobes of the prostate were found hyperplasic. About 50 g prostate tissue was resected, and postoperative pathology was consistent with the diagnosis of benign prostate hyperplasia (BPH). The patient was re-admitted in June 2014 because of dysuria, when DRE suggested prostate hyperplasia with the central fissure disappearing. The consistency was hard without tenderness. The hyperplasia was scored 21 according to the International Prostate Symptom Score (IPSS). PSA was lower than 4 ng/mL. Pelvic computed tomography (CT) scan suggested that the prostate was obviously enlarged with heterogeneous intensities and stippled calcifications inside, forming a prostate tumor invading the bilateral seminal vesicles (Figure 1(a)). Contrast-enhanced CT scan showed no significant enhancement of the tumor (Figure 1(b)). Urinary color ultrasound suggested obviously enlargement of the prostate that protruded to the urinary bladder. Multiple low-intensity local foci were detected with heterogeneous echoes inside. There were rich blood flow signals inside the low-intensity foci (Figure 2). No tumor was detected in other parts of the body by positron emission tomography (PET)/CT. Ultrasound-guided puncture biopsy of the prostate suggested malignant NHL of the prostate. Enzyme-linked immunosorbent assay (ELISA) tended to suggest large B-cell malignant lymphoma (Figure 3(a) and (b)). The patient refused chemotherapy but agreed to receive local radiotherapy with a 40 Gy dosage each cycle, totaling 22 cycles. Re-examination 6 months after radiotherapy showed that the patient’s condition was generally stable with an IPSS score of 15. Pelvic CT scan suggested that the prostate tumor became smaller (Figure 4).

(a) Pelvic CT suggests obvious enlargement of the prostate with heterogeneous intensities and stippled calcifications inside; the prostate tumor invades the bilateral seminal vesicles. (b) Contrast-enhanced CT scan shows no obvious enhancement of the tumor.
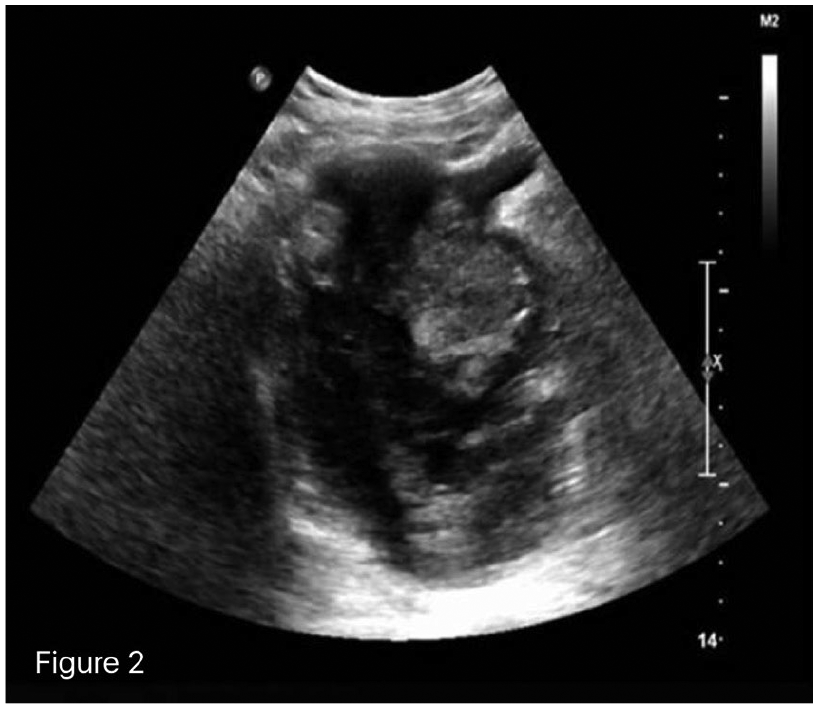
Urinary ultrasound suggests obvious enlargement of the prostate that protrudes to the urinary bladder; multiple low-intensity local foci are seen with heterogeneous echoes inside; rich blood flow signals are seen inside the low-intensity foci.

(a) directions of NHL of the surgery. (b) ELISA tends to suggest large b cell malignant Philippines.

CT reconstruction suggests that the tumor becomes smaller after radiotherapy as compared with that before radiotherapy.
Discussion
PPL is more frequently seen in old people, the mean age of the incidence of which is 62 years, while secondary lymphoma occurs in relatively young people. 3 The common clinical symptoms and signs include dysuria, urine frequency and urgency, anal pendant expansion, and difficult bowel movement. 4 The present case involved an 81-year-old male patient with a histopathologic diagnosis of prostate large B-cell malignant lymphoma. Some other studies reported that DRE often revealed prostate hyperplasia, hard consistency and disappearance of the central fissure, or nodules in some patients. 5 DRE of the present case suggested prostate hyperplasia, disappearance of the central fissure, and hard consistency without tenderness, which are consistent with the reports in the literature. In addition, an overview of the characteristics of the disease in large patient samples showed that serum PSA was usually within 4 ng/mL. 2 These clinical features are significant in assisting the clinical diagnosis of PPL. Previous studies in the literature also reported the presence of prostate tumors and prostate hyperplasia on pelvic CT imaging, 6 which are consistent with the findings in our case. Compared with CT and magnetic resonance imaging (MRI), some researchers believe that ultrasound remains a helpful tool for the diagnosis of PPL. 7 Urinary color ultrasound in our case suggested enlargement of the prostate that protruded to the urinary bladder; there were multiple low-intensity and heterogeneous local echoes, with rich blood flow signals inside.
The current treatment of PPL as reported in the literature is similar to that of other firms of lymphoma, mainly including chemotherapy, radiotherapy, and combined chemoradiotherapy, in addition to resection of the prostate tumor to relive the local symptoms. 8 The use of radiotherapy alone is rare, and combined chemotherapy or combined chemoradiotherapy is more commonly used. 9 Whitmore et al. 10 reported that although resection of the prostate tumor or TURP could relieve the symptoms of urinary tract obstruction, they were unable to improve patient survival. According to the guidelines of the National Comprehensive Cancer Network (NCCN) version 2015, combined therapy using cyclophosphamide + adriamycin + vincristine + prednisone is the treatment of choice. CT re-examination showed that the tumor became smaller than before, and the symptoms of dysuria were relieved to some extent. Presently, the patient’s condition is stable. Although the use of radiotherapy alone is rarely reported, our experience shows that it can relieve the symptoms of urinary tract obstruction.
It is generally recognized that the prognosis of PPL is relatively poor. Bostwick and Mann 11 reported the long-term follow-up observation of their 62 PPL patients, showing that the 1-, 2- and 5-year survival was 64%, 50%, and 33%, respectively. According to Ghose et al., 12 the prognosis of PPL is associated with the histologic type and tumor stage. As this study only included one case, more PPL cases are needed for further research and follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.