
Abstract
Keywords
Background
Intracerebral hemorrhage (ICH) usually occurs when blood pressure suddenly rises, which ruptures an artery to cause bleeding and accounts for about 30% of all strokes. 1 The symptoms appear suddenly during onset, which reach their peaks within minutes or hours from onset. If the treatment is delayed or not devised on time, the mortality rate could be very high.2,3 Former studies have illustrated that the inflammatory pathway functions importantly in the secondary brain injury after ICH, and lymphocytes are main inflammatory cells. 4 Lymphocyte subsets have a major role in adaptive immunity, which are the main immunological responses during brain injury. 5 Post brain injury, the infiltrating T lymphocytes (CD3lymphocytes) level increased and pro-inflammatory cytokines were secreted to aggravate inflammation. Immunosuppressants can reduce infiltrating T lymphocytes, alleviate immune response, inflammation, and brain edema. 6 Investigations report that CD4/CD8 T lymphocyte ratio in peripheral blood (PB) could be a valuable indicator to predict 30-day prognosis post ICH. 7 After surgical treatment, whether lymphocyte subsets in PB and cerebrospinal fluid (CSF) could be predictor for the critical ICH patient prognosis is not unraveled. During the development of some diseases, the T cells in the peripheral blood of patients have higher or lower levels of activated antigen (e.g., CD3, CD4, CD8) expressions. 8 CD3T cells represent the total number of mature T cells in peripheral blood, and their increased numbers indicate that the immune function of T cells is enhanced. CD4T cells are a subset of helper T cells which are called Th cells, and their increased numbers indicate that B cells produce more immunoglobulin to enhance cellular immunity. CD8 T cells are a subset of suppressive T cells, which are called Ts. They are cytotoxic cells (denoted by Tc), and their increasing numbers indicate enhanced immunosuppression. The ratio of CD4/CD8 cells indicates the functional balance between Th and Ts, which is the important index concerning internal environment of human immune system. If the ratio decreases, there would be decrement of the immune function in the bod. NK cells rapidly respond to sterile stimulus-like alarmins and chemokines released by the injured brain. Once being activated, NK cells have cytotoxic activity to produce cytokines and chemokines, by which they orchestrate other immune cells to limit or intensify immune responses. Thus, to assess the predictive values of lymphocyte subsets in PB and CSF, we prospectively collected and analyzed the changes in lymphocyte subsets. Relevant laboratory parameters regarding their clinical characteristics and 60-day outcomes in critical ICH patients post acute surgical treatment were analyzed. Current study is focus on patients with severe cerebral hemorrhage. The blood–brain barrier has been destroyed, and peripheral cells can enter the central nervous system (CNS). In the early stress state, a large number of inflammatory mediators are released into the blood and enter the CNS, which initiates early neuroinflammation. Central nervous T lymphocytes represent most immune cells (more than 80%) in the CSF of healthy individuals. There are T cells with different activation characteristics in the central nervous system. Depending on their location, number and persistence, and the context within the brain, same phenotypes may be associated with either deleterious or protective functions. CNS lymphocytes are critical for controlling a range of pathogens. When being overactivated, T cells could mediate brain injury through the uncontrolled release of pro-inflammatory cytokines and chemokines, which may have deleterious effects in both acute neuroinflammatory and neurodegenerative diseases. At the same time, because of the glial lymphatic circulation in the brain, we want to understand the correlation between extracranial and intracranial inflammatory factors (cells) and lymphocytes as well as their subgroups. The neuroinflammation after the blood–brain barrier is broken. Reaction and even glial lymphatic circulation provide some reference values. In this study, the prognostic value of cytokines, lymphocytes, and subsets between peripheral blood and intracranial cerebrospinal fluid behind the blood–brain barrier was explored 60 days after severe cerebral hemorrhage.
Methods
Patients selection
In this prospective study, we totally enrolled 69 patients with critical cerebral hemorrhage at the First Central Hospital of Baoding City, Hebei Province, China. All patients were admitted to neonatal intensive care unit (NICU), ventilator to assist breathing, and crossed underwent decompression of skull bone flap and/or ventricular drilling and drainage between January to July 2022. Inclusion criteria are as follows: (1) Computed tomography confirmed ICH including hypertensive intracerebral hemorrhage, spontaneous ICH and aneurysmal intracerebral hematoma; (2) patients were admitted and operated within 24 h after the disease occurs; (3) Laboratory tests in cerebrospinal fluid (CSF) and peripheral blood (PB) can be performed in 8 days after operation; (4) patient age was greater than 18 years. Exclusion criteria are: (1) traumatic cerebral hemorrhage, intracranial infection, or intracranial tumor hemorrhage; (2) presence of autoimmune disease or immunodeficiency disease; (3) preexisting critical infection in 1 month; (4) patient used steroids or immunosuppressants in recent 6 months; (5) patients with malignant tumors and blood system diseases; (6) the hospitalization duration in ICU <24 h; (7) family members are unwilling to be enrolled; (8) incomplete clinical, laboratory, or imaging data; (9) have missing follow-up data (Figure 1). Flowchart of patient enrollment.
The patients that involved are those with severe cerebral hemorrhage who were transferred to our department after emergency surgery within 24 h of onset. The surgical methods can be divided into four categories, which determined the groups of the patients. (1). Simple evacuation of intracerebral hematoma (using craniotomy or endoscopic evacuation of hematoma) or urokinase injection into the hematoma cavity for local drainage), (2). Intracerebral hematoma evacuation + ventricular drilling and drainage + decompressive craniectomy, (3). Intracerebral hematoma evacuation + ventricular drilling and drainage, (4). Intracerebral Hematoma evacuation + decompressive craniectomy. Only patients who underwent burr hole drainage were left with a ventricular drainage tube. The subjects of the study were patients with critical cerebral hemorrhage who had postoperative disturbance of consciousness and needed ventilator-assisted breathing (including spontaneous cerebral hemorrhage, hypertensive cerebral hemorrhage, aneurysmal cerebral hemorrhage, but excluding traumatic cerebral hemorrhage and other rare types). Preoperative routine examination includes blood routine examination, electrolytes, blood sugar, etc.
Ethic Committee Baoding First Central Hospital, Hebei approved the study protocols and that treatment methods that involved in present study (approval no. Kuai[2022]010). As the patients with cerebral hemorrhage admitted by NICU were judged to be too critical to provide effective consents, they were informed to sign the consent of the first-degree relatives of the patients authorized by law. This study was carried out in accordance with relevant regulations of Baoding First Central Hospital.
Laboratory parameter detections
For the same patient, the first lumbar puncture cerebrospinal fluid sample and the fasting peripheral venous blood sample (paired) in the morning of the same day are preferred. Blood routine + cerebrospinal fluid routine, blood biochemistry + cerebrospinal fluid biochemistry, blood lymphocyte subsets, and cerebrospinal fluid lymphocytes are performed. Detections focus on cell subsets (CD3T cell, CD3CD4T cell, CD3CD8T cell, CD4/CD8 ratio, CD3CD19B cell, CD3CD16CD56NK cell), blood Interleukin 6 (IL-6) and Cerebrospinal fluid IL-6, blood procalcitonin + cerebrospinal fluid procalcitonin (PCT). If the cerebrospinal fluid circulation channel is severely blocked and there are contraindications for lumbar puncture, and if the patient is indwelling a ventricular drainage tube at the same time, a cerebrospinal fluid sample is taken from the cerebrospinal drainage tube, and a peripheral blood sample is taken at the same time on the same day. If the patient does not indwell Ventricular drainage tube, we take the first lumbar puncture cerebrospinal fluid sample. All paired samples were the first cerebrospinal fluid sample + peripheral blood sample taken in the morning of the same day. Blood routine and biochemistry, cerebrospinal fluid biochemistry routine include those on CSF protein, CSF glucose, chlorine (Cl), WBC classification and count (×109/L), neutrophil absolute counts (×109/L), lymphocyte absolute counts (×109/L), monocyte absolute counts (×109/L), and red blood cell (RBC) count (×109/L). Neutrophil absolute counts/lymphocyte absolute counts (NLR) and monocyte absolute counts/lymphocyte absolute counts (MLR) were calculated. Multiparametric flow cytometry was used to identify and quantify cell types in CSF and PB.
Clinical characteristics
The baseline variables of critical ICH patients were collected, which included age, sex, smoking, drinking, hypertension on admission (systolic blood pressure (SBP), diastolic blood pressure (DBP)), admission time (hour) from onset, admission GCS score, before operation ICH score (ICH volume, Glasgow Coma Scale, origin of ICH (supratentorial or infratentorial), admission Acute Physiology and Chronic Health Evaluation II (APACHEII) score, first time of CSF test, coma, operation mode (trepanation, decompressive craniectomy), complication (such like bleed into ventricle, hernia, hydrocephalus, subarachnoid hemorrhage SAH) fever after surgery, inhalation pneumonia, previous medical history (including hypertension, diabetes, heart disease, stroke), and 60-day outcome.
Flow cytometry analysis
In this study, multi-platform flow cytometry (Sysmex Corporation, Shanghai, China) was employed to detect percentage of lymphocyte subsets in peripheral blood and cerebrospinal fluid of patients with severe cerebral hemorrhage. We utilized BD MultitestTM 6-color TBNK (BD Biosciences, USA, No. 19,194). The subsets include CD3T cells, CD3CD4T cells, CD3CD8T cells, CD4/CD8 ratio, CD3CD19B cells, and CD3CD16CD56NK cells. Multiparametric flow cytometry was used to identify and quantify cell types in CSF and PB. PB samples were collected and processed in parallel with CSF. CSF samples were obtained by lumbar puncture (LP) or ventricular drain without anticoagulant. Ethylenediaminetetraacetic acid (K3 EDTA 7.5%) PB samples were processed without adding preservatives. All samples were collected and sent to the laboratory immediately. Fresh cerebrospinal fluid samples processed within 30 min were subjected to lymphocyte subset detection and data were collected utilizing FACS Aria I cytometer (Becton Dickinson, USA). Absolute counts of lymphocyte subsets were gained utilizing FACS Diva software (BD Biosciences, USA), which were calculated by combining the percentage of lymphocyte subsets detected by flow cytometry with the absolute count of lymphocytes obtained in the same sample by an automated hematology analyzer. Roche automatic biochemical analyzer (Cobas 8000, Basel, Switzerland) was used to detect the biochemistry of peripheral blood and cerebrospinal fluid. The concentration of IL-6 was detected by the chemiluminescence method using the X8 automatic chemiluminescence instrument (Shenzhen New Industry, Shenzhen, China). The levels of serum immunoglobulin IgG, IgM, IgA and the levels of complements C3 and C4 were detected by immunoturbidimetric method via protein analysis system (IMMAGE800, Beckman, America).
Lymphocyte isolation and labeling
Flow cytometry (FMC) is quantitative analysis technique. To identify cell populations, we mainly focus on the special cell marker numbers. Selection of cell populations is closely related to the gating analysis. The purpose of gating is mainly to determine which cell populations to analyze. We select and analyze specific cell subpopulations. FMC detects fluorescent signals to sort cells. The test mainly employs six-color lymphocyte population detection, the principle of which is to use fluorescein-labeled antibodies specific to various lymphocyte CD antigens to label cells such as CD3 FITC/CD4, PE-Cy7/CD8, APC-Cy7/CD45, PerCP-Cy5.5/CD19, and APC/CD16+56PE. Different fluorescein that labeled produced different fluorescence. Through detection and quantitative analysis of the fluorescent signals, the distribution of different lymphocytes and NK cells could be detected and quantified.
Laboratory indicators
Laboratory indicators in PB at admission and post operation included WBC counts (×109/L), PCT, IL-6 and NLR (neutrophil absolute counts/lymphocyte absolute counts), and MLR (monocyte absolute counts/lymphocyte absolute counts).
According to the actual condition evaluation of the patient after the operation, if the lumbar puncture is feasible after the operation, the cerebrospinal fluid of the lumbar puncture and the peripheral blood will be collected at the same time. If there is no ventricular drainage tube, patients would wait for the opportunity of lumbar puncture. If both lumbar puncture and ventricular drainage tube can be maintained at the same time, lumbar puncture is the first choice for cerebrospinal fluid samples to be tested. The paired peripheral venous blood was collected at the same time on the same day, and the peripheral blood and cerebrospinal fluid lymphocyte subset percentage, procalcitonin, and IL-6 were performed. The paired peripheral blood and cerebrospinal fluid routine (including white blood cell classification and counting and calculation of NLR and MLR) and biochemical (sugar, protein, chloride), peripheral blood complement (C3, C4) and immunoglobulin (IgA, IgM, IgG) were tested.
Outcome assessment
Telephone follow-ups were made at 60 days after ICH ictus, and all follow-up outcomes were recorded into ICH database of NICU. The functional outcomes were assessed by modified Rankin Scal (mRS) at 60 days after ICH onset. The favorable outcome was defined as mRS 1-3, whereas mRS ≥4 was regarded as poor outcomes (such as severely disabled, vegetative, and dead). The sensitivity of existing indicators for predicting poor prognosis at 30 days after ICH is 50%∼82%, and the specificity is 65%∼85%. Sensitivity of predicting poor prognosis at 3 months is 50%∼80%, with a specificity of 59%∼85%. Current study expects the sensitivity to be 80%, and the specificity to reach 60%. We take α = 0.10, allowable error δ = 0.1, and estimate the required sample size according to the following formula

Especially,

Normal distribution test.

Statistical analysis
Continuous data were described by mean ± standard deviation (SD) or median with interquartile range. Categorical variables were expressed as numbers and/or percentages. The method depended on the distribution of the variables. The χ2 test or Fisher exact test was used for categorical data. The independent t test or Mann-Whitney U test was applied for normally and non-normally distributed continuous variables, respectively. Since the number of samples is more than 50, the Kolmogorov-Sminov (K-S) test is applied for normality test. When p > .20, the sample distribution is considered as normal. The two measurement data before and after the surgery did not follow the normal distributions. So the repeated measurement analysis could not be utilized. In order to exclude the influence of individual differences, the differences of preoperative and postoperative indexes were compared. The results showed that there was no statistical difference regarding the changes of the peripheral blood indexes of the two groups of patients before and after the operation (p > .09). The variables identified by univariate analysis (p < .1) were included into multiple logistic regression analysis with stepwise backward selection to determine independent predictors for 60-day unfavorable outcome. CSF CD4/CD8ratio at post operation was calculated by CD4T cell relative numbers divided by CD8T cell relative number. Both predictive abilities of CSF CD4/CD8ratio and the cut-off value of best sensitivity and specificity for 60-day outcome of patients were determined by the receiver operating characteristics (ROC) analysis. Univariate linear analysis and multiple linear regression were utilized to assess independent risk factors of CSF CD4/CD8ratio. Statistical analysis was made employing SPSS and Graphpad Prism software. The difference was considered statistically significant when two-side p value < .05.
Results
Baseline characteristics related to 60-day outcome in surgical patients with ICH.

PB test at admission and after surgery.

Paired CSF test after surgery.


Forest plot regarding independent factors for poor 60-day outcome.

Relative number of lymphocyte subsets in CSF.

Relative number of lymphocyte subsets in PB.

Complement and immunoglobulin in postoperative PB.
Multivariable logistic analysis to find independent factors for the 60-day poor outcome.

Model I: adjusted age, sex, smoking, drinking.
Model II: model I plus GCS, APACHEII, ICH score, fever, complications (break into ventricles, hernia, hydrocephalus, SAH) and coexistence diseases (previous hypertension, diabetes, heart disease, and stroke).

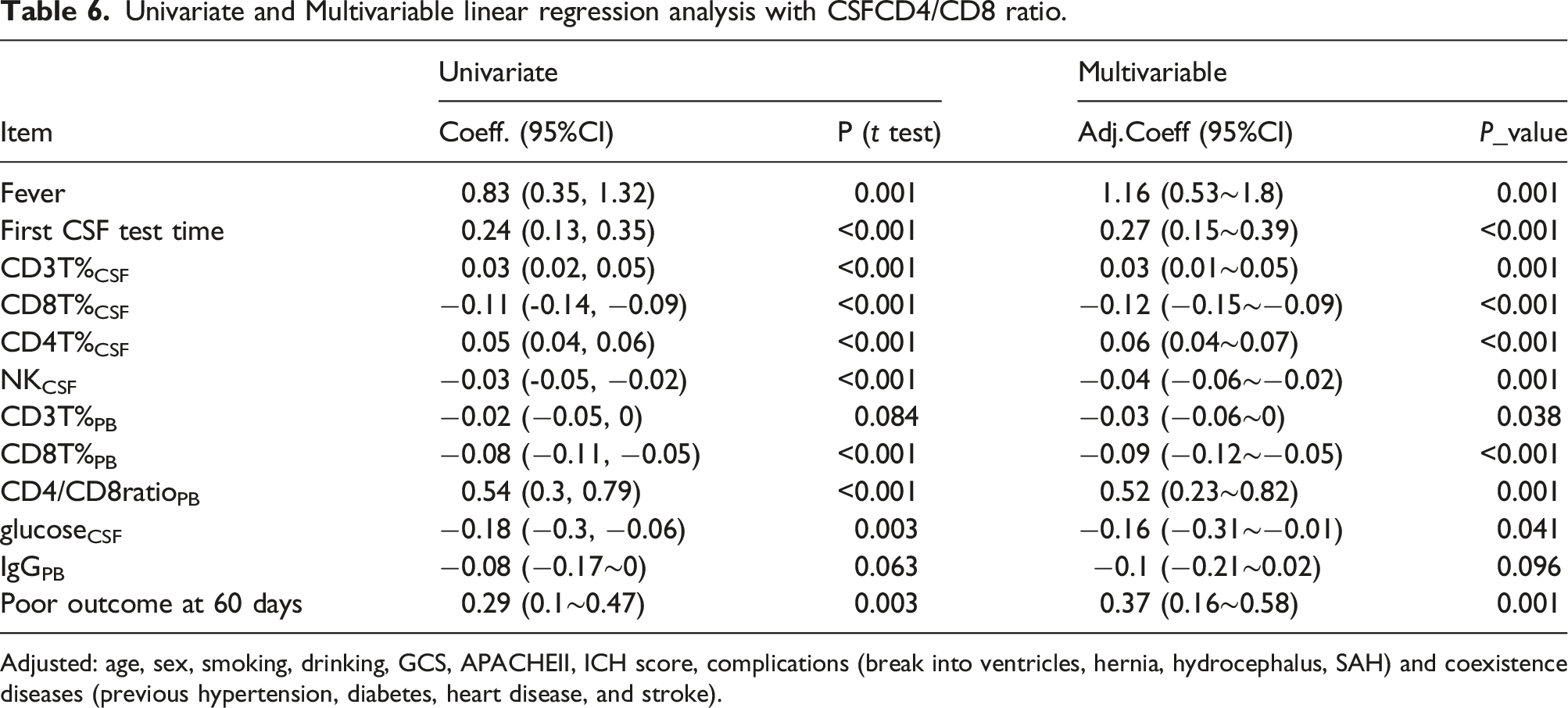
Forest plot regarding univariate and Multivariable linear regression analysis with CSFCD4/CD8 ratio.
Receiver operating characteristic curve analysis was made to estimate predictive ability of CD4/CD8ratioCSF functional outcome of patients with critical ICH after surgeries. Postoperative CD4/CD8ratioCSF level of 1.61 was observed to have the best cut-off value with area under curve (AUC) of 0.6808, sensitivity of 80.39%, specificity of 61.11%, 95% CI: 0.5232–0.8385, p = .0233; CD3T%CSF level of 72.22% was observed to have the best cut-off value with AUC 0.7271, sensitivity of 74.51%, specificity of 61.11%, 95% CI: 0.5885–0.8658, p = .0044; CD4T%CSF level of 33.45% was observed to have the best cut-off value with AUC 0.7048, sensitivity of 92.16%, specificity of 50.00%, 95%CI 0.5477–0.8619, p = .0102 (Figure 7). Univariate linear analysis and Multivariable linear regression analysis were conducted successively for clinical characteristics and corresponding laboratory indicators, and the results identified that postoperative fever, first CSF test time,CD3T%CSF, CD4T%CSF, CD8T%CSF, NKCSF, CD3T%PB, CD8T%PB, CD4/CD8ratioPB, glucose CSF, and poor outcome at 60 days linearly correlated with CD4/CD8ratioCSF after adjustment (Table 6). ROC curves of CD3T%, CD4/CD8 ratio, CD4+T% in CSF. Univariate and Multivariable linear regression analysis with CSFCD4/CD8 ratio. Adjusted: age, sex, smoking, drinking, GCS, APACHEII, ICH score, complications (break into ventricles, hernia, hydrocephalus, SAH) and coexistence diseases (previous hypertension, diabetes, heart disease, and stroke).
Subgroup analyses of the association between first time of CSF test and CD4/CD8ratioCSF of critical ICH.

Adjusted: age, sex, smoking, drinking, GCS, APACHEII, ICH score, complications (break into ventricles, hernia, hydrocephalus, SAH) and coexistence diseases (previous hypertension, diabetes, heart disease, and stroke).
Discussion
Our study systematically investigated the impact of CD4/CD8ratioCSF on 60-days outcomes of critical ICH patients who underwent surgeries. The major research results in postoperative patients with critical ICH are as follows: (1) the patients with poor outcomes at 60 days exhibited greaterCD4/CD8ratio CSF; (2) postoperative fever, first CSF test time,CD3T%CSF, CD4T%CSF, CD8T%CSF, NKCSF, CD3T%PB, CD8T%PB, CD4/CD8ratioPB, glucose CSF, and poor outcome at 60 days linearly correlated with CD4/CD8ratioCSF. (3) The best critical threshold was identified as 1.61 for CD4/CD8ratioCSF; (4) In 3–5 days subgroup, CD4/CD8ratioCSF ≥1.61 was associated with a greater risk for 60-day poor outcome compared with the corresponding subgroup. Other than that, fever after surgery, hernia before surgery, SAH and lower GCS at admission, large hematoma volume, greater CD3T%CSF, greater CD4T%CSF were identified as prognostic factors to predict the 60-day poor outcome, respectively. So far, our results revealed the predictive value of CD4/CD8ratioCSF on prognosis of postoperative patients with critical ICH. It shed a light on potential relationship between immune inflammatory reaction and outcome of critical ICH.
Immune inflammation is involved in secondary brain injury after intracerebral hemorrhage. When the blood–brain barrier is destroyed, white blood cells first enter the central nervous system to promote inflammatory response, and T cells are the main white blood cell group in cerebral tissue after intracerebral hemorrhage. Studies had found that lymphocytes were found in CSF and brain tissue around hematoma as early as 6 h after ICH. 9 However, NK cells can rapidly respond to external inflammatory chemokines. 10 Once being activated, NK has cytotoxic activity to produce cytokines and chemokines, through which other immune cells can be coordinated to limit or enhance immune response. 11 Some animal studies have illustrated that inflammation plays an important role in the injury caused by cerebral hemorrhage and the recovery of the brain. The effect of regulating inflammation on brain damage caused by human ICH has not been determined.12,13 Study reported that T cell subsets, CD8T cells and CD4T cells increased after ICH, which led to inflammatory damage. 14 The use of immunosuppressants can reduce infiltrating T lymphocytes, reduce immune response and inflammatory response, as well as alleviate brain edema. 6 Our study found that the PB lymphocyte subsets after surgery were not significantly associated to the patient prognosis. However, in cerebrospinal fluid, CD3T%, CD4T% and CD4/CD8ratio in patients with poor prognosis at 60 days were significantly higher than those in the control group, perhaps inhibiting the brain T cell immune response may improve clinical outcomes. This needs further follow-up clinical investigations.
CD4T cells have a strong ability to transfer across endothelial cells. CD4T cells account for majority of T lymphocyte subsets in the CSF, which may be related to the ability of CD4T transmembrane transfer. 15 Considering the blood–brain barrier that has been damaged after surgery, peripheral inflammatory cells can enter the brain to cause neuroinflammation. At present, the correlations between CSF CD4/CD8 ratio and 60-day functional outcomes in critical cerebral hemorrhage patients are not yet discussed. The purpose of present study was to evaluate the predictive value of postoperative cerebrospinal fluid and peripheral blood lymphocyte subsets, as well as other laboratory parameters, on the 60-day postoperative prognosis of critically illed ICH patients. Present study found that the main factor affected CD4/CD8ratio CSF was CD4T% CSF, while CD8T% CSF is not significant. In the poor prognosis group, we also found that the CD4T% CSF and CD3T% CSF increased significantly. Therefore, improving the immune response in CSF may improve the short-term prognosis of patients with critical ICH. NLR and MLR reflect the balance between innate immunity and adaptive immunity, which are simple indicators of immune status and inflammation level. Some studies had discovered that the increase of NLR and MLR enhanced mortality of cerebral hemorrhage for 30 days.16,17
However, in our study, no matter in the PB before and after surgery or in the CSF after surgery, NLR and MLR were not found to be associated with the 60-day prognosis, which may be related to the small sample size in our study. It demands further study by expanding the sample size. Another limit is that the calculation and justification of the sample size selected was not done in the study. In summary, this finding provides a possible explanation for importance of immune background in the outcomes of critical ICH patients post-surgery.
Conclusion
Current study is focus on patients with severe cerebral hemorrhage. The blood–brain barrier has been destroyed, and peripheral cells can enter the central nervous system. As for the association of patient prognosis with critical ICH, CSF CD4/CD8 ratio, especially in 3–5 days after surgery, it exhibited potential independent predictive ability for 60-day functional outcomes of critical ICH patients. The underling mechanisms regarding associations between CD4/CD8 ratioCSF and neuroimmune inflammatory background of critical ICH patients should be unraveled in further investigations. Patients with critical ICH exhibited poor outcomes at 60 days, which was associated with fever after surgery, hernia before surgery, SAH and lower GCS at admission and large hematoma volume, greater CD3T%CSF, greater CD4T%CSF, and greater CD4/CD8ratioCSF. To some extent, reducing the immune response in CSF may be beneficial to short-term prognosis of critical ICH patients.
Footnotes
Acknowledgments
We would like to thank anonymous reviewers and editor for suggestive comments, which helped us improve this presentation. We sincerely thank Aditegen LLC, NJ, US for scientific editing.
Author contributions
Chunying Zhu & Yingfu Zhang: Designed this study and prepared this manuscript, and are responsible for the accuracy and completeness of the manuscript. Wei Li: Collected and analyzed clinical data. Qianqian Li and Huan Wang: Significantly revised this manuscript. Chunying Zhu and Yingfu Zhangbuted this manuscript equall.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.