
Abstract
Objectives
Since being declared a global pandemic, the SARS-CoV-2 virus had a significant impact on the entire globe. The pandemic has placed a heavy burden on healthcare systems worldwide, and cancer patients are particularly prone. Despite the fact that initial international reports suggest delays in breast cancer (BC) diagnosis and screening programs, the Egyptian context requires additional research on this topic. To examine whether COVID-19 has changed the pattern of disease presentation before and after the pandemic, focusing on the tumor, node, and metastasis (TNM) staging of the disease at the initial presentation
Methods
This single-center, retrospective study of female BC patients initially diagnosed at Baheya Foundation was conducted during the following time frames: from Jan 2019 to Jan 2020 (Pre COVID-19 cohort) and from Mar 2020 to Mar 2021 (post–COVID-19 cohort). We compared the two cohorts in terms of clinical characteristics, tumor characteristics, and the number of days from presentation to treatment. Our primary endpoint was the difference in the TNM stage of BC at the initial presentation.
Results
This analysis included 710 BC patients, 350 from the pre-COVID cohort and 360 from the post-COVID group. We detected a 27.9% increase in late-stage BC (stages III-IV) in the post-pandemic cohort compared to the pre-pandemic (60.1% vs. 47%, p < 0.001). The time from diagnosis to commencement of treatment was significantly longer (28.34 ± 18.845 vs 36.04 ± 23.641 days, p < 0.001) in the post-COVID cohort (mean difference = 7.702, 95% CI 4.54–10.85, p < 0.001). A higher percentage of patients in the post-pandemic cohort received systemic neoadjuvant therapy (p-value for Exact’s test for all treatment options = 0.001).
Conclusions
The number of patients requiring systemic neoadjuvant chemotherapy increased dramatically in the post-pandemic group with advanced stages of BC at presentation. This study highlights the need for proper management of cancer patients during any future pandemic.
Introduction
In December 2019, the first cases of severe acute respiratory syndrome coronavirus 2 (SARS-Cov2) were identified in Wuhan, China, which resulted in a pandemic and a global health crisis. 1 Shortly after, Egypt announced the first confirmed case of SARS-Cov2 in February 2020. In the subsequent 3 months, 10,000 cases were reported. 2 However, the disease burden at the time may have been underestimated. A study by Tuite et al. estimated a significantly higher number of cases based on the number of exported cases from Egypt at the time. 3
Intuitively, the pandemic was expected to place a heavy burden on healthcare systems worldwide, with conservative estimates predicting that the US healthcare system would be overwhelmed by the pandemic’s healthcare demands.4–6 Furthermore, the pandemic severely affected healthcare workers, leading to more decline in healthcare availability. 7 As a high-risk group for hospitalization, invasive ventilation, and death following infection, cancer patients were not immune to the effects of the pandemic. 8 COVID-19 has also affected cancer patients regarding the availability of healthcare access, as screenings, diagnosis, and commencement of treatment in specialized centers were affected by the pandemic.9,10
The pandemic has significantly impacted the BC patient population with a decrease in screening programs and demanding access to healthcare facilities, leading to a decline in diagnosis and a shift in disease stage distribution at presentation.9,11,12 The number of patients screened by the majority of active cancer screening programs, including BC screening, decreased during the pandemic, 11 as a study by London et al. found a dramatic decline in BC screening by 89.2%. 6 In a subsequent study conducted in Portugal, the number of patients with advanced forms of BC who were admitted for the first time decreased by 40%. 12 Another multi-institutional study found a decrease in BC screenings and diagnosis during the COVID-19 pandemic with a change in disease staging distribution, with more patients diagnosed with stage IIB and IV during the pandemic. 13
As the impact of the pandemic on breast cancer patients in Egypt is currently unknown, our study aims to identify and quantify the changes posed by COVID-19 on BC in terms of the stage at first presentation, diagnostic delays, and the commencement of treatment in our Breast Cancer Center “Baheya Foundation for Early Detection and Treatment of Breast Cancer.” Baheya Foundation provides free services to BC patients. Since its opening in 2015, Baheya’s healthcare services have been provided to 212,985 patients. To our knowledge, this is the first study to assess the impact of the COVID-19 pandemic on Egyptian BC patients and their accessibility to healthcare services.
Methods
Study design and setting
The current study is a single-center retrospective chart review of newly diagnosed BC patients. To evaluate the effects of the COVID-19 pandemic on BC patients, we reviewed the charts of two randomly selected patient cohorts. Data included patients who visited the center the year before the announcement of the pandemic, from January 2019 to January 2020 (pre–COVID-19 cohort), and patients who visited the center the year after the announcement of the pandemic, from March 2020 to March 2021 (post–COVID-19 cohort).
This study was approved by the Institutional Review Board (IRB) at the Baheya foundation, which is a non-profitable BC center based in Giza, Egypt. It provides complete care for BC patients, including screening, diagnosis, and treatment, both medical and surgical. This manuscript was written and revised in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines by Enhancing the Quality and Transparency of Health Research (EQUATOR) Network.
Study objectives
• The primary objective To compare the anatomical TNM stage of BC on initial presentation between the two cohorts. The early-stage disease was defined as stages 0, I, and II. The late-stage disease was defined as stages III and IV. Staging of BC was done according to the 8th edition of the Union of international cancer control (UICC) TNM classification of malignant tumors.
14
• Secondary objectives (a) To compare the duration of the diagnostic process between the two cohorts, determined by the number of days from the date of the first presentation to the date of complete pathological diagnosis, including immunohistochemistry (IHC) tests. (b) To compare the waiting time for treatment between the two cohorts, determined by the number of days from the date of complete diagnosis to the date of commencement of the planned treatment regimen, whether it was surgical or non-surgical.
Sample size calculation
It is essential to guarantee that statistically significant results have clinically relevant outcomes. Consistent with the current study’s scope, a recent single-center study by Shohdy et al. on 368 Egyptian BC patients found the T3–T4 clinical tumor stage to represent a total of 58% of this cohort.
15
The study by Borksy et al. also reported a 10% increase in advanced BC cases during the COVID-19 pandemic.
16
Separate calculations were performed for each study interval (pre- and post-pandemic), and then the total number of cases was considered. The following formula was used:

For the first sample (N1):

For the second sample (N2), we assume a total increase of 10%:

Total sample size (NT):

Patient selection
All malignant cases treated in Baheya undergo a pre-treatment assessment to assess their TNM stage, metastatic status, heart condition, organ function, and status in order to have a baseline profile and choose a treatment modality. This assessment includes: bilateral ultrasound (U/S) scan, breast mammography, U/S guided biopsy from the suspicious lesion (true cut or fine cut), BC hormone receptor and HER2 Status, computed tomography (CT) of the chest, abdomen, and pelvis with contrast, complete blood count (CBC), echocardiography, kidney function tests (KFTs), liver function tests (LFTs), and coagulation profile. According to the patient’s history and clinical condition, other circumstantial tests include bone scintigraphy (bone scan), Dual-energy X-ray absorptiometry (DEXA) scan, MRI brain with contrast, pelvic abdominal U/S, and venous duplex ultrasound.
The patient’s cycle in our hospital begins with screening by the Oncology Surgery Clinic, then referral to the Radiology Department, followed by a referral to the Medical Oncology Clinic if malignancy is confirmed after performing the above assessment or to be managed in the surgery clinic if it is a benign case or a case with no current abnormality. Few patients are referred directly from outside our center to our oncology clinic to start or continue their treatment for several reasons. Therefore, there were some data missing in their medical history.
We collected data from the archive of the Medical Oncology Clinic, where most of the patients referred there have already undergone their initial assessment, and all the data required for our study would be present—followed by categorization of data into two groups: pre–COVID-19 and post–COVID-19 groups. Finally, patients were randomly selected using a random number generator. We searched for the patients using the medical record number (MRN).
After reviewing the charts, we included patients who were first-time presenters diagnosed with BC at our center. While patients with any of the following criteria were excluded from the study: • Known case of breast cancer. • Concomitant malignancy. • Insufficient data for dropped-out patients.
Data collection
Data were collected during the period from 28/4/2022 to 19/5/2022. Using the Baheya foundation’s EMR, we extracted the following data for all the patients. • Demographic data included age, city of residence, and the number of offspring. • Clinical data included menopausal status, body mass index (BMI), history of chronic diseases (diabetes mellitus (DM), hypertension (HTN), cardiac morbidities, others), family history of BC, the date of the first presentation, performance status score (PS)
17
at presentation, type of the treatment assigned to the patient, and the date of treatment initiation. • Imaging data included Breast Imaging Reporting and Data System score (BIRADS)18,19 and clinical TNM for patients initially assigned to medical treatment. • Laboratory data included the date of complete pathological diagnosis, type, grade, hormonal receptors status (HR), human epidermal growth factor receptor-2 (HER-2) status of the tumor, and pathological TNM for patients initially assigned to surgical treatment.
HR status was determined by the percentage of nuclear staining of estrogen and progesterone receptors, with more than 1% considered positive. HER-2 status was determined by the degree of amplification on IHC, with 3 + considered positive. Silver stain in situ hybridization (SISH)20–22 was used in case the IHC result was inconclusive for the HER-2 status. Tumors were further subtyped according to the receptor status into Luminal HER-2 negative (HR+/HER-2-), Luminal HER-2 positive (HR+/HER-2+), HER-2+ (HR-/HER-2+), and Triple negative (HR-/HER-2-).
Statistical analysis
Data entry was done through Microsoft EXCEL. Baseline characteristics of the patients were described as absolute and relative frequencies and then compared using the Chi Squared test with asymptotic or exact significance as appropriate. Continuous variables were expressed as mean ± standard deviation to appreciate variability within the data. Analysis of continuous variables was done using the unpaired t-test. All data were analyzed using IBM SPSSTM 26 (SPSS, Chicago, IL) edition. Results with a p-value less than 0.05 were considered statistically significant.
Results
Baseline clinical and laboratory features of the studied patients. 2

Disease stage and Tumor size at presentation. 5

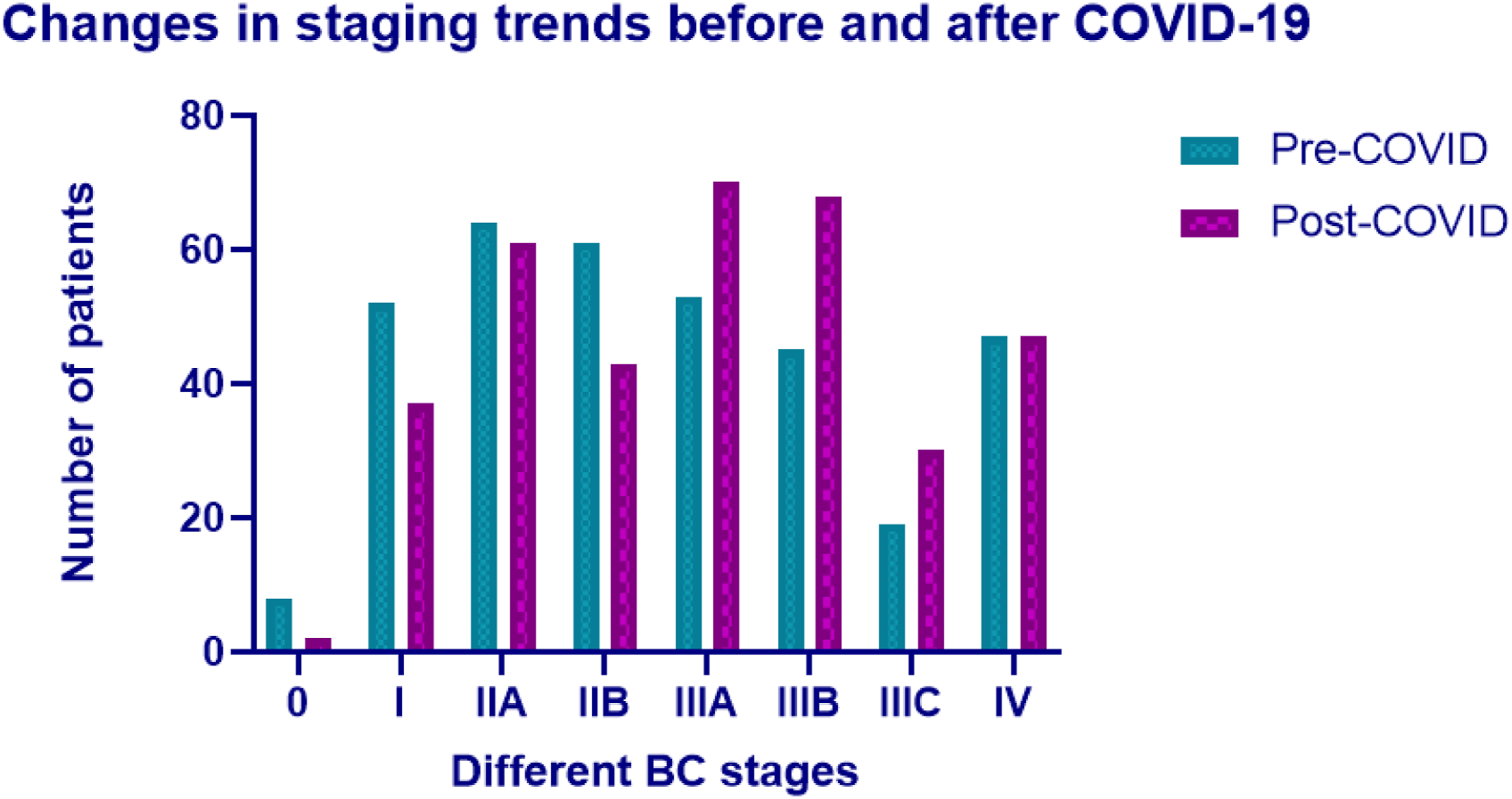
Bar chart of anatomical stages frequencies pre and post COVID-19.
Tumor characteristics: histopathological type, grade, laterality, TNM classifications, anatomical staging, and luminal types. 7

Delay metrics: time from presentation to diagnosis, time from diagnosis to treatment, and time from presentation to treatment.

Type of initial treatment received. 11

Discussion
This retrospective chart review examined the records of 710 BC patients treated in our tertiary center. We observed a 27.9% increase in late-stage BC at the initial presentation in the post–COVID-19 cohort (60.1% of the total cases) compared to the pre–COVID-19 cohort (47%). This change was driven mainly by larger tumor sizes (T3-T4) in the post-pandemic cohort compared to the pre-pandemic cohort (46.4% vs. 34.1%, OR 1.671, CI 1.232–2.265), by a higher percentage of node-positive disease (76% vs. 67%, OR 1.561, CI: 1.122–2.172) and upstaging of the nodal disease. In contrast, distant metastasis played no role in this progression (13.1% vs. 13.4%, p-value = 0.912).
It should be noted that HER-2 Neu enriched patients are of minimal presentation in this study as they are not within the treatment scope of Baheya Charity Women’s Cancer Hospital due to the limited resource available. Most of these patients are being treated in either a government-funded public hospital or in a private practice based on the patient’s own expenses.
COVID-19 has significantly affected the medical community, including BC patients, resulting in delayed screening and diagnoses, 23 more advanced diseases, 24 and less predicted survival. 25 Many of these effects are well documented in countries that follow a screen-based paradigm for early detection and treatment. The situation is vastly different when considering pandemic effects in a context with limited resources and a symptom-based paradigm. This paradigm can exacerbate the delays caused by the emerging pandemic, which has a negative impact on patient outcomes.
Many studies discussed the changes in staging trends before and after the pandemic.12,26–28 A study conducted in the United Kingdom by Borsky et al. reported an increase in node-positive disease on presentation in 2020 compared to 2019 (36.2% vs. 23.6%, p = 0.0063), an increase in metastatic disease at presentation (8.0% vs. 2.9%, p = 0.0295) and increased in median UICC TNM stage at detection from 1b to 2a (p = 0.0184). Conversely, a Turkish study by Kara et al. did not find any statistically significant differences in tumor size, nodal involvement, or overall TNM stage. 28 An Italian study also reported a decrease in stage III & IV BC from 13.1% in 2019 to 12.1% in 2020. 29 In the same study, percentage of surgeries decreased from 30% to 21%, while neoadjuvant chemotherapy increased from 19% to 22%. Another Portuguese study by Simao et al. found a statistically significant increase in the number of patients admitted with metastatic disease at presentation requiring systemic therapy (28.9% vs. 13.6%, p = 0.003). 27
Our patients were comparable in terms of age, BMI, and baseline comorbidities. Due to the lack of data, the use of a validated comorbidity prognostic index such as the “Charlson Comorbidity Index” was not possible. Notably, the BMI values for both groups were high (34.96 ± 10.79 vs 36.19 ± 10.09, p = 0.119). Egypt ranks 18th on the list of countries with the highest prevalence of obesity 30 and carries one of the highest household double burdens of malnutrition (DBM). 31 However, these results should be interpreted with caution because we could not record BMI at the time of diagnosis. Due to the advanced diagnosis stage, many patients received either neoadjuvant or adjuvant chemotherapy. Post-chemotherapy weight gain is a well-documented complication32,33; weight at diagnosis may be significantly lower than previously recorded.
There were differences in tumor characteristics between pre- and post–COVID-19 cohorts. Only 5.3% of patients in the post-pandemic cohort had Grade I tumors, compared with 13.4% in the pre-pandemic cohort (p-value <0.001). We also classified tumors into Luminal HER-2 negative, Luminal HER-2 positive, HER-2 enriched, and triple-negative BC, as Ki-67 testing is not routinely incorporated in our center guidelines. Most cases were Luminal HER-2 negative (89.92% in 2019 vs 92.45% in 2020, p-value = 0.2201). Multiple factors, including but not limited to age, years of hormone therapy use, age at menarche, and time between menarche and first full-term birth, determine hormone receptor status.27,34 However, these factors are beyond the scope of our investigation.
No significant difference was found between pro-and post–COVID-19 cohorts regarding the metastatic status. However, a significant increase in N2 (21.5%–24.9%) and N3 (8.1%–16.5%) was established. This change can be attributed to the delay in diagnosis caused by the pandemic. However, further future investigations are required to investigate the disparity between the metastatic and nodal status.
We did not find a statistically significant difference in time to complete diagnosis (mean difference = 1.108, 95% CI -0.305–2.52), primarily due to the successful reallocation of resources, which was accomplished by mandating that all new patients schedule an appointment in advance. During this process, a call center agent would triage the patients using a predefined questionnaire assessing their risk for active malignant disease and clinical condition. The high-risk or clinically debilitated patients were given the 1-week accelerated admission pathway. On average, others would be added to the regular pathway, in which they would have an appointment within 1 month of their phone call. Additionally, current patients were triaged at our reception unit according to their clinical condition and new complaints. They were also surveyed for any upper respiratory tract infection (URTI) within the past 2 weeks and would be required to undergo a COVID-19 antigen test or CT chest (before the previous test was established). As a resource-limited center in a developing country, screening all patients, regardless of the presence of URTI symptoms, was financially challenging.
Telemedicine is a trending concept due to its efficacy in saving resources, time and effort; especially during COVID-19 pandemic. 35 An Italian study by Tari et al. reported modifications done during the pandemic in a breast cancer unit, including a telephone questionnaire to exclude COVID-19 symptoms, triaging the patients according to their clinical condition and rescheduling confirmed or suspected COVID-19 cases. 36 In our center, a hotline was established with over-the-hour availability designated to our current patients receiving chemotherapy, hormonal therapy, or immunotherapy. All medical oncology specialists were taking turns responding to inquiries received by this hotline by personally talking to the patients while accessing their EMR to review their medical history and current management status before consulting the patients and prescribing medications or requesting urgent presentation to our center if an emergency was suspected. A separate hotline was established for patients receiving hormonal treatment. The medical oncology specialists created a second schedule in which they would call these patients, inquire about their current clinical condition, and extend their hormonal treatment if there was no anomaly. Then, the Baheya Foundation made an agreement with a shipping company to ship the new dosage of hormonal treatment to these patients in order to prevent unnecessary visits to our facility, which could increase their risk of contracting COVID-19.
In contrast, waiting time between complete diagnosis and treatment increased between post–COVID-19 and pre–COVID-19 cohorts (mean difference = 7.7, 95% CI 4.55–10.86). This led to an increased overall process from patient presentation to commencement of the treatment (mean difference = 6.59, 95% CI 3.19–9.99). Many factors contribute to these delays relating to participants’ difficulty accessing the service, disruptions in supply chains related to personnel shortages, equipment maintenance, and modification of treatment regimens. It was difficult to reserve surgical rooms in the initial phase following the declaration of a pandemic state of emergency. After COVID-19, many aspects of emergency and elective care changed globally. According to a Finnish study by Uimonen et al., there was an 8% increase in waiting times in 2020 (from 85.8 days in 2019 to 92.6 in 2020). Furthermore, elective surgeries decreased rapidly in the initial phase of the pandemic. 37 Delaying radiotherapy (RT) and chemotherapy is linked to worse outcomes in terms of locoregional control and overall survival,35,36 according to research on breast cancer and other malignancies.38,39 Moreover, it adds another burden: a decline in quality of life due to fear of cancer progression or recurrence. 40
It is essential to monitor the effects of the pandemic on Low- and Middle-Income Countries (LMICs), as cultural differences affect how the double burden of disease and pandemics are received. As stated by the Institute of Medicine (IOM), the environment changes health behaviors by “shaping norms, enforcing patterns of social control, providing or not providing environmental opportunities to engage in particular behaviors, reducing or producing stress, and placing constraints on individual choice.” 41 In the following years, pandemics will continue to evolve, driven mainly by climate changes and land use changes, which will facilitate viral circulation between areas that were geographically isolated. 42
Limitations
This study has multiple limitations being a retrospective analysis, and it bears limitations inherent in its designs. As this study was conducted at a single tertiary center, it has both advantages and disadvantages. In pre- and post-COVID cohorts, inter-rater variability and homogeneous decision-making processes are ensured. However, as a peculiar pattern of referral and expertise exists, cases at our center may be more advanced than the average Egyptian BC patients, with a more comorbidity profile and higher burden of diseases. A multi-centric study is needed to refine and generalize the results. We excluded patients who did not complete their treatment and those who did not have complete records. Patients’ drop-out is not unbiased. We tried to minimize the unavoidable selection bias by matching pre and post-groups at their baseline characteristics, including age, BMI, and comorbidities. In addition, we ensured that the patients were staged pre/post–COVID-19 using the same radiological guidelines for TNM. Moreover, subjects were chosen by simple random sampling technique with a narrow time span between the two cohorts to reduce the effects of the trend.
Conclusion
During the post–COVID-19 period, the prevalence of late-stage BC disease increased dramatically in comparison to the pre–COVID-19 era. The number of surgeries decreased with an increase in patients requiring neoadjuvant chemotherapy. In the post-pandemic cohort, the interval between a conclusive diagnosis and the commencement of treatment was higher.
Footnotes
Acknowledgments
Special thanks to the hospital directors who allowed the study to be carried out, our colleagues in the different departments for their continuous effort, which provided critical data for our study, and the subjects who participated in the study.
Author contributions
All authors contributed to the design and interpretation of the data; MA, AI, OG, and AB performed analysis, wrote the paper, and revised it. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical committee approval was granted on 26/4/2022 under the reference number 202204260013 from Baheya Centre for Early Detection and Treatment of Breast Cancer & National Research Centre. All patients signed consent of approval of their data usage in retrospective research projects, guaranteeing all patients’ anonymity.