
Abstract
Introduction
Progesterone is essential for both the initiation and the maintenance of pregnancy. The immunological effects of progesterone are mediated by the progesterone-induced blocking factor (PIBF), which is an immunomodulatory factor with anti-abortive properties.1,2
Progesterone-induced blocking factor downregulates natural killer (NK) cell activity, affects the Th1/Th2 balance, and contributes to decreased cell-mediated responses during pregnancy.
1
The cytokines responsible for Th1/Th2 balance in the human immunological system are presented in Figure 1.3,4 Cytokines responsible for Th1/Th2 balance.
Progesterone-induced blocking factor was discovered to be synthesized in different tissues, including human lymphocytes, the placenta, or some malignant tumors.1,5 Most studies assess the concentration of PIBF in the blood serum and urine during pregnancy. Therefore, the knowledge of its influence on fertility treatment, especially in vitro fertilization (IVF) and embryo transfer, is still limited. Evidence exists that PIBF-mediated Th1/Th2 balance is closely correlated with delivery outcomes of IVF-embryo transfer (IVF-ET). 6 Lachman et al. found that PIBF is overexpressed in highly proliferating cells and is associated with the centrosome. 7
In the current study, we aim to determine the concentration of PIBF in follicular fluid (FF) obtained during ovarian puncture in stimulated cycles of IVF-qualified women and understand the correlation between the concentration and outcome of embryo transfer. We also established the concentration of chosen cytokines in the FF and investigated the connection between the cytokine profile of FF and the development of follicles, embryo quality, and the efficacy of IVF-ET.
Methods
This prospective cohort study group consisted of patients who underwent IVF in the Fertility Center in Bydgoszcz, Poland, between April 2021 and January 2022. A total of 78 patients were selected, in order of qualification for IVF, after meeting inclusion and exclusion criteria.
All qualified patients suffered from infertility, defined as the inability to achieve pregnancy after a year of regular intercourse, underwent a detailed medical interview, physical examination, and gynecological assessment to determine the primary reason for infertility. The interview questionnaire was descriptive (Appendix 1), filled in by the investigator, and, based on a typical medical interview, modified by the authors to be appropriate for the study. 8 A similar interview card was used before, in our research on male infertility (52 patients), allowing us to achieve a good interview summary. 9
Patients suffering from other serious or chronic diseases or taking medication that could influence the results of the study were excluded.
Inclusion and exclusion criteria.

The size of the study population was established before conducting the study and was based on previous studies on the cytokine profile of FF in women who underwent IVF. Another factor taken into account was the limited financial support for the research.
Gynecological assessment
All patients underwent a detailed medical interview, including the course of fertility treatment, and physical, gynecological, and cytological examinations. Ultrasound (GE Voluson S10 Expert) assessment of the reproductive system was performed to accurately assess antral follicles. Vaginal biocenosis and pH were determined. All patients had their blood sampled to assess the concentration of basic parameters, including estradiol, prolactin, progesterone, AMH, FSH, morphology, electrolytes, APTT, blood type, and in the direction of viral diseases that could influence their possibility of conceiving and the course of the possible pregnancy.
The sperm quality of the male partners was examined, and their blood was sampled to determine their blood type and the presence of anti-Hbc, Hbs antigen, anti-HCV, anti-HIV 1–2, VDRL, and IgM and IgG cytomegalovirus.
Patients’ hormonal stimulation, ovarian function, embryo quality assessment, and IVF procedure
In the fertility clinic
Follicular fluid samples from each mature follicle (with diameter ≥17 mm) were taken on the day of the ovarian puncture and stored in pools/per patient at -80°C until immunological assessment.
Oocyte fertilization took place between 39 and 41 h after pick-up. Fertilization assessment was performed in 17 ± 1 h. The third-day embryo assessment, according to Gardner and Schoolcraft criteria, took place 68 ± 1 h after fertilization; assessment on the fifth day took place 116 ± 1 h after fertilization. 12
The quality of the embryos was assessed by an embryologist on the third and fifth day after fertilization. As done in previous studies, the embryos were assessed as top-quality or non-top-quality. 13
Depending on a patient’s individual decision and the assessed chances of succeeding, one or two embryos were chosen for transfer to the uterus. Clinical confirmation of pregnancy was based on blood serum B-hCG concentration between the 10th and the 15th day after transfer.
Immunoassay
Follicular fluid, obtained during ovarian puncture, was stored at a temperature of −80°C until assessment. The concentration of IL-18 and PIBF1 was measured using commercially available ELISA kits (Cloud-Clone Corp.: Human IL-18 ELISA Kit SEA064Hu; and Human PIBF1 ELISA Kit SEN433Hu). The PIBF1 immunogen sequence was Asn13∼Val203, and it recognizes both the 90 kDa PIBF protein and the 35 kDa splice variant. This assay employs the quantitative sandwich enzyme immunoassay technique, and color change is measured spectrophotometrically at a wavelength of 450 nm ± 10 nm (Infinite® F50; Tecan, Switzerland). Furthermore, the Magellan™ reader control and data analysis software is used to plot the calibration curve and read the concentrations of the test samples. The results show that sensitivity or the minimum detectable dose of human IL-18 was 5.9 pg/mL. The maximum measurable dose of human IL-18 was found to be 1000.0 pg/mL. No significant cross-reactivity or interference between human IL-18 and analogs was observed. The sensitivity or the minimum detectable dose of human PIBF1 was 0.058 Ng/ml. The maximum measurable dose of human PIBF1 was 10.0 ng/mL. No significant cross-reactivity or interference between human PIBF1 and analogs was observed.
The concentration of IL-2, IL-4, IL-6, IL-10, and IFNγ was measured using commercially available High-Sensitivity (HS) ELISA kits (Diaclone, Medix Biochemica Group: Human IL-2 HS ELISA Kit 1HS2-21; Human IL-4 HS ELISA Kit 1HS4-21; Human IL-6 HS ELISA Kit 1HS6-76; Human IL-10 HS ELISA Kit 1HS10-23; and Human IFNγ HS ELISA Kit 1HSIFG-33).
This assay employs the quantitative high-sensitivity sandwich enzyme immunoassay technique. The absorbance value is determined for each well on a spectrophotometer (Infinite® F50; Tecan, Switzerland) using 450 nm as the primary wavelength and optionally 620 nm as the reference wavelength. The Magellan™ reader control and data analysis software is used to plot the calibration curve and read the concentrations of the test samples. The results show that sensitivity or the minimum detectable dose of human IL-2 was 0.97 pg/mL. The maximum measurable dose of human IL-2 was 60.0 pg/mL. The sensitivity or the minimum detectable dose of human IL-4 was found to be 0.31 pg/mL. The maximum measurable dose of human IL-4 was found to be 10.0 pg/mL. The sensitivity or the minimum detectable dose of human IL-6 was found to be 0.81 pg/mL. The maximum measurable dose of human IL-6 was found to be 50.0 pg/mL. The sensitivity or the minimum detectable dose of human IL-10 was found to be 0.98 pg/mL. The maximum measurable dose of human IL-10 was found to be 50.0 pg/mL. The sensitivity or the minimum detectable dose of human IFN-γ was found to be 0.69 pg/mL. The maximum measurable dose of human IFN-γ was found to be 25.0 pg/mL.
The concentration of IL-1α, IL-1β, IL-5, IL-8, and IL-15 was measured using commercially available ELISA kits (Diaclone, Medix Biochemica Group: Human IL-1α ELISA Kit 101A-33; Human IL-1β ELISA Kit 101B-59; Human IL-5 ELISA Kit 1005-23T; Human IL-8ELISA Kit 1008–85; and Human IL-15 ELISA Kit 1015-11T). This assay employs the quantitative sandwich enzyme immunoassay technique. The absorbance value is determined for each well on a spectrophotometer (Infinite® F50; Tecan; Switzerland) using 450 nm as the primary wavelength and optionally 620 nm as the reference wavelength. Again, the Magellan™ reader control and data analysis software is used to plot the calibration curve and read the concentrations of the test samples. The sensitivity or the minimum detectable dose of human IL-1α was found to be 10.0 pg/mL. The maximum measurable dose of human IL-1α was found to be 1000.0 pg/mL. The sensitivity or the minimum detectable dose of human IL-1β was 6.5 pg/mL. The maximum measurable dose of human IL-1β was 500 pg/mL. The sensitivity or the minimum detectable dose of human IL-5 was 5.0 pg/mL. The maximum measurable dose of human IL-5 was 250.0 pg/mL. The sensitivity or the minimum detectable dose of human IL-8 was 12.3 pg/mL. The maximum measurable dose of human IL-8 was 1000.0 pg/mL. The sensitivity or the minimum detectable dose of human IL-15 was found to be 18.3 pg/mL. The maximum measurable dose of human IL-15 was found to be 1000.0 pg/mL. Moreover, no significant cross-reactivity or interference between the aforementioned cytokines and analogs was observed.
Statistical analysis
The Mann–Whitney test was used to compare the quantitative variables between two groups, while the Kruskal–Wallis test (followed by a Dunn post-hoc test) was used for more than two groups. 14 The relationship between two quantitative variables was assessed with Spearman’s coefficient of correlation. Univariate logistic regressions were performed to analyze the impact of the selected variables on the dichotomous outcome (positive/negative pregnancy test). Odds ratios (ORs) with 95% confidence intervals were determined. The significance level for all statistical tests was set to 0.05. R 4.1.2. and MS Excel 365 were used for computations.
Bioethics committee approval
The study was approved by the Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń, and Bioethical Committee and was assigned the classification number KB 334/2021. All patients gave informed, written consent to participate in the study.
Results
General characteristic of the study group.

Analysis of cells obtained during oocyte retrieval and embryo quality assessment in the study group.

Fourteen (17.95%) women decided to freeze the achieved embryos and did not have a transfer. Of the 64 women who underwent the transfer, 24 (37.5%) achieved a positive pregnancy test and were defined as a successful IVF. In this group, five patients had a spontaneous abortion during the first trimester, and 19 continued with uncomplicated pregnancy. This provides a 29.7% endpoint success rate for the IVF procedure in the studied group, which is defined as an uncomplicated pregnancy >20 hbd. All patients’ standard indicators of fertility (progesterone, estradiol, AMH, and prolactin) had been measured, and no connection between their concentration and the success rate of IVF procedure was found.
Cytokine and progesterone-induced blocking factor 1 concentration in follicular fluid of patients.

Pregnancy test result and immunological parameters of follicular fluid.
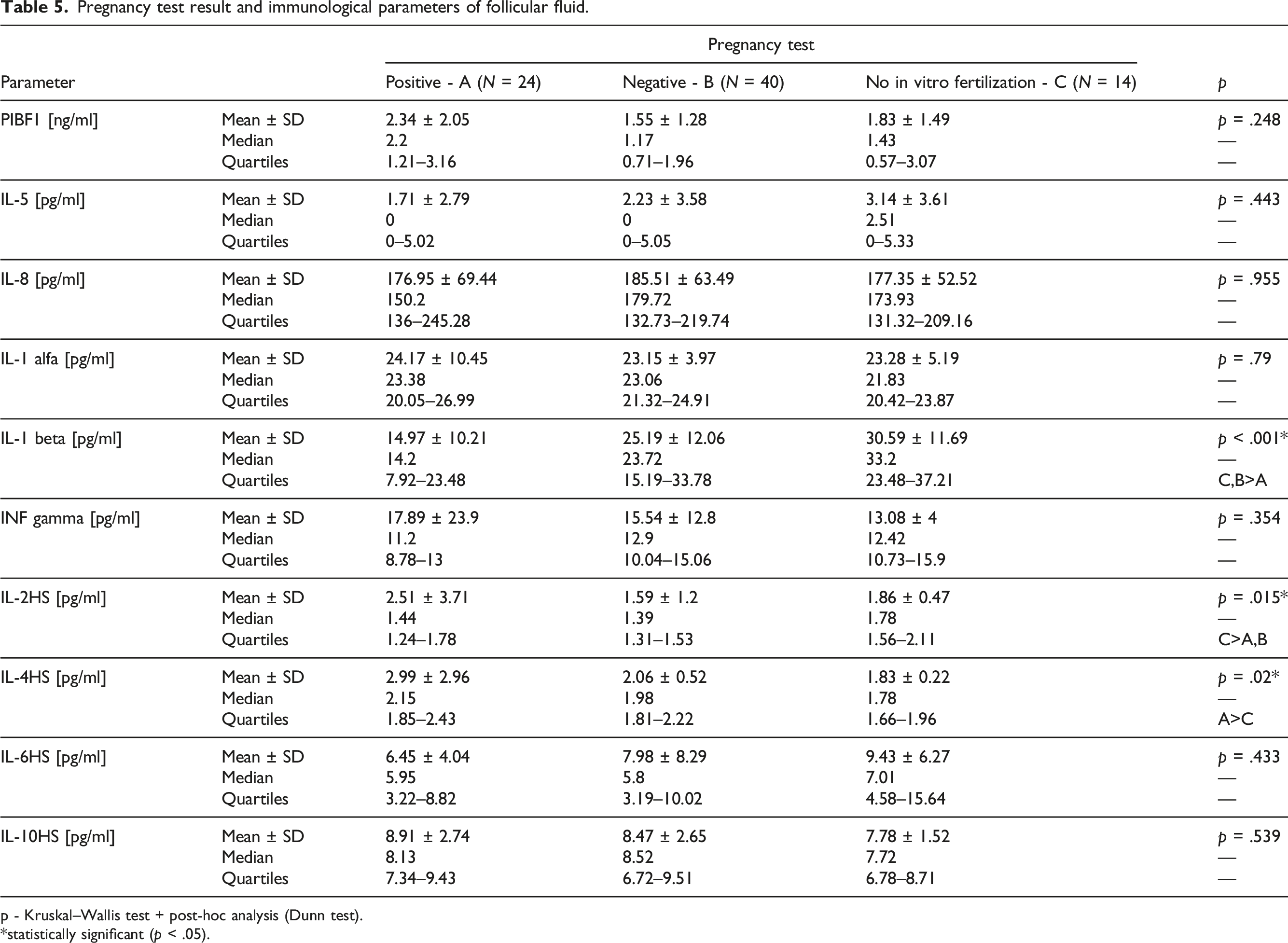
p - Kruskal–Wallis test + post-hoc analysis (Dunn test).
*statistically significant (p < .05).
Noteworthily, when dividing the study group into two categories, of women below and above 35 years old, IL-8 concentration was found to be significantly higher in the group ≥ 35 years old.
When analyzing the primary reason for infertility, the level of IL-1 alfa was found to be statistically significantly higher for patients with unspecified female infertility than for those with infertility of tubal origin, PCOS, or male-associated infertility. IL-10 was found to be higher in patients with tubal infertility and PCOS than in other groups. Moreover, body weight, as well as BMI, correlated positively with IL-6 concentration in FF.
Ovum and embryo quality and the chance of positive pregnancy test.

p - univariate logistic regression.
Immunological profile of follicular fluid and its influence on the number cumulus-oocyte complexes, metaphase II, and top quality embryo.

*statistically significant (p < 0.05).
Discussion
The success rate of IVF-ET is still not high, and therefore, it is important to identify the factors influencing the outcomes of IVF-ET. The fetus is a semi-allograft, and progesterone can prevent its rejection by regulating the PIBF. PIBF is produced by the binding of progesterone to progesterone receptors on lymphocytes. 6
Progesterone-induced blocking factor takes part in the modification of the immune system of pregnant women. In physiological pregnancy, a Th2-dominant cytokine balance is typical. PIBF up-regulates Th2-related cytokines and down-regulates NK activity. The smaller PIBF isoforms bind to a novel form of the IL-4 receptor and induce increased production of IL-3, IL-4, and IL-10, which leads to the shift toward Th2 response. 15
In most studies, PIBF is measured in urine and blood serum and has been noted to increase in a normal pregnancy. However, it fails to increase in women with pregnancy termination and preterm births. 16 On this note, Hudic et al. published an interesting study in 2020. The researchers analyzed the concentration of PIBF in 120 women undergoing IVF-ET. The blood and urine were taken 14 days after embryo transfer together with beta hCG. Of the research group, 78 patients had a positive and 42 had a negative pregnancy test. Among women with a negative beta hCG value (non-pregnant women), the mean concentrations of PIBF in urine and serum were significantly lower than those in women with a positive beta hCG value (pregnant women). Among the pregnant patients, for 49 patients, the pregnancy terminated with a term delivery, for 10 patients, it terminated with a preterm delivery, while for 19 patients, the pregnancy terminated with a miscarriage. PIBF concentrations in the urine and serum samples of women who had experienced a miscarriage were significantly lower than those in women who gave birth. It was found that successful pregnancy after the IVF procedure can be predicted by measuring urine and serum PIBF concentrations. This means that PIBF could be considered a marker of high-risk pregnancy. 17
To our knowledge, our study is the first to analyze PIBF1 concentration in the FF of women who are undergoing IVF. The concentration of PIBF 1 in FF obtained during ovarian puncture was found to positively correlate with the number of MII and top-quality embryos in patients. Further analysis shows that the number of MII and top-quality embryos that were achieved during ovarian stimulation and the IVF procedure directly influences the OR of pregnancy (increasing the chance of pregnancy by 66.6% for every top-quality embryo and 21.3% for every additional MII). This demonstrates that PIBF concentration is important not only in pregnancy development but also before and during ovum maturation and embryo development.
Some pieces of evidence suggest that modifying progesterone–PIBF1 signaling pathways may influence the chances of a successful pregnancy. In B cell-deficient mice, lower basal and lipopolysaccharide (LPS)-induced expression of PIBF1 in the late gestation uterine tissue was observed. LPS-induced PIBF 1 expression was restored through adoptive B cell transfer and the administration of the recombinant human PIBF1, which decreased LPS-induced uterine inflammation and preterm labor and neonatal mortality. 18
Progesterone-induced blocking factor1 has also proven to be an influence on some types of malignant tumors, such as triple-negative breast cancer. 19 In a 2010 review article, PIBF was called a double-edged sword due to its positive influence on facilitating a healthy pregnancy and, conversely, the promotion of tumor cells. 20 Some aspects of pregnancy and malignancy are, in fact, alike. Pregnancy and malignancy share certain characteristics, for example, rapid proliferation, the capacity to invade normal tissue, and the need to evade immune surveillance because they contain antigens foreign to the host. 21
O’Brien et al. published a relevant study in 2019. They compared the FF, AMH, and progesterone (P4) concentrations of follicles in which the oocyte on the fifth day developed into a blastocyst (Group 1) with the FF concentrations of oocytes that failed to reach the blastocyst stage (Group 2). The authors found that FF-AMH and P4 levels significantly increased in Group 1. 22 Thus, progesterone exposure can induce PIBF not only in women but also in men.23,24 An interesting subject for further studies would be to consider the levels of progesterone and PIBF in FF. Moreover, an intriguing hypothesis is whether the ratio of P4 and PIBF could be the best way to predict oocyte quality.
In our study, the IL-1 β concentration was lower in the FF of patients with successful IVF. This finding is in line with the findings obtained in previous studies. Although in the case of the current study, the concentration of IL-1 β was measured not in the sera but in the FF obtained during ovarian puncture. In 2018, Kreines et al. examined the levels of IL-1 β in the blood serum of 205 women undergoing IVF. The serum levels were measured prospectively, before the cycle, at the time of human chorionic gonadotropin administration, on day 24 of the IVF cycle, day 28, and day 35. They found that increased IL-1β serum levels were associated with a viable pregnancy. However, no increase in serum levels was observed for those with subsequent pregnancy loss. Additionally, detectable IL-1β levels at the start of the cycle were associated with successful IVF outcomes (p = .027). 25
Khadem et al. found that in 76 women undergoing IVF/ICSI, a higher concentration of IL-1 in the endometrial secretion, aspirated before performing the oocyte collection, was associated with successful chemical pregnancies (p = .00). 26
In a different study based on 33 women undergoing IVF-ET, the implantation rate indicated significantly higher amounts of FF IL-1 β in the implantation versus non-implantation cycles. 27 These results seem to be in line with our findings.
IL-8 is an important cytokine for inflammatory processes and angiogenesis. It is neutrophil-specific and plays a crucial role in the second, LH-dependent phase of follicle development, mainly characterized by follicular growth. IL-8 is assumed to play important role in the FF of women undergoing IVF.28–30
As mentioned earlier, the current study found that a higher number of COC-1 and MII cells increase the chance of successful IVF, and higher IL-8 concentration in FF is gathered with a higher number of COC-1, MII, and top-quality embryos.
Sarapik et al. presented an analysis of a wide range of cytokines and chemokines in FF collected from women undergoing IVF. The researchers found that low IL-18 concentration was characteristic of unexplained infertility and a higher concentration of IL-12 correlated with the successful fertilization of the ovum and development of an embryo. Conversely, higher concentrations of IL-18, IL-8, and MIP-1β were associated with the patient’s successful IVF, defined as pregnancy diagnosis using ultrasound examination 6–7 weeks after IVF. 31
In the current study, IL-8 concentration was found to be significantly higher in the group ≥35 years old. This result contradicts that of Piccinni et al., who in 83 women with regular menstruation, who decided to have ovarian tissue cryopreservation (OTC) due to necessary oncological treatment, found a correlation between the age of the patients and the concentration of individual cytokines. For women less than 30 years old, as opposed to women more than 30 years old, lower levels of IL-5 and higher levels of IL-1Ra, IL-5, IL-8, eotaxin, and RANTES were observed. 32
Another study revealed the elevated concentration of other cytokines such as IL-8, IL-6, and TNF-α in the peritoneal fluid and IL-1β and IL-6 in the serum of patients with severe ovarian hyperstimulation syndrome. 33
Our results show that IL-2 and IL-6 concentration in the FF had a positive correlation with the number of COC-1 and MII. Importantly, the body weight, as well as the BMI, correlated positively with IL-6 concentration in the FF. Wang et al. analyzed the concentrations of IL-6, IL-10, IL-13, and TNF-α in the peritoneal fluid and found significantly higher concentrations of these cytokines in patients with infertility and endometriosis as compared with the control group of healthy women. 34
In 2020, Kuang et al. analyzed the cytokine concentration in the blood serum of 78 infertile women. The higher concentrations of IL-17a, IL-1Ra, and IL-6 were characteristic of the 49 patients with diagnosed PCOS, indicating a subclinical inflammation characteristic of this group of patients. 35 Moreover, a higher concentration of IL-6, among other cytokines, such as IL-1 or TNF- α, is characteristic of obese women. 36 This is in line with our current results.
There are other possible reasons exist for the increased concentration of IL-6 in serum and other fluids. The promotion of malignant neoplasm development may be gathered with increased levels of some cytokines, for example, IL-6. 37 Furthermore, during the COVID-19 pandemic, IL-6 and IL-8 were found to be clinically important markers of the cytokine storm. The concentration assessment of these cytokines was used to predict the course of the disease and help decide on the most adequate treatment. 38
The interactions between the current state of health of a patient and other factors (besides infertility) for the elevated concentration of cytokines and the interaction between cytokines in the FF and the blood serum are complex. Still, the rate of success of IVF is unsatisfying. Finding universal immunological markers of IVF success or failure is a challenging goal but one that could potentially provide a patient with better insight into their treatment options. An individualized approach to infertility treatment also targeted to specific cytokine profiles could potentially benefit patients’ chances of successful conception. Is a biological treatment aimed at a specific immunological path in the future? As far as we know, a biological treatment used in, for example, arthritis or allergies, can be relatively safe in pregnant or breastfeeding women. However, more studies are needed to establish if the chances of successful IVF could increase as a result. Addressing this gap might be difficult due to bioethical concerns.39–41
The main limitation of this study is its relatively small and diverse research population. A sample size/power analysis was not performed, and the number of patients was based on previous research and the financial support received. Another limitation was that the interview questionnaire was not pilot-tested before the study. The questionnaire was based on a similar one, used in our previous research, and modified for the purpose of the current study. Still, a pilot study would allow to better access the quality of interview cards used. Another limitation is that the study is based on only the analysis of FF cytokines, and a serum immunoassay was not performed. Bersinger et al. analyzed thirteen cytokines in matched serum and FF samples and found IL-4, TNF-α, RANTES, eotaxin, and interferon-gamma-induced protein-10 concentrations were lower in the FF than in the serum. The IL-6, IL-8, IL-10, IL-18, monocyte chemotactic protein-1 (MCP-1), VEGF, and leukemia inhibitory factor (LIF) showed higher median levels in FF than in serum, indicating possible ovarian production. 42 Both 90 kDa PIBF protein and 35 kDa splice variant were recognized by the immunoassay. One might suspect different influences on the oocyte and embryo development depending on the variant. This aspect would require further study. Moreover, analyzing the cytokine profiles of blood serum and FF in selected groups of patients suffering from, for example, PCOS or endometriosis would be beneficial.
Conclusion
FF is rich in cytokines, which play a role in the development and maturation of oocytes. The current study was the first to acknowledge that higher PIBF1 concentration in the FF is related to a higher number of top-quality embryos. One of the most important parameters for assessing the possibility of successful IVF is the archived number of top-quality embryos. IL-1 beta concentration was found to be lower in the FF of patients with successful IVF. In women, ≥ 35 years old IL-8 concentration was found to be significantly higher than in younger women. These observations may be of importance when analyzing the cytokine profile of FF. PIBF1 and IL-1 beta in FF could be candidates for a marker of successful IVF.
Nevertheless, further studies are required because the interpretation of cytokine profile results is difficult due to the many factors involved in promoting the production of cytokines. Finding universal immunological markers of IVF success or failure is a demanding goal, requiring further in-depth studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University, internal funding.
Ethical approval
The study was approved by the Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Torun, Bioethical Committee and was assigned a classification number: KB 334/2021.
Informed consent
Written informed consent was obtained from all subjects before the study.
Appendix
Clinical observation card
Medical history number
Date of examination
Date of birth
WeightHeight
SmokingYes/No
Family history
General clinical signs.
Chronic diseases
Pharmacotherapy
Medical history
Fertility
Date 1 of menstruation, length of cycle, regular/irregular
Children Yes/NoHow many
PregnanciesMiscarriage
Difficulty getting pregnantYes/No
If so:
The course of infertility treatment
Length of treatment
Diagnosis(the main cause of infertility)
Results of diagnostic procedures and other results