
Abstract
Introduction
The Innate immune system senses danger signals of COVID-19 infection and produce an orchestration of cellular, complement and cytokines cascades. These led to the approach using immunosuppressive agents. It is intriguing whether certain biomarkers can aid the proper administration of such drugs.
Methods
Plasma specimens of 58 COVID-19 patients with differing severity, from very mild illness (group A), mild (group B), moderate (group C), and severe/critical illness (group D) were assayed for cyto-chemokines and terminal complement complex (SC5b-9) during the course of diseases. None received anti-IL-6 therapy, there was no mortality in this cohort.
Results
IP-10 and RANTES levels were dominant cytokines. IP-10 levels increased significantly in all groups when compared between pre-nadir and nadir phases (group A, p =0.428; group B =0.034; group C =0.159; group D <0.001) and in groups B and D when compared between nadir and recovery phases (p <0.001). RANTES levels were elevated in all groups across all phases with no significant differences. SC5b-9 levels increased significantly as compared to healthy controls [pre-nadir- group A versus healthy, p =0.122; group B-D versus healthy, p =0.021); nadir-group A versus healthy, p =0.003; group B-D versus healthy, p <0.001; recovery phase (p <0.001)] but not between groups A and B-D at pre-nadir (p=0.606).
Conclusion
The absence of significant pro-inflammatory responses and early elevation of IP-10 levels and complement activation may be favorable and necessary for viral elimination in COVID-19 patients. Expression of distinct cyto-chemokines during each clinical phase may be useful for guiding proper therapeutic interventions on alleviating thrombo-inflammation responses to COVID-19 infection.
Introduction
Coronavirus Disease 2019 (COVID-19) is one of the most devastating pandemics. Thailand was the first country outside China to encounter COVID-19 in January 2, 2020. 1 Several complications arising from the virus due to aberrant immune activation have been recognized.
The innate immune system in response to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) produces an orchestration of cellular, complement and cytokines cascades. Among which, neutrophil extracellular traps (NETs) elicited by neutrophil response are readily recognized as an initial response followed by IL-8, sIL6R alpha, IL-1 beta and IL-6, TNF alpha, with dysregulation of Th1 and Th2, resulting in a cytokine storm (NETS-cytokine loop).2,3 IL-17 A, a key molecule of innate and adaptive immunity, is biased towards the innate system in the presence of IL-17 and -23 cytokine.4,5 Cytotoxic CD 8+ T cells, via antibody-dependent cell–mediated cytotoxicity have an important role in clearing the viruses, however, its cytotoxic effect can also cause severe lung parenchymal damage. 6 The aforementioned inflammation induced by the virus are inadequately regulated by anti-inflammatory mechanisms, such as macrophage inhibitory factor (MIF), IL-10, and IL-11. 7 Lack of immunological homeostasis results in alveolar space filled with counterproductive immunogenic debris and concomitant fibrotic lung repair leading to exaggerated response to further hypoxemia and resulting in death. 8 Thus, exaggerated innate response has been considered critical in respiratory failure with or without multi-system inflammatory manifestations and are considered to be correlated with clinical outcomes.9-12
The expression of a triad of cytokines, interleukin (IL)-6, IL-10, and interferon (IFN)-γ-induced protein 10 (IP-10), is closely correlated with disease progression. 13 Serial IP-10 measurements have been suggested as an aid in managing inflammation in COVID-19 patients and therapeutic decision-making.14-16 Nevertheless, expression of clinical phenotypes may also depend on underlying or pre-existing inflammatory or immune conditions as shown in a case of cystic fibrosis who had pneumonia with COVID-19 with an uneventful outcome. She had lower immune activation responses as compared to the assay prior to the infection; these included IL-6, CCL2, CCL5, CXCL8, CXCL9, and IP-10. 17
In another study, IP-10 tends to elevate earlier in COVID-19 patients than other inflammatory cytokines. 18 Complement activation is one element of innate defenses. Its activation has been considered to play role in immune exaggeration response and damage.19,20
Therapeutic trials in blocking C5a receptors are underway.21-23 Yet, there has been uncertainty at which point blocking of the complement activation would be most beneficial. Current management consists of prompt administration of an anti-viral drug, such as Favipiravir or Remdesivir, thereby reducing viral replication. Expeditious use of anti-inflammatory drugs (such as dexamethasone and anti-IL6 receptor) in a timely manner may help mitigate severe pneumonia.24,25 However, excessive use may prone to superimposed infections resulting to increase mortality and prolonged hospital stay. The complement system, as mentioned above, plays an ambiguous role during COVID-19 infection. While it may be needed to control infection during asymptomatic or early phase with mild symptoms, complement activation, due to its potent pro-inflammatory effect, may also contribute to several pathologies observed in severe COVID-19 patients. 26
The pro-inflammatory and pro-thrombotic state associated with COVID-19 resembles that observed in patients with various auto-immune/-inflammatory disorders in which the complement system is involved. Prediction degree of severity by monitoring as early as possible onwards the thrombo-inflammatory and complement activation profiles may act as a guide for administration of immunosuppressive and complement blockade. 27
We examined blood specimens of 58 patients with differing COVID-19 severity during the course of the disease. This allowed us to construct the dynamic course of cyto-chemokines and complement activation to determine whether there are candidates for predicting outcomes.
Methods
Blood samples were collected and serum and plasma were prepared within 60 min of venipuncture and kept frozen under −80°C until assay. Samples examined in this study were left over specimens from confirmed COVID-19 patients admitted to King Chulalongkorn Memorial Hospital (KCMH) between March and April 2020 were used. The requirement of informed consent was waived by the Institutional Review Board/Ethics Committee of Chulalongkorn University (IRB 400/63) according to the descriptive-retrospective nature of the study. Since specimens were not adequate for all assays, 76 samples from 24 patients and 104 from 34 patients were assayed for cyto- and chemokines and for terminal complement complex (SC5b-9) respectively. 52 healthy blood donors not previously infected by SARS-Cov-2 served as controls for SC5b-9 assay. They were screened negative for COVID-19 Antibody (IgM, IgG, and neutralizing). 28 COVID-19 was confirmed by real-time RT-PCR (rRT-PCR) as per protocol mentioned in previous study. 1 Analyses of viral load shown as cycle threshold (Ct) value, where higher viral load is indicated by a lower Ct value.
Disease severity of patients was categorized based on CDC criteria 29 with minor modification. Group A was asymptomatic at first and had progression to very mild illness with no abnormal chest imaging (21 patients), B had mild illness without shortness of breath, dyspnea but with minimal infiltration on chest imaging, 25 C moderate illness with evidence of lower respiratory disease, by clinical assessment or imaging, and a saturation of oxygen (SpO2) ≥94% on room air at sea level (4 patients) and D severe/critical illness. 25 Severe illness: individuals who had respiratory frequency >30 breaths per minute, SpO2 <94% on room air at sea level (or, for patients with chronic hypoxemia, a decrease from baseline of >3%), a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, or lung infiltrates >50%. Critical Illness: Individuals who had respiratory failure, septic shock, and/or multiple organ dysfunction.
Analysis of laboratory assays in this study was done according to clinical status at each time interval as pre-nadir, nadir and recovery phase. Each particular phase was defined by a team of physicians including internists and those in subspecialties (critical care, pulmonary, nephrology, cardiology, neurology, infectious disease, etc.) during hospitalization since admission. The decision to transfer patients to higher step-care facilities, equipment from oxygenation and high flow, intubation with ventilator and other life supports was made by agreement among internists and subspecialty accordingly. Monitoring details include criteria of severity, general wellbeing, systemic symptoms, vital signs, cardiopulmonary and renal functions, and basic and special laboratory measures where all of them were used to define at which time point additional measures and medications would be applied. Clinical data were also reanalyzed retrospectively in order to reassure at which exact clinical phase each blood sample was collected whether it was in the pre-nadir, nadir, or recovery phase.
Assay for cytokines and chemokines include 5 patients in Group A (13 samples), 13 patients in group B (39 samples), 2 patients in group C (12 samples), and 4 patients in group D (12 samples).
Assay for SC5b-9 includes 16 patients in Group A (52 samples), 13 patients in Group B (34 samples), 2 patients in Group C (8 samples), 3 patients in Group D (10 samples).
Human cytokines and chemokines panel, 48-plex.
Measurement of the levels of the terminal complement complex (SC5b-9) was performed using CUSABIO® Human Terminal Complement Complex SC5b-9 ELISA Kit (CUSABIO, WU, China) according to the manufacturer’s instructions.
Statistical analysis
Cyto- and chemokines results were reported according to xPONENT® Software (Bio-Rad, California) and were designated as a cut-off value using Analysis of Variance (ANOVA). Customized Scatter Plots were generated using Chart studio-plotly.
SC5b-9 results were reported according to Varioskan® Flash (SkanIt Software 2.4.5 RE) and were designated as a cut-off value using Four parameter logistic (4PL) curve. Customized Scatter Plots were generated using Chart studio-plotly. Correlation statistics were undertaken using MedCalc. P<0.05 (two-tailed) was considered statistically significant.
Cut-off values of chemokines and cytokines were derived from data points of each group across all different phases using the software described above. Levels of less than 5000 pg/mL were designated as a cut-off value. Cut-off value for SC5b-9 was 43 ng/mL based on determination of 52 samples from 52 healthy non–COVID-19 blood donors.
Results
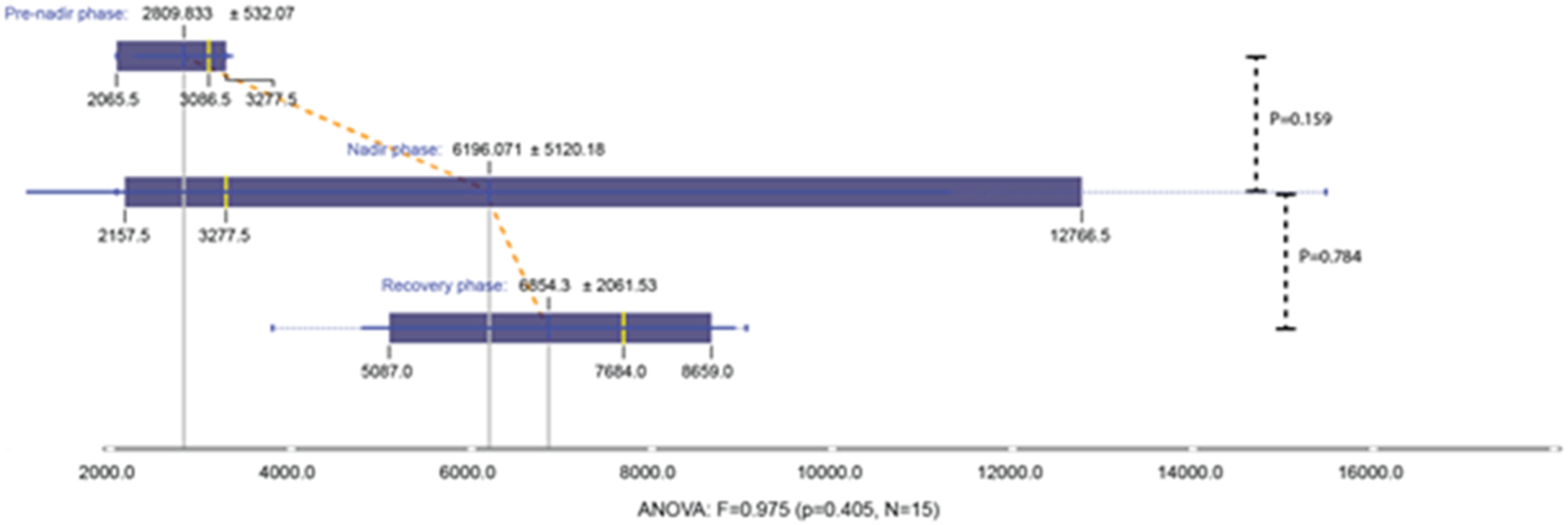
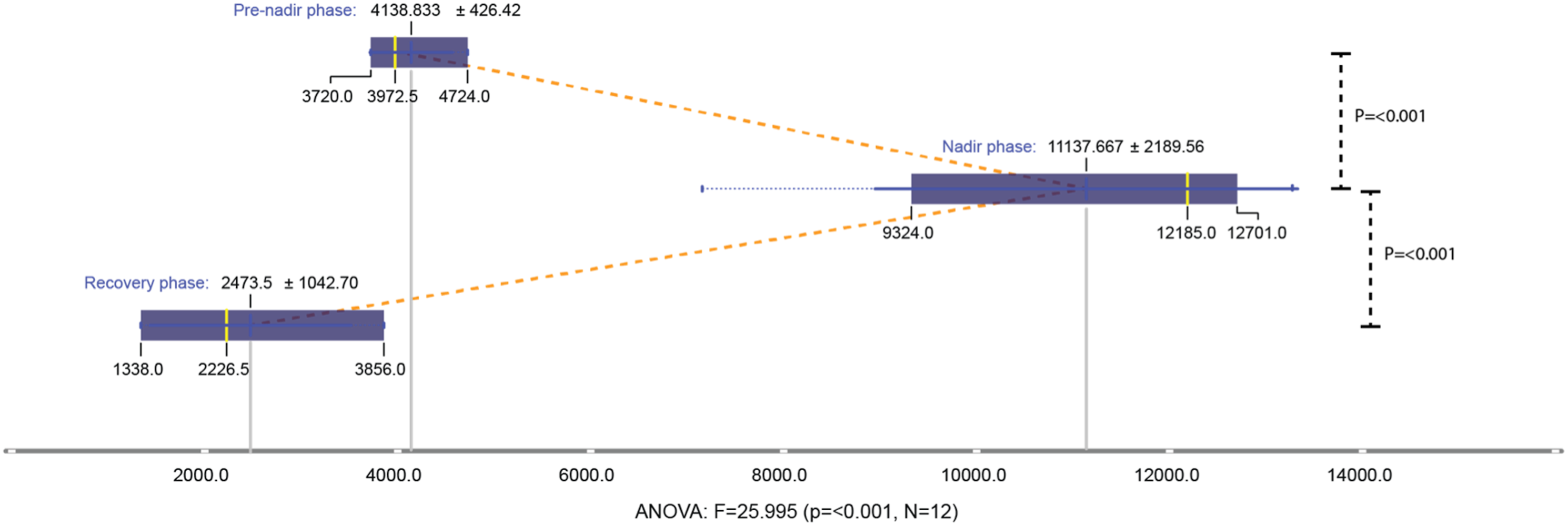
IP-10 and RANTES were the dominant cytokines found with levels consistently over 5000 pg/mL. IP-10 levels increased from the beginning in all groups. Levels increased significantly when compared between pre-nadir and nadir phases (group A, p =0.428; group B =0.034; group C =0.159; group D <0.001). Significant levels were found in groups B and D when compared between nadir and recovery phases (p < 0.001) (Figures 1–4). RANTES levels were elevated from the beginning and maintained throughout the entire course of the infection where no significant differences were found in all groups as compared during each particular phase (Figure 5). IP-10 levels of group A (very mild illness) during pre-nadir, nadir, and recovery phases. Levels were statistically elevated (T-Test p =0.428) as compared between levels during pre-nadir and nadir phases. Values in the figure represent mean ±2 SD (dark blue vertical line) and median (dotted yellow vertical line). Analysis of variance (ANOVA) shows non-significant value (ANOVA p =0.788, N=13). IP-10 levels of group B (mild illness) during pre-nadir, nadir, and recovery phases. Levels were statistically elevated as compared between levels during pre-nadir and nadir phases (T-Test p =0.034) and those during nadir and recovery phases (T-Test p <0.001). Values in the figure represent mean ±2 SD (dark blue vertical line) and median (dotted yellow vertical line). Analysis of variance (ANOVA) shows significant value (ANOVA p <0.001, N=39). IP-10 levels of group C (Moderate illness) during pre-nadir, nadir, and recovery phases. Levels were statistically elevated as compared between levels during pre-nadir and nadir phases (T-Test p =0.0159) and those during nadir and recovery phases (T-Test p =0.784). Values in the figure represent mean ±2 SD (dark blue vertical line) and median (dotted yellow vertical line). Analysis of variance (ANOVA) shows significant value (ANOVA p =0.405, N=15). IP-10 levels of group D (Severe/critical illness) during pre-nadir, nadir, and recovery phases. Levels were statistically elevated as compared between levels during pre-nadir and nadir phases (T-Test p <0.001) and those during nadir and recovery phases (T-Test p <0.001). Values in the figure represent mean ±2 SD (dark blue vertical line) and median (dotted yellow vertical line). Analysis of variance (ANOVA) shows significant value (ANOVA p <0.001, N=12). Levels of RANTES were comparable among all patients of different grades during all phases of the disease.


Mixed pattern of cyto- and chemokine responses were found in three patients, one from group B and two from group D all with superimposed bacterial infections. One patient in group D had RANTES, IP-10 and SCGF-b during pre-nadir phase. The remaining two patients had RANTES, IP-10, IL-6, MCP-1, and sCGF-b during nadir phase. One patient in group B in addition to previously mentioned cytokine response also had IL-1b, MIP-1a, IL-8, GROa, and MCP-3 during nadir phase. RANTES was found in all three during recovery phase.
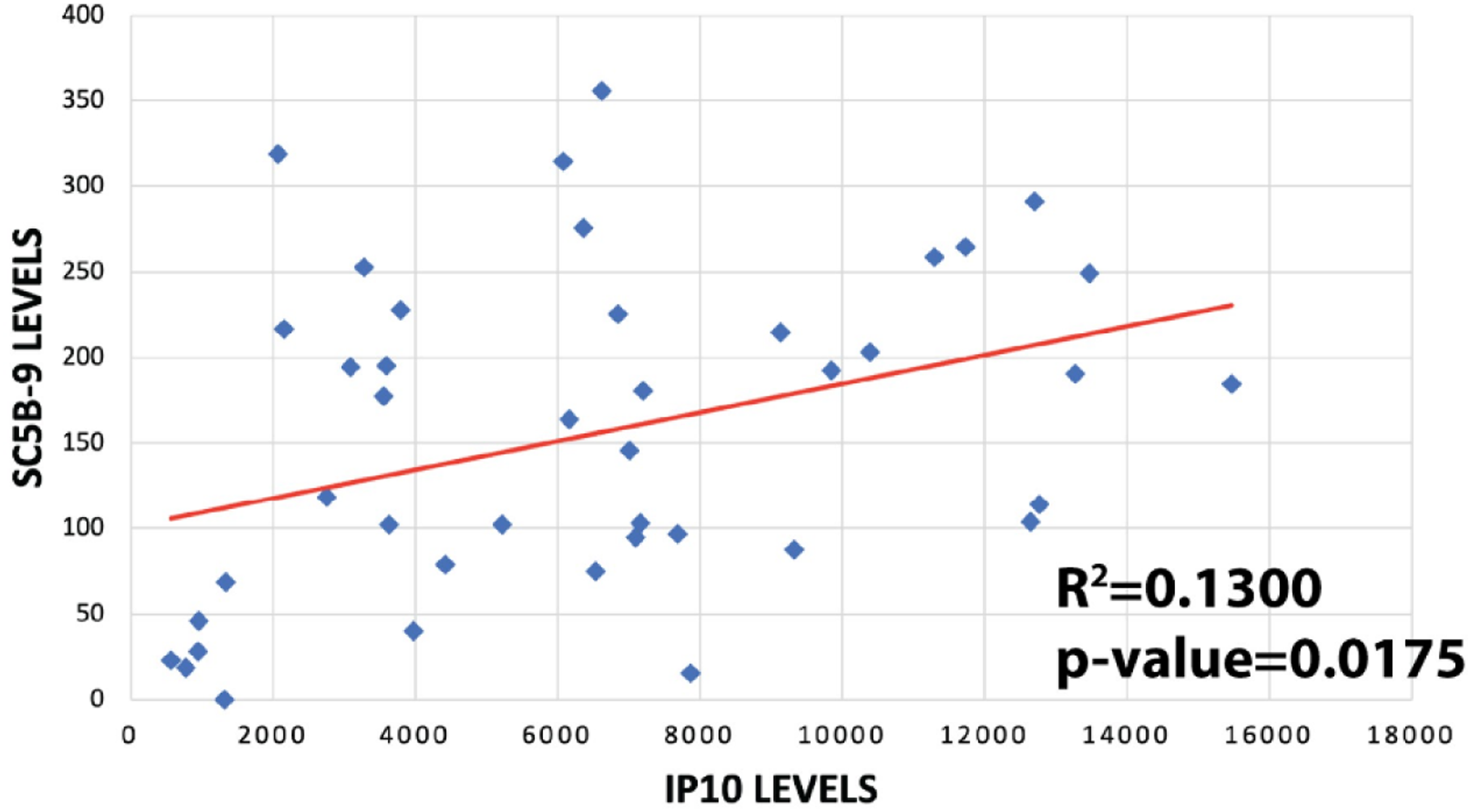
The increase in SC5b-9 levels was also observed from the beginning of the infection with its values increased significantly in group A and groups B, C, and D (group B–D). During pre-nadir phase, levels of SC5b-9 were significantly elevated as compared to healthy controls (group A vs healthy, p =0.122; group B-D vs healthy, p =0.021). Levels remained significant during nadir phase (group A vs healthy, p =0.003; group B–D vs healthy, p <0.001) and during recovery phase (p <0.001). Levels between group A and group B–D were significant during nadir and recovery phases (Figure 6). Significantly correlation was found SC5b-9 and IP-10 using by Pearson test (Figure 7). There was a statistically significant difference in SC5b-9 levels between healthy control and group A and group B–D. Significant differences were observed in levels compared between group A and group B–D at all phases except during pre-nadir. AUC values were 0.935, 0.885, and 0.901 during pre-nadir, nadir, and recovery phases, respectively. IP-10 and SC5b-9 levels measured together in 16 of 34 patients are significantly correlated (Pearson correlation test, p = 0.0175).
Discussion
The results of our study suggest similar features of distinct immunophenotype of COVID-19 to what has been previously described. 13 Interestingly, what appeared missing in our COVID-19 patients were IL-6 and IL-10 in all cases with different severity grades during all clinical phases even those with severe/critical illness. It is noted that all 58 patients in this cohort survived uneventfully.
Furthermore, IP-10 levels were significantly elevated since the pre-nadir phase as compared to those in nadir phase in all groups (Figures 1 to 4). IP-10 specifically regulates CD4+ and CD8+ effector T-cells as well as natural killer cells and dendritic cells which serves as frontline defenses. 30 Antonia et al. proposed mechanism of successful Leishmania infection is via pathogen mediated cleavage of IP-10, impairing human’s adaptive immune responses and failure to clear the parasite. 30 In a neuroadapted John Howard Mueller strain of mouse hepatitis virus, IP-10 are responsible for viral suppression after central nervous system inoculation. 31 It remains to study further with larger numbers of patients whether negative pro-inflammatory cytokines (IL-6 and IL-10) plus elevated IP-10 or early elevation of IP-10 alone maybe used as surrogate markers. IP-10 levels remained elevated significantly during the recovery phase in group B and D patients. (Figures 1 to 4).
Additionally, complement activation appeared at significant levels as compared to healthy controls since pre-nadir phase in group A and group B–D and remained significantly elevated throughout the whole clinical course, suggesting immediate host’s response to control and mitigate the infection. 32 No difference in levels was observed between group A and group B–D at all phases except during pre-nadir.
Although complement activation may play an independent role in mediating the release of von Willebrand factor from damaged endothelial cells, 27 complement activation early on and in all phases of infection may be helpful and may represent a mechanism to protect rather than aggravate the disease. Such activation remained throughout the whole clinical course until recovery. Combining complement activation with cyto-chemokine responses in the future study would clarify at which time points that innate response may be friend or foe and whether complement activation may curtail the viral persistence.
Chemo- and cytokine profile also differed between those with COVID-19 alone and with a superimposed bacterial infection. Responses other than IL-6, IL-10, and IP-10 were found elevated in all three patients with superimposed bacterial infection. However, such a small number of samples may be premature to conclude that a wider response may suggest mixed infection with bacteria. Apart from the limited sample size, the only controls are healthy subjects. Immunologic profiles need to be compared between ARDS patients with bacterial infections and those with COVID-19.
Conclusion
Treatment of COVID-19 involves managing excessive inflammatory reactions which exaggerate pneumonia severity resulting in increased morbidity and mortality. Hospitals in Thailand other than tertiary centers or teaching hospitals may not have access to investigations such as immune parameters. Hence, management with anti-inflammatory or immunosuppressive with dexamethasone and monoclonal antibody against IL-6 begins once pneumonia ensues. It is still not unanimous when to use or to initiate, and varies based on physician’s decision.
Our limited studies among cohorts with no mortality found IP-10 instead of IL-6, IL-10 and others cytokines such as TNF and IL-1 beta, with their level elevated proportional to the severity. Such elevation can be seen also during the time before entering the critical or nadir phase. Our result does not argue against the detrimental role of IL-6 and IL-10. Their absence suggests otherwise. Defining which cytokines or patterns represent immune signatures by their presence or absence at various time points should be proven and may be valuable in designing pharmacological modulation with the aim to reduce the prolonged use of steroids and other broad-spectrum immunosuppressive. Further, it remains to be determined whether complement activation early on and in all phases of infection may be helpful and may represent a mechanism to protect rather than aggravate the disease.
We are aware that our observation may not apply to the present-day situation where other COVID-19 variants become dominant and may influence our biological response. Limitation to this study includes its retrospective nature as there are many confounding factors that can influence outcome despite care made by a team of physicians in tertiary care facility. These ranged from the rapidity of diagnosis, promptness of commencing anti-viral treatment, recognition of disease progression, and secondary complications both directly from COVID-19 and indirectly from its treatment.
Footnotes
Acknowledgments
We are indebted to the physicians, nurses and all health care workers of the Faculty of Medicine, Chulalongkorn University, King Chulalongkorn Memorial Hospital for taking care of all patients. The study was supported by grant from Thai Red Cross Emerging Infectious Diseases-Health Science Center.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Chulalongkorn University Institutional Review Board (IRB 400/63)
Informed consent
The informed consent is waived off by the Institutional Review Board/Ethics Committee (IRB 400/63).