
Abstract
Sorafenib is a multitargeted kinase inhibitor currently used in the treatment of advanced hepatocellular carcinoma (HCC). It is associated with a significant risk of skin toxicity, which nevertheless represents a clinical marker of good response to treatment. Hand-and-foot skin reaction, alopecia, mucositis, xerosis, skin discoloration, and nail involvement occur frequently in course of therapy. More rarely, sorafenib can target hair follicles. We report the case of a patient who developed painful inflamed nodular-cystic lesions in both pubic and axillary regions in course of treatment with sorafenib. Because of the limited therapeutic options, the patient underwent photodynamic therapy (PDT), a topical treatment which combines a photosensitizing drug applied on lesional skin and a source of light, and had no systemic side effects. At the end of the treatment period, the patient experienced progressive clinical improvement, with relief of the symptoms. PDT may be helpful to limit suffering in patients affected by recalcitrant skin toxicity of the pilosebaceous unit who are not candidates for, or not responsive to, standard therapies.
Keywords
Introduction
Sorafenib is the first oral targeted therapy approved by Food and Drug Administration (FDA) for the treatment of advanced unresectable hepatocellular carcinoma (HCC) in patients with a still preserved liver function who cannot benefit from other therapeutic options. 1 Its use is associated with a number of adverse effects (AEs) including anorexia, diarrhea, nausea, and weight loss. Cutaneous toxicity is very frequent, mainly represented by hyperkeratotic hand and foot syndrome (HFS), a painful complication that usually arises during the early weeks of therapy. Alopecia, mucositis, xerosis, skin discoloration, and nail involvement are also commonly observed in course of treatment. More rarely, sorafenib may target hair follicles. 2 When severe or protracted, skin toxicity can result in significant morbidity, requiring dose modification or drug discontinuation, with consequent dramatic impact on patients’ prognosis. Management of cutaneous AEs may be a real challenge because of the limited therapeutic options in patients with impaired liver function, who are often also affected by multiple comorbidities.
Case report
We report the case of a 55-year-old Caucasian man with a 2 years’ history of multifocal HCC. Liver cancer developed in the context of a cirrhosis related to non-alcoholic steatohepatitis (NASH). At the time of HCC diagnosis, the patient was obese (body mass index (BMI), 36.9), affected by type 2 diabetes treated with oral hypoglycemic agents and by hypertension treated with sartans and diuretics. Blood tests were consistent with a compensated liver cirrhosis (Child-Pugh class A). Contrast-enhanced computed tomography and magnetic resonance revealed the presence of 10 HCC nodules (maximum diameter 2.8 cm) in the right lobe of the liver. He had received transarterial chemoembolization (TACE) with no response, probably because of the low vascularization of the lesions. Thus, treatment with sorafenib 400 mg twice daily had been started, with partial response visible in imaging tests performed during follow-up (no growth of known lesions nor appearance of new ones, while some nodules revealed the presence of necrotic areas). Because of the well-known high risk of hyperkeratotic HFS, the patient was instructed to generously apply emollients on hands and feet, and he developed only minimal skin changes without pain in the first 4 weeks of treatment. Two months after the start of sorafenib, he suddenly developed large painful nodules at inguinal folds, and such lesions progressively spread to trunk and axillae. The patient was treated with systemic antibiotic (amoxicillin 1 g twice daily for 12 days) and topical potent steroids, with no improvement. Because of the worsening of the clinical picture and the very intense pain reported by the patient, the dose of sorafenib was reduced to 400 mg daily, with maintenance of therapeutic efficacy, as confirmed by radiologic response, but no relief on skin toxicity. Physical examination showed multiple inflamed discharging nodules, localized on chest, axillae, lower abdomen, pubis, groin, and genital and gluteal regions (Figure 1). Repeated bacteriological and mycological investigations revealed normal skin microbiota. Histologic examination showed dilated follicular infundibula filled with compact parakeratotic cornified cells and occasional vacuolization and dyskeratosis of the upper follicular epithelial cells. Dilated infundibula were often filled with neutrophils; cells were in some cases necrotic. A heavy infiltration of lymphocytes and plasma cells and, to a lesser extent, granulocytes (mainly neutrophils, with some eosinophils) surrounded follicular units; hyperplastic and dilated vessels were also visible (Figure 2). Such protracted painful eruption severely affected the patient’s quality of life, especially because of the persistent purulent discharge, which interfered with daily activities. Treatment options were limited because of the presence of liver cirrhosis, concomitant illnesses, and related therapies. Systemic steroids were not recommended because of the presence of type 2 diabetes and hypertension, while their topical use was insufficient to control symptoms. Prolonged use of antibiotics was judged inappropriate because of negative microbiological tests. Oral isotretinoin was not considered in view of its potential liver toxicity. In agreement with hepatologists, in order to avoid treatment discontinuation, we decided to start anti-inflammatory photodynamic therapy (PDT) using aminolevulinic acid (ALA) as porphyrin precursor. After obtaining written informed consent, 10% ALA in polyethylene glycol ointment was applied in occlusion for 3 h on lesional and perilesional skin of pubis and chest; irradiation was then applied with diode red light at 630 nm. The light source was positioned at 50 mm from skin surface, thus achieving an irradiance of about 160 mW/cm2. The light exposure period was 8 min, resulting in a total light dose of 75 J/cm2. Fluorescence was detected using violet light at 405 nm and, after ALA application, was localized with high intensity in many inflammatory nodules. A visual analogue scale (VAS) was used to assess pain intensity. The patient was treated every 2 weeks for a total of four treatments. Severe reactions were referred after the first two sessions (mean VAS values, 9), with moderate discomfort recorded in the successive exposures (mean VAS values, 6). The treatment did not prevent the onset of new lesions, but determined progressive improvement of those already present, with marked reduction of purulent discharge and pain, ultimately resulting in improved quality of life (Figure 3). Skin eruption quickly stopped after drug discontinuation because of liver transplantation. At 6-month follow-up, only hyperpigmented scars were observed. A written informed consent for patient information and images to be published in the study was provided by the patient.

Diffuse involvement of trunk (a) with many closed comedones (b) and inflamed nodules with purulent discharge (c).

Dilated follicular infundibula filled with compact parakeratotic cornified cells and occasional vacuolization and dyskeratosis of the upper follicular epithelial cells (a, hematoxylin and eosin stain; original magnification, ×20). Dilated infundibula were often filled by neutrophils with some necrotic cells (b, hematoxylin and eosin stain; original magnification, ×40). A heavy lympho-plasmacytic infiltration with an amount of granulocytes mainly neutrophils with some eosinophils surrounded the follicular units in association with hyperplastic and dilated vessels (c, hematoxylin and eosin stain; original magnification, ×60).
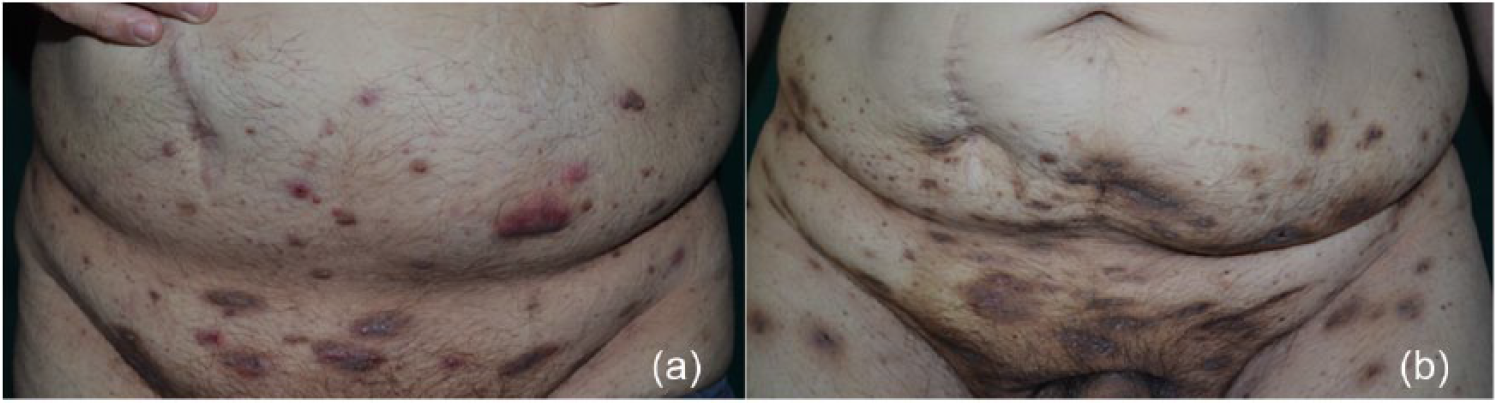
Clinical aspect of lower abdomen and pubis (a) before and (b) after four treatments with photodynamic therapy. The treatment did not prevent the onset of new lesions, but determined the progressive improvement of those already present, with marked reduction of purulent discharge.
Discussion
In the last decade, the increased understanding of the molecular mechanisms involved in tumor development and progression has dramatically changed the therapeutic approach to HCC, with development of targeted therapies tailored on the specific disease, differently from traditional chemotherapies. Compared to cytotoxic drugs, these “biologic” therapies are better tolerated, even if they share many cutaneous adverse events with traditional drugs.2–5 Nevertheless, an increasing number of oncologic patients experience multi-organ toxicities that reflect the effects of the drug on targets not relevant to tumor response and the impact of toxic metabolites. 6 More significantly, many of these toxicities are associated with the impact of the drug on its target, thus representing a potentially reliable clinical biomarker to detect best responders among patients. About sorafenib, a recent meta-analysis on HCC-treated patients demonstrated that the occurrence of cutaneous adverse events is associated with a better overall survival (OS). Pooled hazard ratios for OS for patients developing HFS or skin toxicities of any kind were 0.47 (95% confidence interval (CI): 0.35–0.62; P < 0.00001) and 0.51 (95% CI: 0.36–0.72; P = 0.0002), respectively. 7 Among the vast array of cutaneous adverse events, follicular involvement has been rarely described in course of sorafenib treatment, with anecdotal reports of perforating folliculitis, keratosis pilaris–like eruption, and follicular hyperplasia.8–11 It has been hypothesized that follicular damage may be the result of a complex mechanism including a possible toxic effect on follicular cells via activation of RAF and other kinases and concomitant inhibition of the platelet-derived growth factor (PDGF) pathway, normally involved in human hair follicle cycle. 12 There is only a report dealing with sorafenib-induced acne inversa-like lesions, with a very limited cutaneous involvement requiring only dose reduction and topical application of fusidic acid. 13 In our patient, the chronically relapsing skin eruption affected large areas of the skin with many giant open comedones and inflamed nodular-cystic elements discharging pus through sinus tracts. The magnitude of skin toxicity was clinically correlated with the good anti-tumoral response, so the dilemma for patient and clinicians was how to manage such painful and distressing folliculitis with no modification of the treatment schedule. In light of the above considerations, and given the few therapeutic options available, we decided to take advantage of the anti-inflammatory properties of PDT. PDT typically involves topical application of the photosensitizing prodrug ALA or its methylated ester (MAL), converted by the heme biosynthetic pathway predominantly to protoporphyrin IX (PpIX) and activated by light of appropriate wavelength to produce reactive oxygen species, especially singlet oxygen, which trigger apoptosis and necrosis of target cells. 14 In addition to anti-tumor activities, experimental studies have demonstrated a variety of anti-inflammatory effects and immunological activities.15–17 The greater absorption of ALA together with higher production of protoporphyrin IX in hair follicles compared to other tissues seem to be the way of action in inflammatory diseases of the pilosebaceous unit like chronic folliculitis and hidradenitis suppurativa.18–20 Treatment is generally considered well tolerated, with pain as the main AE. PDT can be easily repeated, with no systemic absorption of the photosensitizer nor pharmacological interaction with concomitantly administered systemic drugs, thus allowing to treat patients affected by multiple comorbidities and/or under pharmacological therapies. 21 It must be underlined that in our case PDT did not stop the eruption of new lesions, but helped to control symptoms, giving relief to the patient and avoiding discontinuation of therapy. The final choice cannot preclude the consideration that many chemotherapeutics, such as sorafenib, are of extreme importance in controlling refractory or metastatic cancers, and their discontinuation or replacement can negatively influence the course of the illness and the prognosis of these patients. Off-label PDT may be accounted as a viable option in “difficult” patients who are not candidate for, or not responsive to, standard therapies for recalcitrant skin toxicity of the pilosebaceous unit.
Footnotes
Acknowledgements
All authors have contributed significantly to the paper. F.B. and C.S. contributed to study concept and design. M.V., M.S.F., and M.L. contributed to acquisition of data. F.B., C.S., M.V., M.S.F., and M.L. contributed to analysis and interpretation of data. F.B., C.S., and M.L. contributed to drafting of the manuscript. F.B. and S.P.C. contributed to critical revision of the manuscript for important intellectual content. S.P.C. contributed to study supervision. All authors approved the final version of the submitted paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.