
Abstract
In this study we analyzed the clinical features of a population of Italian patients with chronic fatigue syndrome (CFS) diagnosed according to the CDC-1994 criteria. The aim was to investigate CFS patients and their relatives, in order to search for events related to the onset of the disease and to identify correlations with other diseases. The analysis was carried out by examining medical records belonging to 82 patients suffering from the syndrome. The documentation was collected between 2008 and 2011 and provided by the non-profit Italian organization AMCFS (Associazione Malati di CFS). The influence of gender on the age of onset and association with potential risk factors were investigated in patients and in their relatives. From the results a significant correlation between the age of onset and autoimmunity was observed.
Chronic fatigue syndrome (CFS) is a highly complex and relatively rare disease that has also been referred to as post-infectious or post-viral fatigue syndrome (PVS), myalgic encephalomyelitis (ME), Royal Free disease, chronic mononucleosis, chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME).1–4 The syndrome is still controversial and poorly understood by health professionals and the general population. 5 CFS/ME diagnosis is performed by exclusion and is mainly based on the presence of persistent or recurrent chronic fatigue associated with a range of symptoms, which often fluctuate, sometimes even over short periods of time. Different case definitions were developed for CFS, the most widely used are the criteria established by Centers for Disease Control and prevention in 1994 (CDC-1994). 6 A more recent clinical case definition of CFS/ME was developed in Canada.7,8 As characterized by CDC-1994, CFS/ME is disabling fatigue for 6 or more months, accompanied by four out of eight core symptoms: impaired memory or concentration; headaches; sore throat; lymph node pain; muscle pain; joint pain; unrestoring sleep; and post-exertional malaise. The prevalence of CFS/ME has been estimated to vary among different populations within a range of 0.1–0.4%,9–13 although in some epidemiological studies much higher prevalence values were reported as, for example, in the Hong Kong population in 2005. 14 A recent study 15 in the United Kingdom on 1,000 primary care patients aged 18–64 years was conducted using three different criteria: CDC-1994; Canadian criteria; and epidemiological case definitions (ECD). The estimated minimum prevalence rate of CFS/ME resulted at 0.2% for cases meeting any of the study case definitions, 0.19% for the CDC-1994 definition, 0.11% for the Canadian definition, and 0.03% for the ECD. All but one of the cases conforming to the Canadian criteria also met the CDC-1994 criteria. A meta-analysis 17 demonstrated that the observed heterogeneity in CFS/ME prevalence in different studies is due to differences in the method of assessment and that the 1994 CDC case definition appeared to be the most reliable clinical assessment tool available at that time.
In Italy, a first study on 205 Italian patients with CFS was conducted in 1993, 18 estimating approximately 400,000–500,000 cases of CFS in Italy assuming the same prevalence observed in USA. A further Italian study, 18 evaluated the prevalence of CFS in patients with fatigue who were sent to secondary referral centers in outpatients clinics, identifying 9.5% with CFS according to the Fukuda criteria. A subsequent study in 1999, 19 by the National Institute of Health of Italy, enrolled six national reference centers that identified nearly 100 patients with CFS, where the strict criteria of the CDC-1994 was used. The authors discussed the Holmes and Fukuda criteria and concluded that patients fulfilling the Fukuda criteria were more likely to be men, of upper social class, married, and less likely to have had an acute onset (symptoms and signs of a flu-like disease) with respect to the patients fulfilling the Holmes criteria. In a study published in 2005, the demographic and socioeconomic profile of CFS patients was conducted on a sample of 81 CFS patients aged 18–50 years. 20 The results confirmed the data of the literature with a female:male ratio of 3:1. 21
The Italian National Agency for Regional Health Services (AGENAS) conducted a survey on the prevalence of CFS, using the ICD (International Classification of disease, ninth revision) codes of hospital discharge records between 2001 and 2010. 22 The results led to the conclusion that CFS is not very widespread in Italy with a prevalence in the range of 0.1–0.2%. However, we must consider that these data are probably underestimated because of the controversy existing on the definition and classification of CFS and, in some cases, even on its nosological recognition. 23 The survey using only the most specific code (Chronic Fatigue Syndrome, CFS, code 780.71) showed a higher number of hospitalizations in southern regions than in northern regions with a prevalence in the 45- and 64-year age group and a male:female ratio of 2:1. From all available information concerning Italian CFS patients we can define a profile of Italian CFS patients and, as in the other countries, the majority of cases occur in women, with a median age between 30 and 40 years and with a socioeconomic profile in accordance with the international literature. It is currently difficult to establish the precise CFS prevalence and distribution in Italy in the different regions because of the lack of extensive epidemiologic studies. Some medical centers for CFS were formed spontaneously, supported by patients associations, for a proper diagnosis and for the application of therapeutic strategies that act on the symptoms of the disease. An epidemiological approach with the aim of looking for an association with environmental exposure, and to assess co-morbidity with other pathologies, would be likely to bring some clarity to the field. CFS, like other conditions of unknown etiology, represents a significant cost to the healthcare system due to the need for clinical analysis and admissions leading to improved health status of patients. Some researchers have reported an incre-ased rate of malignancies, multiple sclerosis, and other diseases in patients with CFS, 24 but at present correlations between CFS and other pathologies are not scientifically proven.
The aim of this study is to explore demographic and clinical information on records collected by the Italian non-profit association Associazione Malati CFS (AMCFS), in northern Italy, between 2009 and 2011, in order to analyze the relationship between CFS/ME and other diseases.
Materials and methods
Data collection
Medical records of CFS patients belonging to the Italian AMCFS association were collected according the informed consent methodology and following current ethical procedures for data protection. Eighty-two medical records of patients diagnosed with CFS by the tertiary referral clinical centers in Aviano and/or Chieti, were selected for the study on the basis of the homogeneity of the information contained and in accordance with the CDC-1994 exclusion criteria. In addition, information on the clinical histories of first-degree relatives (parents, siblings, children) and grandparents were acquired by interview.
Statistical analysis
To investigate whether the gender of the patients has influenced the age of onset, a t-test for homogenous variances was performed. A factorial ANOVA was carried out to investigate whether the age of onset of the syndrome differed according to potential risk factors (PRFs) and the parental history of patients’ relatives with autoimmune diseases. As PRFs, only those whose presence was found in at least 10 patients were taken into consideration: depression, allergies/intolerances, autoimmune diseases, markers of hepatitis virus and of herpesvirus 6 (HHV6), were included. All PRFs were modeled as two level factors (yes/no) and no interactions were used. The initial model was then subjected to a stepdown simplification procedure (using the Likelihood-ratio χ2 test), where non-significant terms (P > 0.05) were sequentially removed until obtaining a minimal adequate model, including only significant variables. 26 Statistical analysis was performed using R software version 3.0.1 (R-Development Core Team, 2013 basic package).
Results
The analysis was carried out on data collected by AMCFS, using the consent form methodology and on the basis of the current ethical procedures. The clinical history of 82 CFS patients and of the patients’ first- and second-degree relatives was considered. A first analysis was performed to assess the CFS gender association. The initial exploratory analysis showed a marked difference between men and women as the sample comprised 75.6% women (62 cases) and 24.4% men (20 cases).
In our sample, the age of onset was in the range of 24–67 years, and the average age of onset of this syndrome is approximately 32 ± 1.3 years. To determine whether the age of onset of the disease is influenced by gender, the sample was divided into two sub-samples, distinguishing men and women. As we can observe in Figure 1, the age distributions extracted from the two sub-samples are very similar, with an average value of about 30 ± 2.3 years for men and 33 ± 1.6 years for women. The difference between the two distributions is not significant (t = −0.9894, P = 0.3254). From these data we can assume that the age of onset is not affected by gender.

Age of onset of CFS in the sample population studied. Age distribution of the total samples (a) and of the two sub-samples of men and women.
Patients were sub-grouped according to the different categories identified on the basis of the information reported in the medical records (Figure 2). The most represented categories in our CFS population are: depression, allergy/intolerance, relatives with autoimmune diseases, positivity for HHV6, with a prevalence higher than 20%.
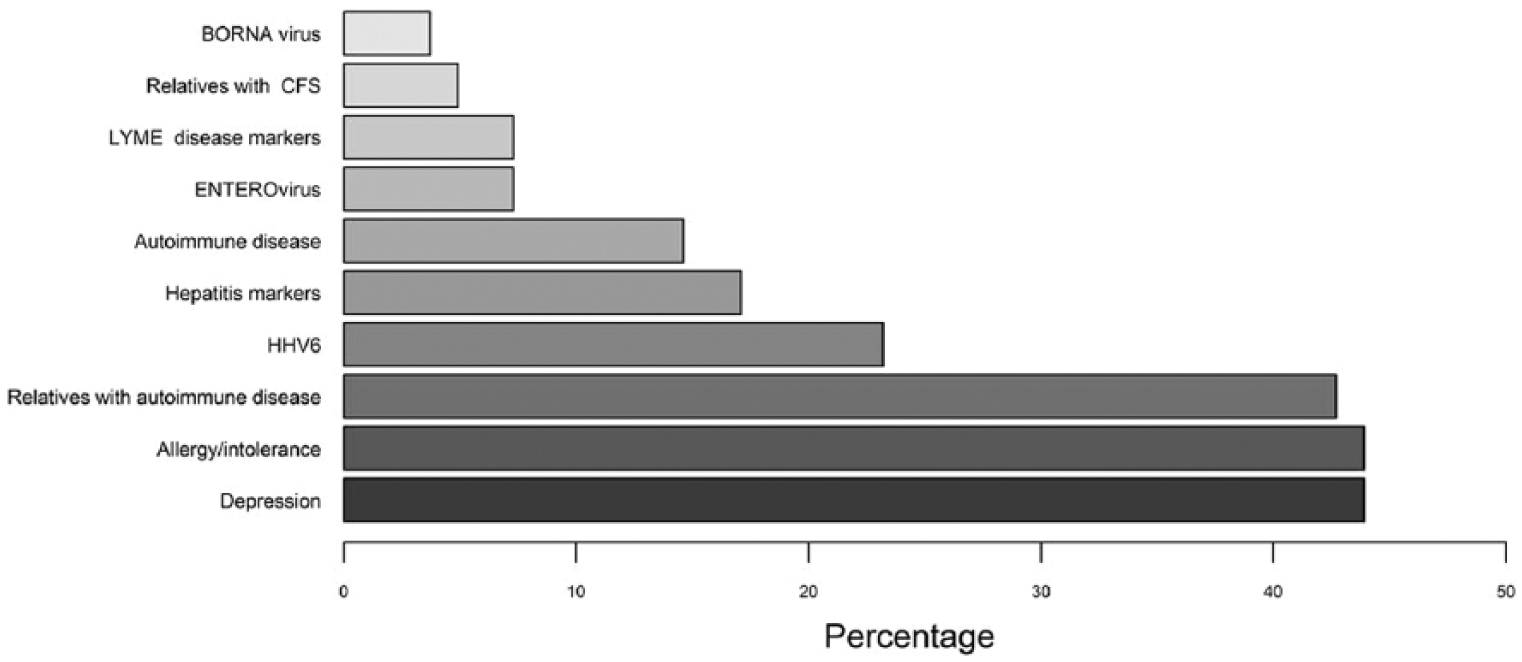
Distribution of the CFS patient population in subgroups.
Allergy and autoimmune diseases are the conditions mainly represented in families with CFS patients with 37 patients (45.7%) suffering from allergies and/or food intolerance and 12 patients (14.6%) with autoimmune diseases. Twenty-two percent of CFS patients have relatives with autoimmune diseases.
The autoimmune conditions reported in the CFS population are: thyroiditis (N = 7), SLE (N = 1), diabetes type 1 (N = 1), rheumatoid arthritis (N = 1), psoriasis (N = 1), and sicca syndrome (N = 1). None of the CFS patients with autoimmune diseases referred more than one type of these diseases.
Autoimmune conditions reported in the relatives’ population are: thyroiditis (N = 5), rheumatoid arthritis (N = 5), diabetes type 1 (N = 5), myasthenia gravis (N = 1), thrombocytopenia (N = 1), and narcolepsy (N = 1).
Depression is present only in CFS patients, with a prevalence of 44%.
Hepatitis markers (HBV and HCV) are present in 14 patients, HHV6 markers in 19 patients, Enterovirus in six patients, Borna virus in three patients, and Lyme disease markers in six patients. Hereditary diseases were not documented in this CFS population and only one of the relatives had a hereditary disease (β-thalassemia). Diagnosis of CFS was not documented for any of the relatives even if a CFS condition could be supposed (but not proven) for three first-grade relatives and one diagnosis of autoimmune thyroiditis was documented.
To understand whether the age of onset is influenced by other conditions, model of analysis of variance (ANOVA) was performed (see Materials and Methods). In Table 1, the PRFs considered are listed and the results of this model are displayed in Figure 3.
The potential risk factors (PRFs) and the corresponding number of patients considered.


Correlation between the age of onset and the presence of autoimmune diseases in the CFS patient population.
It can be observed that, among the PRFs considered, the only one that displayed a significant relationship with the age of onset was the presence of autoimmune diseases: patients with autoimmune diseases showed an average age of onset of approximately 40 ± 3 years, while those without autoimmune diseases showed an average age of 30 ± 1.4 years (F1,80 = 6.979, P = 0.009).
Regarding allergies and intolerances, a negative correlation with the age of onset was observed: patients with allergies/intolerances showed a mean age of onset (29 ± 1.6 years) lower than those without allergies/intolerances (34 ± 1.9 years). This difference is not significant but with a value very close to significance (likelihood ratio χ2: 3.72, df = 1, P = 0.057). No other factor achieved results that were significant or close to significance.
Discussion
From the present analysis on a population of 82 CFS patients from northern Italy, it was found that the average age of onset of this syndrome is about 32 years, with 50% of patients showing the first symptoms between the ages of 24 and 40 years and a prevalence among women (F:M ratio of 3:1). In total, 14.63% of CFS patients suffered from autoimmune diseases. Comparing these data with those reported by a meta-analysis study published in 2009 25 that reviewed the literature and estimated new prevalence values for autoimmune disorders with a range of 7.6–9.4%, it is evident that in our CFS sample there is a further increase in autoimmunity incidence of 5% above the maximum estimated values from this report. Despite the small sample size, this observation needs to be highlighted because this disease was suspected to be of autoimmune origin during the first outbreak known as ‘yuppie flu’ 30 years ago. The prevailing theory during the 1980s and 1990s was that the immune systems of people with CFS simply did not shut down after the initial infection, but remained on ‘high’. CFS displays a fluctuating clinical course with periods of exacerbation and improvement similar to that of several autoimmune pathologies such as multiple sclerosis. Brenu and colleagues 26 stated that CFS/ME may have a potential to be autoimmune because it shares certain parallels with a number of autoimmune diseases. The similarities include decreases in oxidative phosphorylation, reduced NK cytotoxic activity, defects in B cells, and equivocal levels of cytokines. Most autoimmune diseases demonstrate equivocal levels of immune cell numbers and/or alterations in their activation or functional capacity. The differences in cell numbers and phenotypes are related to the severity or the stage of the disease, therefore, patients in the latent phases may differ in the relative numbers of immune cells in comparison to those in the early and active stages of the disease. In CFS, a mechanism for disease presentation similar to that of known autoimmune diseases has not yet been established, so CFS may have an as yet unestablished autoimmune component or perhaps the symptoms of CFS are hallmarks of a novel autoimmune disorder yet to be identified. In accordance with this hypothesis, a recent study on 33 Norwegian CFS patients, fulfilling the Canadian and Fukuda criteria, 27 found an increased number of naive B cells and a reduced number of plasmablasts among the sample. Another evidence of an alteration of the B cell subsets is that the use of Rituximab in anti-B cell therapy reported benefits for CFS patients. 28 The prevalence of women in our CFS population is in accordance with literature data and indicative of a role of an endocrine pathway in the pathology, however, from our data, gender seems not to influence the age of onset. As a consequence, we can speculate that the observed prevalence of women in the CFS population, described in all CFS studies and confirmed in our population, may be due to an influence of the differing endocrine profiles on maintaining the imbalance of immune functions, of unknown origin, occurring in these patients.
In our sample, patients with autoimmune diseases developed CFS at a later age than patients with CFS only. This observation suggests an influence of specific therapies for autoimmune disease and is indicative of an ongoing unidentified autoimmune reactivity in CFS patients, and is in agreement with many researchers who argue that CFS could be an autoimmune disease. The prevalence of women in the CFS population is another element in favor of the autoimmune hypothesis, since women carry a well-known high-risk factor for the majority of autoimmune diseases.
In our sample, 43% of CFS patients suffer from depression. It must be noted that our CFS population was diagnosed using the exclusion criteria (CDC-1994), so patients with a diagnosis of depression before the diagnosis of CFS should not be included. No diagnosis of depression was reported for the patients’ relatives. We can argue that depression described in CFS patients must be related exclusively to a behavior impairment and not to other conditions such as a genetic predisposition.
In conclusion, even if the CFS population analyzed is numerically not very consistent, recruited in only a few regions of northern Italy, and therefore cannot be considered representative of the entire population of Italian CFS patients, interesting elements have emerged that we feel are important for future surveys on the causes of this disease. In particular, the possibility that the disease is supported by an as yet unidentified autoimmune reactivity against antigens, suggests that we must concentrate our efforts in this direction. It is hoped, therefore, that further extensive research will be organized under the patronage of the health institutions, recruiting a sufficiently larger number of Italian population with the aim of identifying putative triggers for CFS and developing intervention strategies through the application of more targeted therapies. This would lead to considerable benefits for both patients and for a reduction in healthcare costs.
Footnotes
Acknowledgements
We thank the non-profit Italian organization AMCFS (Associazione Malati di CFS) in Pavia for its precious collaboration in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.