
Abstract
Background
Non-muscle invasive bladder cancer (NMIBC) is the most prevalent type of bladder cancer, typically associated with a favorable prognosis and a risk of recurrence during the follow-up period. Inflammatory markers have been used to predict prognosis in various cancer types. The aim of this study was to explore the prognostic value of the readily accessible inflammatory markers, platelet-to-lymphocyte ratio (PLR) and interleukin-6 (IL-6), in NMIBC.
Methods
The study comprised a retrospective analysis of clinical data collected from NMIBC patients diagnosed between October 2018 and October 2020. PLR was calculated using the routine preoperative blood test results, and preoperative IL-6 levels were recorded. Receiver operating characteristic (ROC) curves were generated for PLR and IL-6 level and the optimal cut-off values were determined using Youden's index. Survival curves were generated to evaluate the association between PLR and IL-6, and recurrence-free survival (RFS), and univariate and multivariate analysis were performed using the Cox proportional hazards regression model. A nomogram and calibration curve were generated to assess the clinical significance of the model.
Results
The ROC curves demonstrated that PLR and IL-6 levels were significantly associated with tumor pathology grade, with area under the curve (AUC) values of 0.833 (95% CI 0.757, 0.910) for PLR and 0.724 (95% CI 0.622, 0.825) for IL-6 levels. PLR and IL-6 levels were also positively associated with tumor recurrence, with AUC values of 0.647 (95% CI 0.538, 0.756) and 0.846 (95% CI 0.769, 0.924), respectively. The survival curves indicated that patients with high PLR and high IL-6 levels had shorter RFS than those with low PLR and low IL-6 level (P < 0.01). Univariate Cox proportional hazards regression analysis showed that age, tumor size, tumor number, pathological grade, PLR and IL-6 were potential risk factors for NMIBC recurrence. Multivariate analysis further revealed that tumor number, smoking, PLR, and IL-6 were independent risk factors for NMIBC recurrence (P < 0.05).
Conclusions
Preoperative peripheral blood inflammatory markers (PLR and IL-6) are useful predictors of RFS in NMIBC patients at the time of initial diagnosis. High PLR and high IL-6 were identified as independent risk factors for tumor recurrence and could serve as potential biological markers for prediction of NMIBC recurrence.
Keywords
Introduction
Bladder cancer is among the most prevalent urological cancers, ranking as the eleventh most common malignancy in women and the fourth most common malignancy in men. In 2020, the incidence of bladder cancer was approximately 573,000 cases, resulting in approximately 213,000 deaths. 1 Smoking is the most common risk factor leading to the rising morbidity rates. The impact of bladder cancer on human health is gradually rising due to the increasing number of smokers. Non-muscle invasive bladder cancer (NMIBC) accounts for 75% of patients diagnosed at an early stage, and primary treatment involves transurethral resection of bladder tumors (TURBT) and routine intravesical instillation. However, recurrence and progression may be observed in approximately 50%–60% of patients during the follow-up.2,3 Thus, it is imperative to explore novel and effective approaches to predict the prognosis and to detect recurrence of bladder cancer at early stages.
Pathological grade and tumor node metastasis (TNM) staging are currently the most reliable risk factors for the prediction of prognosis. 4 However, these two indicators can only be obtained and assessed postoperatively. In 1863, Virchow discovered leukocytes in tumor tissues and proposed an association between tumors and inflammation. Subsequently, analyses of the tumor microenvironment have revealed that approximately 15% of tumors are related to infectious factors. 5 Abdel-Latif et al. 6 demonstrated that inflammatory mediators play an important role in certain types of cancer, and increased levels of these mediators are associated with tumor angiogenesis, progression, and invasion. Acute and chronic inflammatory responses can modulate the occurrence and development of tumors. Acute inflammation is a self-limiting process, which can affect the development of tumors by transition into chronic inflammation. Extensive research has been conducted on the role of chronic inflammation in cancer. 3 Balkwill and Mantovani 5 reported that the tumor microenvironment represents a state of chronic inflammation. Chronic inflammatory responses affect the release and function of neutrophils, macrophages, and monocytes, leading to damage to tissues, proteins, lipids, and DNA. 7 Peripheral blood inflammatory markers in cancer patients reflect the body's immune and inflammatory responses, potentially indicating the body's immune response to tumors. Studies have also explored the role of lymphocytes in the occurrence and progression of tumors. Tumor-infiltrating B cells recruit and retain T cells within tumors, promoting and maintaining the inhibitory T-cell response. Moreover, B cells can function as antigen-presenting cells, activating the immune system to exert anti-tumor effects. 8 Platelets also play a crucial role in tumor occurrence and progression. Various studies have shown that tumor cells can activate surrounding platelets by releasing various signaling molecules, leveraging these activated platelets to promote tumor cell proliferation, migration, and invasion. Furthermore, platelets can suppress immune cells, such as T cells, macrophages, and natural killer cells, ultimately inhibiting the immune response against tumors.9,10 Interleukin-6 (IL-6) is a cytokine produced by various cells including dendritic cells, B and T lymphocytes, endothelial cells, macrophages, keratinocytes, fibroblasts, and tumor cells. This cytokine can promote the production of IL-4, induce differentiation of activated T cells into T helper 2 cells, and promote the formation of an anti-infective environment. In addition, IL-6 can promote cell survival, proliferation, angiogenesis, invasion, and metastasis by modulating the IL-6/STAT3 signaling pathway, thereby inducing tumorigenesis. Moreover, IL-6 can also induce tumor survival by enhancing upregulation of the anti-apoptotic gene myeloid cell leukemia-1 and cyclin. IL-6 induces the production of matrix metallopeptidase 2 and matrix metallopeptidase 9, increasing the invasive and migratory potential of tumor cells.11–13 Studies have widely explored the prognosis and significance of immunological or inflammation-related biomarkers. 14
Peripheral blood tumor biomarkers are readily accessible biomarkers and their roles in cancer prevention and treatment, such as plasma metabolic fingerprinting, have been extensively explored.15,16 Researchers have explored the clinical significance of platelet-to-lymphocyte ratio (PLR) for the prediction of prognosis in bladder cancer patients, and the prognostic value of IL-6 has been evaluated in other tumors.17,18 However, no studies have explored the prognostic value of the combination of PLR and IL-6 in bladder cancer. In this study, we conducted a retrospective analysis to explore the prognostic value of the combination of PLR and IL-6 to provide a novel approach for the timely prediction of the prognosis of patients with NMIBC.
Materials and methods
Patients and methods
We conducted a retrospective analysis on NMIBC patients at the early stages of diagnosis treated at Nanjing Drum Tower Hospital Group Suqian Hospital from October 2018 to October 2020. The inclusion criteria were: (a) Patients treated with TURBT and intravesical instillation of gemcitabine but did not receive intravenous chemotherapy; (b) patients pathologically diagnosed with T1 stage bladder urothelial carcinoma; (c) the levels of PLR and IL-6 in peripheral blood were measured 2 days before surgery; and (d) patients with completely clinical data with no loss of data during follow-up. The exclusion criteria included: (a) Patients diagnosed with diabetes, severe liver or kidney dysfunction, infection, mental illness, blood or immune system diseases; (b) patients with a history of other malignant tumors; (c) patients presenting with urinary system stones; (d) patients diagnosed with other bladder malignancies, severe perioperative complications, or who receive neoadjuvant therapy; (e) patients with incomplete medical records; and (f) patients diagnosed with carcinoma in situ (CIS) or who received intravesical instillation of Bacillus Calmette-Guerin (BCG). A total of 99 subjects were included in the study. The institutional Ethics Review Committee of the hospital approved this study. All participants gave informed consent according to the committee's regulations.
Treatment
Clinical and demographic data collected from the patients included gender, age, smoking status, number and size of tumors, and pathological grade. The pathological grade was determined based on the biopsy method and classified through consensus classification by urologic pathologists, which was published by the World Health Organization in 2004. In this classification, “low-grade” denotes papillary urothelial neoplasm of low malignant potential and low-grade papillary urothelial carcinoma. All patients underwent TURBT and postoperative intravesical instillation of gemcitabine (1000 mg) within 24 h after surgery. The patients received intravesical instillation weekly for the first 8 weeks and monthly thereafter. Regular follow-up was conducted for all patients after surgery. The follow-up protocol comprised cystoscopy every 3 months for the first year, followed by biannual cystoscopy thereafter. Other auxiliary examinations included regular urinalysis, cytological analysis of urine samples, chest computed tomography (CT) and urinary system CT (CT urography (CTU)). The follow-up period for all patients was 3 years, with the endpoint defined as recurrence or the end of the follow-up period. Methods used for follow-up included communication through telephone/WeChat, outpatient visits, or home visits. Recurrence was defined as the time from the initial pathological diagnosis of bladder urothelial carcinoma to the confirmation of the first recurrent incidence.
Peripheral blood samples (3 mL) were collected from all patients 2 days before the surgery. The PLR was calculated using the platelet and lymphocyte levels measured with an automatic blood cell analyzer (Mindray Biomedical Electronics Co., Ltd, Shenzheng, Guangdong, China) while IL-6 levels were measured by FACSCalibur flow cytometer (Becton, Dickinson & Company, Franklin Lakes, NJ, USA).
Statistical analysis
Statistical analysis and plotting of graphs were conducted using SPSS Statistics 24.0 (IBM Corp., Armonk, NY, USA) and R software (Version 4.2.1). Continuous variables were presented as mean ± SD, whereas categorical variables were expressed as percentages (n (%)). Continuous variables were analyzed by Mann–Whitney U test and Student's t-test. The chi-square test was used to analyze categorical variables. The predictive significance of PLR and IL-6 for RFS was assessed by plotting ROC curves and calculating the Youden index. Optimal cut-off values were determined based on the survival curves. The subjects were grouped into high-level and low-level groups based on the cut-off values of observed variables. The association between high/low level groups and RFS was evaluated by plotting survival curves. Univariate Cox regression analysis was performed to evaluate the relationship between RFS time and the predictor variables. Variables with a significance level of P < 0.05 were used for multivariate analysis and to construct a prediction model. A nomogram and calibration curve were also plotted for the prediction model.
Results
Patient characteristics
All study subjects were followed up and any patients lost during the follow-up were excluded. The follow-up period for all subjects ranged from 3 to 36 months, with an average of 27.71 ± 10.76 months. The subjects in this study comprised 88 males and 11 females, with ages ranging from 32 to 88 years and an average age of 68.94 ± 11.64 years. The subjects were assigned into two groups based on whether the patients presented with recurrence. In this study, 51 cases of recurrence were recorded during the follow-up period. Statistically significant differences in tumor size, tumor number, pathological grade, PLR and IL-6 were observed between the recurrence group and the non-recurrence group (P < 0.05, Table 1).
Association between the clinical data and recurrence.
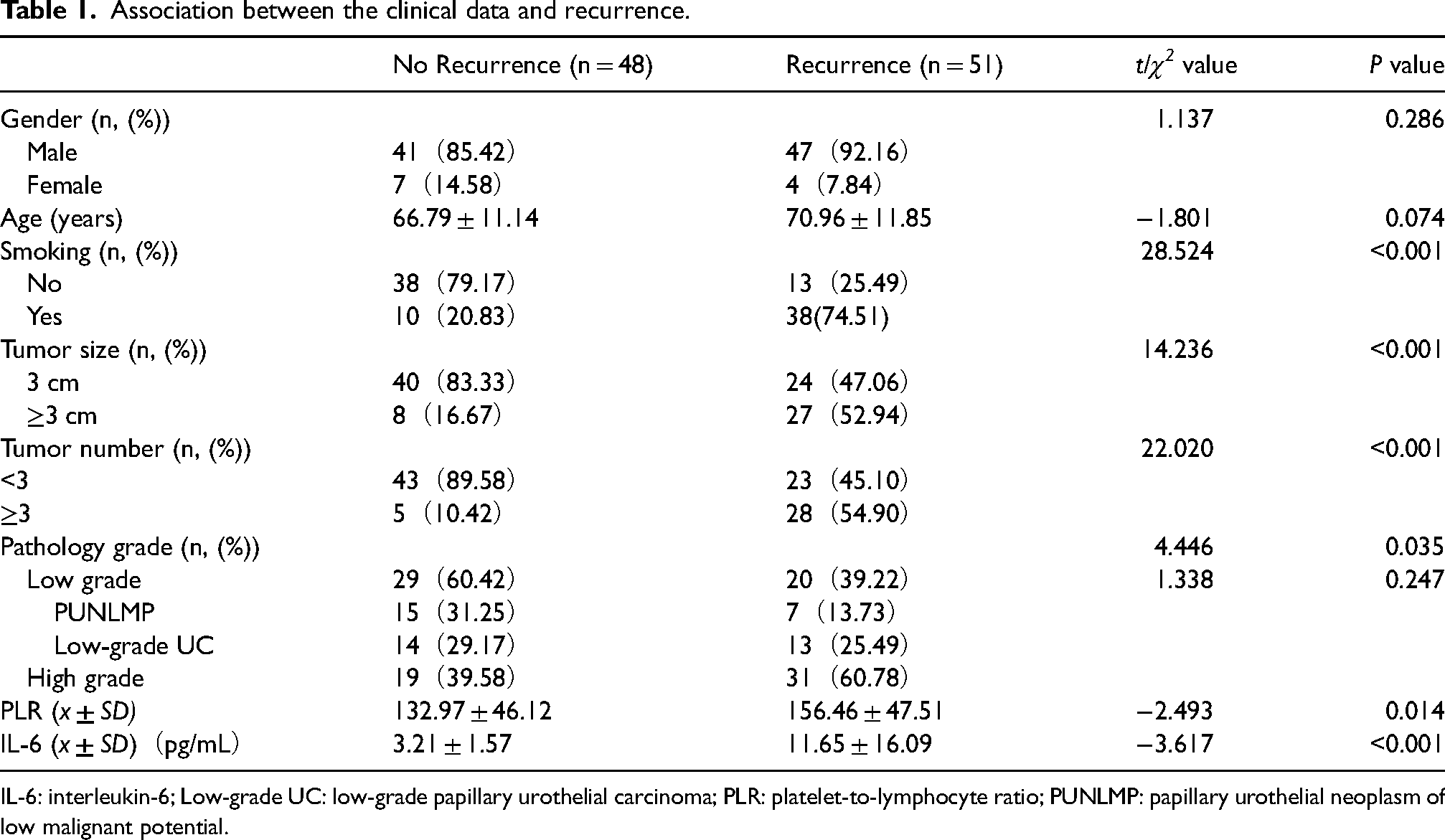
IL-6: interleukin-6; Low-grade UC: low-grade papillary urothelial carcinoma; PLR: platelet-to-lymphocyte ratio; PUNLMP: papillary urothelial neoplasm of low malignant potential.
ROC curves were plotted to explore the relationships between PLR and IL-6 level and pathological grade and recurrence. The AUC represented the reliability of the indicators in predicting high-grade pathological levels or recurrence. A larger area indicated that the variable was a potential predictor of recurrence. The AUC values were 0.833 (95% CI 0.757, 0.910) for PLR and 0.724 (95% CI 0.622, 0.825) for IL-6 level for the association between inflammatory markers and pathological grade. The AUC value for the relationship between PLR and recurrence was 0.647 (95% CI 0.538, 0.756), and the AUC value for the association between IL-6 and recurrence was 0.846 (95% CI 0.769, 0.924; Figure 1). The Youden index was calculated for the inflammation indicators based on the ROC curves, and the optimal cutoff values were obtained as follows: PLR = 157. 965, IL-6 = 4.150 pg/mL. The patients were then categorized into high-level group and low-level group based on the observed variables, and survival curves were plotted (Figure 2).
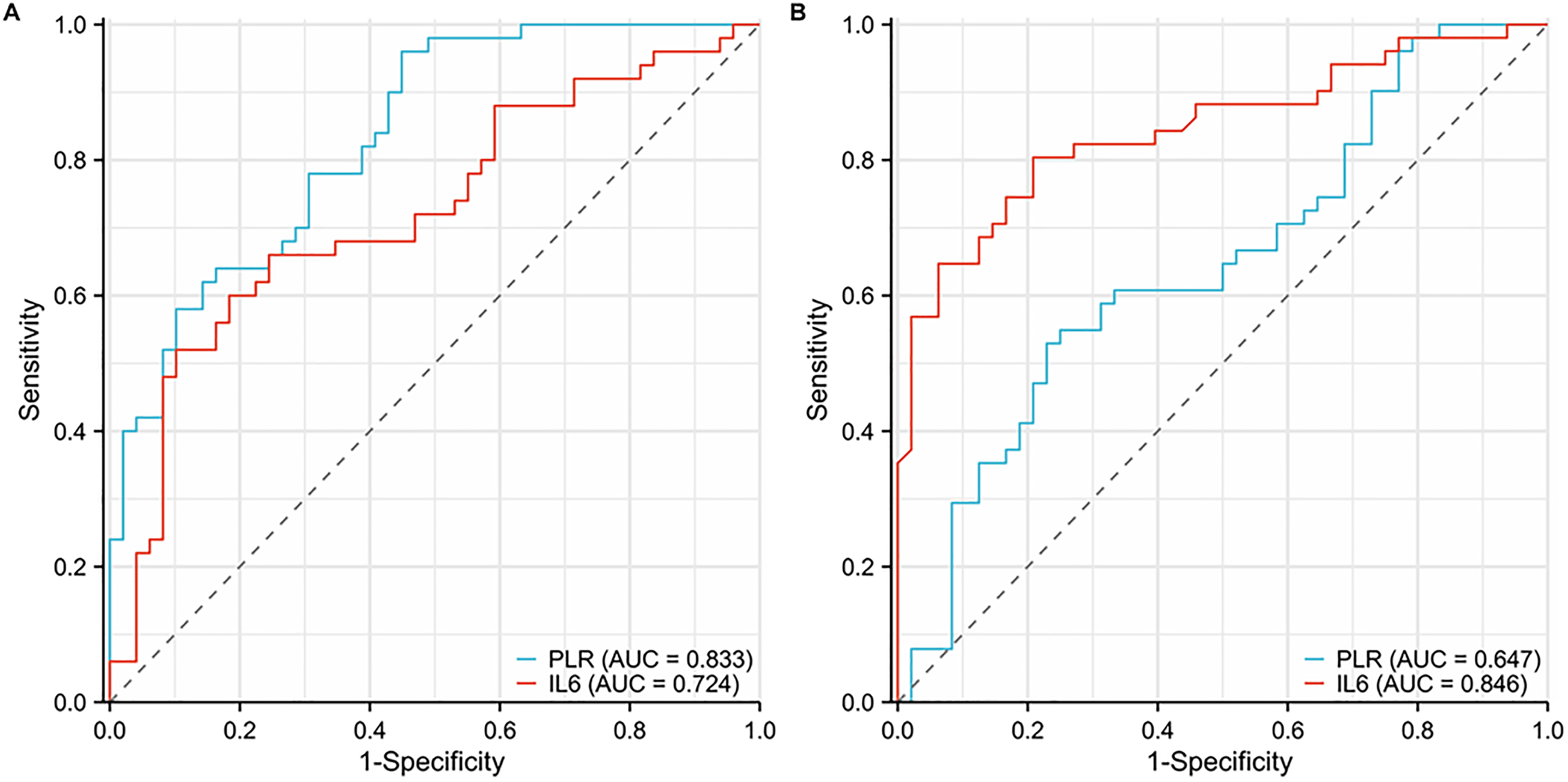
ROC curves of pathology grade and recurrence for PLR and IL-6 level. (A) ROC curves of pathology grade for PLR and IL-6. (B) ROC curves of recurrence for PLR and IL-6.
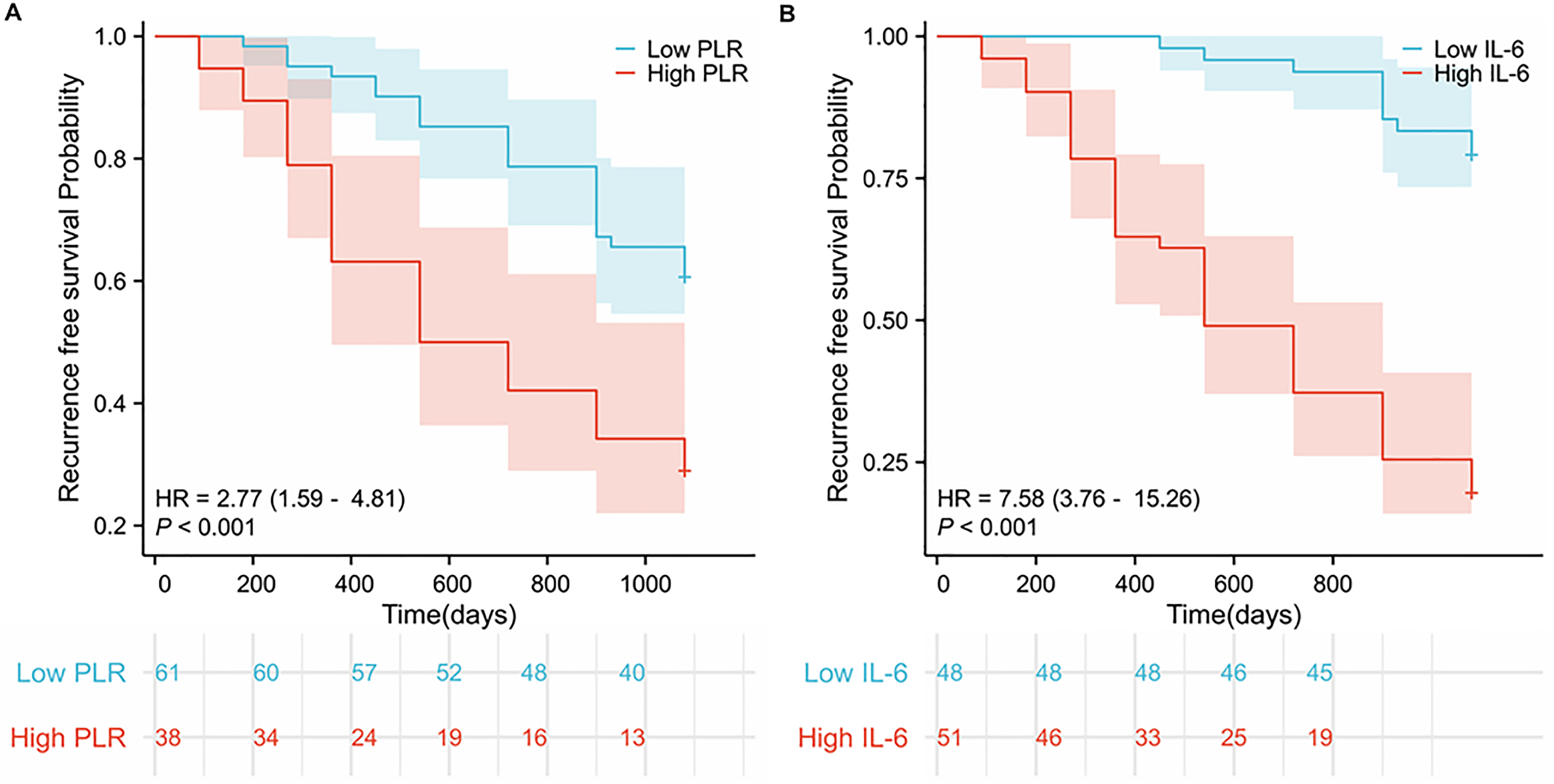
Recurrence-free survival curves of groups with low and high PLR and IL-6 levels. (A) Recurrence-free survival curves of groups with low and high PLR. (B) Recurrence-free survival curves of groups with low and high IL-6 levels.
Independent risk factors for recurrence in NMIBC patients were identified. Univariate Cox regression analysis was performed to explore the relationships between the variables and recurrence. The results showed that age (P = 0.034; 95% CI 1.002, 1.058), smoking (P < 0.001; 95% CI 2.675, 9.542), tumor size (P < 0.001; 95% CI 1.620, 4.901), tumor number (P < 0.001; 95% CI 2.318, 7.070), pathological grade (P = 0.006; 95% CI 1.248, 3.857), PLR (P = 0.001; 95% CI 1.527, 4.618) and IL-6 (P < 0.001; 95% CI 3.462, 14.019) were risk factors for recurrence in NMIBC patients. The variables with a significance level of P < 0.05 were selected for multivariate regression analysis.
A multivariable Cox proportional hazards regression model was constructed using the forward likelihood ratio method. The results showed that tumor number (P = 0.001; 95% CI 1.60, 5.757), smoking (P = 0.001; 95% CI 1.625, 6.451), PLR (P = 0.010; 95% CI 1.226, 4.417), and IL-6 (P < 0.001; 95% CI 1.226, 4.417) were independent risk factors for recurrence of NMIBC (Table 2). As for the factor of gender, the P-value of the association between gender and recurrence is 0.441; thus, we did not include the factor gender in further regression analysis.
Univariate/Multivariate Cox proportional hazards regression analysis of various variables to predict the prognosis for patients with NMIBC.
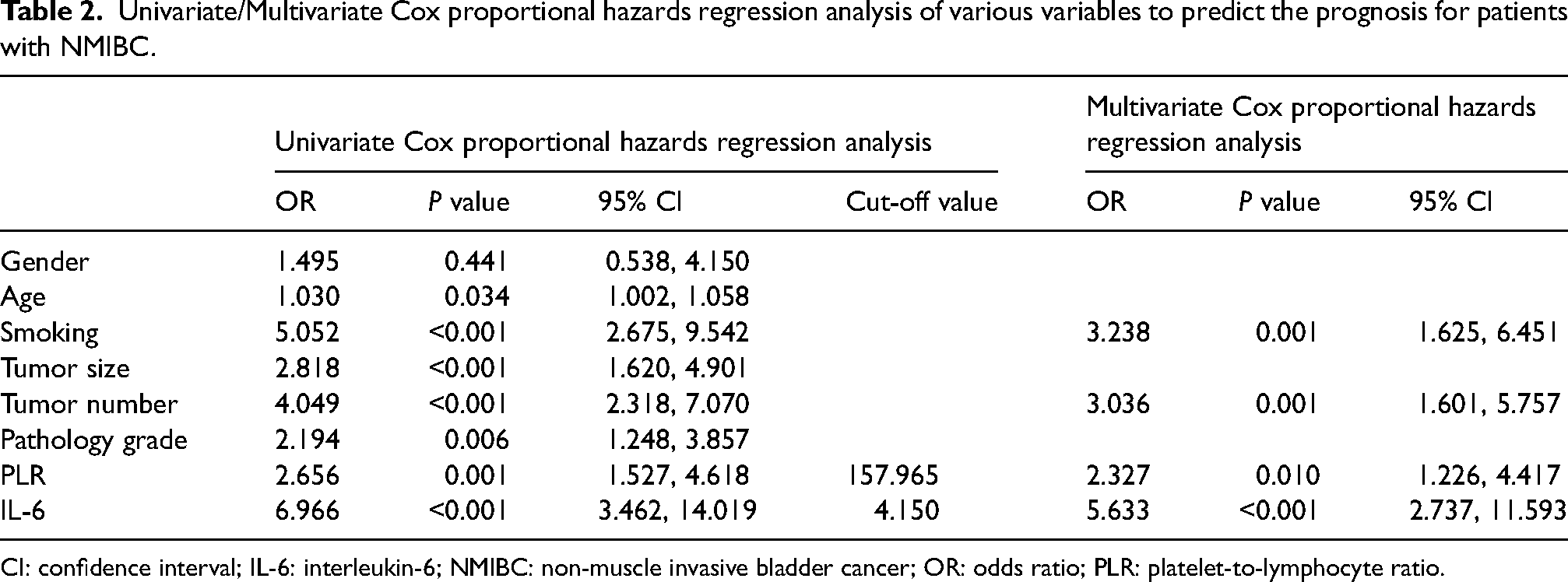
CI: confidence interval; IL-6: interleukin-6; NMIBC: non-muscle invasive bladder cancer; OR: odds ratio; PLR: platelet-to-lymphocyte ratio.
Nomogram of prognosis model and calibration curves. We constructed a prognosis model based on the variables identified as potential risk factors (P < 0.05) using univariate Cox proportional hazards regression analysis, including age, smoking, tumor size, tumor number, pathological grade, PLR, and IL-6 to ensure that no factors potentially influencing prognosis were overlooked that were listed in the literature or in clinical practice. Subsequently, we generated a nomogram based on these variables with the concordance index (C-index) of 0.87 1(95% CI 0.847, 0.895). Each independent hazard factor score corresponded to a straight line drawn upwards from that axis on the score axis. The total score represents the sum of scores for each factor. The predicted probabilities for 1 year and 2 years were directly derived from the total score axis to the 1-year and 2-year survival axis. A calibration curve was generated for the predictive model, which showed that the predictive model had good predictive accuracy for the recurrence rates at 1 year and 2 years (Figure 3).
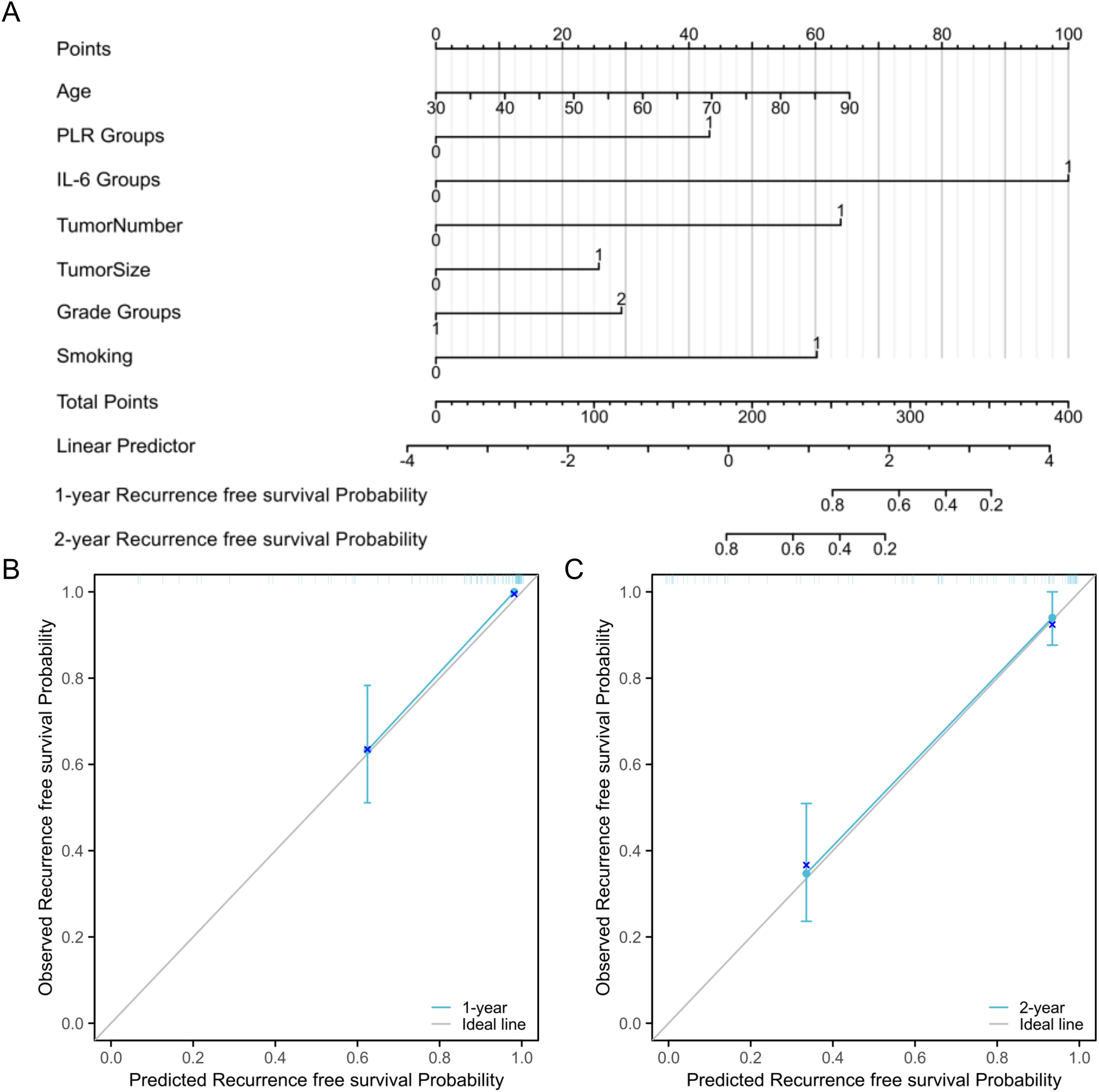
Nomogram constructed based on the variables significantly associated with recurrence and calibration curves. (A) Nomogram. (B) 1-year recurrence-free survival prediction value of the predictive model. (C) 2-year recurrence free survival prediction value of the predictive model.
Discussion
NMIBC is the most prevalent type of bladder cancer, typically associated with a favorable prognosis, and is mainly treated with TURBT combined with intravesical instillation therapy. However, studies report that some patients present with tumor recurrence and progression during long-term follow-up.1,2 Therefore, exploring the risk factors of recurrence is essential for adjusting the treatment methods for high-risk patients and timely management of the disease to improve patient prognosis. In 2021, the European Association of Urology reported the latest risk stratification method for NMIBC based on retrospective analysis of variables from multiple studies with large datasets. The classification system comprised risk factors including age, primary tumor or not, tumor size, tumor number, and the presence of carcinoma in situ. Multiple guidelines propose this risk-scoring system for the management of patients with newly diagnosed NMIBC. 19 However, most of these risk factors can only be evaluated postoperatively. It would be more persuasive for preoperative communication and surgical decision-making if there were risk factors used to assess the prognosis to a certain extent before surgery. Moreover, for patients, they also do not need to wait until the postoperative period to have a better understanding of the risk of tumor recurrence.
As readily obtained biomarkers, studies have been conducted on the prognostic value of PLR and IL-6 in various cancer types, including pancreatic cancer, 20 ovarian cancer,21,22 and thyroid cancer. 23 Hou et al. 24 reported that IL-6 levels in patients with gastric cancer were significantly elevated compared with healthy individuals. Additionally, IL-6 levels are associated with advanced tumor stages, lymph node infiltration, and distant metastasis. Qi et al. 25 conducted a meta-analysis and observed that high PLR is significantly correlated with low pathological response rate, low overall survival (OS), and disease-free survival in breast cancer patients receiving neoadjuvant chemotherapy. Gawiński et al. 26 performed a prospective analysis and reported that PLR levels are significantly associated with lymph node involvement in locally advanced rectal cancer patients. Liang et al. 18 demonstrated that the differential expression of IL-6 in gastric cancer patients has significant prognostic value through a retrospective study. Moreover, IL-6, N staging, and T staging are independent prognostic factors, and a new survival prognostic model based on these three indicators is more accurate than the traditional TNM staging system.
Chen et al. 27 conducted a study involving 208 subjects with a follow-up period of 1 year. The findings revealed that the preoperative peripheral blood PLR level was significantly associated with NMIBC grade and recurrence. Wang et al. 28 conducted a retrospective study comprising 222 patients with NMIBC treated with intravesical chemotherapy or intravesical chemohyperthermia and observed that high PLR level was significantly associated with RFS for the intravesical chemotherapy group and intravesical chemohyperthermia group. A retrospective study involving 183 NMIBC patients who received intravesical BCG demonstrated that PLR was significantly different between BCG-responders and BCG-non-responders. Moreover, the finding showed that patients with high level PLR at initial diagnosis had poor RFS. 29 The results in the present study are consistent with the previous findings. In our study, we observed a significant association between PLR and pathological grade with an AUC value of 0.833 (95% CI 0.757, 0.910). The results showed that high-level PLR was associated with poor prognosis.
In a retrospective study comprising 200 patients, Zheng et al. 13 observed that serum IL-6 levels were significantly higher in patients with high-pathological-grade bladder cancer than low-pathological-grade patients, and high levels of serum IL-6 were significantly associated with tumor recurrence. The findings in our study also showed a significant association between IL-6 levels and pathological grade, with an AUC value of 0.724 (95% CI 0.622, 0.825). Tong et al. conducted a retrospective study comprising 71 T1 stage NMIBC patients receiving gemcitabine intravesical treatment with a median followed-up period of 31 months. The results indicated that IL-6 expression and secretion levels were significantly higher in gemcitabine-resistant subtypes. Serum IL-6 levels are significantly associated with clinical and pathological characteristics such as tumor diameter, multiple lesions, concurrent CIS, and pathological grade. Previous findings indicate that patients with high serum IL-6 levels have shorter RFS after bladder gemcitabine treatment, and IL-6 is an independent prognostic factor for post-treatment recurrence in NMIBC patients. 30 In our study, high IL-6 levels were significantly associated with poor prognosis.
High PLR and IL-6 levels are associated with poor prognosis for patients with muscle invasive bladder cancer (MIBC). Warli et al. 11 conducted a prospective study of 32 bladder cancer patients and reported that the level of serum IL-6 is a potential prognostic factor for bladder cancer, and high levels of IL-6 are associated with lymph node metastasis. Kayar et al. 31 demonstrated that preoperative PLR was an independent prognostic factor for OS after radical cystectomy in non-metastatic MIBC patients after conducting a retrospective analysis of data collected from 119 subjects. A retrospective study comprising 226 MIBC patients showed that high PLR level is an independent factor for poor prognosis in patients with locally advanced or metastatic bladder cancer after chemotherapy. In addition, high PLR level was significantly associated with the pathological grade. 32 However, some studies showed contradicting results. Claps et al. 33 reported that the preoperative immune-inflammatory characteristics described by neutrophil-to-lymphocyte ratio, PLR, lymphocyte-to-monocyte ratio, systemic immune-inflammation index, and C-reactive protein were poor predictors for perioperative complications after radical cystectomy.
The findings from our study showed that age, smoking status, tumor size, tumor number, pathological grade, PLR, and IL-6 are risk factors for bladder cancer recurrence, which is consistent with previous results.27–31 We observed that tumor number, smoking, PLR, and IL-6 were independent risk factors for NMIBC recurrence. Some studies showed that smoking could induce the expression of IL-6.34,35 However, the observed P value of the correlation between smoking and IL-6 levels is 0.055, which means, according to our data, there was no significant association between smoking and IL-6 levels. A prognostic model, which included more risk factors than that in a previous study, 36 was constructed by plotting a nomogram of the risk factors based on univariate Cox regression analysis. Regarding factors with a P-value > 0.05 in further multivariate Cox regression analysis (e.g., age, tumor size, and pathology grade) we did not exclude them from this model to ensure that no factors that proved to potentially influence the prognosis in the literature or in clinical practice were overlooked. The C-index of this model was 0.871 (95% CI 0.847, 0.895), which means good predictive significance. Calibration curves were also used to evaluate the reliability of the nomogram. The calibration curves showed that the model had good predictive value for 1-year and 2-year RFS probability.
Ours was a retrospective study, so it has some limitations. The study subjects were from a single center and the sample size was small. Therefore, the findings from the study may not be generalized to other study sites. The results indicated that pathological grade was not an independent risk factor for NMIBC recurrence, contrary to findings from previous studies, which can be attributed to the small sample size. Additionally, the inflammatory markers in peripheral blood are influenced by the overall immune status, nutritional status, medication, and lifestyle; thus, the predictive value should be considered comprehensively. Some patients that were diagnosed with high pathological grade tumor did not receive intravesical BCG due to economic factors. Although this study used strict inclusion criteria, the results may still be influenced by these factors. We will conduct larger multicenter studies to address these limitations and provide more conclusive results.
Conclusion
The results showed that elevated peripheral blood levels of PLR and IL-6 are associated with tumor recurrence in NMIBC, so they can be used as prognostic predictors. Furthermore, PLR and IL-6 are independent risk factors for tumor recurrence and have important implications in the prognosis of NMIBC patients. These two markers can be used to predict the risk of tumor recurrence in this group of patients.
Footnotes
Abbreviations
Acknowledgments
Not applicable.
Author contributions
XYW and JJZ were responsible for study conception and design; JJZ provided administrative support; XYW, YMS, SQZ, and LJC collected the clinical data and conducted the follow-up; XYW, YMS, and SQZ collected and assembled the data; and YMS and LJC performed data analysis and interpretation. All authors read and approved the final manuscript. XYW and JJZ confirm the authenticity of all the data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The whole procedures in the study involving biological samples or medical record information and data were approved by the Ethics Committee of Nanjing Drum Tower Hospital Group Suqian Hospital. Written informed consent was obtained from all adult participants or the parents and guardians of younger participants included in the study. All methods were performed in accordance with the relevant guidelines and regulations (Declaration of Helsinki).
Funding
This work was supported by Suqian Talent Work Leading Group (Grant Number 20220049).