
Abstract
Objective:
To determine whether flexible ureteroscopies (f-URS) affect renal function by performing dynamic renal scans (DTPA or MAG3) pre- and post-operatively.
Patients and methods:
Between April 2010 and March 2024, 945 renal units underwent ureterorenoscopy, of which 101 renal units with upper urinary tract stones (UUTS) completed a renal scan, either DTPA or MAG3 pre- and post-f-URS. The cases were divided into three groups: worsened (>10%), improved (>10%), or unaffected (stable) renal function (⩽10% change). Patient demographics, imaging data, stone properties, and treatment outcomes were comprehensively evaluated. The evaluation of postoperative complications was performed using the Clavien-Dindo classification.
Results:
The mean patient age was 53.4 years. The mean stone size was 11.4 mm. Renal pelvis, upper, and middle calyces, and lower pole stones were found in 12.9% (13), 28.7% (29), and 34.7% (35) of cases, respectively. Single- and second-session SFRs were 95% and 99%, respectively. A third auxiliary procedure was needed in one renal unit (1%). The mean number of procedures per renal unit was 1.06 (107/101). The mean renal function pre and post-operatively was 47.3% and 48%, respectively. The majority of patients (94.1%) had unchanged renal function. However, three female patients (3%) had a decline in differential renal function (>10%) while three patients (two males and one female) (3%) had an improvement (>10%). A re-intervention was necessary in one patient, interestingly not among those with declined renal function.
Conclusions:
Flexible ureteroscopy due to renal or ureteral stones has minimal to no impact on renal function. Renal scans pre- and post-operatively may be used in potentially high-risk patients.
Introduction
As known, nephrolithiasis is a common disease in Asia with a rate of 1%–5%. 1
With the development of small flexible ureteroscopes (f-URS) and the improvement of laser lithotripsy, ureteroscopy has become the standard of care for treating urolithiasis less than 2 cm.2,3 F-URS is also a competent modality of treatment for renal stones larger than 2.5 cm, even though the stone-free rate (SFR) is higher in percutaneous nephrolithotomy-PCNL. 4
Piao et al. 5 and Hoarau et al. 6 showed that retrograde intrarenal surgery (RIRS) didn’t improve renal function in all patients. Both investigations’ shortcoming was the use of the estimated glomerular filtration rate, or eGFR, to assess renal function and the consequent inability to demonstrate the differential function of each kidney or renal unit independently.
We believe that utilizing renal scans both before and after the procedure could provide a superior indication of each unit’s function as well as potential obstruction that needs to be addressed.
In theory, different procedures like percutaneous nephrolithotomy (PCNL) or RIRS may affect renal function. 5 Therefore, to determine whether every operated renal unit has improved, deteriorated, or remained unchanged, the delta of renal scans pre- and postoperatively were examined. As stated in Asali and Hallak, 7 we can also identify renal obstruction due to ureteral stricture and treat it as soon as possible. The incidence rate of postoperative ureteral stricture varies from 0.23% to 2.97%.8–12 Subsequent treatment of the stricture should be tailored according to the stricture length and severity of hydronephrosis. During f-URS, there is high intrarenal pressure that threatens tubular function, which could be another cause of renal deterioration. In our practice, we suggest renal scans for every patient undergoing flexible ureteroscopy (f-URS), however, not everyone undergoes the test for different reasons.
Patients and methods
One surgeon performed ureterorenoscopies on 945 patients between April 2010 and March 2024, of which 101 renal units with upper urinary tract stones (UUTS) completed renal scans (either diethylenetriaminepentaacetic acid (DTPA) or mercapto acetyl tri glycine (MAG3)) pre- and post-f-URS.
At the medical center where the surgeries were performed, a renal scan is routinely recommended for all patients undergoing ureteroscopy or RIRS, due to concerns about the potential development of strictures or future legal claims related to postoperative renal dysfunction.
All patients undergo a urine culture test prior to surgery. Those with a positive culture do not proceed to surgery at this center.
The differential renal function was compared pre- and post-f-URS. The cases were divided into three groups: decreased by more than 10%, improved by more than 10%, or stable renal function (⩽ 10% change).
A 7.5 Fr flexible ureteroscope was utilized with Holmium: YAG (yttrium aluminum garnet) laser lithotripsy in all patients. The laser fibers used were 200, 230, and 272 µ, with a mean energy of 0.5 J and a mean frequency of 25.3 Hz. The calculi fragments were taken out with a basket. The ureteral access sheath (UAS) was always placed in the lower ureter below the ureteral stone and moved up to the middle or proximal ureter for renal stone treatment. Inflow pressure of 300 mmHg was used in all patients.
All the patients were included in the study after meeting our inclusion and exclusion criteria:
The inclusion criteria were as follows: UUTS, the use of the same 7.5 Fr flexible ureteroscope (flexible uretero-renoscope FLEX- X2s [Karl Storz & Co. KG, Tuttlingen, Germany]), utilizing a Holmium: YAG laser with consistent energy, frequency, and fibers (200, 230, and 272 µ), the use of Sphinx JR 30 W [LISA Laser Products GmbH, Germany], Mega Plus 15 W [Richard Wolf GmbH, Knittlingen, Germay], or Luminis 120 W [Luminis, Yokneam, Israel] laser generator. the use of a UAS (Flexor ureteral access sheath 12/14 Fr, 28, 35, and 45 cm; FUS- Cook Medical, Bloomington, IN, USA), adults aged 18 years and older.
* A dynamic renal scan, either DTPA or MAG3, was done preoperatively.
* A dynamic renal scan, either DTPA or MAG3, was done postoperatively.
The exclusion criteria were as follows:
Using other flexible ureteroscopes.
Incomplete data.
No other access sheath type use.
Using a rigid ureteroscope.
Single kidney.
At the end of the operation, a triple test was done for all calyces, using a plain abdominal radiograph of the kidneys, ureters, and bladder, using the scope and the c-arm while injecting contrast intraoperatively as a retrograde pyelography and screening every calyx using the endoscope and simultaneously following the anatomy on the C-arm screen as described in Asali. 13
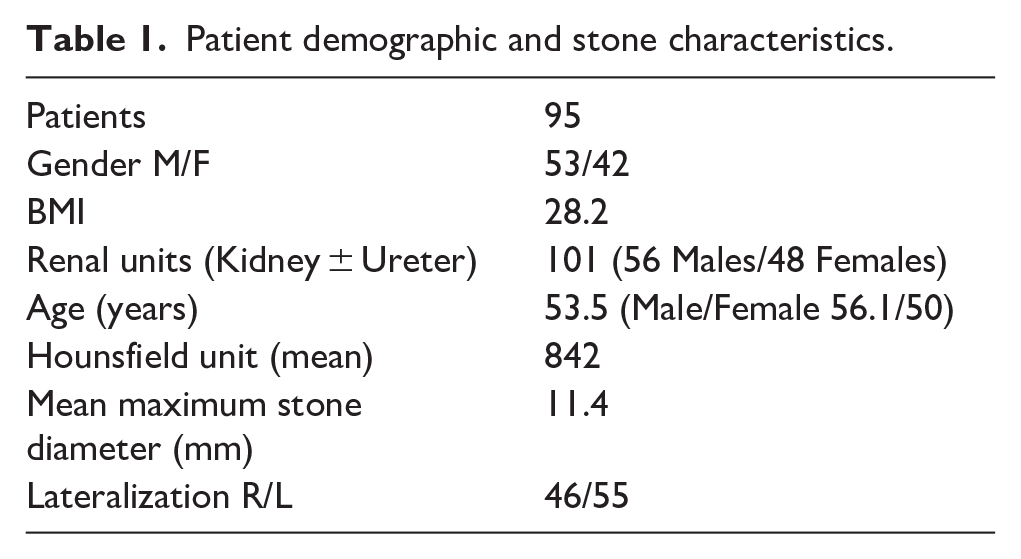
In all the patients, the following characteristics were examined: gender, BMI, age, Hounsfield unit, stone diameter, laterality (Table 1), renal/ureteral stones (Table 2), stone-free rate (Table 3), auxiliary procedures per renal unit (Table 3), double-J stent insertion, pre- and post-f-URS renal function (Table 4), and perioperative complications (Table 5). Stone-free status was defined as complete stone removal.
Patient demographic and stone characteristics.
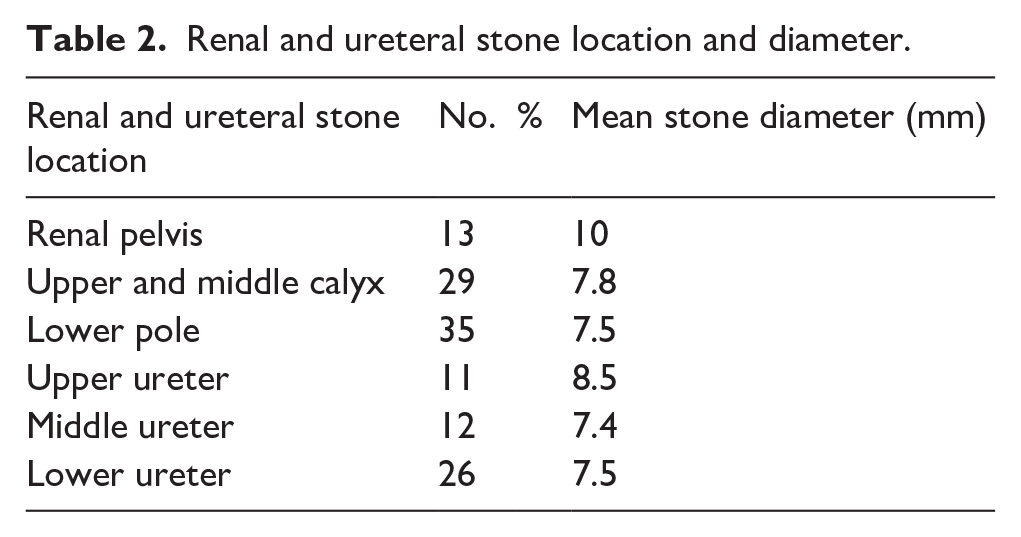
Renal and ureteral stone location and diameter.
Stone-free rate/auxiliary f-URS.
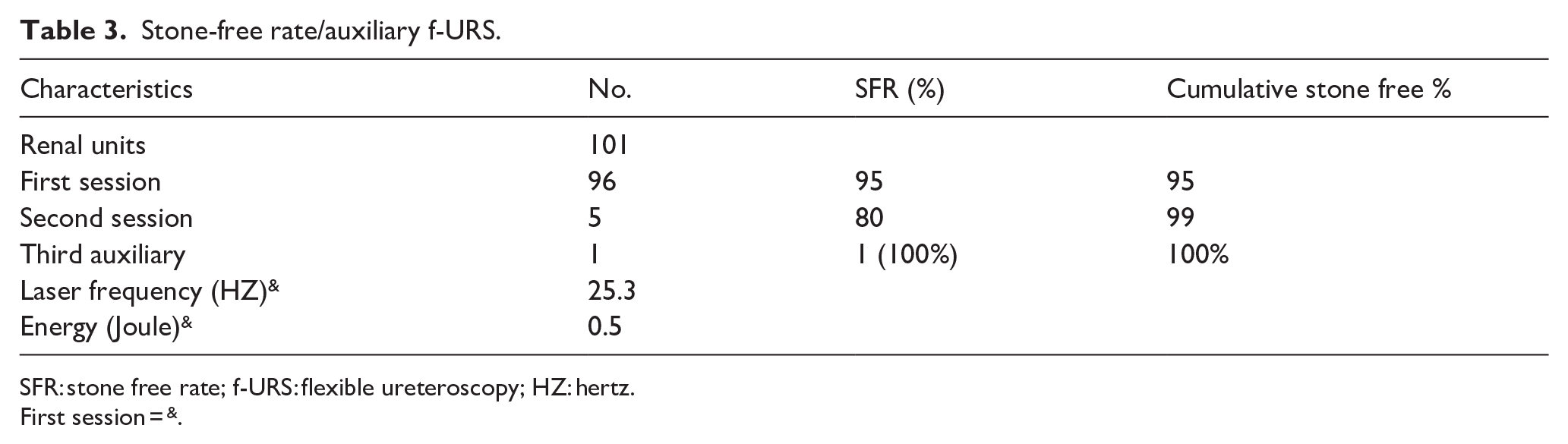
SFR: stone free rate; f-URS: flexible ureteroscopy; HZ: hertz.
First session = &.
Renal scan DTPA results and analysis.
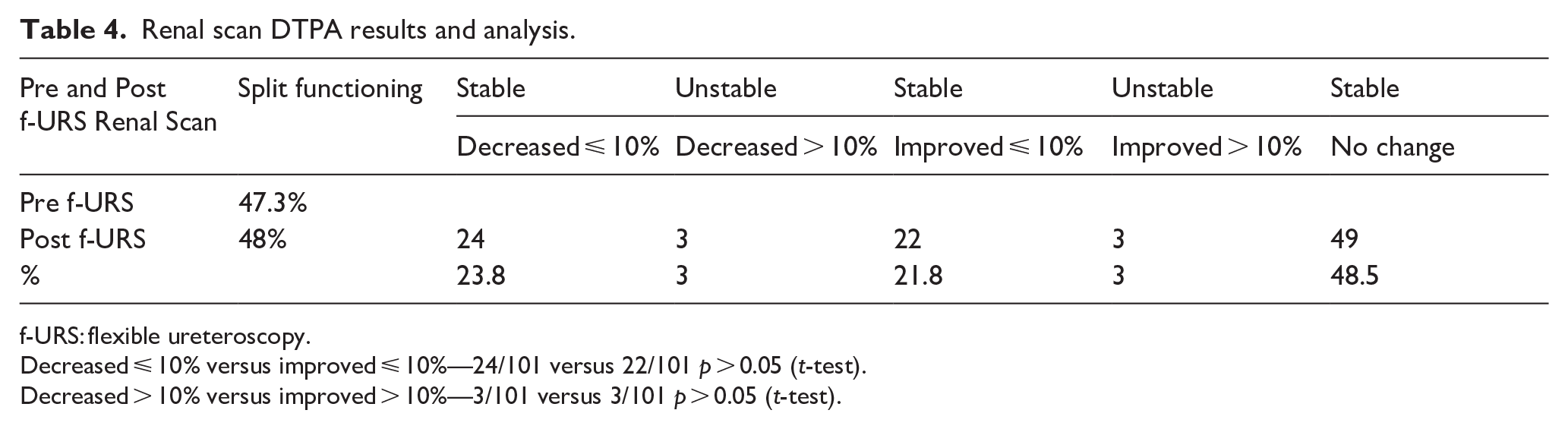
f-URS: flexible ureteroscopy.
Decreased ⩽ 10% versus improved ⩽ 10%—24/101 versus 22/101 p > 0.05 (t-test).
Decreased > 10% versus improved > 10%—3/101 versus 3/101 p > 0.05 (t-test).
Complications.
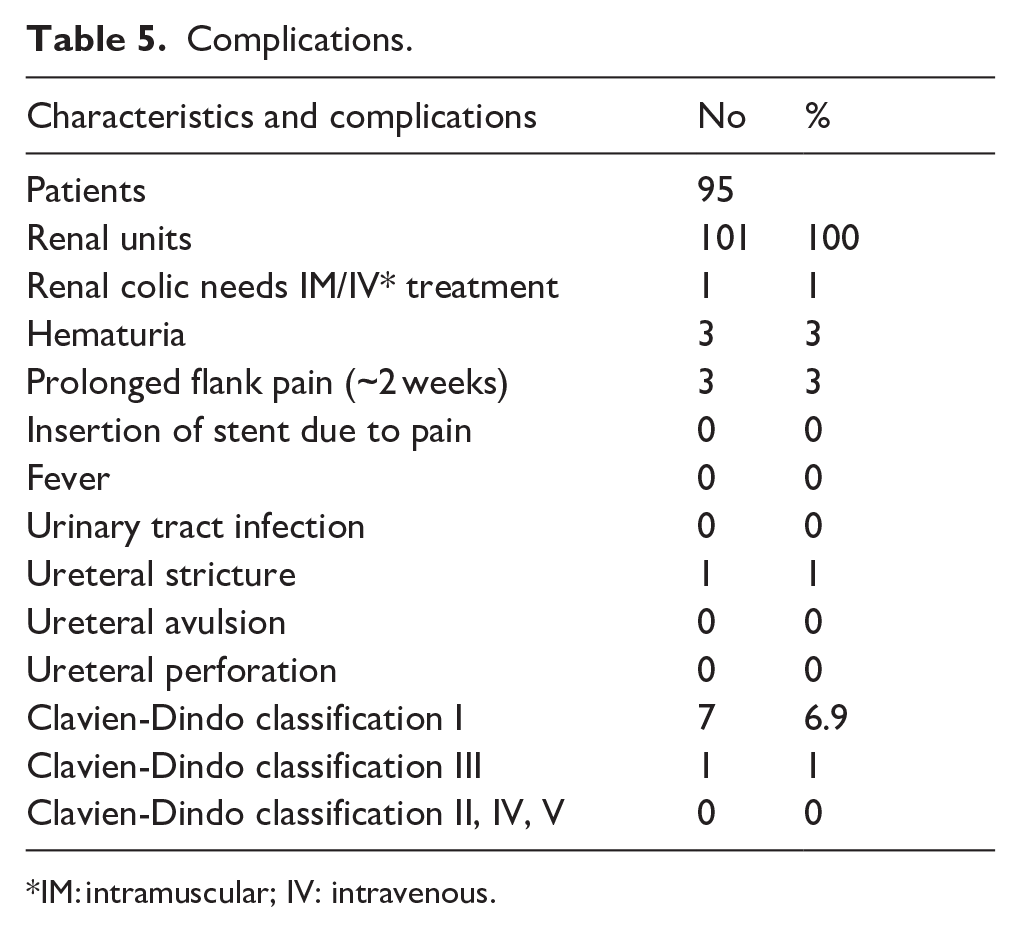
IM: intramuscular; IV: intravenous.
This study was retrospective, and all the data (demographic data, stone characteristics, operative, and postoperative data) were recorded prospectively.
This study was retrospective, with all the data recorded prospectively. Informed consent for all patients was collected according to the Good Clinical Practice Guidelines in conjunction with local ethics board approval.
Postoperative follow-up was scheduled 1 month later with a dynamic renal scan DTPA/ MAG3, urine culture, and renal function.
Patients with residual stones were scheduled for a second f-URS/ RIRS (retrograde intrarenal surgery), and patients with obstruction were scheduled for re-intervention.
The Clavien–Dindo classification was used to report complications. 14
Results
In this cohort, a total of 95 patients were included, comprising 53 males and 42 females. Interestingly, the number of renal units treated was 101, indicating that some patients had bilateral involvement or multiple stones requiring treatment. The distribution of renal units was relatively balanced between genders, with 56 units in males and 45 units in females.
The mean age of the overall cohort was 53.5 years, but there was a notable age difference between genders: males had a higher mean age of 56.1 years compared to 50.0 years in females. This could suggest that males tend to present with symptomatic stone disease requiring intervention at an older age compared to females.
Overall, the relatively even distribution between male and female patients and renal units, along with the modest age difference, provides a balanced demographic background for interpreting the outcomes of the study.
The mean stone size was 11.4 mm.
Renal pelvis, upper and middle calyces, and lower pole stones were found in 12.9% (13), 28.7% (29), and 34.7% (35) of cases, respectively. The single- and second-session SFRs were 95% and 99%, respectively.
A third auxiliary procedure was needed in one renal unit (1%). The mean number of procedures per renal unit was 1.06 (107/101).
Ureteral double-J stents were inserted in 58.4% (59) of the cases. In 6 (5.9%) cases, a stent was placed preoperatively.
The mean differential function of operated renal units pre- and post-operatively was 47.3% and 48%, respectively. Deterioration in differential renal function of >10% was observed in three (female) patients (3%), while an improvement of >10% was similarly observed in three (two males and one female) patients (3%). The remaining 95 renal units (94.1%) demonstrated stable differential function (⩽10% change; Table 4).
Post-operative complications were mainly minor, with readmission and pain control needed in only one patient (1%), while three patients (3%) had intermittent hematuria secondary to the stent. No avulsion or perforation of the ureters was observed.
One patient (1%) who had previously undergone a radical prostatectomy developed a ureteral stricture that required reintervention and laser endoureterotomy (Table 5). Interestingly, this patient was one of the 95 (94.1%) who demonstrated stable differential renal function (⩽10% change).
As to the Clavien-Dindo classification, seven patients (6.9%) (7/101) had grade I surgical complications, whereas one patient (1%) had grade III surgical complications. No grades II, IV, or V were noted.
The mean stone diameter was 10, 7.8, 7.5, 8.5, and 7.4 mm, and 7.5 mm of the renal pelvis, upper and middle calyces, lower pole, upper ureter, middle ureter, and lower ureter, respectively. The renal and ureteral stone characteristics are shown in Table 2.
The mean hospital stay was 1 day.
Discussion
RIRS is a well-established procedure that is constantly improving with advances in technique and technology. It has gained worldwide popularity due to its minimal invasiveness, safety, and satisfactory outcomes. 15 f-URS has become the standard of care for treating urolithiasis less than 2 cm.2,3 F-URS is also a competent modality of treatment for renal stones larger than 2.5 cm, even though the SFR is higher in PCNL. 4
Comparing renal scans pre- and post- f-URS could reveal differential renal function and obstruction due to stricture or edema.
Asali and Hallak 7 concluded that post- f-URS ureteral stricture incidence is low. Gadelmoula et al. 16 showed that impacted stones are the most common cause of URS complications and stricture formation. In this study, we showed that renal unit function remains mostly stable post- f-URS, Jung et al. also showed that RIRS and Mini-PCNL had similar effects and favorable outcomes on renal function for 1-year follow-up period. They monitored their patients with 99mTc-DTPA preoperatively and postoperatively. 17
Even if our standard approach involves the use of UAS and small-diameter flexible ureteroscopes, the concern is how to diagnose an obstruction secondary to strictures or deterioration of renal functioning because of the operation early and as feasibly as possible. In our hospital, we advocate renal scan in every patient with renal colic and renal scan post ureteroscopy as a standard, but not all patients have the time or the chance to do the scans; many patients do the test after surgery, and only some perform the test before.
Early diagnosis and treatment of renal function deterioration is the cornerstone of management. Patients with high-risk indicators for the development of stenosis, such as impacted stones, should undergo postoperative imaging, according to May et al. 18 Piao et al. reported their results and used 99mTc-DTPA to check the relative renal function post minimal invasive renal surgery, but the purpose was not to diagnose ureteral stricture. 5 Out of all the patients, only six showed a significant (>10%) change in their differential renal function, of which three saw a decline in their function. It’s interesting to note that this group did not include the solidary patient who required laser endoureterotomy due to a ureteral stricture.
Interestingly, all cases of significant deterioration in differential renal function (>10% decline) were observed exclusively in female patients. Although the overall number was small (three patients, 3%), this gender-specific finding may suggest a potential, albeit subtle, gender-related vulnerability to postoperative functional decline. However, given the limited sample size, no definitive conclusions can be drawn, and this observation warrants further investigation in larger cohorts.
The advantages of this study include: outcomes may be more easily compared because all surgeries were carried out by the same surgeon using the same equipment, personnel, ureteroscope, and holmium laser energy with the UAS used from the same company. The disadvantages include being a retrospective design and the untested duration of the surgery, which may be a risk factor for stricture formation.
We showed that f-URS was successful in 95% (96/101) of cases in the first session, and cumulative SFR in a two-stage procedure was 99% (100/101). A third auxiliary procedure was done successfully in one patient.
An in-depth discussion regarding the development of ureteral strictures following ureterointestinal anastomosis after radical cystectomy is presented. However, it is challenging to directly extrapolate these findings and the underlying theories to the development of ureteral strictures following flexible ureteroscopy (F-URS). 19
It is indeed essential to select the appropriate treatment for the right patient, which is why a Micali’s nomogram was developed to assist in choosing the optimal surgical approach for stones measuring 1–2 cm. Nevertheless, flexible ureteroscopy (f-URS) remains the most widely used treatment among all available options today. 20
Resorlu-Unsal Stone Score (RUSS) was externally validated as a reliable predictor of stone-free rates after RIRS. In 79 patients, RUSS was the only independent factor associated with postoperative success. It is a simple and effective tool for preoperative evaluation. 21
Mantica et al. in their letter to editor asserted that RIRS continues to be the gold standard for minimally invasive treatment in endourology, with anticipated expansion in its application and indications in the forthcoming years. Nonetheless, we have not yet attained a point at which PCNL can be completely supplanted. Ongoing investment in training and simulation is crucial to guarantee the safe and effective execution of PCNL for patients who are unsuitable candidates for RIRS. 22
In this study, the f-URS procedure was performed using Dr. Asali’s 13 technique without the use of a guidewire, employing a flexible ureteroscope. This contrasts with another study, which reported successful outcomes but utilized a semi-rigid ureteroscope with a guiding wire. 23
We couldn’t conclude that renal scans should be done before and after f-URS, and we couldn’t prove that this surgery improves renal function or, on the contrary, causes kidney damage in the short term. However, the medicolegal value of this study should be considered.
Lawsuits against urologists are most common in endourology and urological oncology. The majority of endourological procedure malpractice lawsuits are the consequence of urolithiasis and purported technical faults. 24 Defensive medicine, which is the act of supplementing, replacing, or reducing care through assurance and avoidance behavior, is now widely practiced as a result. 25
In our study, we demonstrated that only 4% of our patients experienced a significant decline in differential renal function. As a result, dynamic renal scans could be a form of defensive medicine; however, their medicolegal value could prove to be consequential.
Conclusions
Flexible ureteroscopy due to renal or ureteral stones has a minimal impact on renal function. There was no significant change in renal function, neither for the worse nor for the better in the short term. Renal scans pre and post-operatively may be used in selected high-risk patients.
Footnotes
Author credit statement
M.A: Conceptualization, visualization, investigation, supervision, original draft preparation, data curation, methodology. O.H: Data, English editing, original draft preparation. G.A: Data, English editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study were performed after receiving informed consent from all the patients.