
Abstract
Background:
Surgical treatment of small renal tumours remain gold-standard for individuals who are suitable candidates. Over the last decade, minimally invasive surgery has provided significant advancements within the field of urological surgery. However, there is still a debate on which surgical modality is superior. This study aims to review the current literature on perioperative outcomes between laparoscopic (LPN), open (OPN) and robotic-assisted partial nephrectomy (RPN) using the standardised system, Clavien-Dindo Classification (CDC).
Methods:
A literature search was performed on Cochrane, Embase and PubMed databases. Articles between January 2016 and December 2021 were included. Perioperative outcomes investigated include estimated blood loss (EBL), operating time (OT), conversion rate (CR), warm ischaemia time (WIT), positive surgical margin (PSM) and postoperative complications using CDC. Relevant pieces of literatures were analysed and data were extracted.
Results:
This study included 12 studies, with a total of 3908 patients. (LPN = 1120, OPN = 1206 and RPN = 1580). LPN demonstrated a lower overall EBL (p = 0.004). There was no significant difference between OT (p = 0.291), CR (p = 0.200), WIT (p = 0.760), PSM (p = 0.549), CDC I (p = 0.556), CDC II (p = 0.779) and CDC⩾III (p = 0.663) of the three surgical approaches.
Conclusion:
Compared with OPN and RPN, LPN demonstrated a lower EBL. All other perioperative outcomes demonstrated similar results between the three treatment modalities. Future large-scale, prospective, randomised studies is necessary to draw a definitive conclusion from this analysis.
Introduction
Surgical treatment for small renal mass remains the gold-standard curative treatment for individuals who are suitable candidates. With the difficulties in distinguishing its pathological status from radiological imaging, and only 20% of all small renal tumours being accounted as benign (e.g. angiomyolipoma and oncocytoma), it is assumed that all are renal cell carcinoma (RCC). 1 In the past, these patients would undergo traditional open surgery or radical nephrectomy (RN). However, several studies in the 1980s have suggested comparable results in patients undergoing partial nephrectomy (PN).2,3 Thus, PN has now become the standard surgery performed in patients with small renal tumours. According to the European Association of Urology (EAU) guideline in 2023, PN is the treatment of choice in cT1 (⩽7 cm) renal tumour, and in some cases of cT2 disease if technically feasible. 4
Urological surgery has seen drastic development over the last decade, with a significant shift towards minimally invasive surgery (MIS), replacing the traditional open approach. Urologists were one of the early adopters of MIS, with the first laparoscopic urological procedure described in 1976. 5 The evolution of MIS has led to the use of a robotic-assisted approach, with the first robotic partial nephrectomy described in 2004. 6 Currently, laparoscopic partial nephrectomy (LPN), robotic partial nephrectomy (RPN) and open partial nephrectomy (OPN) are all feasible options when performing PN. Minimally invasive approaches have demonstrated lower morbidity and faster recovery rates while producing similar oncological results. 7 However, the use of MIS is not without its trade-offs. They have been associated with significant economic implications and physical restraints. 8 In 2020, it was recorded that 1.25 million operations were performed using Da Vinci surgical system alone, with the vast majority being in the urological practice. 9 However, there is still significant controversies on the outcomes between the different surgical modalities. 10
A study by Flegar et al. 11 reported that robotic surgery has become the standard approach when performing NSS in the United States, accounting for 54.5% of cases, compared to laparoscopic (9.8%) and open (43.1%) in 2014. Contrastingly in the same year, open NSS was still the standard approach in Germany, accounting for 70.8% of cases compared to LPN (23.3%) and RPN (8.6%). A retrospective study by Asker et al. 12 at a single institution concluded similar surgical outcomes between the three surgical modalities (open, laparoscopic and robotic-assisted). However, open surgery was associated with higher blood loss, longer operating time and hospital stay compared to MIS. Despite the growing surge in performing MIS, there is still no robust evidence demonstrating which approach is superior to the other.
A systematic review and meta-analysis performed by Zhang et al. 13 reported no significant difference in perioperative outcomes when comparing LPN to RPN. However, Tsai et al. 14 found that RPN was associated with lower morbidities, including lower blood loss, transfusion rate, postoperative complications and shorter hospital stay when compared to the traditional open approach. 14 A more recent study by You et al. 15 reported comparable results when looking at the surgical, oncological and postoperative outcomes of open and laparoscopic approaches in partial nephrectomy.
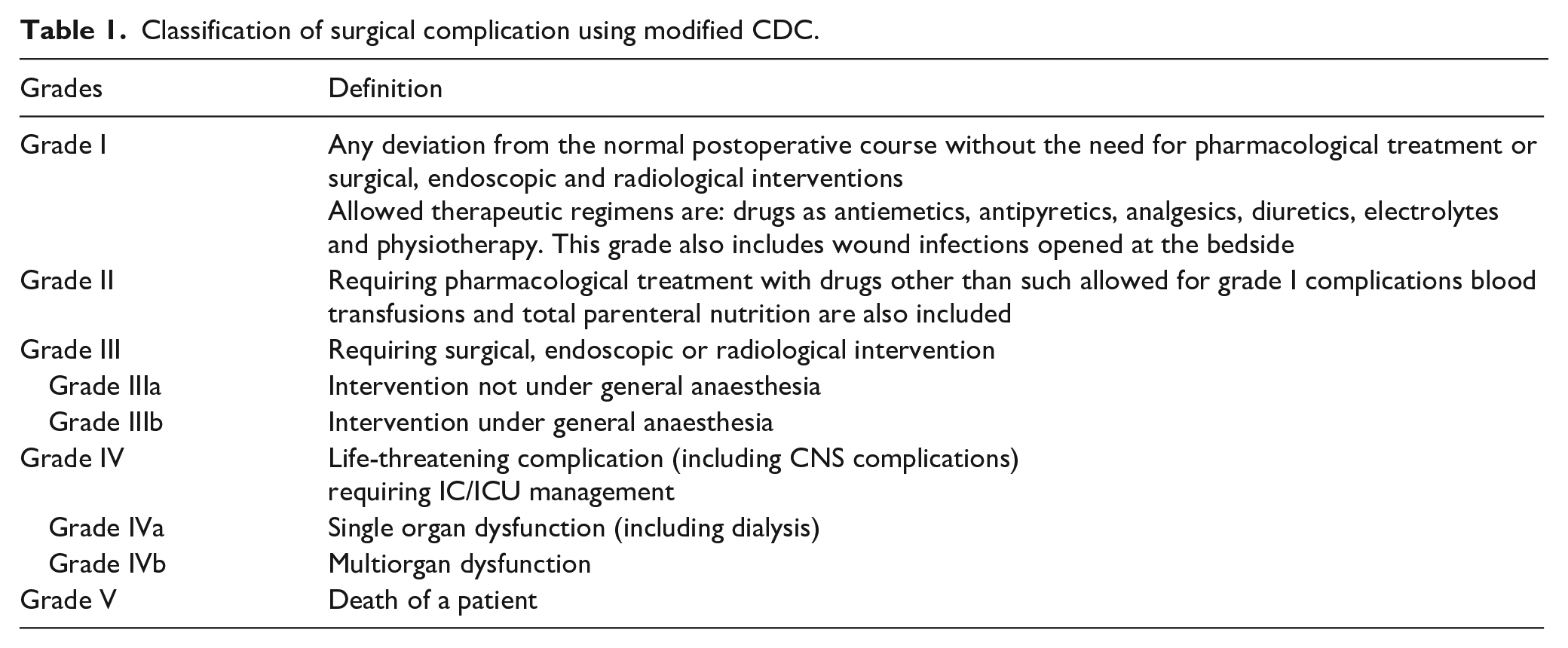
Perioperative outcomes of surgical procedures are fundamental to improving the quality and safety of patient care. They are largely influenced by patient factors (including co-morbidities), tumour factors (including size and location) and surgical system factors (including surgeon and hospital). Using a standardised system to report this information ensures consistency, and allows surgeons to gauge a clear interpretation of the outcome when comparing different surgical modalities across institutions worldwide. Clavien et al. 16 proposed a classification namely T92, to grade postoperative surgical complications. Following a large-scale research conducted in 2004, the modified Clavien-Dindo Classification (CDC) was introduced. It is now widely used in literature to report postoperative surgical complications. 17 The CDC is classified from Grade I to V, which is presented in Table 1.
Classification of surgical complication using modified CDC.
Overall, there has been a significant growth in literature which use CDC to report surgical complications. The CDC has also been incorporated into a standardised system developed by EAU in 2012 to evaluate the overall PN outcomes, called Margin, Ischaemia and Complications (MIC) binary system. 18 According to the system, the goal of PN is reached when: (1) surgical margins are negative; (2) warm ischaemia time (WIT) <20 min and (3)] no major complications, classified by CDC⩾3. The MIC was developed to further improve the current methods of comparing overall results between surgical approaches and centres. Interestingly, a paper by Mitropoulos et al. 19 noted that the CDC was not properly used in 72 (35.3%) of all papers reviewed. Despite the current standardised system available, there is still no consensus about reporting complications within urological surgery.
To date, there is still a lack of evidence demonstrating which of the three surgical modalities is superior when performing PN. The primary aim of this review is to evaluate the postoperative surgical complications associated with LPN, OPN and RPN for patients with small renal tumours using the validated standardised system, CDC. The secondary aim is to evaluate perioperative outcomes associated with PN when performed via laparoscopically, open and robotic-assisted approach. This aggregate information will benefit urological surgeons when counselling patients who require NSS, and improve future research in this area
Methods
A literature search was performed in February 2022 using the search strategy (see section 2.4) on the three databases: Cochrane, Embase and PubMed. The defined search period was between January 1st 2016 and December 31st 2021. Search terms combined ‘kidney’ OR ‘renal’, ‘tumour’ OR ‘cancer’ OR ‘carcinoma’ OR ‘neoplasm’, ‘partial nephrectomy’, in conjunction with ‘laparoscopic’ OR ‘open’ OR ‘robot’ OR ‘computer-assisted’ and ‘clavien’ OR ‘dindo’ OR ‘Clavien Dindo’. The search was limited to primary studies published in English language, where there was extractable data on laparoscopic, open or robotic partial nephrectomy. Studies that included patients with bilateral or metastatic disease, or where the Clavien-Dindo system was not utilised was excluded from the review. Data from the literatures were extracted, analysed and reviewed.
Evidence synthesis
A total of 12 studies were included in the review, with a total of 3906 patients (LPN = 1120 patients, OPN = 1206 patients and RPN = 1580 patients). All data extracted are shown in Table 2. Three studies recruited patients from Italy and USA. Other studies recruited patients from Finland, Japan, India and Australia. Two studies were multicentre; one recruited patients from Belgium, Egypt, Korea, Portugal, Spain, Italy and USA, while the other study recruited patients from Prague and France. Studies included data ranging from 2005 to 2019.
Classification of surgical complication using modified CDC.
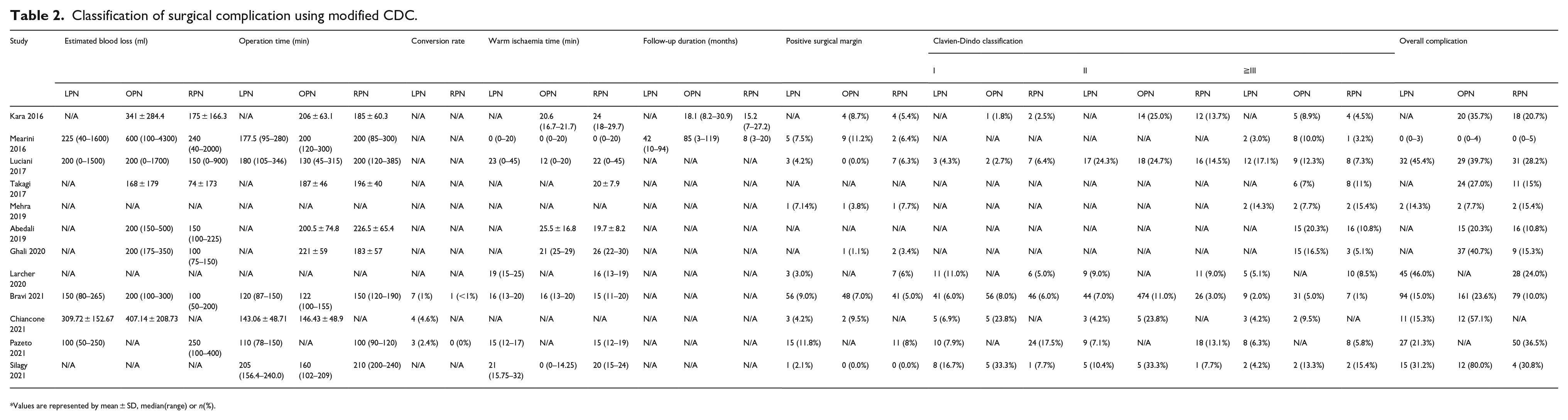
Values are represented by mean ± SD, median(range) or n(%).
Estimated blood loss
Multiple studies reported reduced EBL when performed via RPN approach.20–24 Mearini et al. and Chiancone et al. both reported favourable results of EBL in LPN compared to RAPN/OPN and OPN respectively. Contrastingly, Pazeto et al. 25 reported a higher EBL in RPN compared to LPN (225 ml vs 100 ml; p = 0.008). Our analysis demonstrated that LPN had a statistically lower EBL compared to RPN. A comparison of EBL via the three surgical approaches is presented in Figure 1. Statistical significance was noted between the three surgical approaches (p = 0.004). Pairwise comparison between the surgical approaches is demonstrated statistical significance was noted between EBL in LPN compared to OPN (p = 0.003). However, these results were comparable between LPN and RPN, and between RPN and OPN. Previous study by Haber et al. 26 concluded higher EBL in RPN compared than LPN (323 vs 222 ml, p = 0.01). A systematic review performed by Tang et al. 27 reported a 24–50 ml lower EBL in RPN when compared to LPN, and 39–84 ml lower EBL when compared to OPN. Similar findings was noted by Chen et al. 28 where RPN had a significantly lower EBL compared to LPN (100 vs 150 ml, p < 0.001). Our differing results is most likely attributed to the heterogenicity between the patient cohort and surgeon’s experience between the surgical approaches.
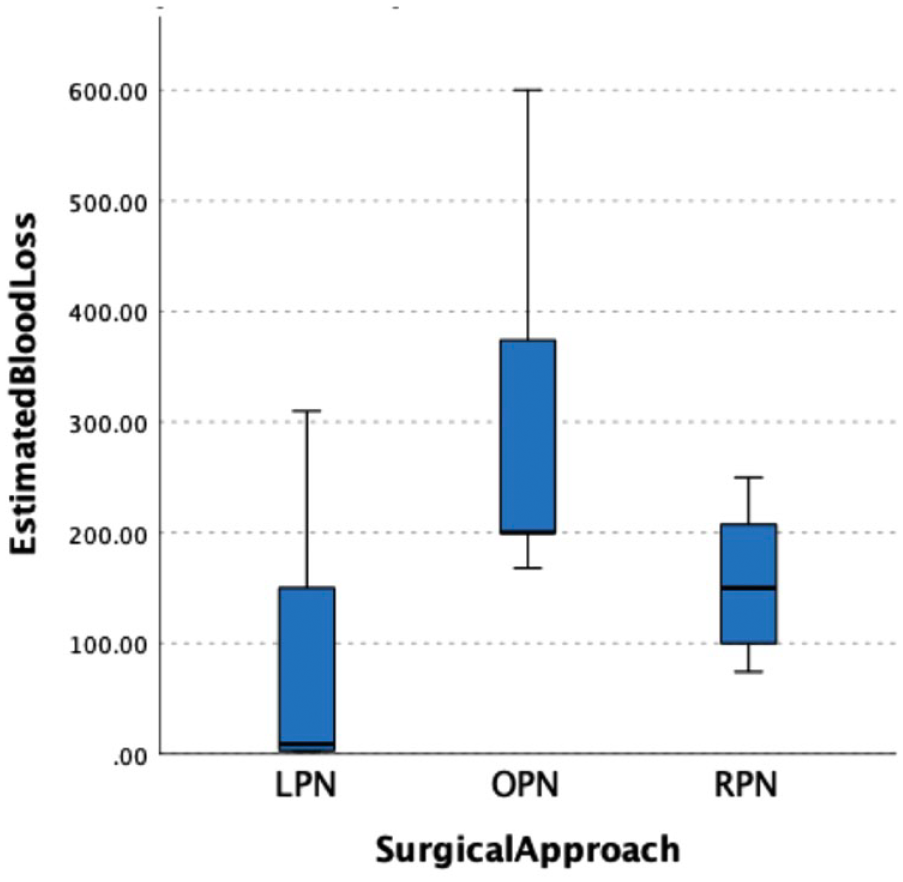
Boxplot showing the estimated blood loss in the three surgical approaches.
Operative time
Mearini et al. 29 noted the mean OT between LPN, OPN and RPN was 201.6 versus 180.3 versus 190.0 min (p = 0.019). They reported that a higher OT was associated with on-demand ischaemia, higher blood loss, need for transfusion and thus, longer hospital stay. Similar results were noted in Bravi et al. 24 where the median OT between LPN, OPN and RPN were 120 versus 122 versus 150 min (p < 0.0001). Abedali et al. 22 noted a reduced OT in OPN compared to RPN (200.5 vs 226.5 min; p = 0.010). The remaining studies demonstrated no statistical differences between the OT when comparing the different surgical approaches.
Our study concludes comparable operative time among the three surgical approaches (Figure 2). A recent meta-analysis performed by Xia et al. 30 reported similar findings for OT between OPN and RPN following sensitivity analysis. Longer OT is known to be associated with higher risk of complications and longer LOS. 31 While the results were comparable, it is important to bear in mind that MIS require additional time for setting up equipment, accurate instrument placements and robot docking in RPN. Thus, after these have been taken to account, the overall ‘skin-to-skin’ contact duration is comparable between the three surgical approaches. 32 From the studies in our review, it was unclear whether the setup and docking time were included in the overall OT. Furthermore, one study included data which predated the RPN era, and only half the studies included data from procedures performed within the last 10 years, resulting in high level of heterogeneity. With surgeon’s gaining more experience in MIS, the overall OT may reduce. Thus, a more updated analysis with recent data is required.
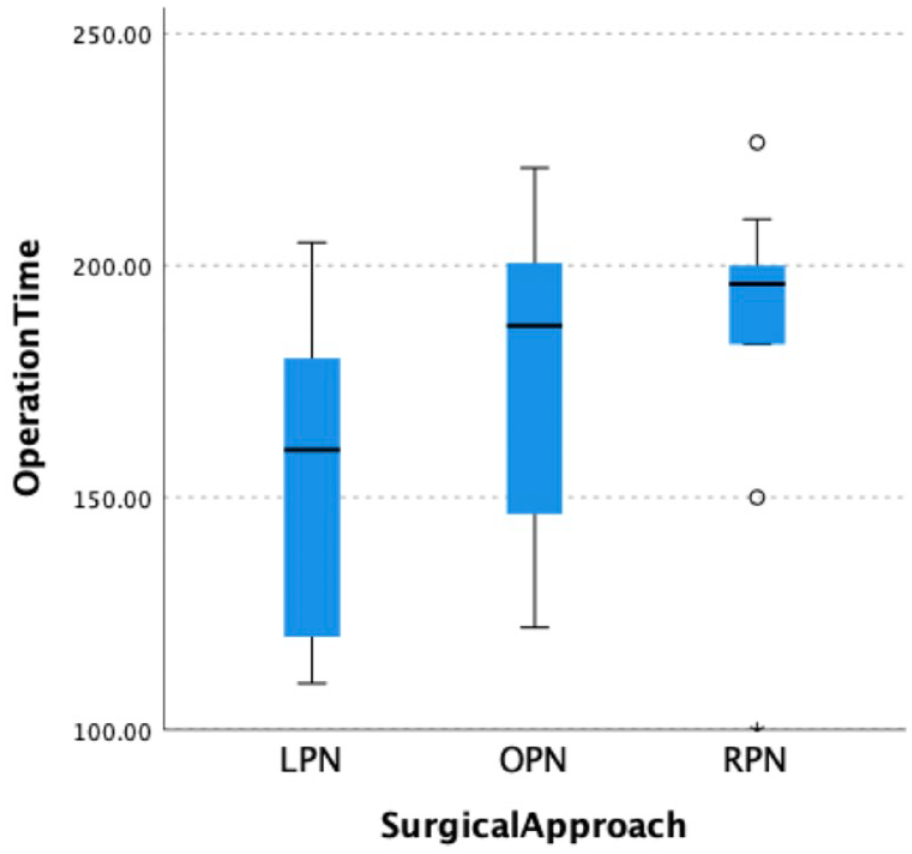
Boxplot showing operating time in the three surgical approaches.
Conversion rate
Three out of all included studies reported their data on the conversion rate from LPN or RPN to OPN. Bravi et al. 24 noted a statistical significance in the CR between LPN and RPN, accounting for seven and one case respectively (p = 0.002). Chiancone et al. 33 noted a total of 4 out of 72 LPN cases which required conversion to open approach. Similar results were demonstrated in Pazeto et al. 25 with reported three LPN cases requiring conversion to OPN, although this was statistically not significant (p = 0.07). Our review concluded no significant difference between conversion rate between LPN and RPN (p = 0.200).
Warm ischaemia time
Our study demonstrated no significant difference was noted (p = 0.760). Most studies reported a lower WIT in MIS compared to open approach, with three studies favouring RPN. Abedali et al., 22 Bravi et al. 24 and Larcher et al. 34 reported statistical significance in WIT when performed via RPN compared to OPN and LPN.22,24,34 Luciani et al. 35 and Silagy et al. 36 both reported a reduced mean WIT via OPN. Mearini et al. 29 reported a lower WIT in LPN compared to OPN and RPN (0.8 min vs 3.3 min vs 1.3 min; p = 0.024). However, three studies demonstrated similar results between the surgical approaches.20,23,25
Positive surgical margin
A positive surgical margin rate provides information on the oncological outcome, which in turn determines the probability of future recurrence and potential metastasis. In our study, no significant difference was noted between the PSM rate in the three surgical approaches (p = 0.549; see Figure 3). A similar finding was noted in Tsai et al. 14 when comparing between RPN and OPN. Luciani et al. 35 reported a higher PSM of 6.3% RPN, 4.2% LPN and 0% OPN. They felt that this correlated to the higher rate of pT1b between the groups (31.8% vs 14.2% vs 15%) and malignant histology (90% vs 82.9% vs 68.5%) in RPN, LPN and OPN respectively. 30 Pazeto et al. 25 noted a statistical difference between LPN and RPN, with favour towards RPN (12.6% LPN vs 4.2% RPN; p = 0.037). While this review did not analyse the long-term follow-up results of the patient cohort, future studies can review the recurrence rate following a PSM. This will provide additional benefits for surgeons when counselling which surgical approach to offer their patients.
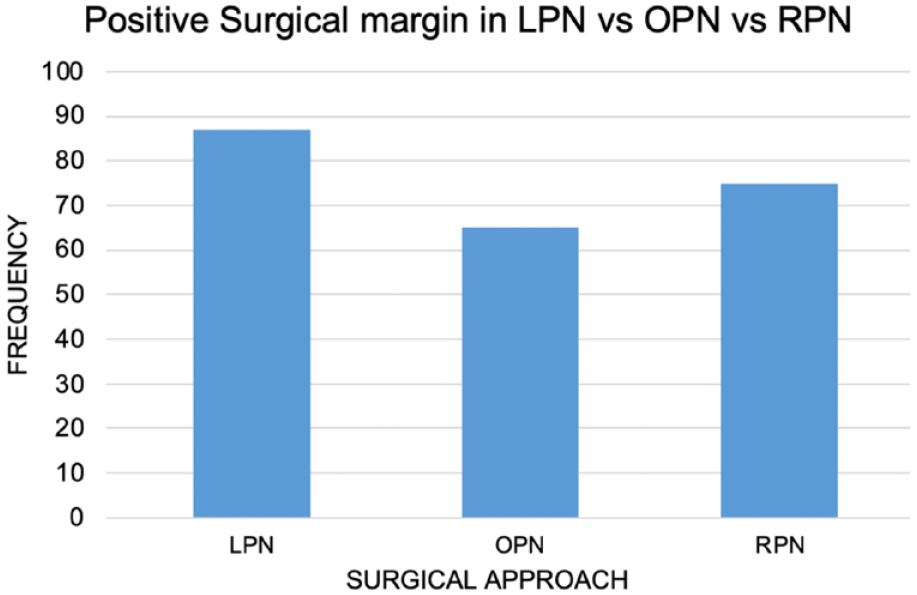
Overall positive surgical margin in the included studies.
Complications
The CDC was used in this review as a standardised methodology to compare the postoperative complications between surgical approaches, thus allowing an objective assessment to draw conclusions. All 12 studies reported its postoperative complications using the CDC. The majority of the studies reported their findings by grouping the complications into Grade I, II and ⩾III. Only Luciani et al. 35 and Silagy et al. 36 reported a breakdown of all complications from CDC I to V. Comparable results were noted between CDC I, II and ⩾III among the three surgical approaches. A systematic review by Choi et al. 37 noted similar results where there were no significant differences between all grades of CDC between RPN and LPN.
Some studies reported comparable results between the surgical approaches.20,38 One study noted a lower rate of overall postoperative complications in LPN compared to OPN (15.3% vs 57.1%). 33 Three studies demonstrated lower rates of overall complications21,34,35 in RPN, and similar findings were noted in a review by Bravi et al. 24 when evaluating the major complications against the three surgical approaches. High-grade complications are commonly seen in OPN.22,23 While Pazeto et al. 25 noted similar results in high-grade complications between LPN and RPN, there was a significant reduction in low-grade complications in LPN.
Statistical analysis was performed to investigate the statistical difference between the surgical approaches in CDC I, II and ⩾III. We found that OPN was associated with higher grade II and ⩾III complications, although this observation was not statistically significant. No significant differences were noted between the three surgical approaches in CDC I, II and ⩾III (p = 0.556, 0.779 and 0.663, respectively). These results were consistent with the literature to date.39,40
Conclusion
The gold-standard treatment for patients presenting with small renal tumours is NSS as per current EAU guidelines. With technological advancements over the last decade, NSS can be performed by laparoscopic, open or robotic approach. Despite the shift towards minimally invasive approach, there remains a significant debate in literature which surgical approach offers better perioperative outcome to patients. In this review, we conclude a lower overall EBL is demonstrated in LPN compared to OPN and RPN. Similar results were noted between OT, CR, WIT, PSM and CDC grades across the three surgical approaches.
We acknowledge that most studies in our review were retrospective, with significant heterogenicity between patient cohort, tumour characteristics and availability of different treatments among centres. Future large prospective, multi-centre studies should be undertaken to provide more validated result of this topic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.