
Abstract
Introduction:
The negative effects of the COVID-19 pandemic on sexual satisfaction have been emphasized in many studies. However, there is not much information about the effects of the COVID-19 pandemic on the sexual satisfaction of healthcare professionals. In addition, it is not known exactly how vaccination application affects sexual satisfaction. Therefore, in this study, we aimed to evaluate whether the sexual satisfaction of male health personnel would change with vaccination.
Materials and methods:
One hundred and two unvaccinated and 95 vaccinated male healthcare professionals participated in this study. The COVID-19 Phobia Scale (C19P-S) and The New Sexual Satisfaction Scale (NSSS) were administered to the participants.
Results:
We did not detect any difference in sexual satisfaction according to vaccine administration. However, we found significant relationships between COVID-19 anxiety and sexual satisfaction. On the other hand, age, fear of COVID-19, and previous COVID-19 infection story were predictive factors on sexual satisfaction.
Conclusion:
The effects of the COVID-19 pandemic on sexual satisfaction are multifaceted. Our findings indicate that fear of COVID-19, rather than vaccination, determines sexual satisfaction.
Introduction
The World Health Organization (WHO) shared information on some cases of pneumonia of unknown etiology in China on 31 December 2019. As a result, WHO declared COVID-19 as a pandemic on 11 March 2020. 1 SARS-CoV-2, the virus responsible for COVID-19, undergoes constant mutations and accumulates changes in its genetic code as time passes. The emergence of new variants of SARS-CoV-2 is anticipated. Some of these variants will appear briefly and then disappear, while others will emerge and persist, potentially supplanting earlier variants. 2
The modes of transmission of COVID-19 are known as direct contact and respiratory tract, 3 but the additional transmission of SARS-CoV-2 may be possible due to its presence in fecal swabs and blood. 4 In the light of previous information in the literature, it has not been shown that COVID-19 is sexually transmitted.5,6 In contrast, sex, by its very nature, requires close contact, so concerns about spreading the disease during sex may be natural. Situations, such as easy and fast transmission routes and the clinical course of the disease, may increase the anxiety of getting sick and carrying the disease. The effects of isolation policies applied during the pandemic process is also important. Restrictions and uncertainty affect individuals psychologically and negatively affect sexual life. 7 Previous studies have also shown that major disasters increase anxiety and negatively affect sexual function.8–10 In addition, a rapidly increasing workload is a critical problem for healthcare professionals during the pandemic. There is also a significant risk of transmission, and there is a high risk of infection of healthcare workers themselves and their family members. Thus, it may cause more intense psychological effects on healthcare workers, who are at the forefront of the pandemic, than the community population.
In the literature, there is little information about the sexual attitudes of healthcare professionals during the pandemic.11–13 For example, a study conducted with 185 healthcare professionals showed that sexual desire, the number of sexual intercourse/masturbation, duration of foreplay, duration of sexual intercourse, and face-to-face sexual intercourse positions decreased during the pandemic. In the same study, it was underscored that the male gender was also riskier regarding sexual dysfunction, 11 which is consistent with the findings obtained in previous studies. In a study conducted with 536 male participants, it has been reported that 19.4% of the participants fear the transmission of COVID-19 during intercourse and the number of weekly sexual intercourse decreases. 14
To our knowledge, there are no studies in the literature reporting on the effects of vaccination on the sexual attitudes of healthcare workers. Therefore, in this study, we aimed to evaluate whether sexual satisfaction of male personnel have changed with COVID-19 vaccination. For this purpose, our main hypothesis was that male health personnel would be more sexually satisfied after administering two vaccine doses in our country. In addition, we hypothesized that other factors, such as age, chronic disease, and whether their current duties in the health system constitute a risk factor for the pandemic, would also affect the sexual satisfaction of male health personnel.
Materials and methods
Sample
Male healthcare professionals who volunteered for the present study between April 2021 and August 2021 were invited. Preliminary information about this study was given to all participants. Participants who volunteered were given research forms consisting of sociodemographic data form, COVID-19 Phobia Scale, and The New Sexual Satisfaction Scale. In this study, 215 people participated. The results of 18 people were not evaluated due to random marking, and analyses were performed with 197 people in this way. One hundred and two unvaccinated male healthcare workers and 95 vaccinated male healthcare workers participated in this study. Volunteering to participate in this study and working actively in hospitals serving during the pandemic and the pandemic process were determined as inclusion criteria. Being under 18, not having an active sexual life, and receiving treatment for sexual dysfunction were determined as exclusion criteria. In power analysis, the findings showed that the participation of 136 people would be sufficient for an accurate statistical analysis with a confidence level of 99% and a confidence interval of 5%.
All procedures performed in studies involving human participants were in accordance with the ethical standards local clinical research ethics committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Scales
Sociodemographic Data Form was used as a form prepared specifically for this research by the research team. In addition to demographic data, such as age, gender, and occupation of the participants, it included questions such as their professional duties during the COVID-19 process and the duration of their regular sexual lives.
COVID-19 Phobia Scale (C19P-S) is a 5-point Likert-type scale consisting of 20 questions and four dimensions: psychological, psychosomatic, social, and economic. 15 High scores indicate high coronavirus elation and negative significant correlations The New Sexual Satisfaction Scale (NSSS) is a 5-point Likert-type scale with 20 questions developed to measure sexual satisfaction. 16 The scale has two sub-dimensions: self-centered and partner-centered. The Turkish validity and reliability study of NSSS was conducted. 17
Statistical analysis
Statistical Package for Social Science windows version 15.0 (SPSS) web software was used for the statistical analysis of this study. Participants were grouped according to their vaccination status, and normal distribution conditions were evaluated with the Kolmogorov-Smirnov test. Independent sample t-test was used to compare the scale scores between groups. The relations of the scale scores with each other were analyzed using the Pearson Correlation test. While evaluating the predictive factors of sexual satisfaction, multiple linear regression analyses were applied. All analyses were based on a p < 0.005 for significance.
Results
According to the results of our sociodemographic data form between the groups, we found a difference only in the number of children and in the death of a first-degree relative or close friend (Table 1).
Sociodemographic data form and reasons of the effect of the pandemic on sexual life reported by the participants.
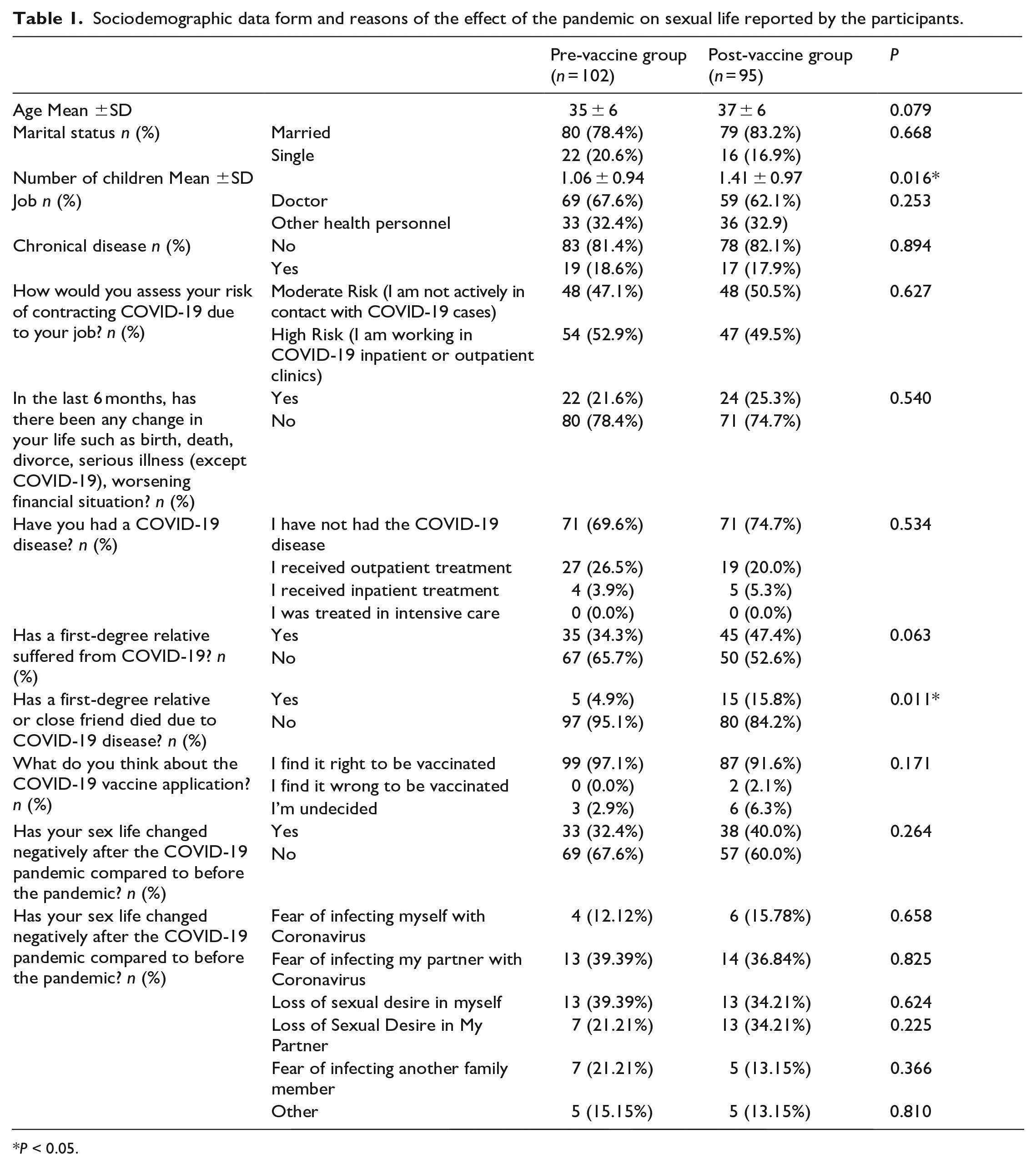
*P < 0.05.
The factors reported by the pre-vaccine (n = 33) and post-vaccination (n = 38) participants, who reported a negative effect on their sexual life, regarding the causes of this negative effect are given in Table 1.
An independent two-sample t-test was applied to examine the relationship between the scale scores between the pre-vaccine and post-vaccine groups. According to the results, no difference was found between both C19P-S and NSSS total scores and subscales (Table 2).
Scale scores in the pre- and post-immunization group.
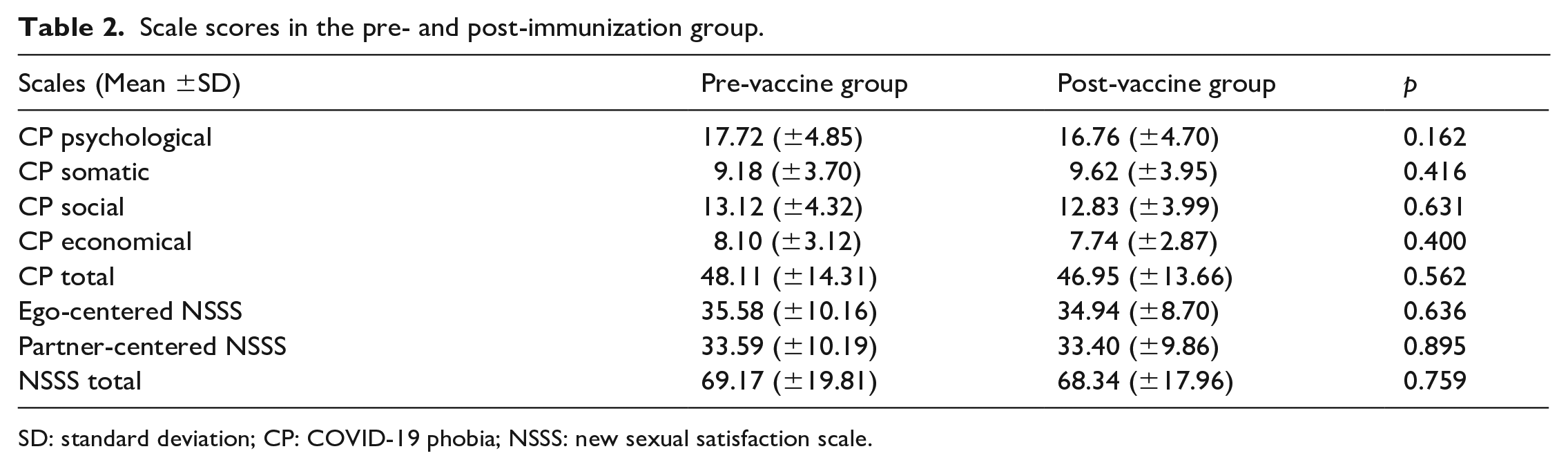
SD: standard deviation; CP: COVID-19 phobia; NSSS: new sexual satisfaction scale.
Relationships between scale scores were examined using Pearson Correlation, and significant negative correlations were found between SF and YCDO scales (Table 3).
Correlations between scales.
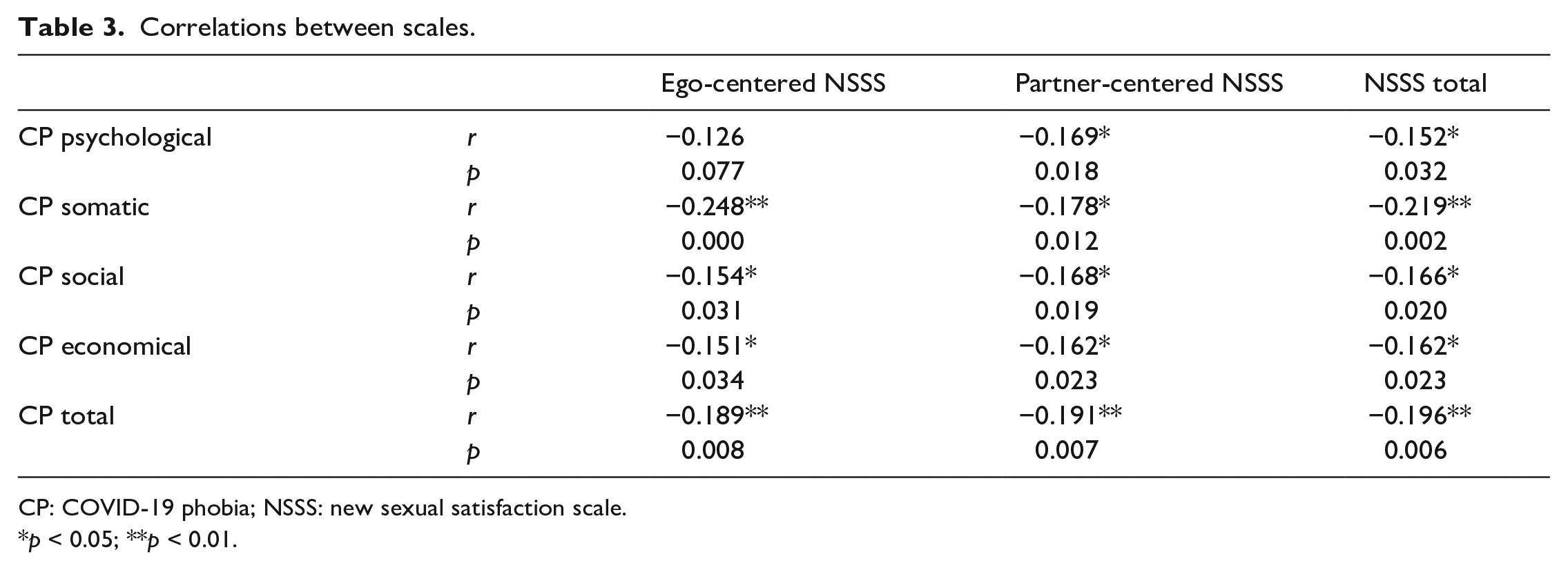
CP: COVID-19 phobia; NSSS: new sexual satisfaction scale.
p < 0.05; **p < 0.01.
Finally, stepwise regression analysis was applied to determine the factors that may affect the YCDO scores. Accordingly, age, CF total score, and COVID history have a negative predictive effect on YCDO (Table 4). On the other hand, there was no significant effect of chronic disease status, working conditions during the pandemic, and vaccination status on YCDO.
Regression analyses for NSSS.
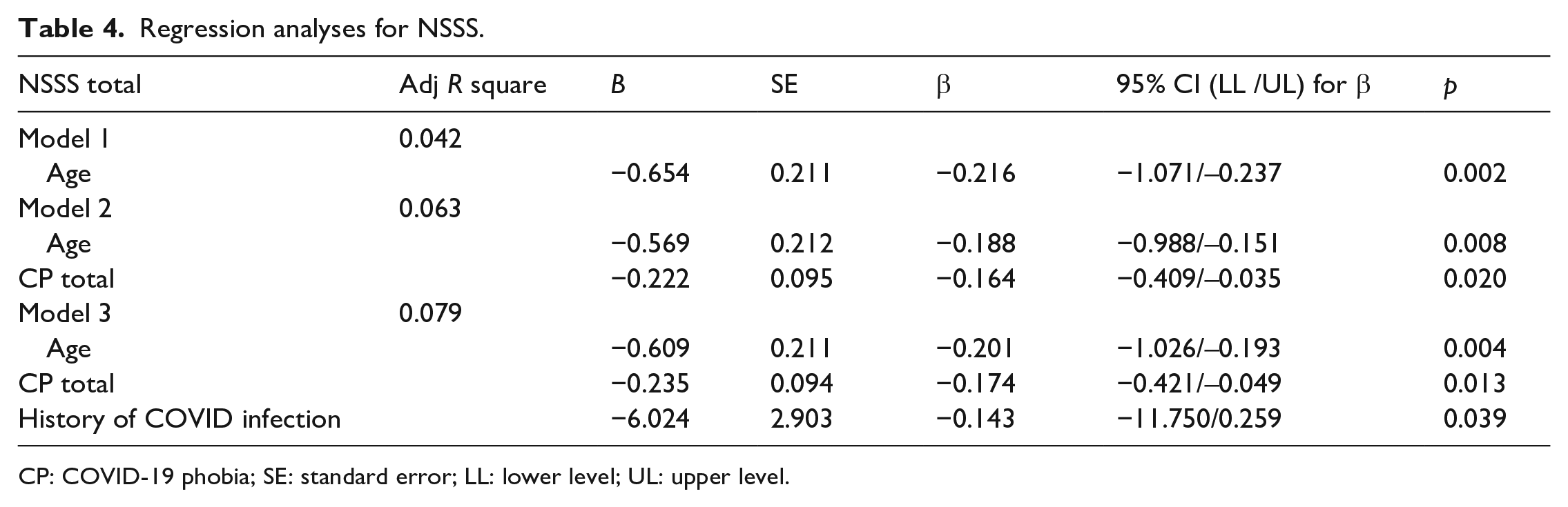
CP: COVID-19 phobia; SE: standard error; LL: lower level; UL: upper level.
Discussion
In this way, our initial hypothesis that the vaccine would have positive effects on sexual attitudes could not be confirmed. According to our second hypothesis, it was partially confirmed that other factors would be effective on sexual attitudes during the pandemic period. In other words, having a chronic disease and taking an active role in the departments where the risk is high in the pandemic did not have a predictive effect on sexual attitudes. However, age, COVID history and coronaphobia-related anxiety had a negative predictive effect on sexual attitudes.
Post-pandemic observations and prospects for mental health point to increasing mental health problems. It is predicted that there may be an increase in the frequency of anxiety disorders, post-traumatic stress disorder (PTSD), and depression in particular.18,19 The pandemic has also had severe adverse effects on healthcare workers. Increased workload, greater risk of transmission, and witnessing more adverse health outcomes may affect healthcare workers more than the general population. For example, in the SARS epidemic in 2003, it was reported that healthcare professionals who were actively involved were more negatively affected socially and psychologically than the rest of the society. 20 Studies on the current COVID-19 pandemic, on the other hand, found 29.8% stress, 24.1% anxiety, and 13.5% depression symptoms in healthcare workers. 21 This study also reported that medical staff experienced 1.4 times more fear and twice more anxiety and depression symptoms than administrative staff. It can be expected that healthcare professionals, who have the potential to be most affected by the pandemic, will also be adversely affected regarding sexual satisfaction and sexual activity. However, our findings showed that working in high-risk places was not a predictor of sexual satisfaction. In this sense, the subjective interpretation of the risk of contamination regarding their duties may play a more important role than the objective nature of the place of duty. We discuss possible interpretations of our findings below.
The relationship between sexual activity with the pandemic is multifaceted. Sexual activity positively affects mental health during the pandemic. 22 However, the pandemic also negatively affects mental and sexual health. 23 Previous studies indicate that sexual desire and sexual activity decreased in both sexes during the pandemic. 24 In a study conducted in England with 868 people who were self-isolating due to the pandemic, the prevalence of sexual activity was less than 40%. 22 In the same study, a relationship was found between advanced age, female gender, being single, low alcohol consumption, and low sexual activity. Our findings showed that the negative relationship between age and sexual satisfaction seems to be compatible with the data in the literature. In addition, approximately one-third of participants in both groups reported that there were negative changes in their sexual lives than in the pre-pandemic period. In a study conducted with 967 people, 22% of the participants reported a decrease in sexual desire, and 41% (n = 396) reported a decrease in sex frequency. 7 In this sense, our data seem to be compatible with the literature. In addition, it is noteworthy that having a history of COVID, which is another finding of ours, has negative effects on sexual satisfaction. Previous studies have suggested mechanisms, such as endothelial dysfunction, impaired pulmonary hemodynamics, and subclinical hypogonadism related to the development of erectile dysfunction in patients with COVID. 23 The role of psychological factors, such as anxiety, is important concerning the negative effects of a history of COVID-19 on sexual satisfaction. However, it may not be sufficient to account for this effect only with psychological factors. Thus, further studies on possible organic factors are required.
There are few studies in the literature on the sexuality of healthcare professionals during the pandemic process. In a study conducted with healthcare professionals working in pandemic hospitals, the sexual desire, duration of foreplay, and the number of sexual intercourse decreased. 11 In addition, 47.8% of the participants in this study reported that they were worried about sexuality due to the COVID-19 outbreak. 59.4% of the participants were worried about infecting their partner, and 21.9% reported that they were worried about catching this virus from their partners. The same study also reported higher anxiety scores in patients with sexual dysfunction. 11 A study conducted with 359 male participants showed that healthcare professionals obtained higher IEFF-5 scores than the control group. 12 In a study conducted in our country, it was revealed that the level of sexual desire, frequency of sexual intercourse, and duration of foreplay decreased in healthcare professionals during the pandemic; the findings suggested that high anxiety levels seemed to be a risk factor for sexual dysfunction. 13 Similar to the findings obtained in our study, it can be said that there is a significant relationship between sexual satisfaction and sexual attitude and anxiety. People can be expected to feel responsible both because of the risk of contamination themselves and the risk of infecting their environment. This responsibility also causes anxiety and anxiety, which may have direct and indirect effects on sexual attitudes. Our current data suggest that anxiety may be more effective on sexual satisfaction than vaccination. Even with the vaccine, people may experience anxiety that may affect their daily functioning. Therefore, anxiety-related interventions may play a central role in sexual health services. According to our findings, the vaccine did not affect sexual satisfaction. However, possible explanations that may have an impact on our vaccine results may be that the pandemic remains effective at the time of our study, administrative social isolation limitations continue, and vaccination can be completed in a small population. In addition, non-healthcare partners of healthcare professionals were not able to access the vaccine at the time of our study. All these factors may prevent the emergence of a relationship between vaccination and sexual satisfaction.
There is a high probability of experiencing stigma and medical distrust, which can affect the acceptance of the COVID-19 vaccine in society. In a compilation of 18 studies involving a population of 62,728 healthcare workers examining vaccine hesitancy, considering the periodic conditions of the pandemic, vaccine refusal or indecision ranging from 19.1% to 37.7% was detected. 25 This result suggests that healthcare workers continue to struggle with the COVID-19 crisis and exhibit hesitancy toward vaccination, which is similar to the correlations found in the general population. Even if vaccination has been administered, mistrust in treatment may have also influenced our results.
The limitations of our study are that the scales are self-report scales; they are designed as cross-sectional and LGBT individuals are not included in this study. The fact that the relationship between administrative social isolation restriction and sexual satisfaction was not examined in our study is one of our limitations. This is because healthcare professionals are excluded from administrative social isolation limitation. Therefore, prospective studies with a higher number of participants can be instructive.
Conclusion
The negative effects of the pandemic process on sexual health have been reported in many studies. Our study examined the factors that may be related to sexual satisfaction and found that age, coronavirus anxiety, and COVID history were significant. In this sense, the anxiety factor may be an intervening target in health care. It would be helpful to consider the psychological factors in the services provided regarding sexual health.
Footnotes
Authors’ contributions
Conceptualization: Metin Yığman; Methodology: Fatih Yığman; Formal analysis and investigation: Cihat Özcan, Cuma Aytekin; Writing-original draft preparation: Metin Yığman, Fatih Yığman; Writing—review and editing: Fatih Yığman; Supervision: Metin Yığman
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Health Sciences University Gülhane Training and Research Hospital Clinical Research Ethics Committee (Date: 08.04.2021, decision no: 2021/82) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
All authors give their consent to publish the article in the current form.