
Abstract
Objectives:
The aim of this study is to analyze the compositions of urinary stones and investigate their distributions in different ages, genders, seasons, and clinical features of Northern Vietnamese patients.
Methods:
A total of 231 patients with urinary stones from Northern Vietnam were collected and analyzed composition from 1/2021-12/2022. For all patients, age, sex, stone location, stone side, urine pH, and hospitalized date (month) were collected.
Results:
Kidney stones are more frequently found in men than women with the male: female urinary stones ratio in this study being 1.96:1. The highest stone prevalence appeared between 60 and 69 years old. The most common stone composition was calcium oxalate, followed by calcium phosphate, uric acid, struvite, and cysteine. Mix stones of CaOx and CaP were more prevalent than pure stones. Males submitted more CaOx, CaP, and UA stones, whereas females were susceptible to infectious stones. Stones were more frequently found on the left side of the upper urinary tract (51.9%) than on the right side (27.3%) and lower urinary tract (7.8%). Cultural tendency leads to a smaller number of stones during the Lunar new year (February), and Ghost month (August).
Introduction
Urolithiasis is a disease that has been present throughout human history, and it is one of the most common and painful types of urological disorders.1,2 Despite advancements in medical science, it continues to be a significant problem. Urolithiasis is characterized by the formation of stones in the urinary tract, including the kidneys, ureters, bladder, or urethra due to an imbalance in the biochemical components that promote or inhibit lithogenesis. The disease has many causes, including environmental, genetic, infectious, metabolic, nutritional, and socioeconomic factors. However, the epidemiological profile of urolithiasis has changed over the past 50 years and affects 4%–20% of the population, with different prevalence rates in different regions of the world and a recurrence rate of 50% in the first 5 years.3,4
The prevalence of kidney stone disease in Vietnam is rising significantly these years. The reasons for this trend are not entirely sure. With a global incidence of around 10%, urolithiasis and its management is becoming a major healthcare issue.2,3 A more detailed and in-depth understanding of the urinary stones composition in each patient case, and also a static study in specific populations will help to assess, treat and prevent the disease more effectively.4–6 However, to date, there is no study of urinary stone composition in Vietnam. Our laboratory is the first and only laboratory in Vietnam to analyze the urinary stone composition. According to our knowledge, epidemiologic data about this condition in Vietnam are limited with the few works focused on questionnaires to detect chronic kidney, 7 and the temperature trend of kidney disease. 8
The purpose of the present study is to determine whether differences in gender, age, season, and clinical characterizations may account for differences in stone formation and stone composition.
Materials and methods
Patient population
In the period from 1/2021 to 12/2022, 231 urinary stones from patients diagnosed with urolithiasis in Hanoi, Vietnam were submitted for this study.
Stone analyses
Each stone was washed before being dried in the oven at 100°C. The specimen was then crushed into a fine powder using a mortar and pestle. Powder samples were analyzed by Fourier transform infrared spectroscopy. Chemical analysis using titration and atomic absorption spectroscopy, and crystal analysis using X-ray diffract were used to confirm the composition of the stones when needed.
Statistical analyses
Data were analyzed using Minitab. A p-value of <0.05 was considered significant. Results were expressed as mean ± standard deviation (SD). The two-sample t-test was used to compare the mean age of male and female patients. The Chi-square tests were used to evaluate the effects of age, sex, and month on stone type. For monthly trends, the one-sample chi-square test was used.
Ethics approval
This study was in accordance with ethical standards and received approval from the Ethics Committee of the E Hospital, Hanoi, Vietnam.
Results and discussions
Age and sex distribution
Table 1 and Figure 1 show the sex and age distribution of patients having stones submitted in this study. Two hundred thirty-one patients distributed as 153 male (66.2%), and 78 female (33.8%), with a male: female ratio is 1.96:1.
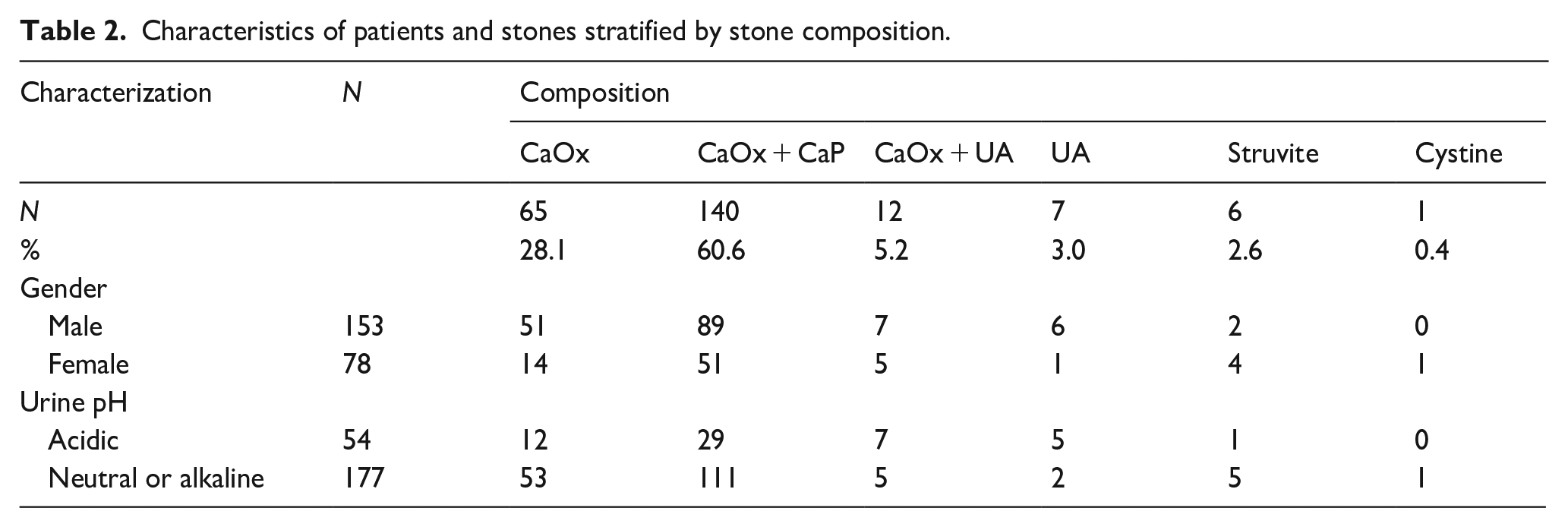
Characteristics of patients and stones stratified by stone composition gender.
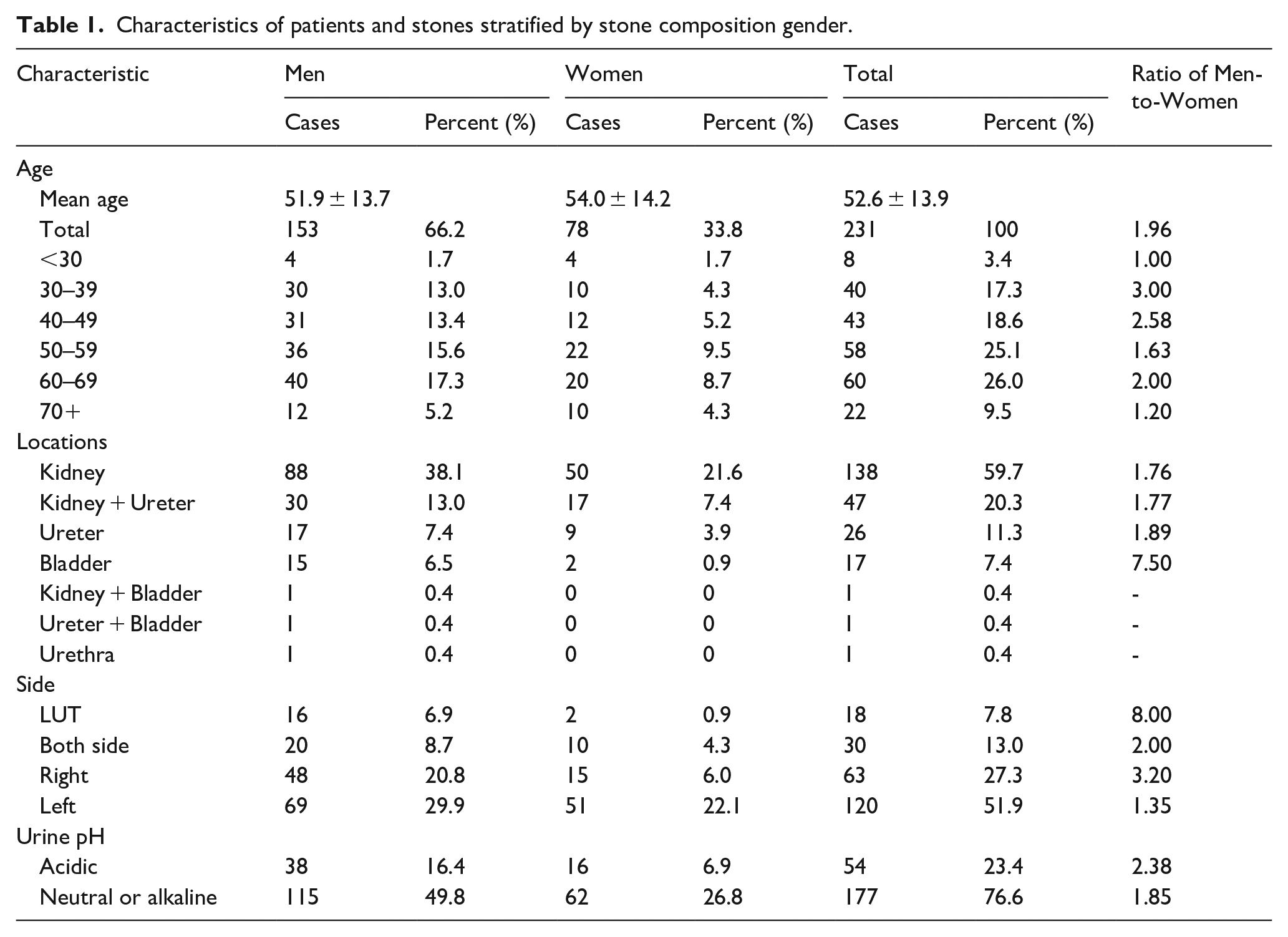
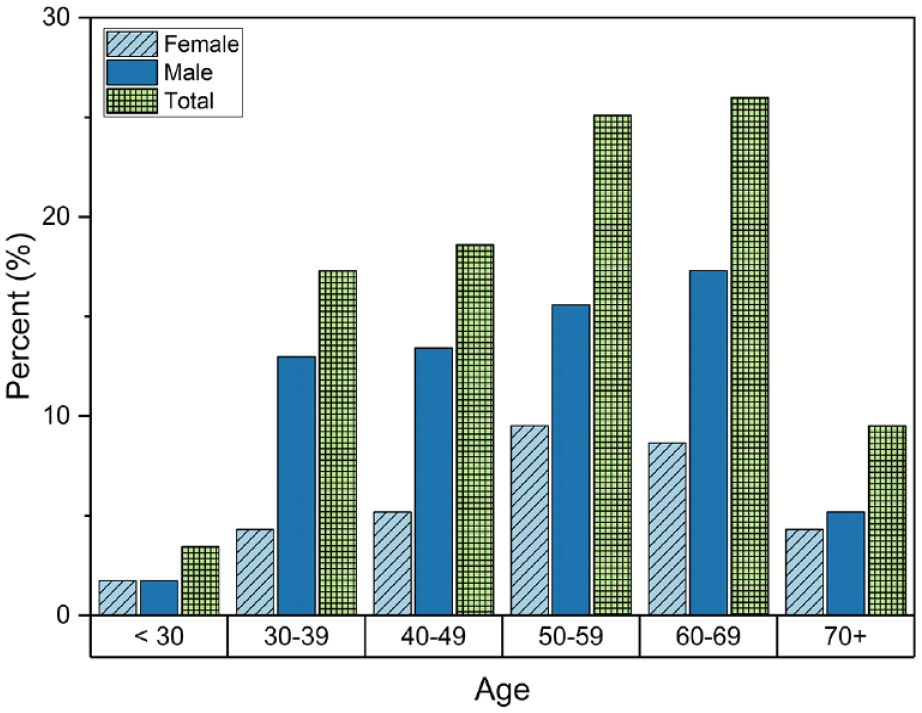
Gender and age of 231 patients.
The patients were from 14 to 88 years old, with a mean age of men, women, and total cases of 51.9 ± 13.7, 54.0 ± 14.2, and 52.6 ± 13.9 years old, respectively. At α = 0.05 level of significance, there is no difference in the average age of female and male patients. The highest occurrence of urinary stones was observed in patients aged between 60 and 69 years. At ages <30 and ⩾70, men and women cases are somewhat equal, with the ratio of Men-to-Women stone formers of ~1. From 30 to 69 years, men were more likely to form stone than women, with a ratio of Men-to-Women > 1.
Stone location and side
Figure 2(a) shows that upper urinary tract (UUT) stones counted for 91.3%, including 59.7% at the kidney, 11.3% at the ureter, and 20.3% at both the kidney and ureter. Lower urinary tract (LUT) counted for 7.8%, including 7.4% at the bladder, and 0.4% at the urethra. 0.8% of stones are found at multiple locations at both the upper and lower urinary. This data confirms that main urolithiasis in Vietnam is also in upper urinary tract stones, similar to Japan, 9 China, 10 and Thailand. 11
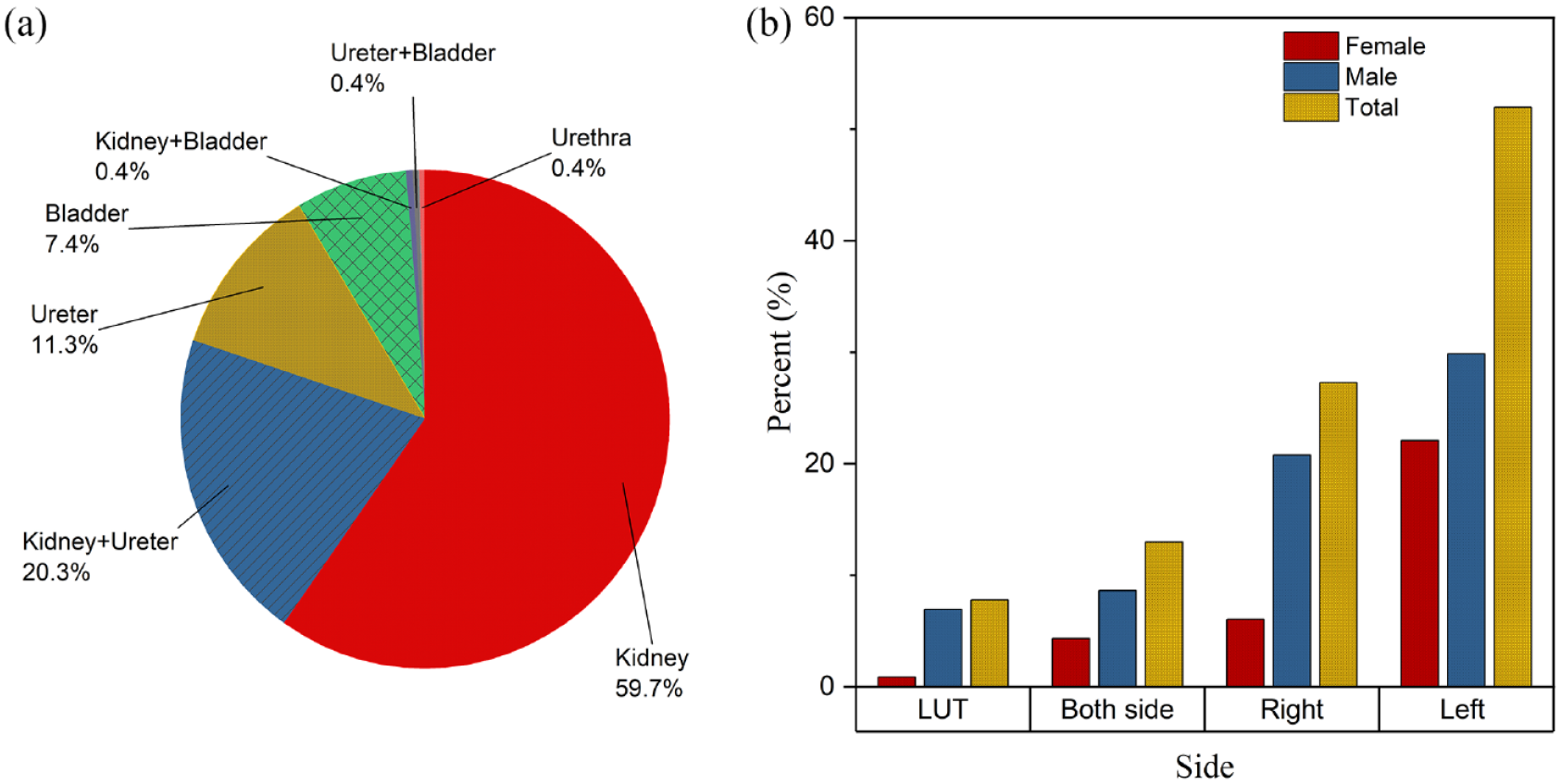
(a) Stone location and (b) stone sides.
LUT stones in men are significantly larger than in women (χ2 = 10.89, p < 0.001), with a relatively high male:female ratio of 8:1, which is significantly higher than the overall male:female ratio of 1.96:1. Several factors contribute to this observed difference. First, men typically have a longer and more crooked urethra than women, leading to the potential of stone getting stuck and growing more within the LUT. Second, men usually delay seeking medical care or underestimate the urinary stone symptoms,12–14 leading to a longer time for stone growth and increasing the potential of passing stones from the UUT to the LUT. In addition, urinary stasis, such as benign prostatic hyperplasia (BPH), neurogenic bladder disorder, or inverted papilloma of the bladder (IPB), causing bladder outlet obstruction is also another primary cause of bladder calculi.15,16 These conditions affect males more commonly than females. 16 Thus, LUT stones are more commonly found in men than in women.
Figure 2(b) shows 51.9% of stones were found on the left side of the UUT, 27.3% were on the right side, 13.0 were on both sides, and 7.8% cannot classify the side because they were in the LUT. This data agrees with many previous studies.17,18 The reason for this trend is not entirely clear, but several factors may contribute to the observed pattern. Anatomical differences between the right and left kidneys, such as variations in blood supply and drainage, can affect stone formation. The right kidney is positioned slightly lower than the left kidney, which may influence the path and flow of urine and the propensity for stone development.
Month distribution
Figure 3 shows that there was a significant decrease in the number of urinary stone patients in February (p = 0.005) and August (p = 0.012). Monthly patients of 10 other months did not significantly vary by month (p = 0.536).
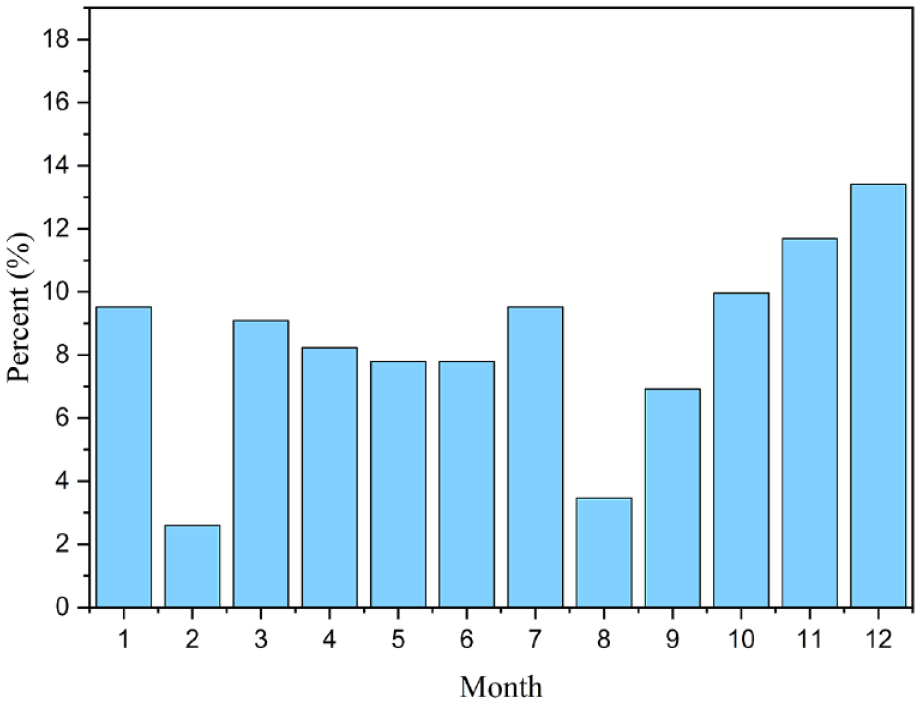
Month distribution of stones.
February is the Vietnamese Lunar New Year (the first month of the Lunar calendar). During the Lunar new year month, hospitals are partially closed, transportation is limited, and in Vietnamese culture, hospitalization is a bad luck activity that people tend to avoid as much as possible in the first month of the year. Similarly, August (the seventh month of the Lunar calendar) in Vietnamese culture is the Ghost month, when the gate of hell is open. People believe that Ghost Month brings bad luck to them, thus they avoid surgery, buying cars, moving house, marrying... These reasons led to a small number of urinary stone patients being hospitalized in February and August.
China and Taiwan also celebrate the same Lunar New Year as Vietnam, and some studies19–21 also showed that there was also a significant decrease in the number of urinary stones in February. Interestingly, this phenomenon was explained by the winter season with low temperatures instead of the Lunar New Year.19–21 However, the difference in the temperature average of winter and summer in Northern Vietnam is only ~10°C, much smaller than the difference in the temperature average of winter and summer in China and Taiwan ~30°C. Therefore, low temperatures in February cannot be the main reason for the small number of patients in Vietnam. Moreover, low temperatures cannot explain the same phenomenon of fewer patients in August.
To evaluate the effect of Lunar New Year and Ghost Month on the number of patients with a larger population, we also collected the number of inpatients and outpatients of the whole hospital (hospital E) during 12 months of the year. Interestingly, the data shows that both inpatients and outpatients in February are the smallest of the year. Inpatients and outpatients in February are statistically smaller than in the other months with p = 0.001 and 0.000, respectively. This data supports that the small number of patients in February is due to the Vietnamese Lunar New Year, and this phenomenon is observed for urinary stone patients, as well as other inpatients and outpatients of the hospital. On the other hand, both inpatients and outpatients in August are smaller than in adhesion months (July and September). However, inpatients and outpatients in August are not significantly different from the other months with p = 0.948 and 0.973, respectively. While both Lunar New Year and Ghost Month are affected by cultural tendencies, only Lunar New Year is a national holiday with officially about 7 days off. It could probably be the reason why the Lunar New Year shows significant effects on decreasing the number of patients than Ghost month.
Stone composition
Table 2 and Figure 4 show that of 231 stones, only 73 stones (31.6%) had one component, 152 stones (65.8%) consisted of two components, and 6 stones (2.6%) mixed three components. We detected calcium oxalate (CaOx) in 223 stones (96.5%), including 65 stones (28.1%) of pure CaOx, 140 stones (60.6%) mix of CaOx and calcium phosphate (CaP), 12 stones (5.2%) mix of CaOx and uric acid (UA), and 6 stones (2.6%) mix of CaOx, CaP, and struvite. CaP was found in 140 stones (60.6%), and all of them are in a mixture with CaOx. UA was found in 19 (8.2%), including 7 stones (3.0%) of pure UA, and 12 stones (5.2%) mix of CaOx and UA. Struvite was found in 6 stones (2.6%), all of them in a mixture of CaOx and CaP. Cystine was found in 1 stone (0.4%).
Characteristics of patients and stones stratified by stone composition.
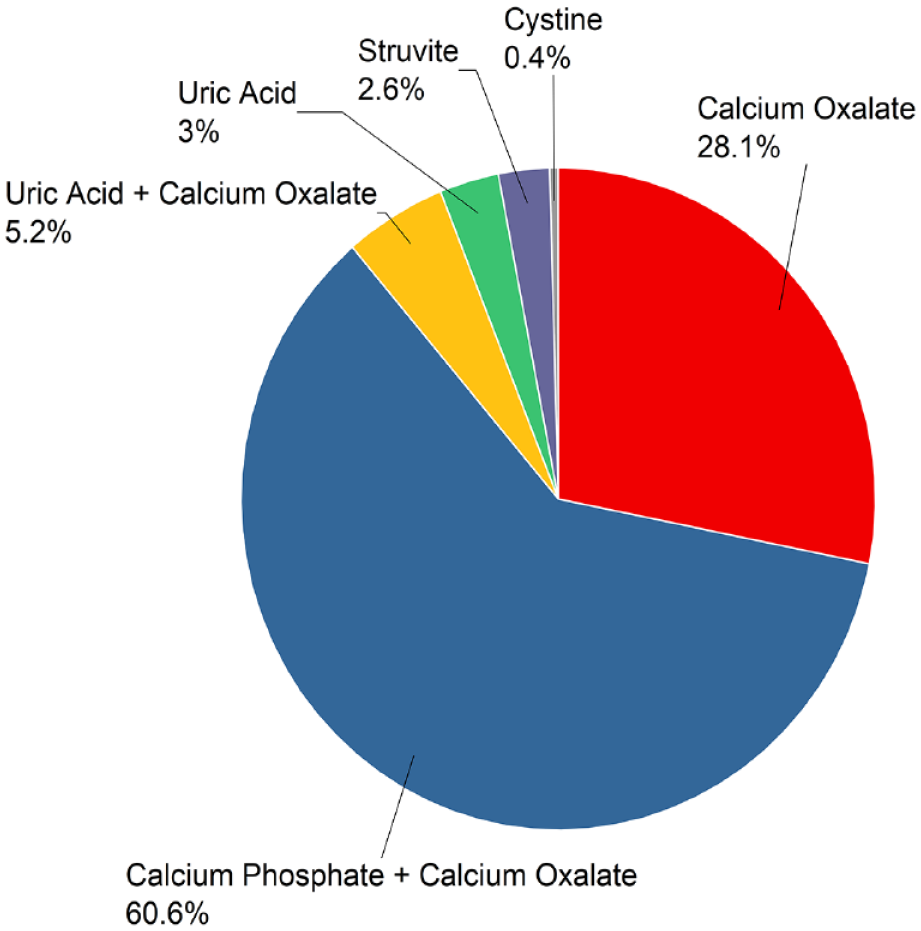
Stone composition.
The data shows that CaOx stone was the most prevalent kidney stone type (96.5%), similar to the reports of stone distribution worldwide. 22 In Europe, CaOx stone was reported 61%, 23 in Japan was 82%,24,25 and in India was 93%. 26 Our data revealed that mixed stones, notably CaOx mixed with CaP were more prevalent than pure stones. Early-formed CaP crystals can nucleate CaOx in metastable urine at the later nephron segments; thus, heterogeneous nidus is predominantly formed. 27 This might be the explanation for the high prevalence of CaOx cohered with CaP.
Stone composition by gender and urinal pH
CaOx stones were preponderant than other stones in both sexes. The proportions of CaOx were much higher in males than in females (χ2 = 25.2, p < 0.001), with male:female ratio of 2.01. Similarly, the proportions of CaP were much higher in males than in females (χ2 = 8.9, p = 0.003) with male:female ratio of 1.74. There is no significant difference in gender trends of UA stone (χ2 = 2.8, p = 0.108), and cystine stone (χ2 = 1.0, p = 0.317). Similarly, there is no significant difference in gender trends of struvite stone (χ2 = 0.7, p = 0.414).
Men are at higher risk for kidney stones overall, possibly because of diet tendencies that raise CaOx, CaP, and UA supersaturations, such as higher protein intake in men.28,29 Overall, males submitted more CaOx, CaP and UA stones, which are stones due to lifestyle tendencies. whereas females were susceptible to infectious stones such as struvite and cysteine.
The struvite stone has a male:female ratio is 1:2, while the overall stone male:female ratio is ~2:1. This ratio is in good agreement with some previous studies.30,31 The origin of this ratio is because struvite stones are caused by an upper urinary tract infection (UTI) from bacteria. Women have a shorter urethra than men, which allows bacteria to ascend more easily into the bladder and urinary tract. This anatomical difference increases the risk of developing UTIs in women, which significantly contributes to struvite stone formation. 1
Cystine stones are primarily caused by a rare genetic disorder called cystinuria, which is inherited in an autosomal recessive manner. 32 This means that both males and females have an equal chance of inheriting the cystinuria gene mutation from their parents. 32 In this study we found one case of cystine stone from a female patient.
Urinary pH (⩽ 5.5) was associated with UA stones, while neutral urine or alkaline urine was more associated with struvite stones, which is consistent with previous studies. 23
Limitation and strength
Limitation of this study: Stones are collected during surgery, leading to a selection bias because of the exemption of stones passed naturally through the urethra. Second, the patient population in this study is small and within a single hospital, which may not reflect the composition of stones in the population. Also, due to the small number of samples, it is hard to correlate uric acid, struvite, and cystine stones with age and month. Further epidemiological study of urolithiasis with a larger number of patients needs to be investigated in the future.
Strength: This stone composition study is the first time conducted in Vietnam. Our data is the first set of data about the epidemiology of urolithiasis in Vietnam. A detailed understanding of the composition of urinary stones and a statistical study in specific populations will help to assess, treat, and prevent the disease more effectively.
Conclusions
Kidney stone disease is common in the rural communities of Northern Vietnam. Our study presented an analysis of stone compositions of urinary patients in Northern Vietnam. Significant disparities of stone compositions existed among different genders and ages. Overall, males submitted more CaOx, CaP and UA stones, whereas females were susceptible to infectious stones. The underlying mechanism, including metabolic differences and the function of estrogen, needs to be investigated in the future.
Supplemental Material
sj-xlsx-1-urj-10.1177_03915603231208090 – Supplemental material for The first epidemiology of urolithiasis in Northern Vietnam: Urinary stone composition, age, gender, season, and clinical features study
Supplemental material, sj-xlsx-1-urj-10.1177_03915603231208090 for The first epidemiology of urolithiasis in Northern Vietnam: Urinary stone composition, age, gender, season, and clinical features study by Lien D Nguyen, Trung T Nguyen, Luc V Mai, Phuong V Bui, Van Thi Nguyen, Giang TB Truong, Minh TN Luu, Hung T Duong, Loi D Vu and Thao TH Hoang in Urologia Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Institute of Chemistry, VAST [the grant number CSCL06.04/22-23].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.