
Abstract
Introduction:
Bladder stones account for 5% of all urolithiasis. Patients present with LUTS or acute urinary retention. Thus, warranting an early intervention. Minimally invasive approach with laser lithotripsy is the present gold standard to treat bladder stones.
Aims and objectives:
To evaluate the outcomes of TFL (60 W) for bladder stones performed under local anesthesia as a day-care procedure.
Materials and methods:
This was a retrospective single-center study conducted after obtaining IRB approval. Study period was between June 2021 and June 2022 were included. All patients were operated under local anesthesia as a day care procedure. The procedure was carried out using an 18 Fr laser sheath and calculus dusted using TFL energy (15–30 W). Parameters including operative time in minutes, complications were recorded. Patients were encouraged oral and normal voiding in the immediate post-op period.
Results:
A total of 47 patients with bladder stones presented during this period. Of these, 30 underwent laser lithotripsy (TFL) for bladder calculi. The clinical presentation of patients was LUTS in 28 (93%) and 5 (16%) patients had AUR. The average size of the stone in this series was 15 ± 2.8 mm. The mean duration of laser lithotripsy was 15 ± 5.4 min. Energy to dust the stone was variable with mean LASER energy of 18.23 ± 10 W. All patients tolerated the procedure well and none required conversion to conventional anesthesia. One patient failed to void in the post-op period. 100% clearance rate was documented in all patients.
Conclusion:
Thulium fiber laser for transurethral cystolithotripsy of bladder stones under local anesthesia is a feasible technique with minimal morbidity and good outcome.
Introduction
Bladder stones account for approximately 5% of all cases of urolithiasis. 1 The most common clinical presentation is lower urinary tract symptoms (LUTS) with or without acute urinary retention (AUR). Open surgery is an effective approach for the management of bladder stones but is associated with high morbidity. Therefore, less invasive modalities, such as endoscopic management of bladder stones, are preferred in view of less morbidity and good stone clearance rates.
There has been a paradigm shift in the management of urolithiasis with the introduction of light activation by the stimulated emission of radiation (LASER) technology—specifically pulsed lasers 33 years ago. 2 Pulsed lasers are the only lasers suitable for safe endoscopic lithotripsy,3,4 and of these, Holmium: Yttrium Aluminum Garnet (Ho: YAG) laser is the current gold-standard laser in endourology.4–6 Recently, Thulium Fiber laser (TFL) has emerged as a new laser technology for endoscopic lithotripsy. 7 The TFL showed its appealing characteristics in several preclinical studies, exhibiting the widest and most flexible range of parameters among the existing laser lithotripters.8,9 The first clinical trial of TFL was conducted in Russia in 2018 and it was in June 2020 that this technology was approved worldwide.7,10
TFL differs from the Ho: YAG laser in many aspects. Instead of using a flash lamp as the energy source, the TFL uses several laser diodes that excite the thulium ions contained inside a very long and thin fiber (10–20 µm core diameter), and the emitted laser beam (wavelength: 1940 nm) can work in a continuous or pulsed mode with the widest range of parameters ever seen in the market.11,12 The pulse energy in a 60 W thulium laser machine can go as low as 0.025 J and as high as 6 J, and the pulse frequency can reach up to 2400 Hz, with a peak power of 500 W, and an average power of 2–60 W. Additionally, the operator can choose between a short or long pulse duration as the case may be, thus adding to the versatility of the laser (200 µs–50 ms).11,13 These characteristics largely surpass those of the HO: YAG technology. So,TFL technology offers greater versatility and control of pulse parameters than the HO: YAG laser. The ablation speed of the TFL is faster than that observed with the HO: YAG laser at any setting.13–15 Studies comparing both laser technologies under identical parameters reveal a higher ablation speed of the TFL of up to two to five times higher in terms of fragmentation and dusting modes, respectively.14–16 Owing to these advantages, TFL is being preferred over HO:YAG laser in urology.
In this study, we aimed to evaluate the outcomes of TFL (60 W) for bladder stones performed under local anesthesia as a day-care procedure.
Materials and methods
This was a retrospective single-center study conducted after obtaining IRB approval. Patients who underwent TFL treatment for bladder stones between June 2021 and June 2022 were eligible for inclusion. All patients were operated under local anesthesia by a single surgeon with more than 10 years of endourology experience.
The exclusion criteria were: (1) patients not willing to undergo surgery under local anesthesia; (2) patients with limb deformity; (3) stricture urethra; (4) concomitant ureteric stone; (5) benign prostatic hyperplasia; (6) chronic kidney disease (CKD); (7) active febrile urinary tract infection (UTI); and (8) pediatric patients with bladder stones.
All patients were counseled regarding the procedure and assured that in case of any pain they would be converted to standard anesthesia. Bladder stone size was documented on ultrasonography (USG) and plain KUB radiograph (Figure 1).

X ray KUB showing bladder stone.
All patients underwent basic investigations. A single dose of injection ceftriaxone (1 g intravenous), injection amikacin (10 mg/kg body weight), and injection diclofenac (75 mg, intramuscular were administered 30 min prior to the procedure. The patient was initially placed supine and under all aseptic precautions’ xylocaine jelly 2% (20 mL) was instilled slowly in the urethra and then the meatus was occluded with a penile clamp for 15–20 min. The patient was then placed in the lithotomy position and under sterile conditions an 18 Fr laser sheath (Shree Surgicals; India) with 2.9 mm telescope (Scholly; Germany; Figure 2) was introduced under vision and calculus dusted using TFL 400 µm fiber at apulse energy of 0.5–1 J and a total power ranging from 15–30 W. Operative time was calculated in minutes from the time of introduction of laser scope till the removal of the scope. The bladder was filled at the end of the procedure and the patient was encouraged to void. No indwelling catheter was placed. Patients were allowed oral intake immediately in the postoperative period and encouraged normal voiding. Patients were discharged after an average of 6 h of hospital stay.

Armamentarium used for TFL cystolithotrity.
Patients were advised to first follow up after 5 days for a check ultrasound KUB (to confirm complete clearance) and a urine routine examination, and then after 3 months to rule out any sequel of the procedure. Complications were recorded as per Clavien Dindo scale. 17
Results
A total of 47 patients with bladder stones presented during the study reference period. Of these, 30 patients (27 males and 3 females; mean age: 35 ± 10.4 years) who underwent laser lithotripsy (TFL) for bladder calculi were included in this study. The clinical presentation of patients was LUTS (dysuria, hesitancy, and intermittency) in 28 (93%) patients while 2 (7%) patients were asymptomatic (Graph A). Hematuria was observed in 3 (10%) patients while 5 (16%) patients had AUR. The average size of the stone in this series was 15 ± 2.8 mm. The mean duration of laser lithotripsy was 15 ± 5.4 min. Energy to dust stone was variable with a mean LASER energy of 18.23 ± 10 W.
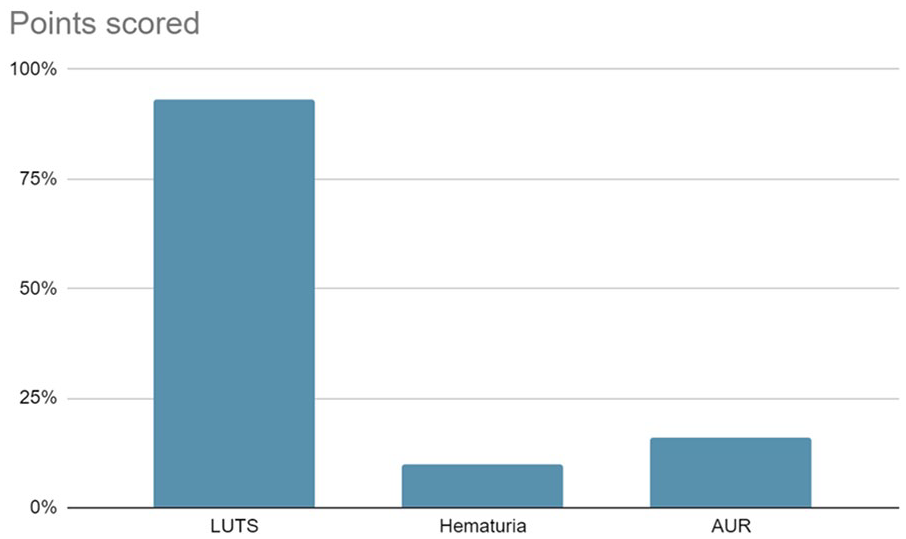
Clinical presentation of patients with bladder stones.
All patients tolerated the procedure well and none required conversion to conventional anesthesia. All patients except one passed urine comfortably in the immediate postoperative period. One patient was catheterized for 24 h and he passed urine after removal of the catheter. All patients were discharged on the same day after the surgery with the advice of first follow-up after 5 days. These patients were discharged on quinolones (ofloxacin 400 mg once a day). 100% clearance rate was documented in all patients. Mild hematuria was noted in five patients and AUR needing catheterization in one patient, which were graded as Grade 1 in Clavien-Dindo Scale. 17 None of our patients had fever in the postoperative period.
Discussion
Management of bladder stones has transformed over the years from open to complete endourology. Open surgery is almost obsolete with the availability of endourology expertise and armamentarium. ESWL is a non-invasive modality to fragment bladder stones, but patients may require intervention in the form of cystoscopy and bladder wash to retrieve the larger fragments. 18 Various other modalities such as transurethral and percutaneous removal of bladder stones have been used depending on the experience, size of the stones, and the type of energy source utilized (electrohydraulic, ultrasonic, pneumatic, or laser energy). 19
Since these procedures were done with the aim of fragmentation and stone retrieval, they often require large caliber endoscopes (25 Fr) which in turn required anesthesia (regional or general anesthesia), prolonged hospitalization, and catheterization. However, the use of lasers has made it possible to fragment the stone into minute dust which can be passed through smaller caliber scopes or spontaneously, thus reducing the need for analgesia/anesthesia.
Majority of the contemporary literature regarding the management of bladder stones under regional/general anesthesia is on the use of Ho:YAG or Pneumatic lithoclast. We share our experience of managing bladder stones of up to 20 mm with TFL under local anesthesia as a day-care procedure.
Of late, lasers have become the energy source of choice for intracorporeal lithotripsy, both for upper tract and lower tract stones. Especially, the Thulium Fiber laser is faster (two to four times) and facilitates better dusting vis-a-vis the gold standard Ho:YAG laser. 7 Water ablative effect seen with TFL is not observed with the HO:YAG laser, thus making it the laser of choice for faster stone fragmentation. 20 Moreover, the quality of stone dust attained with the use of TFL is finer in terms of particle size when compared to the Ho:YAG laser regardless of the composition of the stone. 21 Furthermore, the penetration depth of TFL laser is 0.25 mm versus 0.5–1 mm of Ho:YAG, thus reducing the probability of inadvertent mucosal damage. 22
Garg et al. 23 and Karami et al. 24 in their study included 46 and 48 patients, respectively, with an average stone size of 21 mm; the mean operative time was approximately 43 and 35 min, respectively. They performed the procedures under sedoanalgesia. Although the stone size in these studies was comparable to that in our series, the operative time in our series was considerably shorter (15 ± 5 min). This may be attributed to the modality of the fragmentation device. The TFL laser used in our study is faster compared to Ho:YAG laser used in their studies.
Stephen et al. operated 86 patients with an average stone size of 15.04 mm, which is almost similar to the stone size in our study (15 ± 2.8 mm), with a mean operating time of 23.81 min with HO:YAG laser under local anesthesia. The longer operative time in their study may be attributed to the instrument used for stone fragmentation which was 9.5 Fr URS. We used an 18 Fr laser scope which was well tolerated by all our patients. This not only provided a good vision but also facilitated the instant removal of the majority of the stone dust. 25
Several instruments have been used for transurethral cystolithotripsy, ranging from semirigid ureterorenoscope (URS), flexible cystoscope, specialized cystolithotripsy sheaths (25 Fr), laser scopes (19/22 Fr) to even nephroscopes.26,27 The main criteria for the choice of any instrument are that it should be well tolerated in terms of comfort, especially for procedures conducted under local anesthesia, and not cause urethral injury to prevent sequelae like urethral stricture. This is especially true for the management of large bladder stones via the transurethral route. Therefore, keeping these factors in mind, we use an 18 Fr laser sheath with 2.9 Fr telescope which was well tolerated in our series.
Ho:YAG lithotripsy is the present gold standard for stone fragmentation, but with the introduction of TFL laser, things are changing fast. The stones fragmented with the Ho:YAG laser can be retrieved by Ellik evacuator/Toomy glass syringe wash or can pass spontaneously.28,29 But the quality of dust and fragmentation attained with TFL is far minute compared to HO: YAG laser, thus obviating the need for the wash or extraction of the stone. This was our observation as all our patients with stones <20 mm passed the stone dust spontaneously and completely as was evident on the follow-up ultrasound which documented 100% stone clearance.
Further advantage of the use of TFL for bladder stone management is minimal or no vibration or movement of the stone; the stone remains quite stable at the time of dusting, thus facilitating reduced operative time. 7 This may not be the same with the use of other energy sources like pneumatic or HO:YAG which may not keep the stone stable and the stone vibration at the time of fragmentation can cause inadvertent mucosal injury with increased operative time. 30
Regarding the complications, only five patients in our series developed complications (all Clavien Dindo grade I) which included mild postoperative hematuria which subsided spontaneously with hydration. One patient could not void in the postoperative period and required catheterization for 48 hrs. However, the exact cause could not be known in this case. This is similar to the observation in the series reported by Stephen et.al. Although some patients in their series developed fever in the postoperative period, none of the patients in our series had fever. This may be attributed to the preoperative use of additional aminoglycosides in all patients.
We preferred to perform the procedure under local anesthesia as it was well tolerated by our patients; this averted the risk of morbidity/complications associated with the use of regional or general anesthesia. 31 Moreover, the use of local anesthesia also reduces the overall cost of the procedure. We used TFL laser which further facilitated faster dusting of the stone as is evident from the operative time for our case. That would be one of the reasons that none of our patients required conversion to full anesthesia as we could finish the procedure fast.
Conclusion
Using Thulium fiber laser for transurethral cystolithotripsy of bladder stones under local anesthesia is a feasible technique with minimal morbidity and good outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.