
Abstract
Background:
The most prevalent cancer of the urinary system and the fourth most frequent cancer in men is bladder cancer. Up to 45% of non-muscle-invasive bladder cancers (NMIBC), may develop into muscle-invasive disease within 5 years after initial diagnosis, depending on the risk profile. The neutrophil to lymphocyte ratio (NLR), which is an emerging marker of host inflammation and can be easily calculated from routine complete blood counts (CBCs) with differentials, has shown to be an independent prognostic factor for a variety of solid malignancies, including urinary tract cancer. Pyuria is a well-documented prognostic factor in urinary tract carcinomas, according to several research. The relationship between preoperative pyuria and recurrence in patients with NMIBC is unclear, even though some studies found that pyuria was a strong predictor of poor prognosis in patients with NMIBC. Our study’s objective was to compare the prognostic effect of pre-treatment pyuria and NLR on the likelihood of progression and recurrence in individuals with primary NMIBC.
Materials and methodology:
Data obtained from 100 bladder cancer patients who underwent transurethral resection of bladder tumor (TURBT) from June 2021 to January 2023 were evaluated prospectively.
Inclusion criteria:
Age more than 18 years, having tumor size less than 3 × 3 cm, single tumor, no H/O TURBT.
Exclusion criteria:
Age less than 18 years, size more than 3 × 3 cm, multiple tumors, H/O TURBT.
Results:
We demonstrated in the current study that, compared to NLR, preoperative pyuria was more substantially linked with intravesical recurrence, higher T stage and disease progression following TURBT for NMIBC.
Introduction
The most prevalent cancer of the urinary system and the fourth most frequent cancer in men in developed nations is bladder cancer. 1 Approximately 70% of patients have malignancies that are restricted to the epithelium or the subepithelial connective tissue at the time of their initial diagnosis. Endoscopic resection (also known as transurethral resection of the bladder tumors, or TURB) is typically the main treatment for these tumors.2–4 Concerning the care of non-muscle-invasive bladder cancer (NMIBC), up to 45% of tumors may develop into muscle-invasive disease within 5 years after initial diagnosis, depending on the risk profile, with the likelihood of recurrence ranging from 30% to almost 80%. 5 The likelihood of prior recurrence, tumor stage, nuclear grade, number of tumors, size of tumors, and the presence of carcinoma in situ (CIS) have all been described as clinicopathological indicators of recurrence and progression of NMIBC. 5 The neutrophil to lymphocyte ratio (NLR), which is an emerging marker of host inflammation and can be easily calculated from routine complete blood counts (CBCs) with differentials, has also been shown to be an independent prognostic factor for a variety of solid malignancies, including urinary tract cancer.6–8 There are few and retrospective data on the prognostic role of NLR in patients with NMIBC, despite a recent study’s finding that preoperative NLR was linked to advanced pathologic stage at the time of cystectomy, as well as an increased risk for disease recurrence, cancer-specific mortality, and all-cause mortality. 9
Pyuria, which may be easily diagnosed with inexpensive, non-invasive urine testing, is a sign of an inflamed urinary tract. Pyuria is a well-documented prognostic factor in urinary tract carcinomas, according to several research.10–14 The relationship between preoperative pyuria and recurrence in patients with NMIBC is unclear, even though these studies found that pyuria was a strong predictor of poor prognosis in patients with NMIBC. Our study’s objective was to compare the prognostic effect of pyuria and pre-treatment NLR on the likelihood of progression and recurrence in individuals with primary NMIBC.
Materials and methodology
This study was carried out at Department of urology, SMS medical college, Jaipur from June 2021 to January 2023. All participants provided written informed consent before enrollment and the study was conducted in accordance with regulatory standards of Good Clinical Practice and the Declaration of Helsinki (1996). The study was approved by our Institutional Research Ethics Committee.
Data obtained from 100 bladder cancer patients who underwent transurethral resection of bladder tumor (TURB) from June 2021 to January 2023 were evaluated prospectively after institutional internal review board approval was obtained. The diagnosis of bladder cancer was histologically confirmed by TURB in each patient. The clinical T stage of a bladder tumor was determined according to the 2002 Union International Centre of Cancer (UICC) TNM classification of bladder tumors. Tumor size was defined as the maximum tumor dimension estimated at the time of TURB and/or by clinical imaging. Tumors size were below 3 cm taken for inclusion criteria. The number and shape of the tumors were examined in the same manner. Age more than 18 years, having tumor size less than 3 × 3 cm, single tumor, with no previous history of TURB would be included in the study. Any other than inclusion criteria like, age less than 18 years, size more than 3 × 3 cm, multiple tumors, with history of TURB would be excluded from the study. Concomitance of CIS was revealed in the surgical pathology of TURB. According to the pathology reports, patients were grouped as non-muscle invasive bladder cancer (NMIBC) or muscle-invasive bladder cancer (MIBC). Only patients with NMIBC were included in our study. Demographics and laboratory data, including macrohematuria, neutrophil count, lymphocyte count and serum values of neutrophil to lymphocyte ratio (NLR) were obtained from each patient before TURB. The NLR was defined as the absolute neutrophil count divided by the absolute lymphocyte count. Patient demographics, preoperative full blood count, operative details, and standard histologic tumor characteristics were recorded. Exclusion criteria for the present study were previous operation due to bladder tumor, ongoing treatment for bladder cancer, hematologic disorders or history of conditions that may have influenced blood cell lines such as connective tissue disease, presence of an active infection and/or immunodeficiency virus infection at the time of surgical intervention, prior or concomitant intra-vesical therapy with Bacille Calmette–Guerin(BCG), prior blood transfusion, and the presence of other cancer types or prior chemotherapy. Patients with non-urothelial cancer or for primary prostatic urothelial carcinoma were also excluded in order to maintain a homogenous cohort.
A second TURB was routinely performed in patients who had a T1 or high-grade tumor on initial TURB. Patients received post-operative intravesical instillations based on tumor characteristics, and at the discretion of the treating urologist. Postoperative follow-up consisted of cystoscopy and upper urinary tract imaging performed every 3 months for the first 2 years, every 6 months after surgery, and annually thereafter. Patients with a suspected recurrence underwent TURB. Disease recurrence was defined as the first pathologically confirmed tumor relapse in the bladder, regardless of the tumor stage. Disease progression was defined according to the International Bladder Cancer Group consensus definition for progression in NMIBC, in the presence of an increase in T category from CIS or Ta to T1 (lamina propria invasion), development of ⩾T2 or lymph node (N+) disease or distant metastasis (M1), or an increase in grade from low to high.
Statistical analysis
Factors analyzed were the presence of macrohematuria, preoperative urinary cytology, presence of pyuria, tumor number, tumor size, tumor shape, T category, presence of concomitant CIS and tumor grade. Clinical features between groups were evaluated using Student t-test or chi-square test. The Recurrence Free Survival (RFS) rate was calculated using the Kaplan–Meier survival function, and evaluated using the log–rank test. Univariate and multivariate Cox proportional hazard regression models were used to investigate the associations between various clinicopathological factors and intravesical recurrence. The multivariate Cox analysis was carried out using a forward stepwise variable selection method. All p-values were two-tailed, and p-values <0.05 were considered statistically significant. All analyses were carried out using GraphPad version 3.1.
Result
Between June 2021 and January 2023, 100 patients were recruited to the study. The cohort included 80 men and 20 women with a mean age of 66.19 ± 9.58 and 68.59 ± 10.21 years in NLR and pyuria group respectively, with a confirmed pathological diagnosis of NMIBC. Fifty-seven patients (57%) have had a recurrence during the study, occurring at the median time of 9 months (IQR 4, 14), while the median follow-up time for patients without recurrence was 18 months (IQR 14, 30). The median NLR was 2.69 (IQR 1.9, 4.35). Table 1 shows an analysis of differences in clinical features between groups divided by recurrence. Table 2 shows an analysis of univariate and multivariate differences in clinical features between groups.
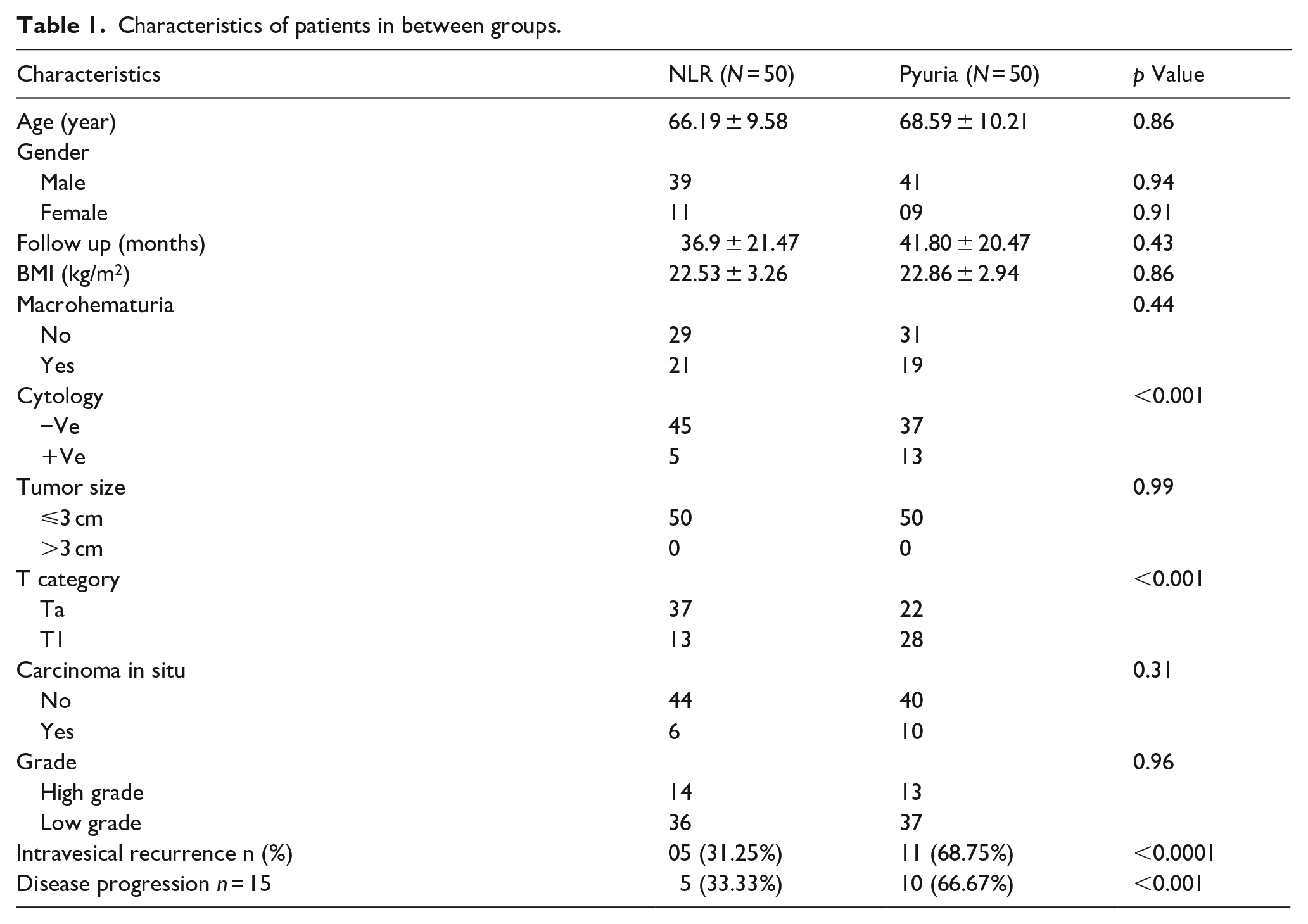
Characteristics of patients in between groups.
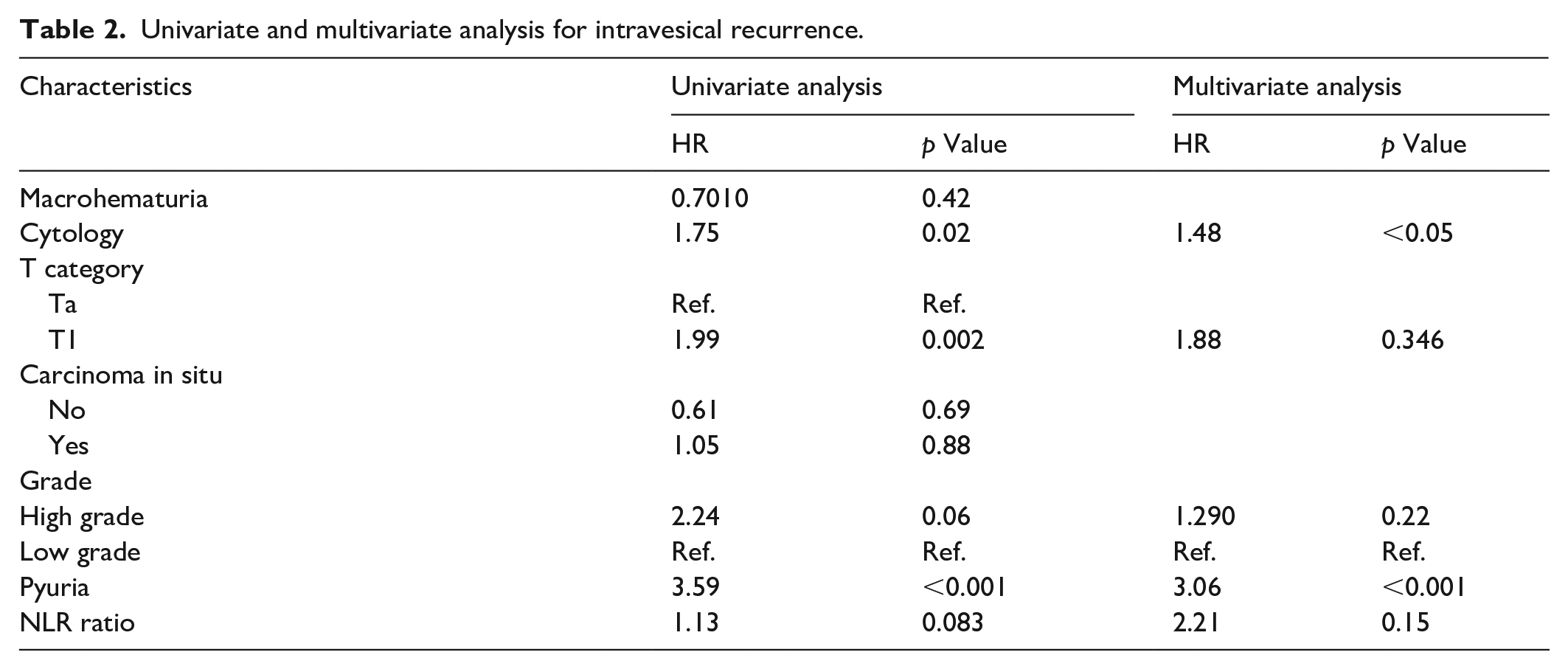
Univariate and multivariate analysis for intravesical recurrence.
Out of 100 patients, 16 had recurrence of bladder cancer in which 11 (68.75%) patients with pyuria and in 11 (31.25%) patients with NLR > 2.5, showing a significant statistical difference (p < 0.001). Pyuria was significantly associated with advanced age, positive cytology, T1 tumors and higher-grade tumors (Figure 1).
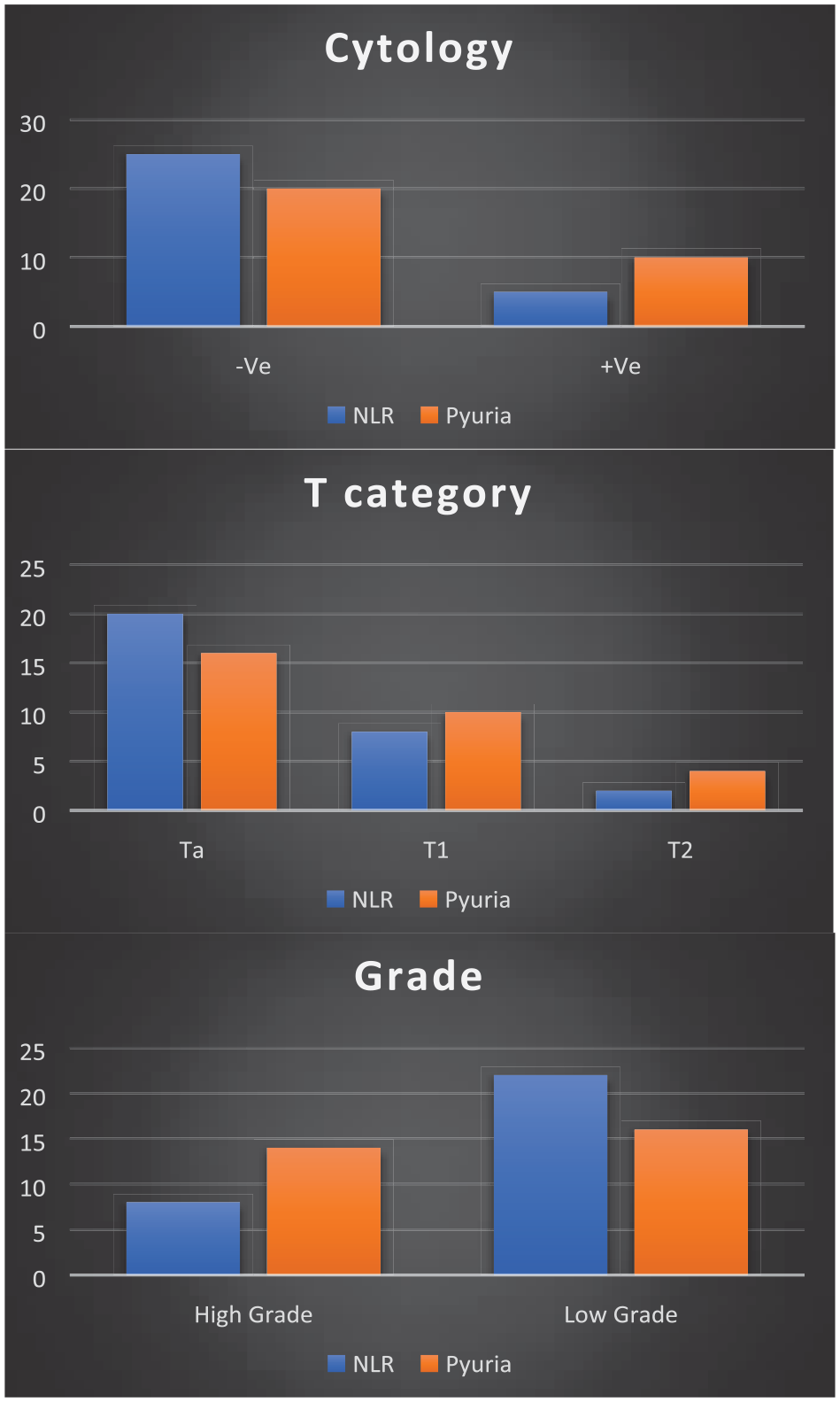
Tumor characteristics.
In univariate analysis, preoperative pyuria, positive urine cytology, pathological T category were found to be significantly associated with recurrence compared to NLR. Multivariate analysis showed that preoperative pyuria, positive urine cytology were independent predictors of recurrence (Table 2). RFS curves by pyuria Vs NLR are shown in Figure 2. The 1-year and 2-year RFS rates in patients with pyuria were significantly lower than those in patients with high NLR (p < 0.001).
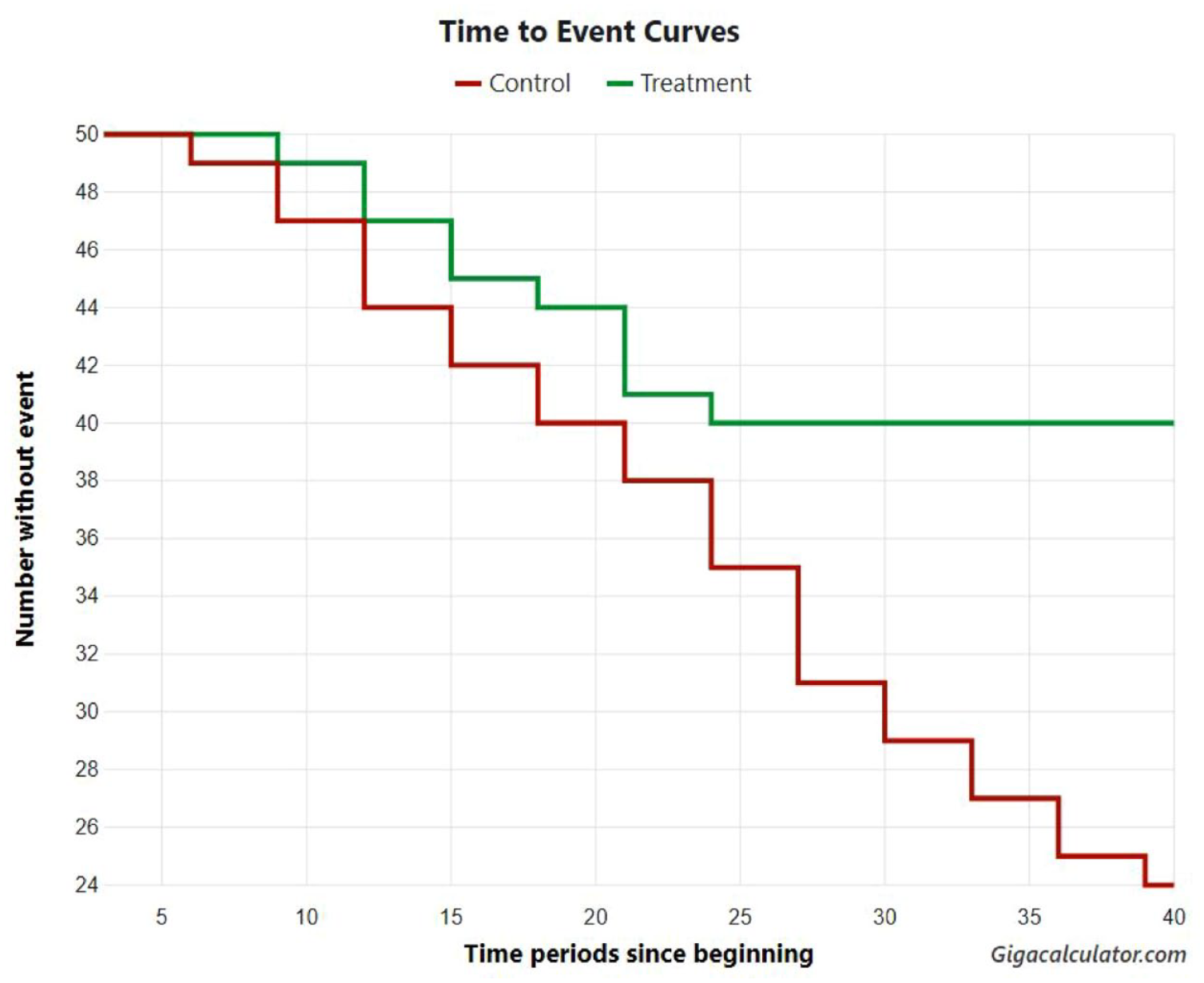
Recurrence free survival duration in Pyuria (Green Line) and NLR (Red line) by using Hazard ration using Long rank test.
Discussion
We demonstrated in the current study that, compared to NLR, preoperative pyuria was more substantially linked with intravesical recurrence following TURBT for NMIBC. Positive urine cytology and pyuria were independent predictors of recurrence in individuals with NMIBC in our analysis of the entire group. This outcome is consistent with recent research by Azuma et al. who found that pyuria is a major predictor of recurrence and progression in NMIBC patients. 10
It is still unclear what causes the relationship between preoperative pyuria and intravesical recurrence. Leukocytes have been implicated in numerous studies as being a major contributor to cancer-related inflammation.15–18 Tumor infiltration of monocyte–macrophage and granulocytic myeloid cells, which are a source of several chemokines/cytokines, has also been linked to bladder cancer inflammation and immune dysfunction. 19 Additionally, bladder cancer cells release granulocyte-colony stimulating factor, which has been shown to significantly stimulate the generation of leukocytes in the host, resulting in a leukemoid response. 20 Leukocytes seen in the urine of individuals with NMIBC have, however, raised some questions in the past. Preoperative pyuria was substantially related to positive cytology, T1 tumors, and higher-grade malignancies in the current investigation. Preoperative pyuria was also a reliable predictor of intravesical recurrence, suggesting that it may be a more accurate sign of tumor aggressiveness than NLR. To fully understand the nature of this relationship, more investigation is necessary.
In their multivariable studies, Yoshida et al. 13 likewise found a significant correlation between preoperative pyuria and poor cancer-specific survival (CSS), OS, and recurrence-free survival. The results of the current study are likewise consistent with patients who have pyuria having poor progression-free survival as well as poor recurrence-free survival.
Reactive oxygen species, which are able to cause DNA damage to cells and genetic instability, may be released by neutrophils, and they can also emit a variety of cytokines to regulate and shape tumor growth. The balance between lymphocyte-mediated, anticancer immune response and neutrophil-dependent, tumor-promoting inflammation is reflected by NLR. 21 Recent studies have revealed the predictive significance of NLR in MIBC and NMIBC independently.9,22–25 Numerous investigations have revealed that in a group of MIBC patients, increased NLR was linked to lower cancer-specific survival and Overall Survival (OS). In particular, it has been demonstrated that NLR functions as a standalone predictor of disease progression and recurrence in NMIBC. These results are supported by the Kaplan-Meier analyses they conducted in their research. However, they discovered that preoperative NLR was not a reliable indicator of oncologic outcomes in NMIBC after controlling for confounding factors. 26 In the current investigation, we found that individuals with NMIBC who also had pyuria had a greater recurrence rate than those who did not. There are a number of theories that have been put up regarding the process of NMIBC recurrence, including tumor cell implantation, the development of tiny tumors, and new tumor formation. 27 However, it is still challenging to determine if pyuria speeds up carcinogenesis or proliferation. Pyuria and MIBC progression were also connected, a result that may be explained by an increase in cell invasion brought on by inflammation. 27 Thus, pyuria and inflammation may have an impact on different stages of the development of bladder cancer.
Our study’s nonrandomized design, which adds biases, is one of its limitations. Additionally, because this is a single-institution research, external validation is necessary. All patients were freshly diagnosed and only had TURBT, therefore we believe this impact to be a minimum for recurrence analysis. However, because patients get various therapies after recurrence, these variables may significantly impact the time to progression study. Our data set lacked information on intravesical treatment, such as the number of cycles and maintenance therapy plans. Some of the treatment plans might not be in accordance with the current standard of care. It is necessary to do more research to confirm these findings and account for subsequent therapies.
Footnotes
Acknowledgements
We would like to express our special thanks of gratitude to our patients and staff in Urology Department, SMS Medical College, Jaipur.
Author contributions
Dr Rahul Singh – Conception, Design, Materials, Data collection and processing, Analysis and Interpretation, Writing. Dr. Govind Sharma – Materials, Data collection and processing, Analysis and Interpretation, Writing, Literature Review. Dr. Shivam Priyadarshi – Design, Supervision, Analysis and Interpretation, Writing, Critical Review. Dr Gaurav Fauzdar – Materials, Data collection and processing, Analysis and Interpretation, Writing, Literature Review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics committee approval
Approved by Institutional Ethics Committee.
• Approval number – sms/134/MC/EC/2021
• Date – 01/02/2022
Patient consent
Obtained.