
Abstract
Background:
In addition to ensuring cancer control, prevention of incontinence which significantly impact patients’ quality of life, is also an important issue in robot-assisted radical prostatectomy (RARP) operations. In this study, we aimed to find the correlation of urinary continence recovery with various factors after Robot assisted radical prostatectomy.
Methods:
This study included 162 patients treated with RARP with perioperative data and at least 1 year of follow-up. Also, the preoperative, intraoperative, and postoperative parameters of the patients were analyzed. The continence recovery rate in our study was assessed at 6th week, 3rd month, 6th month, 9th month, and 12th month, post-surgery. Logistic regression analysis evaluated the association between the predictive factors and urinary continence recovery in the early and late stages.
Results:
The majority of patients with prostate cancer present in sixth decade of life. The majority of our patients (56.7%) were categorized as high risk using D’Amico classification. The continence rate in our study at 6th week, 3rd month, 6th month, 9th month, and 12th month were 40.1%, 72.2%, 85.2%, 89.5%, and 91.4%, respectively. No improvement in continence status was observed after 1 year in our study. There was significant correlation of age with continence status at 6th week, 3rd month, and 6th month. The young age is associated with early recovery of continence. At 3 and 9 months, the non-diabetics cases achieved significantly higher continence rates than diabetics (p < 0.05) which shows that diabetes causes delay in attainment of continence.
Conclusion:
The young age may be associated with early recovery of continence, but further validation requires large number of cases. We attributed good continence recovery rate to meticulous dissection and preservation of good urethral length.
Introduction
Prostate cancer (PCa) is often diagnosed in middle aged or elderly men, and in addition to providing long-term cancer control, preserving patients’ quality of life is also an important goal. Prostate cancer has an age-standardized incidence rate of 64 per 100,000 in Europe and is responsible of 11.3 death per 100,000. 1 The Indian Council of Medical Research reported an incidence rate of 9–10/100,000 population, higher compared to other countries in Asia/Africa, but lower when compared to the United States (US)/Europe. 2
Beside achieving adequate oncological outcomes, ensuring suitable functional outcomes, thus the preservation of urinary continence, is a main goal after radical prostatectomy (RP). Postoperative incontinence still continues to be one of the most defacing side-effects, affecting about 9.0%–16.0% of all patients after RP.3,4 The level of postoperative incontinence has an immense influence on patient’s quality of life. For instance, people suffering from incontinence are more often afflicted with depression or sexual dysfunction. 5
The causes of urinary incontinence after radical prostatectomy are likely multi-factorial and include both functional and anatomical changes related to removal of the prostate gland and alterations in the pelvic floor musculature and the urinary sphincter complex.6,7 The most widely reported risk factors that predict continence recovery after robotic-assisted radical prostatectomy (RARP) include age, body mass index (BMI), severity of lower urinary tract symptoms (LUTS), preoperative comorbidities, preoperative continence, prostate volume, urethral length, and surgeon experience. 8 RARPs have comparable functional outcomes to the traditional open approach with a number of advances in surgical techniques to improve continence. 9 The use of robotic surgery in radical prostatectomy has provided better visualization of apical dissection and external sphincter. In addition, surgical techniques, like nerve-sparing and Retzius-sparing surgery, anterior and posterior reconstruction, and bladder neck preservation approaches, have improved particularly early urinary continence. 10
There is a lack of studies that examine the correlation between factors that contribute to continence recovery in patients undergoing robot-assisted radical prostatectomy (RARP). Currently, there are no known studies on this topic specifically within the Indian context. We hypothesized that the more adverse risk factors for incontinence the patient has before RARP, the more likely he will remain incontinent. The purpose of this article was to find out the correlation of urinary incontinence with various factors after Robot assisted radical prostatectomy in Indian setup.
Methods
This observational study included 162 cases with carcinoma prostate who underwent RARP prospectively. This study was conducted in accordance with the hospital ethical committee requirements at Department of Urology at two tertiary care hospitals in north India. All surgeries were performed by experienced robotic surgeons.
All patients with carcinoma prostate who underwent RARP at our institute with 1 year of minimum follow-up were included in our study. Patients who have died of unrelated causes in follow-up and patients those who were lost to follow-up were excluded from the study.
The data on prospective cases have been collected from follow-up, whereas the data of retrospective cases has been collected from the Record section of the hospital. These patients were contacted by phone and were asked to come with old records and the deficit information was collected.
In our study, confirmed cases of prostate cancer by prostatic needle biopsy who underwent RARP were included. Patients, who were willing for RARP, underwent complete pre-operative work up to assess the patient’s fitness for surgery under general anesthesia.
Urinary continence status was assessed at 6th week, 3rd month, 6th month, and 12th month post-surgery. Correlation of continence recovery was done with various factors such as age, Pre-Operative prostate-specific antigen (PSA), D’ Amico Risk classification, Operative Time, and Post-Operative Gleason Score.
In our study, continence was defined as either no or one pad per day as a precaution only.
Statistical analysis
Descriptive statistics were analyzed with SPSS version 23.0 software. Continuous variables were presented as mean ± SD. Categorical variables were expressed as frequencies and percentages and were associated using Chi-square test or Fisher’s exact test as appropriate. For all statistical tests, a p-value less than 0.05 was taken to indicate a significant difference.
Results
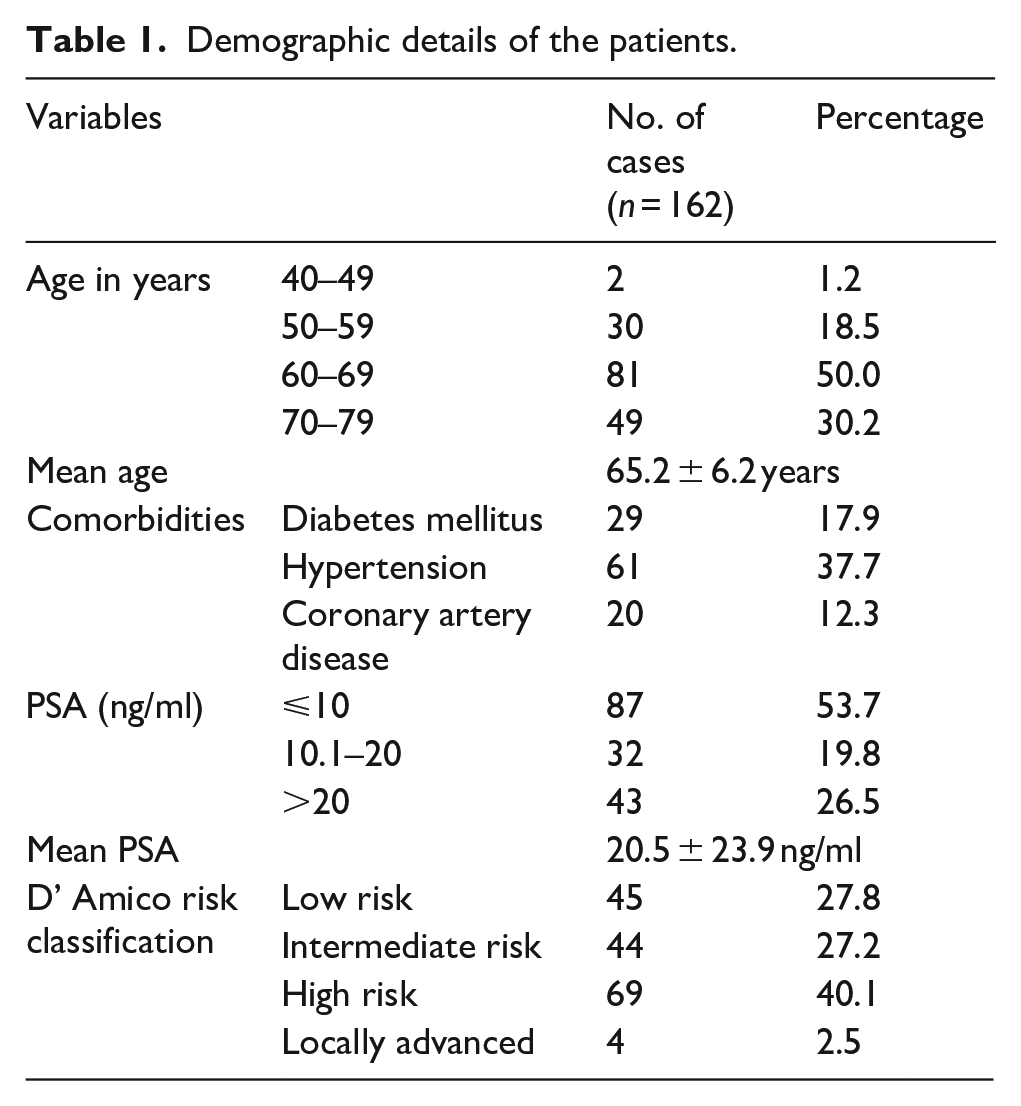
The mean age in our study was 65.2 ± 6.2 years with majority of patients belonging to 60–69 years age group as shown in Table 1. The mean PSA was 20.5 ± 23.9 ng/ml with majority of patients having PSA ⩽ 10 ng/ml and majority of patients were classified as high risk according to D’ Amico risk classification. The mean operative time was 245.4 ± 60.6 min and mean hospital stay for the total studied cases was 4.1 ± 1.9 day whereas mean catheter duration was 13.5 ± 6.9 days.
Demographic details of the patients.
Urinary continence rate
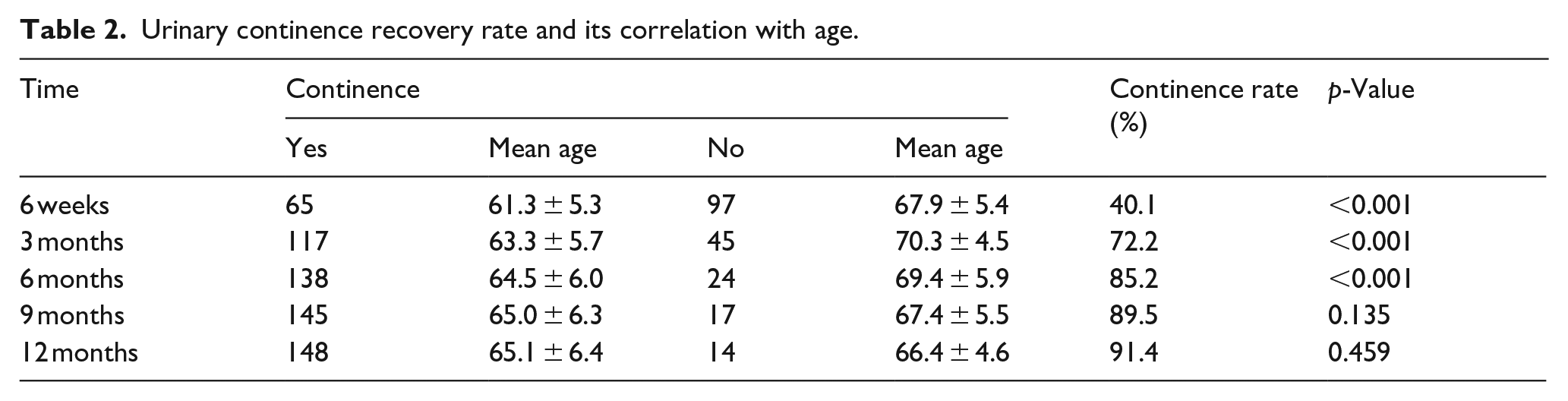
The continence status was assessed post-operatively at 6th week, 3rd month, 6th month, 9th month, and 12th month. The median time to achieve continent status was 3 months. We had observed that there is a substantial improvement of continence with time. The continence rate in our study at 6th week, 3rd month, 6th month, 9th month, and 12th month post RARP, were 40.1%, 72.2%, 85.2%, 89.5%, and 91.4%, respectively as shown in Table 2. No improvement in continence status was observed after 1 year in our study.
Urinary continence recovery rate and its correlation with age.
Correlation of urinary continence rate with age
We observed that young age is associated with early recovery of continence. The mean age of patients continent at 6th week, 3rd month, 6th month, 9th month, and 12th month was 61.3 ± 5.3, 63.3 ± 5.7, 64.5 ± 6.0, 65.0 ± 6.3, and 65.1 ± 6.4 years, respectively. The mean age of patients incontinent at 6th week, 3rd month, 6th month, 9th month, and 12th month was 67.9 ± 5.4, 70.3 ± 4.5, 69.4 ± 5.9, 67.4 ± 5.5, and 66.4 ± 4.6 years, respectively. There was significant correlation of age with continence status at 6th week, 3rd month, and 6th month, but no significant correlation seen at 9th and 12th month as shown in Table 2. Age shows a significant positive correlation with continence time, indicating that older age is associated with longer continence recovery time.
Urinary continence correlation with PSA level
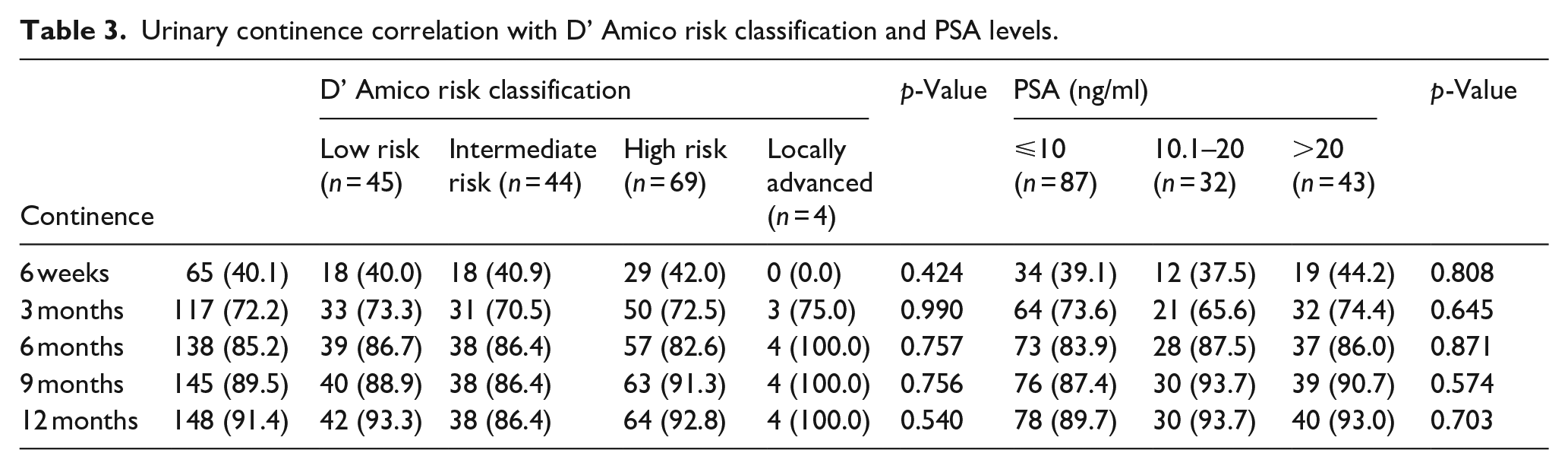
We studied correlation of continence recovery rate with PSA level as shown in Table 3. The continence rate at 6th week, 3rd month, 6th month, 9th month, and 12th month was assessed in various PSA subgroup for example, PSA level ⩽10, 10.1–20, and >20 ng/ml. There was no statistically significant correlation between urinary continence and PSA levels at any time point.
Urinary continence correlation with D’ Amico risk classification and PSA levels.
Urinary continence correlation with D’ Amico risk classification
At 6 weeks post-surgery, there were 65 patients who achieved continence. Among these patients, 18 (40.0%) were classified as low risk, 18 (40.9%) as intermediate risk, and 29 (42.0%) as high risk. There were no patients with locally advanced risk who achieved continence. The p-value of 0.424 suggests that there is no statistically significant correlation between D’Amico risk classification and continence recovery at this time point as shown in Table 3.
At 3, 6, 9, and 12 months post-surgery, the continence rates increased. The proportions of patients achieving continence across different risk classifications were relatively consistent. The p-values for these time points (0.990, 0.757, 0.756, and 0.540, respectively) indicate no statistically significant correlation between D’Amico risk classification and urinary continence at these later time points.
Correlation of urinary continence with diabetes, coronary artery disease (CAD), and hypertension
In our study, 17.9% were having diabetes mellitus, 37.7% were having hypertension, and 12.3% were having coronary artery disease. The diabetes mellitus shows the positive but insignificant association with continence recovery time according to our findings as shown in Table 4.
Correlation of continence recovery with diabetes, CAD, and hypertension.
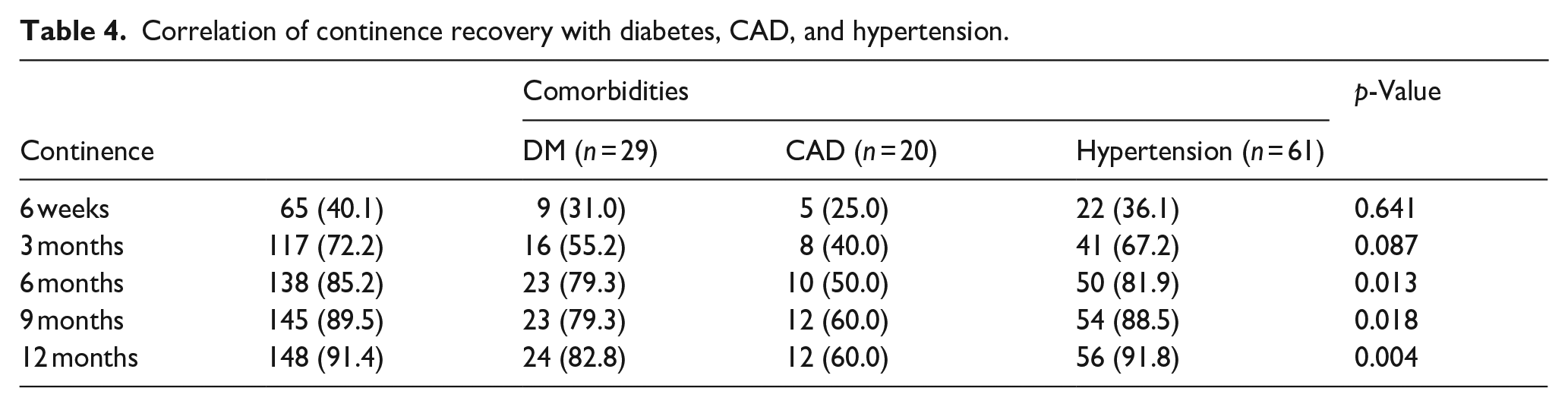
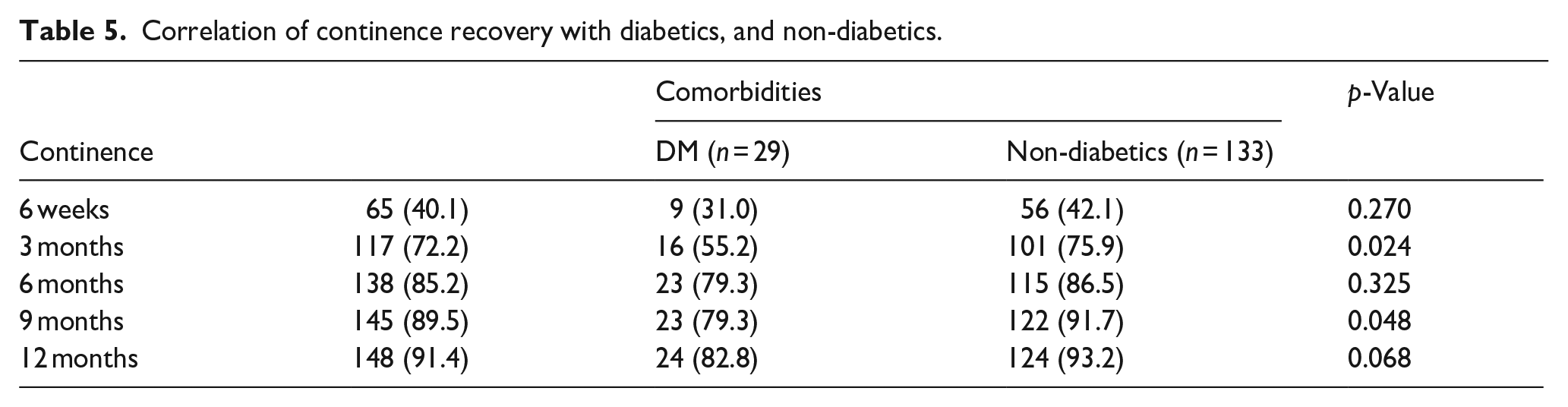
Table 5 depicts that at 3 and 9 months, the non-diabetics cases achieved significantly higher continence rates than cases with diabetes (p < 0.05) which shows that diabetes causes delay in attainment of continence.
Correlation of continence recovery with diabetics, and non-diabetics.
Correlation of urinary continence recovery with post-operative Gleason score
We correlated urinary continence with post-operative GS, but there was no statistically significant correlation between urinary continence and postoperative Gleason Score at any time points. The p-values for these time points were 0.649, 0.447, 0.429, 0.425, and 0.304 respectively as shown in Table 6.
Correlation of continence recovery with post-operative TNM staging and Gleason score.
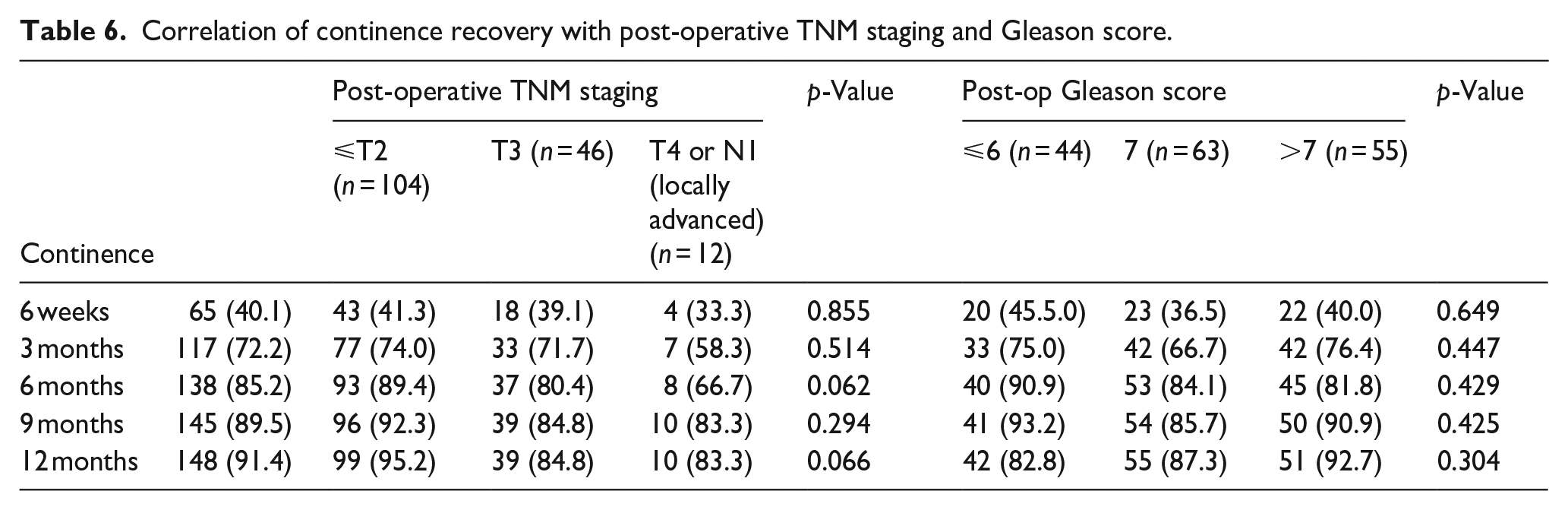
Correlation of urinary continence with post-operative TNM staging
There was no statistically significant correlation between urinary continence and postoperative TNM stages at any time points as shown in Table 6. The p-values for these time points were 0.855, 0.514, 0.062, 0.294, and 0.066 respectively.
Discussion
Radical prostatectomy disrupts the inherent anatomy of the male pelvis and the functional mechanisms of urinary continence, directly affecting the voiding dynamics. These alterations mainly result in urinary symptoms, especially stress incontinence. The etio-pathology of urinary incontinence after RP is found to be complex and multifactorial. It depends on multiple factors like surgical technique, surgeon’s skill, and patient characteristics such as increasing age, prostate volume, BMI, and preoperative LUTS.
In our study, we studied urinary continence rate and its correlation with various factor in Indian set-up.
In our study, the continence rate at 6th week, 3rd month, 6th month, 9th month, and 12th month were 40.1%, 72.2%, 85.2%, 89.5%, and 91.4%, respectively. There was significant correlation of age with continence status at 6th week, 3rd month, and 6th month, but no significant correlation seen at 9th and 12th month. The young age was associated with early recovery of continence. Various studies in past also reported that younger patients tended to have higher rates of early continence recovery after radical prostatectomy. Catalona et al. 11 examined the influence of age on return of continence in 1325 men after 18 months of RRP and found that men younger than 70 had continence rates of 92%–97%, while men in their 70s had a significantly lower continence rate of 87.0%. Kim et al. 12 reported that younger patients tended to have higher rates of early continence recovery. Gupta et al. 13 also noted early continence recovery in younger patients after RARP. Novara et al. 14 found that younger age was an independent predictor of continence at 12 months. The younger patients are having strong pelvic floor muscles in comparison to older counterparts. Therefore, with an adequate pelvic floor muscle training, these muscles help protect against development of the incontinence after surgery and also lead to early recovery of urinary continence than the older patients. Also, the younger patients are healthier with higher level of albumin leading to better healing and early recovery. These factors could explain why the younger patients recover faster from the post-operative incontinence.
The comorbidities (DM and hypertension) were affecting the continence significantly at 6, 9, and 12 months after RARP in our study (p < 0.05). Our findings were supported by Cakmak et al. 15 who in their study reported that diabetes seems to be a significant disadvantage in gaining urinary continence compared with nondiabetic patients particularly in the first 18 months after RARP. Diabetic patients should be informed about possible late recovery of postoperative urinary continence compared with nondiabetic patients after RARP. It is known that presence of older age and diabetes might have a negative impact on recovery and healing process following tissue damage and surgery. Since DM is strongly associated with conditions that attenuate tissue repair and healing process, such as microvascular circulation disorder or neuropathy, it is very likely that differences in short-term urinary continence rates are attributable to a delayed recovery and healing process in DM patients. 16 Additionally, it is plausible that the sphincteric system of DM patients is already preoperative exposed to microcirculation disorders and to diabetic neuropathy, which furthermore might attribute to lower rates of urinary continence at short-term follow up. In line with our findings, Teber et al. 17 reported similar findings in regards to short-term urinary continence.
According to Holze et al. 18 TNM stage and PSA pre surgery, additional therapy, pelvic lymph node dissectionare not predictive for continence. Kim et al. 19 reported an overall continence rate of 79.9% 3 months after RARP. Age <70 years, a higher preoperative Sexual Health Inventory for Men (SHIM) score, a lower clinical T1 stage, a lower biopsy and pathologic Gleason score, a shorter operative time, a lower estimated blood loss, and a smaller prostate volume (40 cc) were associated with recovery of urinary continence within 3 months after RARP (p = 0.05). In multivariate logistic regression analysis, younger age, a higher SHIM score, a lower clinical T1 stage, a lower body mass index (BMI), and a smaller prostate volume were predictors of continence return within 3 months after RARP (p = 0.05). Clinical T1 stage permits for simple dissection, improved surgical resection, and ample urethral length preservation. In addition, they discovered that preoperative AUA symptom score, surgical margin status, pathologic stage, and nerve sparing were unrelated to early incontinence recovery.
Conclusion
The young age may be associated with early recovery of continence, but further validation requires large number of cases. We attributed good continence rate to meticulous dissection and preservation of good urethral length. Post RARP continence depends on multiple factors including pre-operative patient and tumor factors and surgical factors. While a number of these factors are non-modifiable, there are a number of surgical techniques, which can improve continence post RARP. Therefore, attention should be focused on developing and utilizing these techniques when performing RARP, especially in men with high risk of developing incontinence. Diabetes seems to be a significant disadvantage in gaining urinary continence compared to non-diabetics after RARP. Diabetic patients must be informed about the possible late recovery of post-operative urinary continence than non-diabetics following RARP procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.