
Abstract
Objectives:
To verify if the maximum thickness of the ureteral wall at the stone site (m-UWT) can affect the outcomes of primary retrograde ureteroscopic lithotripsy (P-URSL) within a single-center dataset.
Material and methods:
We retrospectively reviewed data on 354 consecutive URSL performed from January 2020 to May 2022 at “Fondazione Poliambulanza” in Brescia (Italy). We included patients older than 18 years who underwent URSL for a single ureteral stone with a maximum diameter ranging from 5 to 10 mm. Patients with anatomical abnormalities, a positive preoperative urinary culture, or without a NCCT performed during the acute event were excluded. Patients were treated in an emergency setting (P-URSL within 48 h from the diagnosis of acute ureteral colic) or in a delayed one (D-URSL after a period of maximum 90 days of ureteral double-j stenting). For the resulting 139 patients we recorded demographic, clinical and stone-related features and perioperative data. We processed these data by univariate and multivariate analysis, and with a logistic regression analysis.
Results:
Of the 139 included procedures, 63 were P-URSL and 76 D-URSL. At the univariate analysis we found that stone diameter (OR 0.845, p = 0.017), stone volume (OR 0.023, p = 0.001), stone density (OR 0.998, p = 0.000) and m-UWT (OR 0.499, p = 0.013) are predictors of P-URSL. Stone density (OR 0.998, p = 0.002) is an independent predictor of P-URSL at the multivariate analysis. At a logistic regression analysis, a distal ureteric position (OR 0.189, p = 0.014), stone diameter (OR 1.289, p = 0.006), and m-UWT (OR 2.297, p = 0.02) were found to be statistically significant predictors of incomplete stone clearance in patients undergoing P-URSL. m-UWT is the only predictor of short-term postoperative adverse events in patients undergoing P-URSL (OR 3.386, p < 0.001). From a descriptive analysis, it emerged that an increased m-UWT (>2 mm) significantly correlates to an endoscopic finding of ureteritis’ signs and to an increase in operative time, hospital stay and post-procedural stenting time. A m-UWT greater than 2 mm also correlates with a lower stone free rate (SFR) and with a significant increase in both short and long-term postoperative complications.
Conclusions:
Our study confirmed a connection between m-UWT and poor endoscopic findings, as well as a direct correlation with the main morphometric parameters of the stone and finally with the outcomes of P-URSL itself. Further studies are necessary to validate our results, so that m-UWT might be routinely considered a useful tool in the decision-making process for P-URSL.
Introduction
The lifetime prevalence of urolithiasis is around 14% and rising. Acute ureteric colic is one of the most common reasons for access to the ER.1,2 Acute uncomplicated ureteric colic may be approached with different strategies, including primary retrograde ureteroscopic lithotripsy (P-URSL). P-URSL is offered based on the stone size and location and in the absence of an underlying infection.3 –10
Recently, many studies have focused on the clinical impact of the maximum thickness of the ureteric wall nearby the stone (m-UWT), easily measurable in the CT scan images11 –15 (Figure 1). None of these studies has ever correlated m-UWT with the outcomes or the possible complications of a P-URSL. Our study aims to verify if the m-UWT may play a role in the decision-making process for P-URSL.
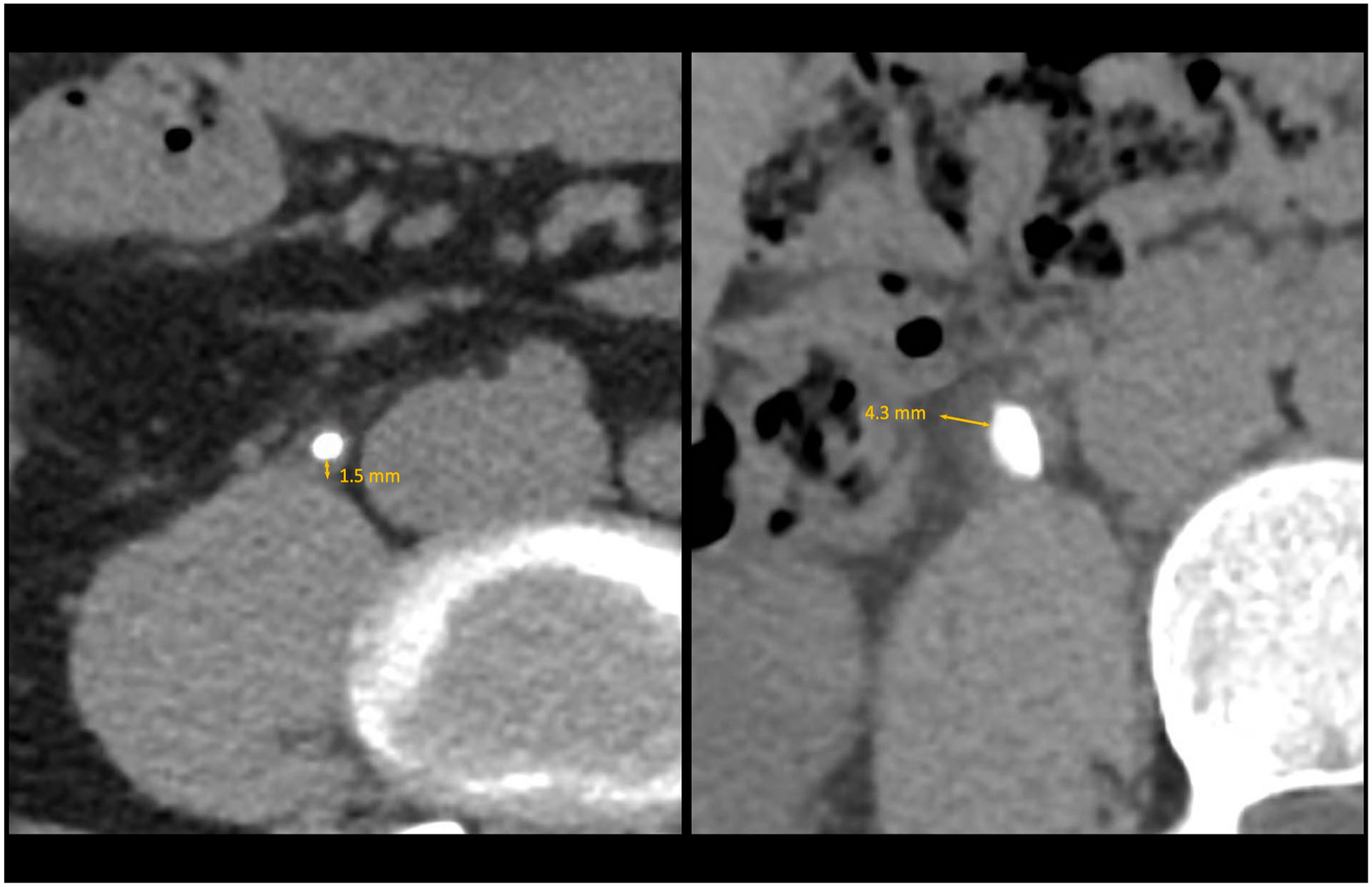
Ureteral wall thickness.
Materials and methods
Study design
After the approval of the local Ethics Committee, we retrospectively reviewed collected data on 354 consecutive URSLs performed between January 2020 and May 2022 at our institution. Patients were treated in an emergency setting (P-URSL within 48 h from the diagnosis of acute ureteral colic) or a delayed one (URSL after a period of a maximum of 90 days of ureteral double-j stenting). Inclusion criteria: ⩾18 years old, URSL for single ureteral stone (maximum diameter ranging from 5 to 10 mm). Exclusion criteria: anatomical abnormalities of the upper urinary tract, a positive preoperative urinary culture or other signs of infectious complications, and NCCT not performed. Of the 354 procedures, 219 were excluded. The remaining 139 URSLs were analyzed in the present study.
All data were collected within an “ad hoc” deidentified dataset which was accessible only to the main investigators and encrypted with a password. Features recorded from all patients included: age, gender, body mass index, smoking history, general and stone-related comorbidities, drug history, previous renal colic or treatments for stones, biochemical evaluation at the time of the colic, morphological characteristics of the stone (maximum diameter, volume, position, side, mean density, core density, m-UWT), perioperative antibiotic prophylaxis, operative data (ureteroscope gage, operative time, endoscopic ureteritis’ signs, intraoperative complications, basket use, ureteral stent type and maintenance time), stone clearance, postoperative course (hospital stay, postoperative complications, biochemical evaluation), long-term complications, and follow-up data.
CT scans were performed using a 64-MDCT (GE Lightspeed VCT 64, General Electric™, Boston, Massachusetts, United States). URSLs were performed by skilled surgeons, with experience in at least 30 similar procedures per year. Endoscopic signs of ureteritis were obtained from the operative report and described as chromatic variations of the ureteral mucosa, edema, polyps, or other typical inflammation features. URSL procedure was performed in standard lithotomy position under general anesthesia with a 4.5 Fr, 6 Fr, or 8 Fr Wolf™ semi-rigid ureteroscope. Stones were fragmented with the help of Jena™ Ho: YAG laser lithotripter (Jena Surgical™ Multipulse Ho, Jena, Germany), with a 200 µm fiber.
All complications were described according to the Clavien-Dindo classification system. We evaluated stone clearance with US/X-ray or NCCT at 3 months. “Stone-free” state was defined as no residual fragment greater than 2 mm. 1 year of follow-up allowed us to evaluate long-term complications, such as iatrogenic ureteral strictures.
Statistical analysis
Statistical analysis was performed following guidelines for reporting statistics in urology 16 and it consisted of two steps. First, a descriptive statistic was performed and the Mann-Whitney U test was used for continuous variables whereas Fisher exact test was used for categorical variables. Second, univariable and multivariable logistic regression models were built to assess the predictors of P-URSL, postoperative complications, and stone incomplete clearance. All the analysis was performed using Stata® 15.0 (StataCorp 2017. Stata Statistical Software: release 15. StataCorp LLC, College Station, TX, USA). Statistical significance was set at p < 0.05. Statistical syntax was: tabstat, ranksum, tabulate-exact, logistic.
Results
The study population was divided into two cohorts based on treatment timing. Of the 139 procedures, 63 (45%) were P-URSL and 76 (55%) were D-URSL. Baseline, clinical and perioperative characteristics are shown in Table 1. We collected all data regarding previous renal colic, urinary tract infections, and endourological treatments; previous endourological maneuvers were analyzed specifying whether the patient had undergone one or more procedures. Hydronephrosis degree was divided into mild to moderate (⩽2) or severe (>2).
Baseline and perioperative features.
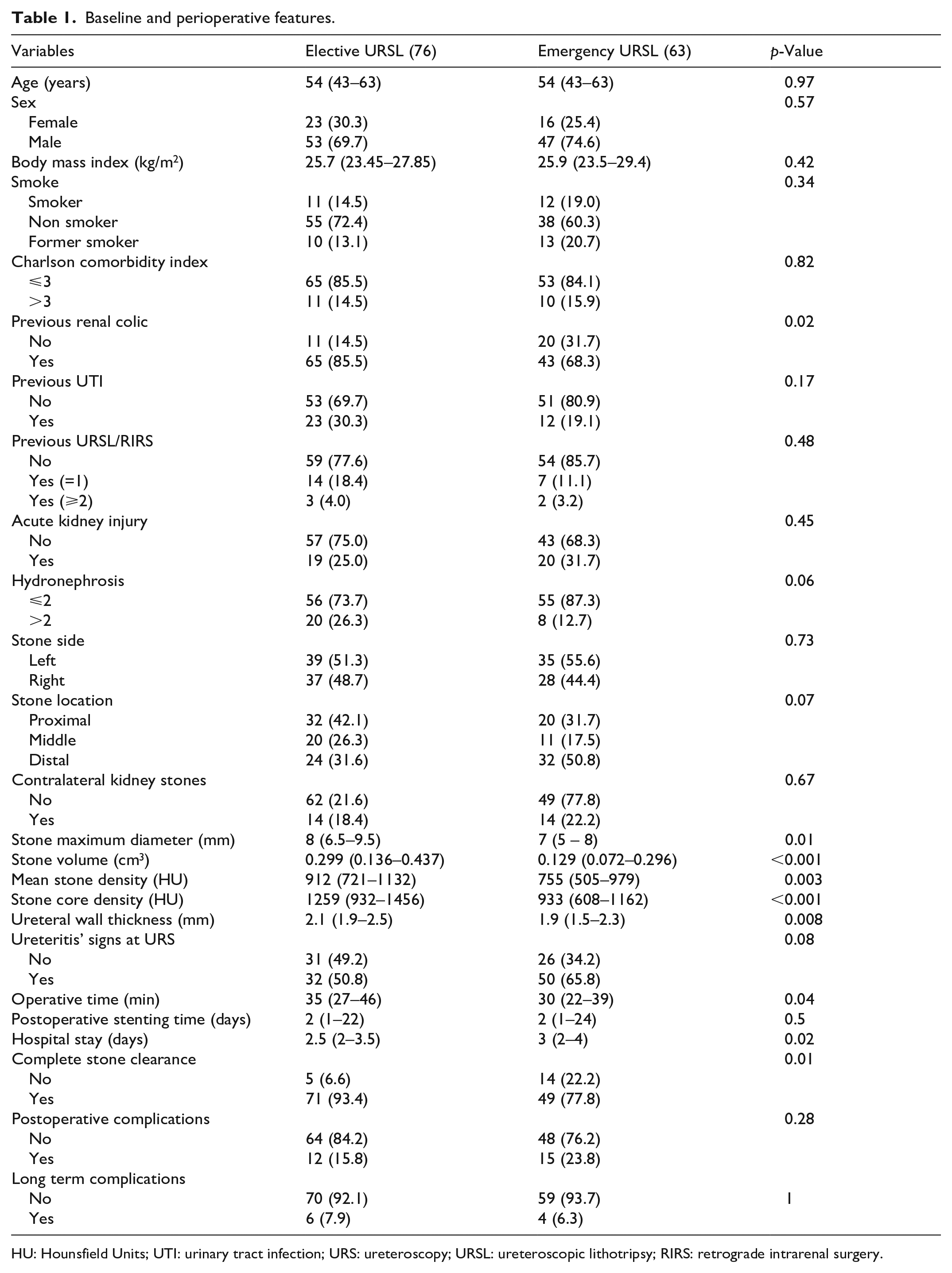
HU: Hounsfield Units; UTI: urinary tract infection; URS: ureteroscopy; URSL: ureteroscopic lithotripsy; RIRS: retrograde intrarenal surgery.
Clinical factors significantly different in these two groups included a history of previous renal colic (p = 0.02), maximum stone diameter (p = 0.01), stone volume (p < 0.001), mean stone density (p = 0.003), stone core density (p < 0.001), and m-UWT (p = 0.008). Perioperative factors significantly different in the two groups included operative times (p = 0.04), hospital stay (p = 0.02), and complete stone clearance (p = 0.01).
Postoperative complications (Supplemental Table 1) were cumulatively counted, without distinction between different types, as no severe event was found (Clavien-Dindo grade >2). Few cases of ureteral substenosis or stenosis were the only long-term complications that occurred, and they were demonstrated at clinical imaging or during subsequent ipsilateral endourological maneuvers.
Using significant factors in the univariate analysis, we then assessed factors associated with impacted stones using multiple logistic regression analysis (Table 2). We found that stone diameter (odds ratio [OR] 0.845, p = 0.017), stone volume (OR 0.023, p = 0.001), stone density (OR 0.998, p = 0.000), and ureteral wall thickness (OR 0.499, p = 0.013) are predictors of P-URSL. Stone density (OR 0.998, p = 0.002) is an independent predictor of P-URSL even in multivariate analysis.
Logistic regression analysis of preoperative factors associated with P-URSL.
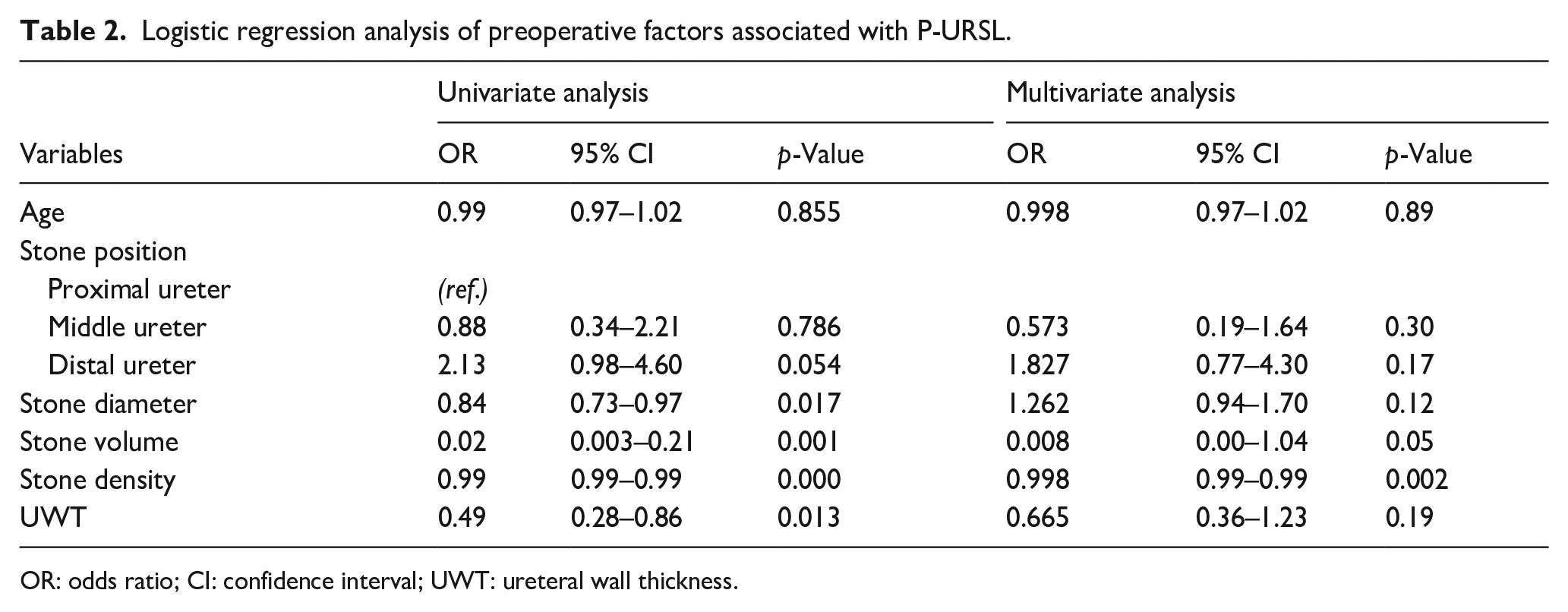
OR: odds ratio; CI: confidence interval; UWT: ureteral wall thickness.
A logistic regression analysis (Table 3) was performed to verify the success rate of lithotripsy, considering the timing of URSL. Stone position in the distal ureter (OR 0.189, p = 0.014), stone diameter (OR 1.289, p = 0.006), and ureteral wall thickness (OR 2.297, p = 0.02) were found to be statistically significant predictors of incomplete stone clearance in patients undergoing P-URSL.
Logistic regression analysis of preoperative factors associated with incomplete stone clearance.
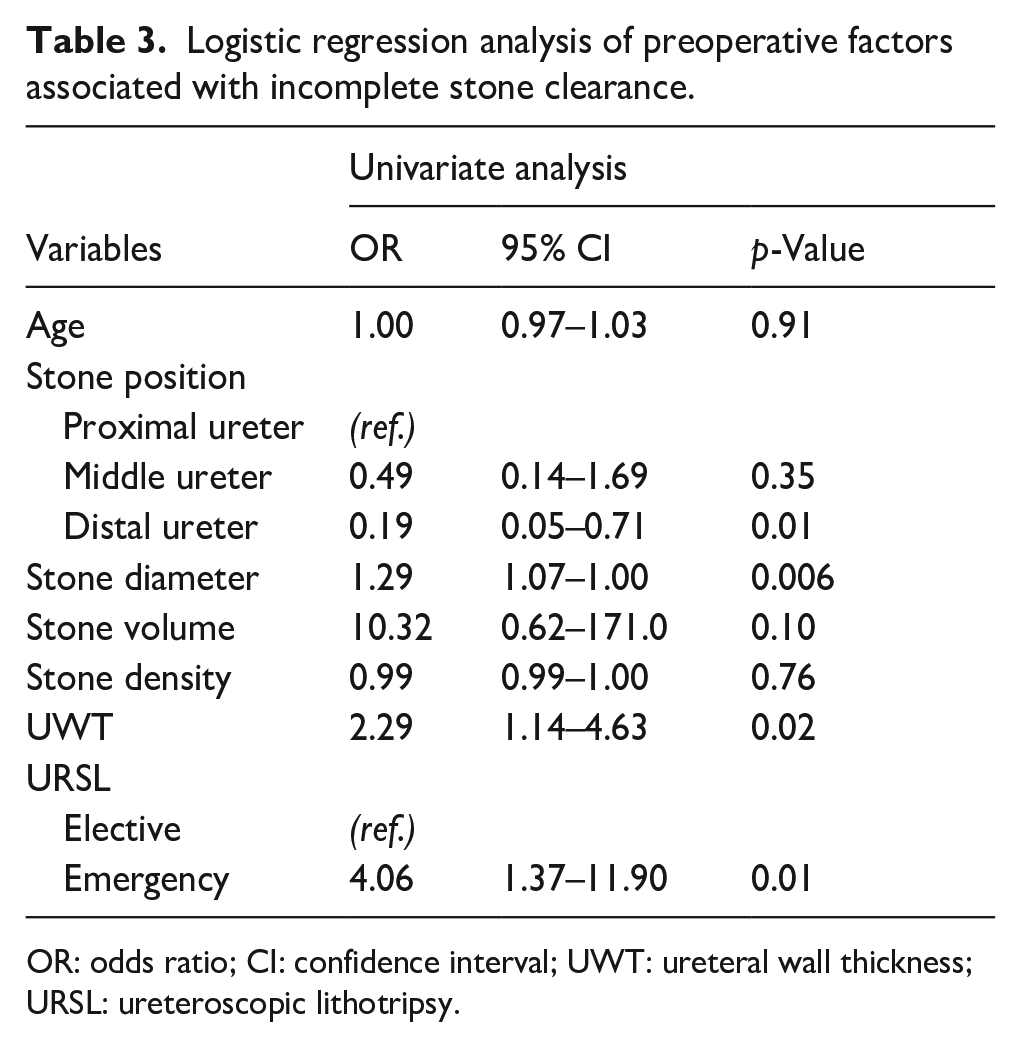
OR: odds ratio; CI: confidence interval; UWT: ureteral wall thickness; URSL: ureteroscopic lithotripsy.
Another logistic regression analysis (Table 4) identified m-UWT as the only predictor of short-term postoperative adverse events in patients undergoing P-URSL (OR 3.386, p < 0.001).
Descriptive analysis of correlations between ureteral wall thickness and clinical and perioperative features.
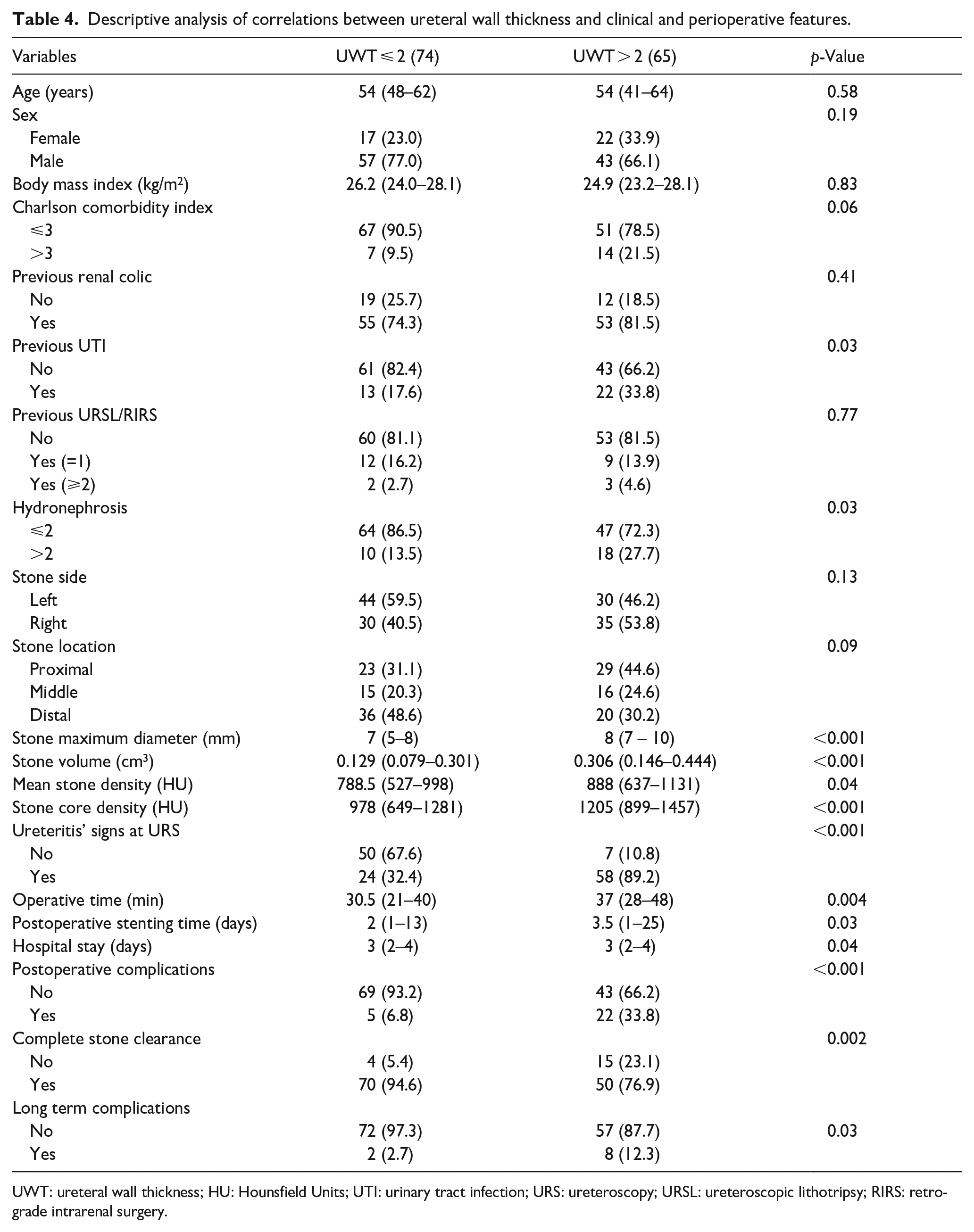
UWT: ureteral wall thickness; HU: Hounsfield Units; UTI: urinary tract infection; URS: ureteroscopy; URSL: ureteroscopic lithotripsy; RIRS: retrograde intrarenal surgery.
To support these results, a descriptive analysis (Table 5) of the correlations between ureteral wall thickness and clinical features was conducted. Patients undergoing URSL were cumulatively analyzed and divided into two groups according to the thickness of the ureteral wall, by using a cut-off of 2 mm.
Logistic regression analysis of preoperative factors associated with postoperative complications.
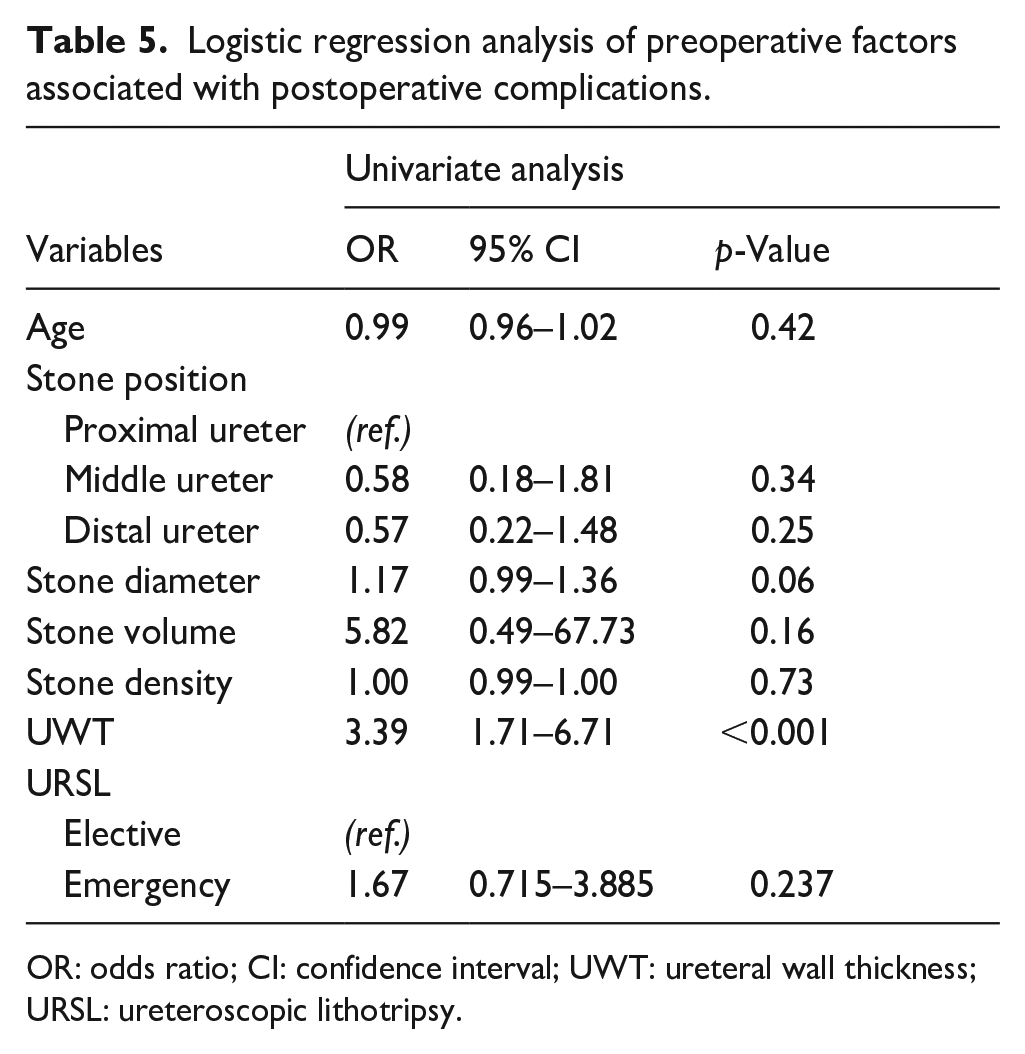
OR: odds ratio; CI: confidence interval; UWT: ureteral wall thickness; URSL: ureteroscopic lithotripsy.
No significant differences were found between the two groups in terms of demographic and clinical features, except for a positive history of UTI, hydronephrosis grading (>2 in case of m-UWT greater than 2 mm), and morphometric characteristics of the stone (larger and harder stones were associated with an m-UWT > 2 mm). From a descriptive analysis of the correlations between m-UWT and operative and postoperative features, it emerged that an increased m-UWT (>2 mm) significantly correlates to an endoscopic finding of ureteritis signs and an increase in operative time, hospital stay, and post-procedural stenting time. An m-UWT greater than 2 mm also correlates with a lower SFR and a significant increase in both short and long-term postoperative complications.
Discussion
In the present study, we found that m-UWT at the stone site was a statistically significant predictor of P-URSL. The logistic regression analysis revealed that m-UWT is predictive for an increased risk of complications and a significant reduction in stone-free rate (SFR) in patients treated in emergency modality. Small stone diameter and distal ureter location are predictors of an increased SFR, but, of note, only ureteral wall thickness was found to be correlated with postoperative complications.
These data allow us to state that ureteral wall thickness may represent a clinical parameter to be considered in the process for P-URSL.
Previous studies investigated the preoperative predictors of clinical outcomes following URSL.17 –20 A nomogram predicting SFR after URSL using a semi-rigid ureteroscope included stone length, number of stones, stone location, and the presence of pyuria, although this study did not include factors based on preoperative NCCT or intraoperative endoscopic findings. 21 Another study showed that secondary signs on NCCT before URSL, including ureteral edema and the rim sign, was not associated with pre- or postoperative SFR. 22 This study, however, did not assess the absolute diameter of secondary signs but evaluated only their presence or absence. An NCCT-based prediction model for SFR of URSL suggested that periureteral edema (almost equal to UWT) was an independent predictor of URSL failure. 23
A normal UWT is approximately 1 mm. Inflammation, interstitial fibrosis, and urothelial hypertrophy associated with stone impaction may cause ureteral edema and polyps and involve surrounding tissues, increasing UWT in the impacted area. Takashi et al. 12 demonstrated that UWT is a reliable predictor of impacted stones, associated with subsequent poorer ureteroscopic findings.
Our study shows that UWT > 2 mm was significantly associated with inflammatory signs at ureteroscopy and a higher hydronephrosis grading. We have also verified that an increased UWT correlates with harder and larger stones, and this data confirms that the periureteral reaction is directly related to stone’s features. For these reasons UWT could be used as an additional morphometric parameter.
Postoperative and long-term complications (ureteral stenosis or sub-stenosis) are significantly more frequent in patients with UWT > 2 mm. The same subgroup of patients underwent significantly longer surgeries: this data makes us reflect on the hypothesis of an association between technical difficulties in performing ureteroscopy in an inflamed ureter and increased operative times, resulting in a greater risk of complications; this finding could explain the higher complication rate in patients with an increased UWT. Mishra et al. 24 have shown similar findings in a 100 cases study correlating m-UWT with elective URSL outcomes.
The present study has several limitations, starting from its retrospective design and its relatively small cohort. Furthermore, we cannot rule out the influence of NCCT slice thickness when measuring UWT. Intra- and interobserver reliabilities of endoscopic findings could not be assessed.
Despite these limitations, our study is the first to show a novel aspect of the use of UWT as a prognostic factor for poor surgical outcomes, thus becoming a helpful tool for the urologist in the decision-making process for the emergency URSL.
Conclusions
In the present study, we found that m-UWT at the stone site was a statistically significant predictor of P-URSL, and it correlates with the outcomes of P-URSL itself. These data could be the first step to consider the m-UWT a morphometric feature helpful for the management of ureteral colic.
Supplemental Material
sj-docx-1-urj-10.1177_03915603231189618 – Supplemental material for Outcomes of primary ureteroscopic lithotripsy: The role of maximum ureteral wall thickness at the site of stone impaction
Supplemental material, sj-docx-1-urj-10.1177_03915603231189618 for Outcomes of primary ureteroscopic lithotripsy: The role of maximum ureteral wall thickness at the site of stone impaction by Tonino Morena, Andrea Vismara Fugini, Alessandro Veccia, Marianna Riva and Angelo Peroni in Urologia Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.