
Abstract
Introduction:
Foreign body insertion associated with sexual gratification is known as polyembolokoilomania. Following removal of the foreign body, long-term complications are infrequently seen. Whilst conservative and endoscopic approaches usually suffice, in extreme cases open surgical approaches are required. We describe an unusual case of polyembolokoilomania in a 25-year-old male involving a single ‘AAA’ battery who developed a urethrocutaneous fistula requiring delayed reconstructive surgery.
Case presentation:
Following an initial successful open extraction of an ‘AAA’ battery from the mid penile urethra the patient developed a delayed urethrocutaenous fistula of the glans. This was managed using a single stage closure with a preputial graft on its vascular pedicle thereby preserving the foreskin and avoiding a buccal graft. No intra-operative or post-operative complications occurred with a catheter left in situ for 2 weeks. Formal histology confirmed a foreign body type reaction. Following outpatient review successful cosmetic, functional, and sexual outcomes were recorded with questionnaires and medical photography.
Conclusion:
Preputial advancement flap with foreskin preservation for distal urethrocutaenous fistula is a successful method of treating delayed urethrocutaenous fistula of the distal urethra in cases of polyembolokoilomania.
Introduction
Foreign body insertion into the urinary tract is well documented with 63% of these cases occurring in adult males between the ages of 18 and 55. 1 The true incidence is unclear and under-reported owing to the sensitive nature and mechanism of the injury. Obtaining an accurate and timely history from these patients can be challenging. Cultural attitudes or embarrassment may delay presentation until the symptoms become intolerable. 2 Intravesical or intraurethral foreign body insertion for the purpose of sexual gratification is known as polyembolokoilomania and is extensively reported in medical literature.3,4
Primary treatment involves careful extraction of the foreign body to avoid erectile dysfunction and other sequalae in male patients. Extreme and rare cases can result in serious injury necessitating emergency reconstructive surgery. 5 Urethral stricture, infection, abscess and persistent lower urinary tract symptoms are well documented complications following insertion and retrieval of a foreign body. 6 The role of the interventional radiologist is increasingly important as their involvement is pivotal in both identifying the foreign body and in removal in select cases. 7
We report an unusual case of polyembolokoilomania in a male patient involving an ‘AAA’ battery which, following successful extraction from the penile urethra via an open approach developed a delayed urethrocutaneous fistula of the glans which was repaired with a preputial advancement flap.
Case presentation
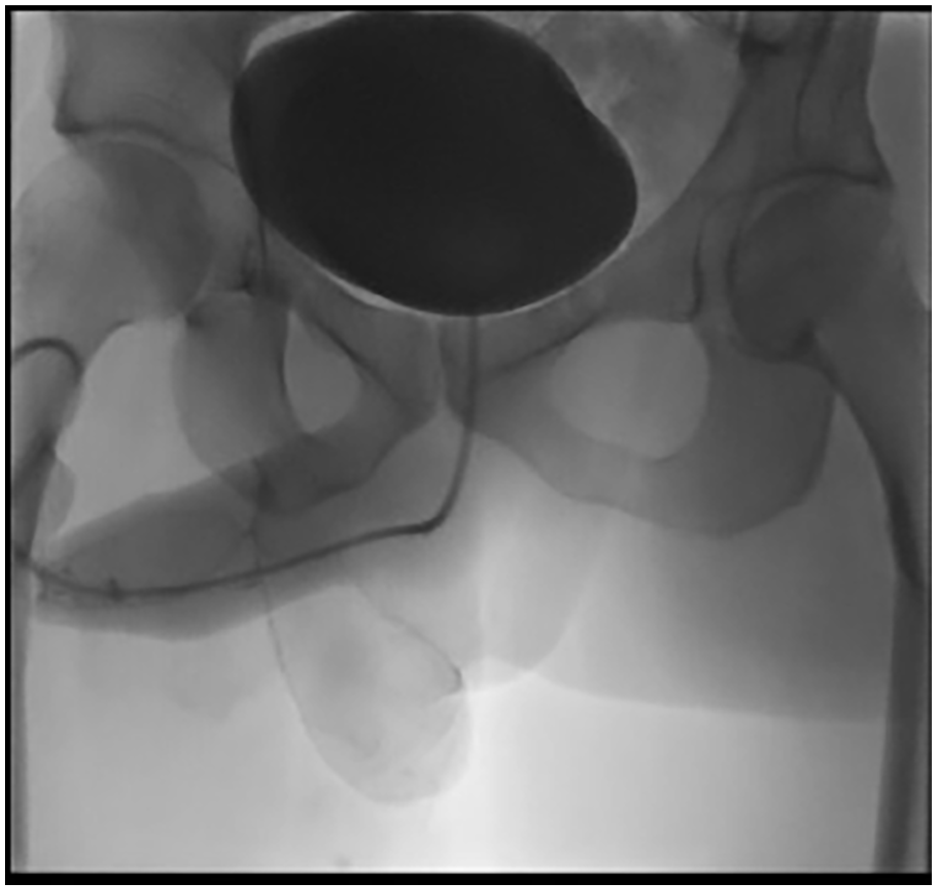
A 25-year-old male presented to the emergency department following 1 h after his female partner inserted a single AAA battery into his urethra during sexual activity. He had attempted unsuccessfully to extract the foreign body prior to presentation by milking the urethra to advance it towards the meatus. His past history was notable for facial plastic surgery following an accident and unmedicated depression. He reported lower abdominal pain, strangury and a slow stream. His observations were stable and he was apyrexial. Physical examination revealed a non-palpable bladder, a retractile foreskin, intact meatus and a palpable foreign body in the mid penile urethra. A plain pelvic radiograph identified the position of a battery in the distal urethra (Figure 1). His baseline International Prostate Symptom Score (IPSS) and International Index of Erectile Function (IIEF-15) scores returned at 3 + 6 and 25 respectively.

A plain X-Ray pelvis demonstrating an ‘AAA’ battery lodged in the urethra.
The patient was taken to theatre for an open extraction of urethral foreign body and flexible cystoscopy under general anaesthetic. Augmentin and gentamicin were given on induction of anaesthesia. Flexible cystoscopy showed a submeatal haematoma and an impacted AAA battery in the distal urethra with significant oedema. An open urethrotomy via a ventral incision was performed. Stay sutures were inserted and the AAA battery extracted. Completion cystoscopy revealed an ischaemic distal urethra around the sub-meatal region but a healthy proximal urethra, posterior urethra and bladder. A 14Ch sialiastic catheter was inserted over a guidewire and a four-layer urethral closure was completed with the catheter taped to the abdomen. After a tetanus injection and a further 24 h of IV Co-amoxiclav, the patient was discharged with a further 3 days of oral co-amoxiclav. The catheter was left in situ for 3 weeks pending a post-op pericatheter urethrogram.
When he presented for his post operative review in the X-ray suite, physical examination revealed a well healed penile shaft wound but a separate, new right sided glans erosion (Figure 2) resembling a distal cutaneous fistula not evident at the time of his first operation. A peri-catheter urethrogram was unremarkable and he voided to completion (Figure 3). It was postulated that the submerged battery had caused a delayed chemical necrosis of the glans which presented as a urethrocutaneous fistula.

Distal urethrocutaneous fistula at the level of the glans 3 weeks post operatively.
Post operative urethrogram showing normal bladder outline with no extravasation of urine 3 weeks post open extraction of AAA battery.
After 2 months following initial presentation and open extraction of an impacted penile urethral AAA battery, the patient underwent closure of a distal urethral fistula with a preputial advancement flap and foreskin preservation. Examination under anaesthetic confirmed bilateral, communicating glans fistulae either side of the frenulum. Flexible cystoscopy revealed a normal penile, bulbar and posterior urethra with no strictures noted. The frenulum and glans were divided and stay sutures inserted. The urethral meatus was calibrated with 18Ch soft tip dilator (Figure 4(a)). A tourniquet was applied for the duration of the procedure (1 h 18 min). There was visible necrosis of the glans plate but the distal urethra remained intact (Figure 4(b)).
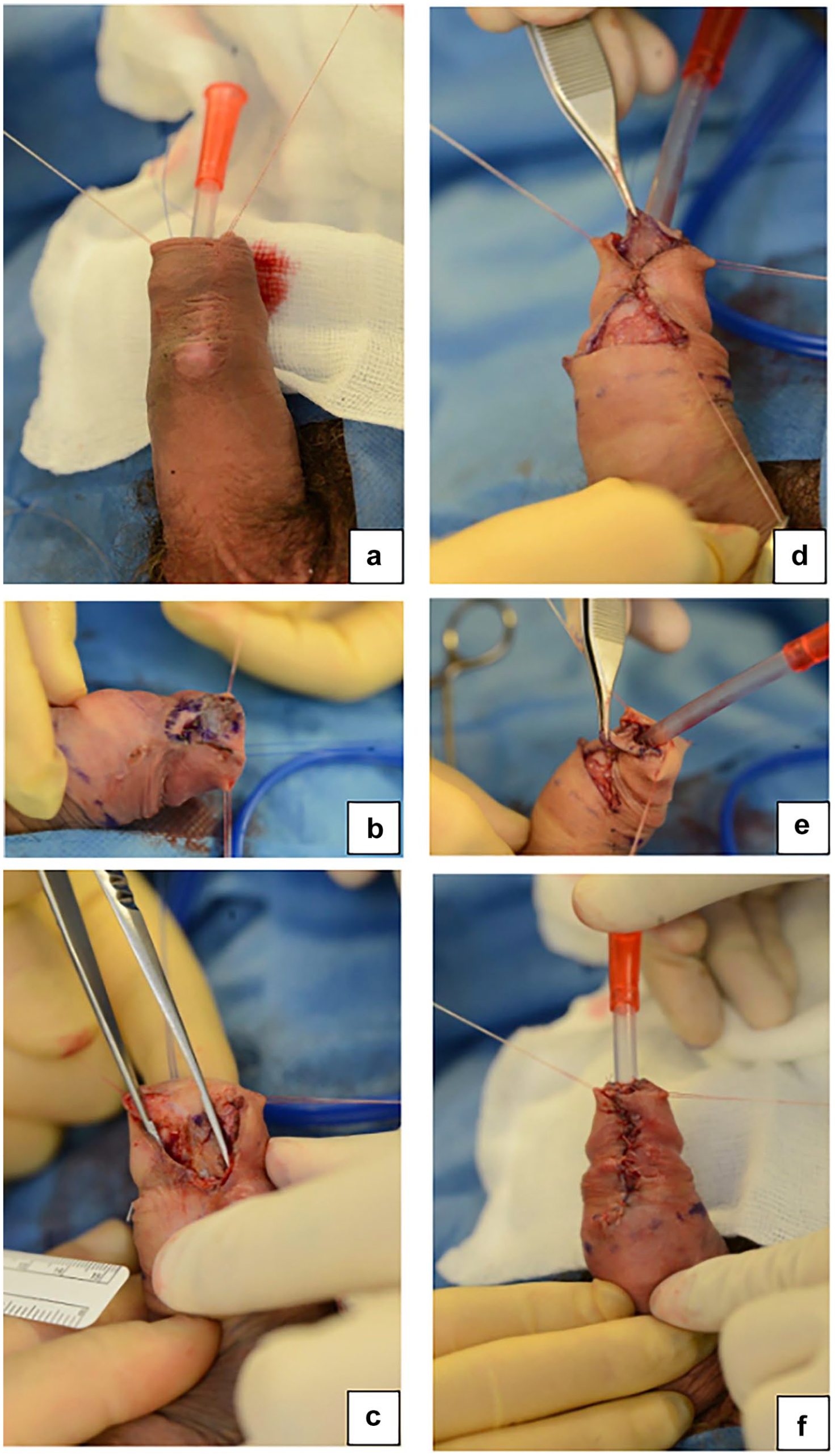
Surgical technique: (a) urethral meatus calibration with a soft tip catheter, (b) necrosis of distal glans plate, (c) 1 cm × 1.5 cm defect, (d) advancement of preputial graft, (e) Glansplasty, and (f) closure of preputial bed graft.
A 1 cm × 1.5 cm defect (Figure 4(c)) was closed using a preputial graft on a vascular pedicle which was mobilised, advanced and tacked onto the ventral surface of the existing urethral plate using 5/0 vicryl interrupted sutures (Figure 4(d)). The meatus was refashioned and trimmed. A glansplasty (Figure 4(e)) was then performed following which a 16Ch catheter was inserted and the preputial bed graft closed (Figure 4(f)). A local anaesthetic penile block with levobupivacaine was given at the end of the operation. The patient was discharged after 24 h with 3 days of oral antimicrobials.
The patient was seen in clinic 2 weeks later for review, catheter removal and repeat medical photography (Figure 5(a) and (b)). Formal histology of the glans fistula confirmed extensive haemosiderin deposition and dermal fibrosis with a foreign body-type reaction but no features of dysplasia or malignancy.
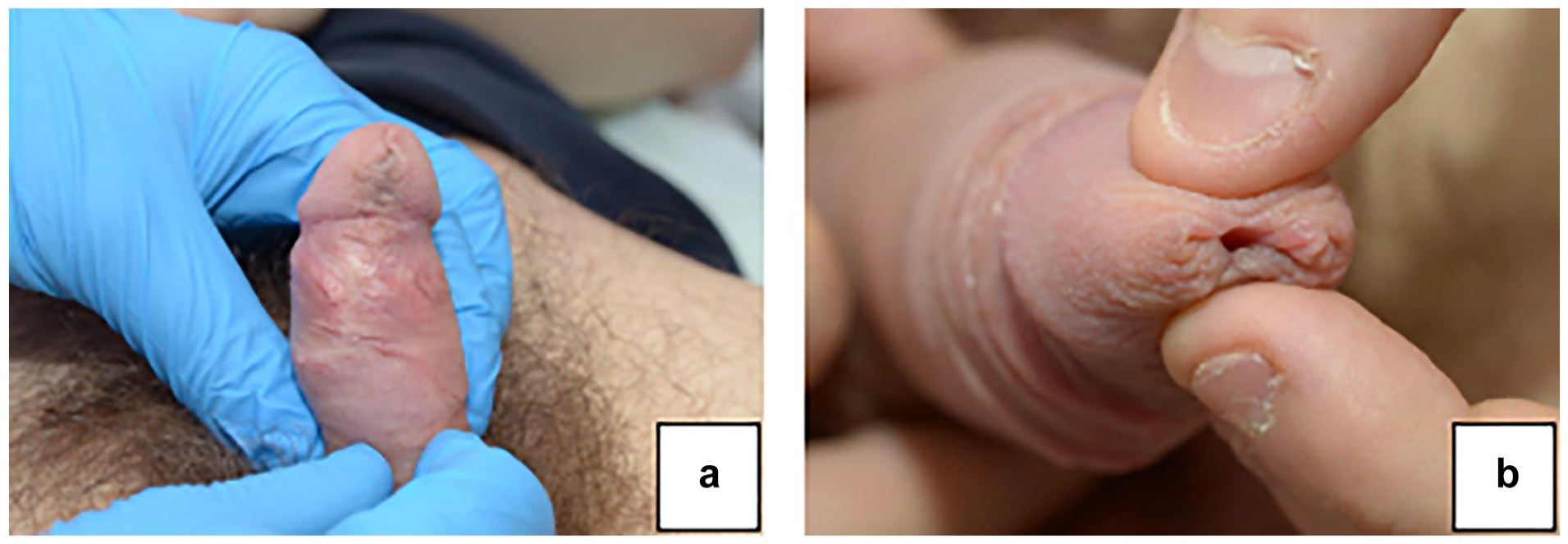
Medical photography taken at 8 months post operatively: (a) retracted preserved foreskin and (b) normal meatus.
At 8 months post operatively he reported satisfactory cosmesis and denied voiding symptoms as evident by an IPSS score of 1+0 and a Peelings voiding picture of 1. His IIEF-5 score remain unchanged at 25 although he had not resumed penetrative intercourse.
Conclusion
Multiple case reports exist of polyembokoilomania with pencils, nail scissors, barbed wires, open safety pins, speaker wire, cables, screws and nuts all found within the urogenital tract.8,9 One study found autoeroticism and self-therapy as the main reasons for auto-insertion. 10 Numerous studies have also reported an overt psychiatric component and intoxication as other causes of foreign body placement. 11 In more extreme cases, Klingsor syndrome, also known as self-inflicted traumatic penile amputation can result from hallucinations, paranoia and religious pre-occupations. 12
Urethral polyembolokoilomania is predominantly recognised in men although cases in women and children have been documented. In males, the foreign body is often retained in the urethra owing to its length and winding course. In women, the inserted body often passes the short distance into the urinary bladder. The diagnosis of urethral polyembolokoilomania is often challenging owing to the stigma associated with this behaviour. Patients may present with symptoms of cystitis, haematuria, poor flow or urinary retention. 11 Rarely, reports exist of complete urethral avulsion following urethral foreign body insertion necessitating emergency urethroplasty. 5 Specific to our case, presentation to the emergency department was prompt however there are reports of delayed presentation of up to 2 years. 8
The effects of batteries are well described within the lining of the oesophagus. 13 Highly corrosive materials are known to have a caustic effect on mucosa through alkaline leakage. Other suggested aetiologies of mucosal damage include direct pressure and completion of an electrical circuit, which produces electrical energy that burns surrounding tissues. 14 However, although the same principles can be potentially applied to the lower urinary tract there remains a paucity of literature regarding the specific effects of battery acid on the urethral mucosa with only two case reports identified.15,16
Labine et al reported a case of a 77-year-old male with neurocognitive decline who presented 24 h following auto-insertion of 3 ‘AAA’ batteries per urethra who required both manual and endoscopic extraction. 15 Prompt endoscopic retrieval confirmed leakage of battery acid within the penile and bulbar urethra. Repeat cystoscopy revealed a urethral stricture requiring urethral dilatation and eventual urethroplasty, with no reported outcomes. 15
Hosseini et al reported a separate case of an ‘AA’ battery urethral insertion in a 49-year-old male who presented after 9 months with obstructive lower urinary tract symptoms, requiring an endoscopic retrieval followed by a delayed buccal graft urethroplasty for a long penobulbar defect. 16
In 2002, Eke reviewed 1454 cases of coital injuries in males and females. 2 Urethral injury was the most common complication frequently associated with coital injury. Other complications in men included penile fracture, vascular injuries, penile lymphangitis, bladder injuries and urinary incontinence. Young female patients can sustain vesico-vaginal fistula from coitus. 2 Conservative approaches are seldom used but are described in the literature. Palmer et al. described manually milking non-impacted foreign bodies located in the distal urethra. 17
Minimally invasive endoscopic procedures using biopsy forceps or stone baskets usually allow successful removal of the foreign body and permit endoscopic assessment of the proximal urinary tract. Generally, open surgery should be considered as a last resort. The approach usually depends on the location of the foreign body within the urethra. Meatotomy and external urethrotomy is commonly used for anterior foreign bodies whilst for posterior foreign bodies suprapubic cystostomy may be required. Following management of the acute urological issue, the cause of polyembolokoilomania must be addressed. These patients often have co-existing medical and psychosocial issues. As well as sexual gratification, it is associated with mood disorders, cognitive decline and intoxication which require further assessment. Liaison with psychiatric teams should occur before discharge and can prevent repeated episodes.
Urethrocutaneous fistula formation is described as an iatrogenic complication following hypospadias surgery. 18 Reports exist of delayed development of a urethrocutaneous fistula with a retained condom ring. 19
Preputial advancement flaps are well established in the treatment of penile hypospadias with good outcomes. There is evidence that use of this flap can reduce the incidence of fistula post hypospadias repair. They have also been utilised in the management of urethral stricture especially in patients with unfavourable buccal mucosa. Obi in 2013 described the use of fasciocutaenous flap to repair a traumatic urethrocutaneous fistula. 20 To date, the use of preputial advancement flaps in the management of urethrocutaneous fistulae has not been documented and we believe our case to be the first.
Specific to the effects of battery insertion on the urethra our case is unique for several reasons. Firstly, it is the youngest case reported of an open extraction which was required as an initial procedure despite an early clinical presentation. Additionally, although the mid penile defect healed easily within 3 weeks, a delayed urethrocutaneous fistula developed distal to the initial obstruction which required a formal reconstructive repair. Final histology confirmed the presence of pigmented type foreign material and we postulate that the brief submersion of the battery in the urethra caused a delayed chemical reaction which resulted in fistula formation distal to the original urethral insult. Our case is also noteworthy in that we performed a preputial flap, preserved the foreskin and did not require a buccal graft.
Our patient has been followed up for 8 months following his fistula repair. He has had an uncomplicated post-operative course with satisfactory wound healing and good cosmetic (Figure 5), functional and sexual function outcomes as documented with both medical photography and validated scoring systems.
Consent
Informed written consent for medical photography was taken prior to photographs being taken and consent for publication was obtained prior to this report.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.