
Abstract
Introduction:
A constant growth in the population suffering from osteoporotic vertebral weakening is observed. As a result, vertebroplasty procedures become more and more common. Unfortunately, they may be associated with several complications occurring during bone cement injection, including its leakage or overheating of tissues. Despite several experimental studies, there is a lack of data related to random aeration of the bone cement. Therefore, the main objective of the following investigations was to emphasize that random aeration of the bone cement, and, consequently, a compressibility factor, could not be treated as a negligible factor during the vertebroplasty procedure and had to be taken into account in the development of the mathematical model.
Materials and methods:
A special test rig to reproduce the vertebroplasty procedure was designed and built. The authors conducted numerous experiments on polymethylmethacrylate-based bone cement flows, analyzing different flow conditions, such as volume flow rate and flow channel diameter. Time periods of the flow front between characteristic sections and pressures (differential and gauge) were measured.
Results:
All investigations revealed that bone cements mixed in special mixing kits were characterized by a random level of aeration which led to varied flow parameters. Comparing the experimental results with the theoretical values of the continuity equation, the highest difference in the flow duration reached 140%.
Discussion:
It has been proven that the aeration of the bone cement alters the flow dynamics. Therefore, much more data are required for statistical analysis to validate a mathematical model of the bone cement flow.
Introduction
A significant progress in medicine is constantly increasing an average human lifespan. The organism aging and a wrong diet usually lead to an inevitable degradation of bone tissues. As a result, an increase in the number of people suffering from osteoporotic vertebral weakening and compression fractures can be observed. This internal breakage can be stabilized and solidified with vertebroplasty or kyphoplasty procedures. In these minimally invasive procedures, polymethylmethacrylate (PMMA) or other acrylic copolymer is injected to the augmented vertebral body. 1 Bone cements are usually considered to be non-Newtonian pseudoplastic fluids with shear thinning behavior;2–4 however, they have also been modeled as Newtonian fluids. 5 Unfortunately, vertebroplasty may be associated with common complications occurring in the clinical practice such as leakages of the bone cement (especially dangerous when leading to contact with the spinal cord), overheating of the surrounding tissues, incomplete filling of vertebral cavities, and bone breakage due to the overpressurized bone cement. Thus, more effort is needed to investigate experimentally and describe mathematically the process of the bone cement flow, while taking into account the polymerization and macroscopic behavior of cements, such as temperature, aeration, viscosity, and stress which are functions of time and flow conditions (shear strain rate).
Bone cements can vary in chemical composition, 6 and thus their rheological and final mechanical properties (viscosity, strength) are different. The cement behavior between the moment of polymeric compound mixing, when the polymerization starts, and the time when the injecting cannula is removed from the vertebral body is of paramount importance. During the first stage, referred to as a swelling process, a liquid monomer dissolves polymer beads—powder is wetted with the monomer. The second stage is a polymerization reaction6–8—the liquid structure of the bone cement changes into solid. 4 This is an exothermal process and can raise significantly the temperature of the bone cement during the injecting procedure. 9
Numerous studies on bone cements reveal that polymerization is strictly related to many factors that can be gathered into two separate groups: intrinsic and extrinsic. 6 The former group includes several factors contributing to changes in the polymerization level, such as a cement brand and its additive constituents9–11 or a size of PMMA beads. 12 The latter group, extrinsic factors, includes temperature and shear strain rate.8,13,14 Only one research focused on the mixing method impact on the polymerization process. 2 The authors of the above-mentioned publication proved that automated oscillatory mixing led to a decreased mean viscosity of the bone cement in comparison with manual mixing. For the manual mixing, cement components were placed in a plastic beaker and mixed manually with a spatula. Such a mixing method does not resemble the phenomena that can occur inside the mixing kits that are delivered together with bone cements. Some of these kits are designed in such a way that the mixing process comprises two parallel methods: translational and rotational motion of the piston.
Therefore, the main objective of this investigation was to indicate that the traditional vertebroplasty, performed with the above-mentioned kits, yields bone cements of a varied aeration level. As a result, polymerization, hardening time, temperature, and the final volume can be different than expected. Thus, the research novelty consists in emphasizing the fact that random aeration of the bone cement, and, consequently, its compressibility factor, cannot be neglected during the vertebroplasty procedure and has to be taken into account in the mathematical model. Such a model cannot be generated without a statistically significant amount of experimental investigations revealing the flow characteristics of the given material.
Materials and methods
The PMMA-based vertebral cement is characterized by dynamic viscosity that increases with time, which leads to an increase in the flow resistance and, as a result, an increase in the pressure drop between selected points of capillaries. The experimental procedures used during these investigations required sustaining a uniform volume flow rate; hence, a device injecting the cement had to be able to adjust dynamically its exertion force. It was decided to use a Legato™ 210 infusion pump (KD Scientific Company, Holliston, MA, USA) since it offers a variety of functions and can be easily programmed and controlled by the user. A schematic view of the entire test rig is outlined in Figure 1.
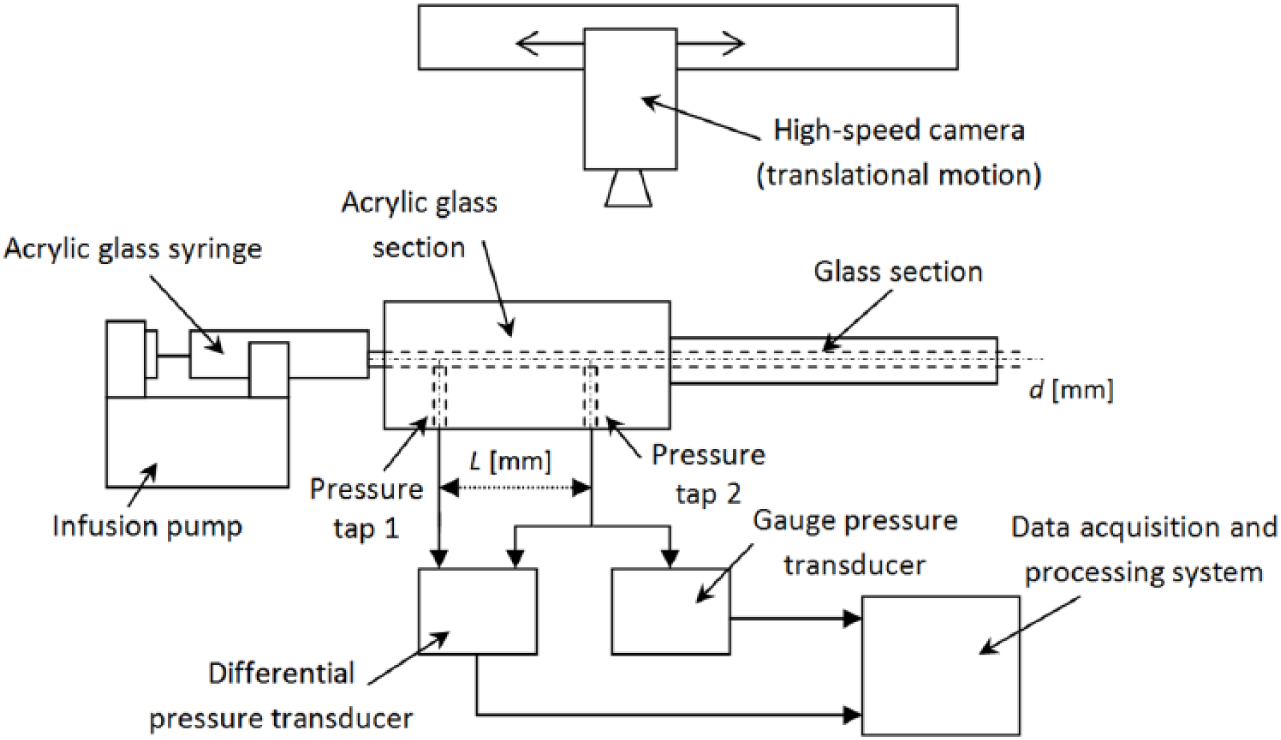
Schematic view of the test rig for investigations of bone cement flows in cannulas.
The analysis of the bone cement flow in cannulas comprised two main parallel stages: the first one devoted to the pressure data gathering and the second to the measurements of the flow time. Due to the fact that pressure in the analyzed channels could reach the value of 2.0 MPa, all components of the test rig had to be mechanically resistant. Moreover, to observe the cement propagation and macroscopic air bubbles trapped in the material, all components had to be transparent. It was decided to split the tested cannula into two sections: the first one was made of acrylic glass, having high fracture resistance, to create taps for connection to pressure transducers; the second cannula section was made of glass tubes. Both cannula sections had the same internal diameters (2.0, 3.0, and 5.0 mm) and were joined together collinearly to avoid any flow disturbances. Pressure taps of diameters equal to 1.0 mm were connected to pressure transducers via hydraulic hoses filled with de-aerated water. The distance between the pressure taps, L, was equal to 60, 60, and 75 mm for the channels of diameters 2.0, 3.0, and 5.0 mm, respectively. In order to connect the first cannula section to the syringe located in the infusion pump, a standardized Luer Lock adapter was used. Such a connection maintains a leak-free interface between both parts due to a tabbed hub on the female part which screws into threads of the male fitting. The syringe was made of acrylic glass with hard and stiff walls to minimize its deformation under high pressure. Considering the pressure data acquisition, we performed measurements in two different parts of the flow channel. A pressure difference was measured on the reference distance, L, inside the acrylic glass section, with a differential pressure transducer. A pressure drop of the fluid flowing through the remaining part of the cannula, mainly a glass capillary section, was measured with a gauge transducer. A high-speed camera was used to register the propagation of the fluid front in both sections of the cannula. With a vast data set of images taken at a specific, constant frequency, the location of the cement front at the given time could be pinpointed and its overall flow time could be calculated. Moreover, this method enabled us to observe the shape of the material front and detect changes in the material velocity resulting from the air phase compression. All investigations were conducted for the constant initial temperature equal to 24°C ± 1°C. The obtained pressure values and time of the flow between particular points in the system under analysis were compared with the theoretical values determined for Newtonian fluids obtained from the Hagen–Poiseuille flow solution

and the corresponding Darcy–Weisbach equation
where Δp is the pressure drop, Q the volume flow rate, u the flow velocity, ρ the fluid density, µ the dynamic viscosity, D the channel diameter, L the channel length, λ the friction factor, and Re is the Reynolds number.
After mounting the entire test rig, its performance and reliability were validated with silicone oils classified as Newtonian fluids. Straight channels of different diameters (2.0, 3.0, and 5.0 mm) with the volume flow rate set to 1.0 and 4.0 cm3/min were tested. The dynamic viscosity values of the analyzed substances were equal to 96 and 294 Pa s—it was considered to be constant, but of a relatively high value, similarly as the PMMA-based bone cement at different stages of polymerization. Prior to the experiment, the syringe had been filled with silicone oil and left open to the atmosphere for several hours to minimize the amount of air bubbles trapped inside the oil (de-aeration process). In the case of bone cements, de-aeration could not be performed due to its time-dependent polymerization. In order to reproduce real vertebroplasty procedure conditions, we had to use the system for cement mixing delivered with the cement, the idea of which is presented in Figure 2. It consisted of a seal-closed chamber with a mixing piston inside, moved by a handle. Mixing of the bone cement compounds was via pushing and pulling the handle for approximately 20 s (1–2 strokes per second). The first few mixing strokes had to be performed slowly with a reciprocating-rotating movement. Although the time of mixing was the same in each of the cases tested, there were several factors that might have contributed to the randomness of the bone cement aeration, such as speed of mixing, additional rotational motion of the mixing kit, and a number of oscillatory strokes.
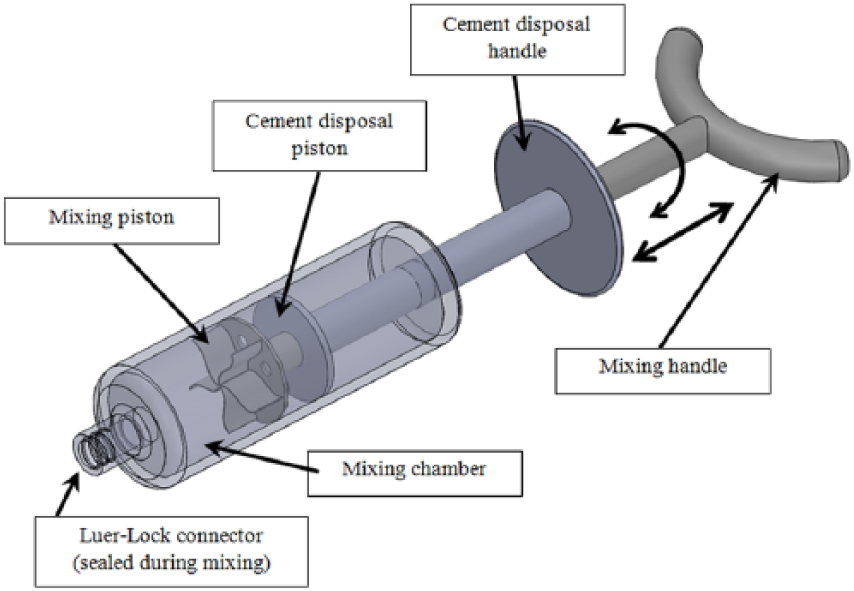
Simplified model of the provided cement mixing kit.
Results
In order to validate the test rig performance as well as to master the experimental procedure, we performed numerous tests on silicone oils, analyzing varied flow parameters. Examples of pressure characteristics are outlined in Figure 3. Vertical lines correspond to the time moments, when the material reached specific points inside the test channel.
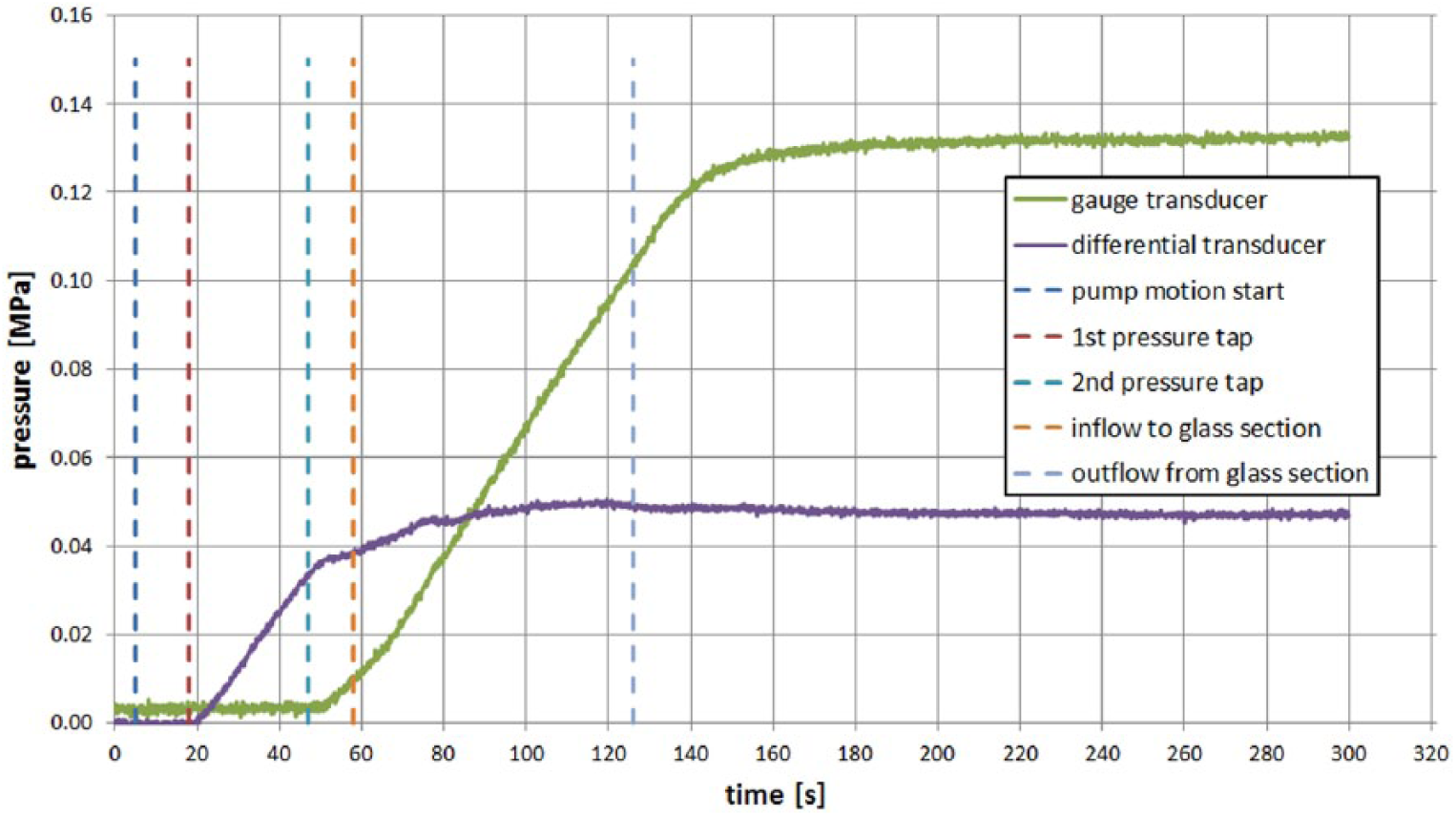
Pressure data obtained for the silicone (96 Pa s) flow in the 3.0-mm channel with 1.0 cm3/min volume flow rate.
On the basis of the obtained database, we decided not to investigate channels of diameter 2.0 mm and flows with the volume flow rate equal to 4.0 cm3/min in the cement flow studies. Such flow parameters entailed a high risk that the infusion pump exertion force was insufficient to keep the motion and, as a result, the flow could be interrupted and stopped.
After pressure stabilization, the obtained values were compared with the Hagen–Poiseuille flow solution and the Darcy–Weisbach friction factor (see Figure 4). It can be stated that the majority of the results are in conformity with the main principles of fluid mechanics. Thereby, it can be concluded that the mounted test rig enables one to measure properly all the investigated flow parameters and can be used for further accurate analysis of PMMA-based cement flows.
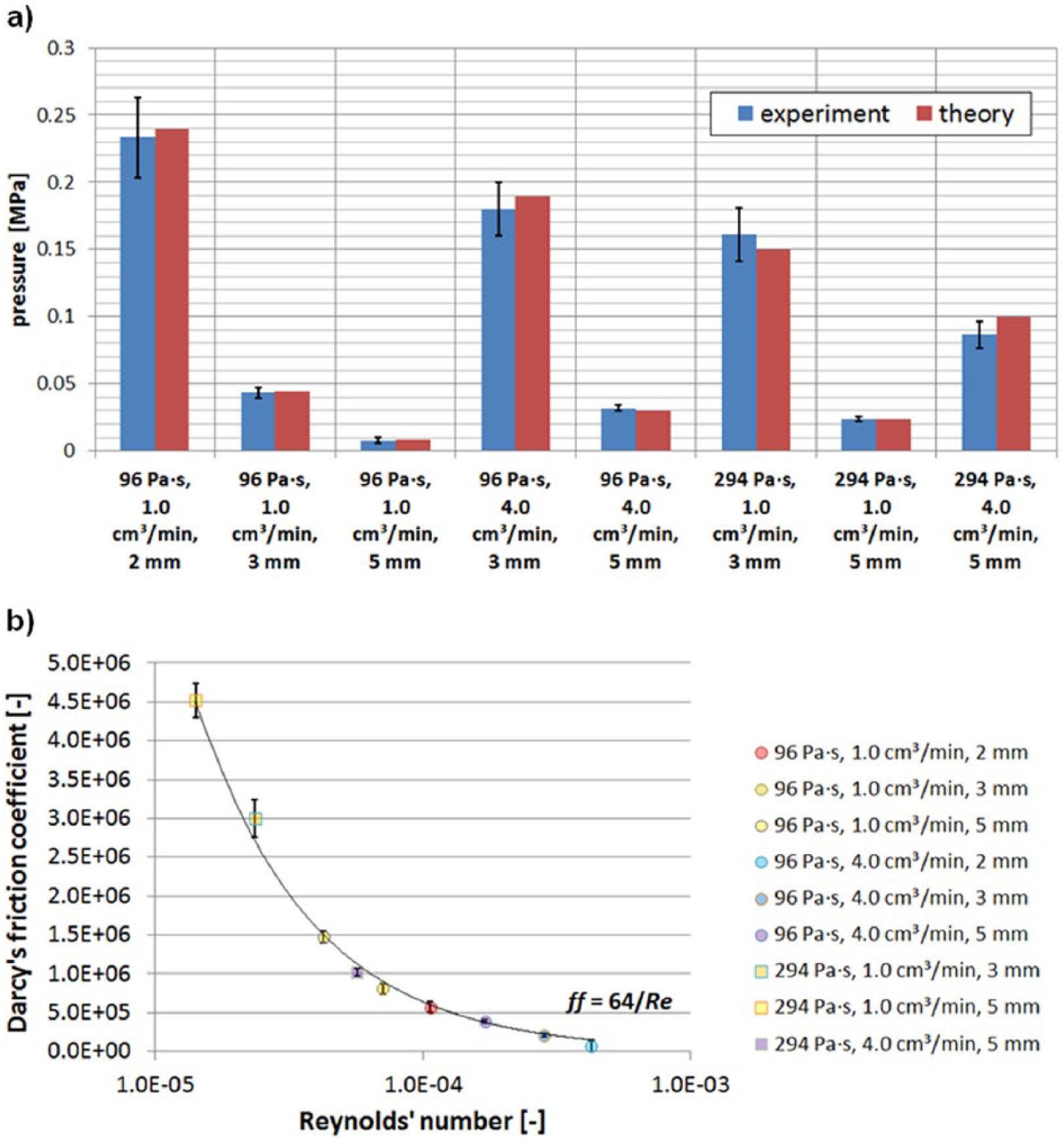
Comparison of the obtained data set for silicon oils with (a) Hagen–Poiseuille equation and (b) Darcy–Weisbach friction factor.
In order to prove that the aeration of the material alters the flow characteristics and, therefore, can play a significant role during vertebroplasty, the experimental values of the flow time between characteristic sections in the system were compared to the theoretical ones determined for an incompressible fluid. Knowing the distance between pressure taps in the test section, the length of glass capillaries, and the volume flow rate set on the infusion pump, one could calculate the theoretical time of the flow. The above-mentioned juxtaposition is outlined in Table 1. It is worth mentioning that the data presented in this table correspond to the averaged values together with the standard deviation calculated for each data set.
Comparison of the averaged flow durations obtained for silicone oils and bone cements.
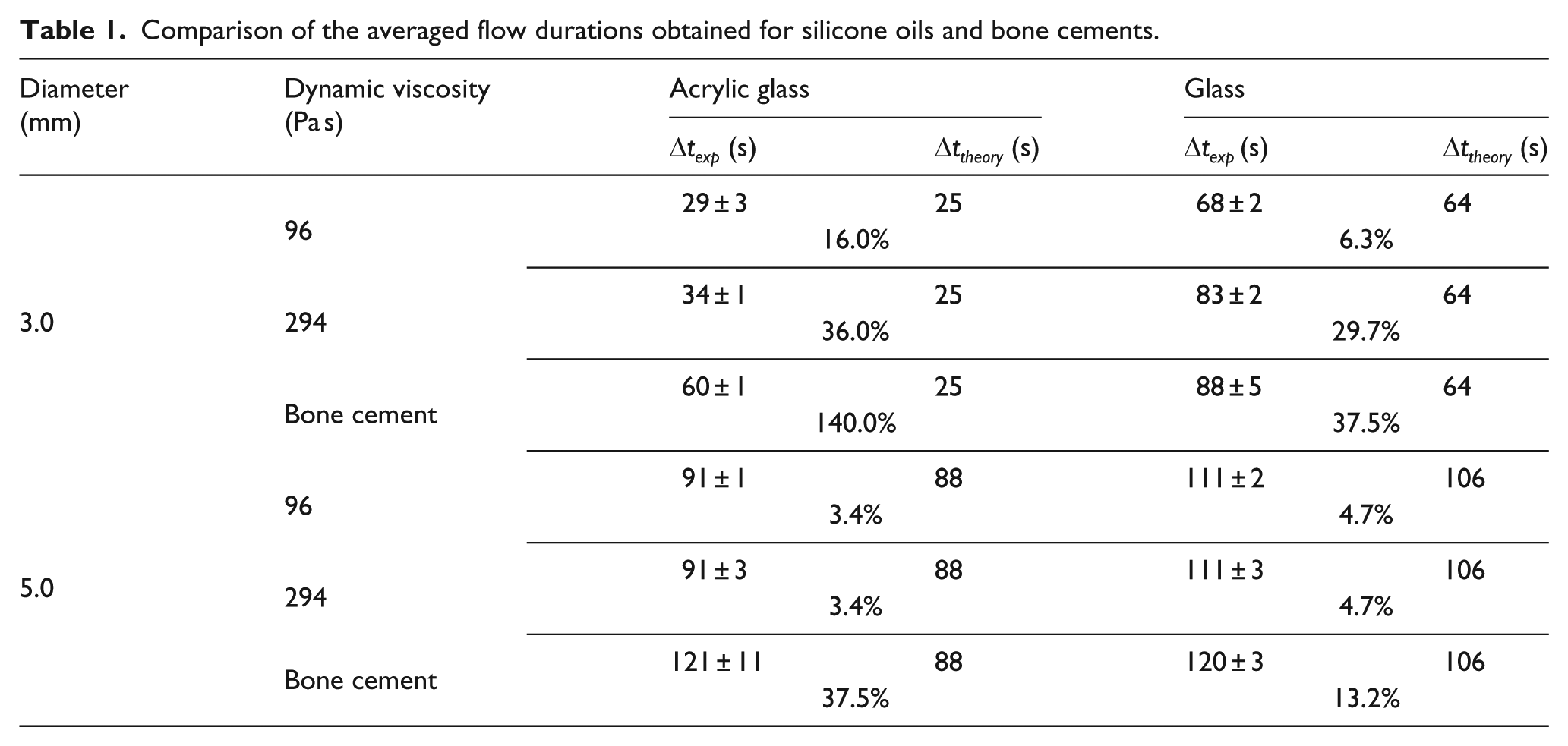
As can be observed from Table 1, flow durations for both silicone oils and bone cements are burdened with some discrepancies when compared to the theoretical values. It means that both substances were moving slower than estimated on the basis of the continuity equation. The aeration of the substance is the most plausible explanation. The air trapped/dissolved in the liquid was compressed when subjected to the exertion force, thus reducing the velocity of the propagating material. It can be clearly seen that for smaller channel diameters and higher volume flow rates the differences are more significant. It indicates that higher pressure results in larger material compressibility. The flow time difference reaching 36% for the silicone oil indicates that, despite a long de-aeration process, compressibility of this material was significantly high. Nevertheless, it can be clearly seen that the discrepancies obtained for bone cements reach significantly higher values than for silicone oils; hence, the aeration of the bone cement is definitely higher. Due to the fact that these differences reach even 140%, it can be stated that the aeration level of cement cannot be treated as a negligible factor. It cannot be left unmentioned that, while the syringe was being filled with the bone cement, a macroscopic bubble that could not be removed from the syringe without a significant loss of the cement volume was formed.
Furthermore, for a better outline of the aeration influence on the cement flow, gauge pressure characteristics in tap 1 for the cases with the same flow conditions are presented in a single plot—see Figure 5. The syringe filling and its mounting time in the infusion pump were similar in each case under analysis. Thereby, the aeration level of cement, changing the compressibility of the mixture, was the only possible factor affecting the flow characteristics. Despite the similar initial temperature and the same volume flow rate set on the infusion pump (1.0 cm3/min), the bone cement flow varied significantly in each case. As pressure is directly related to dynamic viscosity, volume flow rate, and polymerization degree, the time when the same pressure value was achieved was recorded in all cases under investigation. The gauge pressure used for the comparison was equal to 0.8 MPa since it was the lowest reading obtained in all the experiments. As shown in Figure 5, the time measured differs significantly. For the channel of 3.0 mm diameter, the highest difference between the measured and averaged values was equal to 21%. Similarly, as in the analysis of the flow time, it was proven that the initial aeration of the bone cement played a significant role during its flow and injection. Thus, PMMA-based cements should not be treated as incompressible. This conclusion is in conformity with the work by Baroud et al., 2 where significant differences among measurements obtained for the same flow parameters and the manual mixing were observed. The random aeration of the prepared bone cement was the most plausible reason behind such a variability. The cement aeration is clearly shown in Figure 6 for a solidified cement specimen fracture.
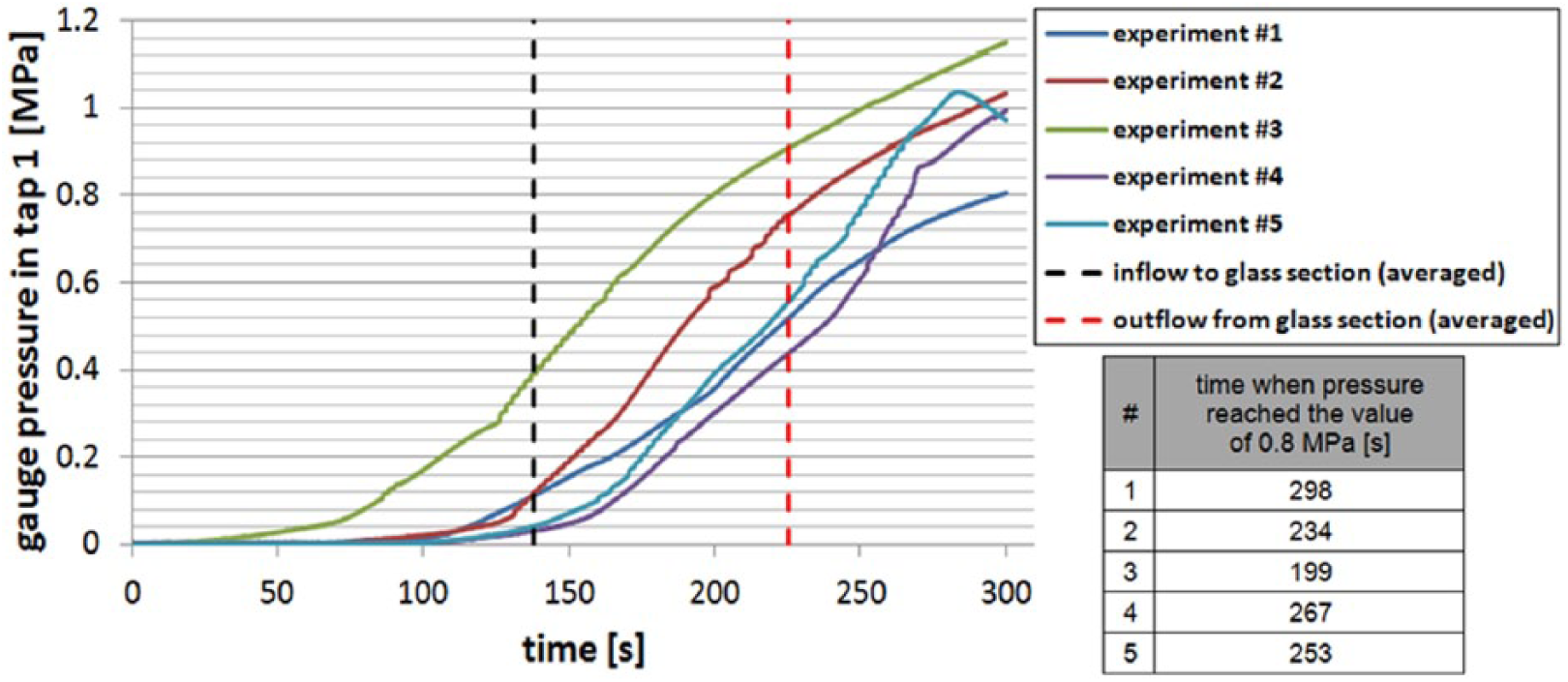
Several tests on the bone cement flow in the 3.0-mm channel with 1.0 cm3/min volume flow rate.
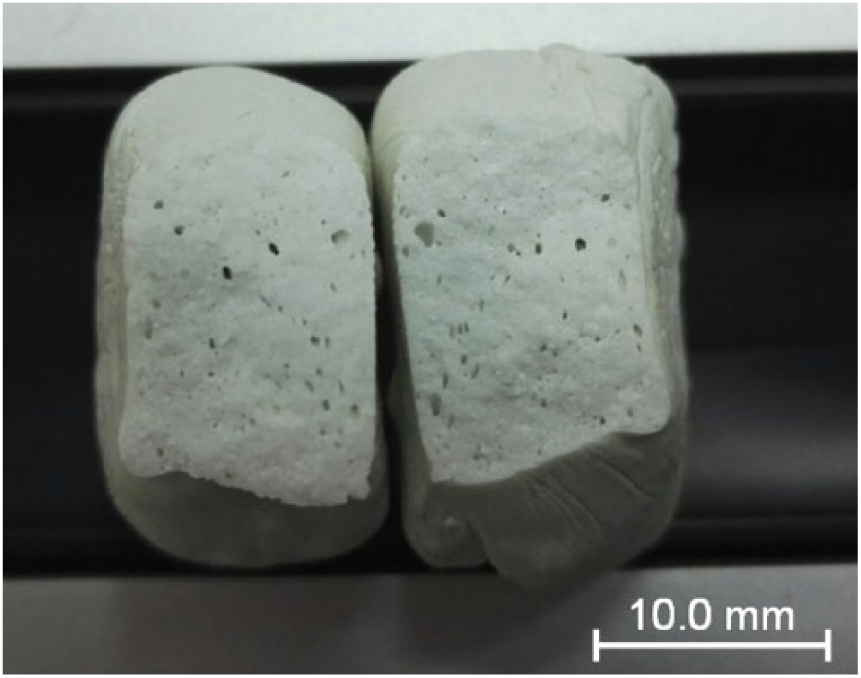
Cross-section of the solidified cement specimen with air pores (cement aeration outcome).
Discussion
We prepared a test rig to reproduce the real vertebroplasty procedure. The reliability of the experimental equipment was verified by numerous tests on silicon oils. The obtained results proved the sufficient accuracy and repeatability of the tests. During the experiments of the PMMA-based bone cement flow, a special mixing kit, provided by the bone cement producer, was used. Numerous experiments were performed on the bone cement under the same flow conditions, that is, initial temperature, volume flow rate, and diameter of the flow channel, and they resulted in different pressure drop characteristics. They indicated that bone cements were characterized by a relatively high and unrepeatable level of aeration. This specific property is strictly connected to the compressibility factor of the flowing medium, which can bear significant consequences on the flow dynamics. The more aerated the material, the lower its volume flow rate and the longer the flow time. Similar results were obtained by another group of scientists. They proved that the viscosity variability for the cement mixed manually was three times higher than that for the cement mixed with a controlled method. 2
In the currently available references, there are multiple numerical models of the bone cement polymerization that depend on several factors, that is, initial temperature, PMMA bead size, or shear strain rate. However, they neglect and do not place a significant emphasis on the mixing method which is closely related to material aeration, and, as a consequence, a compressibility factor, which has tremendous influence on the flow parameters. Therefore, in the mathematical model of the flow of the PMMA-based bone cement, the aeration level has to be defined. This parameter can differ significantly not only among various cement types and cement mixing kits, but also due to different mixing parameters, that is, speed of mixing or rotational motion of the mixing kit. Thus, the cement mixed during the traditional vertebroplasty procedure is characterized by a random, unrepeatable aeration level. Hence, the most reasonable and reliable approach to define the aforementioned level is to perform numerous tests on particular bone cements and cement mixing kits for statistical processing and analysis. One of these tests could focus on a quantitative and qualitative analysis of cement compressibility with automated hydraulic press and proper measurement systems.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was financially supported by the National Center for Research and Development in Poland (PBS3/B9/45/2015, project entitled Innovative Medical Surgical Technology with Implantable Inter Intra Vertebral Body Fusion (IIVbF) device expanding effective healing of degenerative spine, realized in cooperation with L.F.C., IBeMT, and BioNanoPark).