
Abstract
Background
Household food insecurity is a critical concern for ultra-poor families in low- and middle-income countries like Bangladesh, particularly those with members who have disabilities. The COVID-19 pandemic has worsened this situation.
Objective
This study aimed to assess the impact of microfinance-based livelihood programs on food insecurity in ultra-poor families with members affected by cerebral palsy in Bangladesh.
Methods
Data were extracted from the SUPPORT CP trial for 251 children with cerebral palsy. The Household Food Insecurity Access Scale score was the outcome variable. The explanatory variable was the intervention type, dividing the sample into 3 arms: Arm C (care as usual), Arm B (Community-Based Rehabilitation [CBR]), and Arm A (CBR with the integrated microfinance-based livelihood program [IMCBR]). Both linear regression and the Generalized Estimating Equations model were used to determine the association of outcome variable with explanatory variables adjusting for covariates.
Results
We found a consistent level of household food insecurity across each time point, with a significant increase in the midline during the peak of COVID-19 pandemic in 2020. However, following the end of the COVID-19 pandemic, both Arms A and B, where interventions were provided, reported a significant decline in food insecurity. Notably, Arm A, where IMCBR was provided, exhibited the fastest decrease in food insecurity followed by Arm B, where only CBR was provided, compared to Arm C.
Conclusion
Microfinance programs can reduce food insecurity among families of children with cerebral palsy in Bangladesh, especially during crises like COVID-19, underscoring the need to integrate them with tailored disability rehabilitation services.
Plain language title
How Microfinance Can Help Families with Disabilities in Bangladesh Reduce Hunger
Plain language statement
Many families in Bangladesh face hunger, especially those living in poverty and caring for children with disabilities like cerebral palsy. The COVID-19 pandemic made this problem worse. This study looked at whether combining microfinance programs with community rehabilitation services could help these families have more reliable access to food. Families who received both microfinance support and rehabilitation services experienced the biggest improvements in food security. These findings suggest that microfinance-based programs can play a key role in reducing hunger for the most vulnerable families, including families with severe form of disabilities, such as families of children with cerebral palsy.
Keywords
Introduction
In Bangladesh, nearly 17% of the population is currently experiencing food insecurity, equating to almost 2 out of every 10 households. 1 This figure is significantly higher than the global household food insecurity rate of 11.7% and has contributed to Bangladesh's ranking of 75th in the Global Hunger Index among 107 qualifying nations.1,2 Such an assessment underscores the impact of the current global economic slowdown on food insecurity and hunger faced by many emerging economies. Factors such as extreme poverty, inadequate access to land for cultivation, social exclusion, and natural disasters all contribute to the exacerbation of food insecurity in Bangladesh, with vulnerable households and marginalized communities particularly more vulnerable.3,4 Additionally, the war in Ukraine, export bans, the COVID-19 pandemic, and climate change have impacted the global food system and further worsened the situation. 5 This therefore considers a significant barrier to achieving multiple Sustainable Development Goals (SDGs), including no poverty (SDG 1), zero hunger (SDG 2), health and well-being for all (SDG 3), inclusive and equitable quality education for all (SDG 4), gender equality (SDG 5), and inclusive and sustainable economic growth, employment and decent work for all (SDG 10). 6
Microfinance-based livelihood programs have shown a positive impact on poverty reduction globally, primarily by increasing household income and empowering its members, especially women.7–12 It can serve as a crucial social safety-net for vulnerable households and marginalized communities and may significantly mitigate the adverse effects of unpredictable and unalterable factors.8,11,12 However, the extent of its efficacy is yet to be comprehensively investigated, particularly for the most vulnerable populations (ie, persons with disabilities and their families), where the effectiveness of microfinance-based livelihood programs remains uncertain due to conflicting findings, with relevant studies having reported positive, negative, and null effects. Moreover, while there are some studies available that focus on poor households in Bangladesh, similar to other LMICs, there is a notable gap in research concerning households with persons with disabilities, who face even greater marginalization in several areas. These include access to education, employment opportunities, healthcare services, and social inclusion.8,10,13 Persons with disabilities often encounter barriers and discrimination that exacerbate their already challenging circumstances, resulting in limited access to essential resources and opportunities for socioeconomic advancement. 13 Additionally, societal attitudes and stigma further contribute to their exclusion and marginalization.13,14 Therefore, there is a critical need for research that specifically addresses the intersecting challenges faced by households with persons with disabilities in Bangladesh, as well as the effectiveness of microfinance-based livelihood interventions among these families. However, these aspects are still lacking. Most studies on microfinance-based livelihood interventions in Bangladesh and other LMICs have focused on the general population, particularly those living in poverty and women, with little to no attention given to people with disabilities.15–19 We, therefore, conducted this study to explore the impact of microfinance-based livelihood programs on household food insecurity among ultra-poor families with persons with disabilities in Bangladesh.
Methods
Study Design and Sampling
The data analyzed in this study were extracted from the programmatic and open-label cluster randomized controlled trial entitled “Supporting People in Extreme Poverty with Rehabilitation and Therapy (SUPPORT CP)” conducted from December 2019 to February 2021. 20 This trial aimed to investigate the efficacy of an integrated microfinance/livelihood and community-based rehabilitation (IMCBR) program in improving the health-related quality of life and motor function of children with cerebral palsy (CP) living in ultra-poor families. The trial was conducted in 3 rural subdistricts: Shahjadpur, Belkuchi, and Ullahpara, all situated within the Sirajganj district of Bangladesh. The baseline assessment was conducted in December 2019; however, the study was disrupted by the COVID-19 pandemic, and the 6-month follow-up (midline) data were collected during the peak of the pandemic, from June to August 2020. The second follow-up assessment was conducted in February 2021, when Bangladesh had nearly returned to normal, although schools remained closed as a protective measure. Despite this disruption, the survey timeline provided us with an opportunity to compare household food insecurity during the prepandemic, peripandemic, and postpandemic periods. The trial protocol has been previously published in a separate publication. 20
Participants and Recruitment
Children with CP and their primary caregivers, mainly mothers or grandmothers (in absence of mother), were recruited for this study. Participant selection was based on the Bangladesh CP Register, which has been diligently monitoring children with CP since its establishment in 2015. Between January 2015 and December 2019, a total of 1862 children with CP were recruited from the 3 subdistricts within the Sirajganj district⸱ Children with CP aged ≤5 years and their primary caregivers were included in the trial. Additional inclusion criteria included families experiencing extreme poverty, defined as having a per capita income of less than USD 1.90 per day according to the World Bank's 2017 guidelines (which was updated to USD 2.15 per day in 2022), and whose primary caregiver provided informed consent. 21 Conversely, families that had received microfinance/livelihood support from other organizations or were concurrently participating in other clinical trials were excluded. Initially, 338 children with CP were selected from these 3 subdistricts; however, 87 of them were excluded either for not meeting the inclusion criteria or for not expressing an intention to participate. In the end, a total of 251 children with CP and their primary caregivers were included in the trial.
Cluster Formation and Randomization
We formed 24 clusters based on mouzas, which are the smallest public administrative units in Bangladesh, with each mouza comprising approximately 5 villages. Within each mouza, there were 10 to 14 children with CP and their primary caregivers. Subsequently, these 24 clusters were divided into 3 arms, namely Arm A, Arm B, and Arm C, in a 1:1:1 ratio. The allocation of clusters to each arm was carried out randomly using a computer-generated randomization schedule. This resulted in 8 clusters with 80 children in Arm A, 8 clusters with 82 children in Arm B, and 8 clusters with 89 children in Arm C.
Interventions Allocated to Created Arms
Among the 3 arms created, Arm A received Community-Based Rehabilitation (CBR) integrated with a microfinance-based livelihood program for parents (IMCBR). The CBR component of the program included a Parent Training Module, and a Goal-Directed Training program designed for children with CP. The microfinance-based livelihood program included supporting the primary caregivers of children with CP in the arm to create microfinance/livelihood groups, initial consultation, skill identification, and training to facilitate participation in microfinance-based livelihood activities, retention, and meeting logistics and livelihood commodity (eg, goat, lamb, chicken) worth AUD$ 200 per primary caregiver/family. The support was provided only once at the beginning of the trial. Arm B received the CBR intervention alone. Meanwhile, Arm C functioned as the control group, with households receiving information solely about early intervention and rehabilitation and care as usual. A comprehensive description of these interventions is presented elsewhere. 20
Outcome Variable
The outcome variable considered was the Household Food Insecurity Access Scale (HFIAS) score. The survey gathered food insecurity data using a set of 9 questions originally developed by the Food and Nutrition Technical Assistance project of USAID to create the HFIAS. 22 These questions were posed during the baseline, first follow-up, and second follow-up assessments. Respondents were provided with dichotomous options, with “0” indicating a positive response and “1” indicating a negative response. Based on the responses collected, we computed a HFIAS score for each household in which the respondents resided. This was done separately for the baseline, first follow-up, and second follow-up evaluations, with scale values ranging from 0 to 9. A higher value of scale indicates greater food insecurity. The resulting scale score served as the outcome variable for analysis.
Explanatory Variables
The primary explanatory variable considered was the type of intervention, including Arm C (care as usual), Arm B (CBR), and Arm A (IMCBR). Additionally, other explanatory variables examined were respondents’ sociodemographic characteristics. These included mother's occupation (nonhousewives and housewives), mothers’ education (no education, up to primary, up to secondary, and higher), fathers’ education (no education, up to primary, up to secondary, and higher), father's occupation (agriculture, blue-collar worker, white-collar worker, and others), and socioeconomic status (high, middle, and low). An additional characteristic considered was the respondents’ perceived impact of COVID-19 on household food insecurity, categorized as Yes and No.
Statistical Analysis
We used descriptive statistics to explore the characteristics of the respondents. A multivariate linear regression model was employed to examine the association between the outcome variable and the explanatory variable. Both unadjusted and adjusted models were implemented. In the unadjusted model, only the outcome and explanatory variables were considered separately for the baseline, first follow-up, and second follow-up assessments. These associations were further explored in the adjusted model with adjustments made for respondents’ sociodemographic characteristics. We also run the Generalized Estimating Equations model to determine the association of outcome variable with explanatory variables accounting for correlation within the subjects/clusters over time. Results are presented as odds ratios (ORs) and their corresponding 95% confidence intervals (95% CI). All analyses were conducted using the statistical software Stata version 15.1.
Results
Background Characteristics of the Respondents at the Baseline
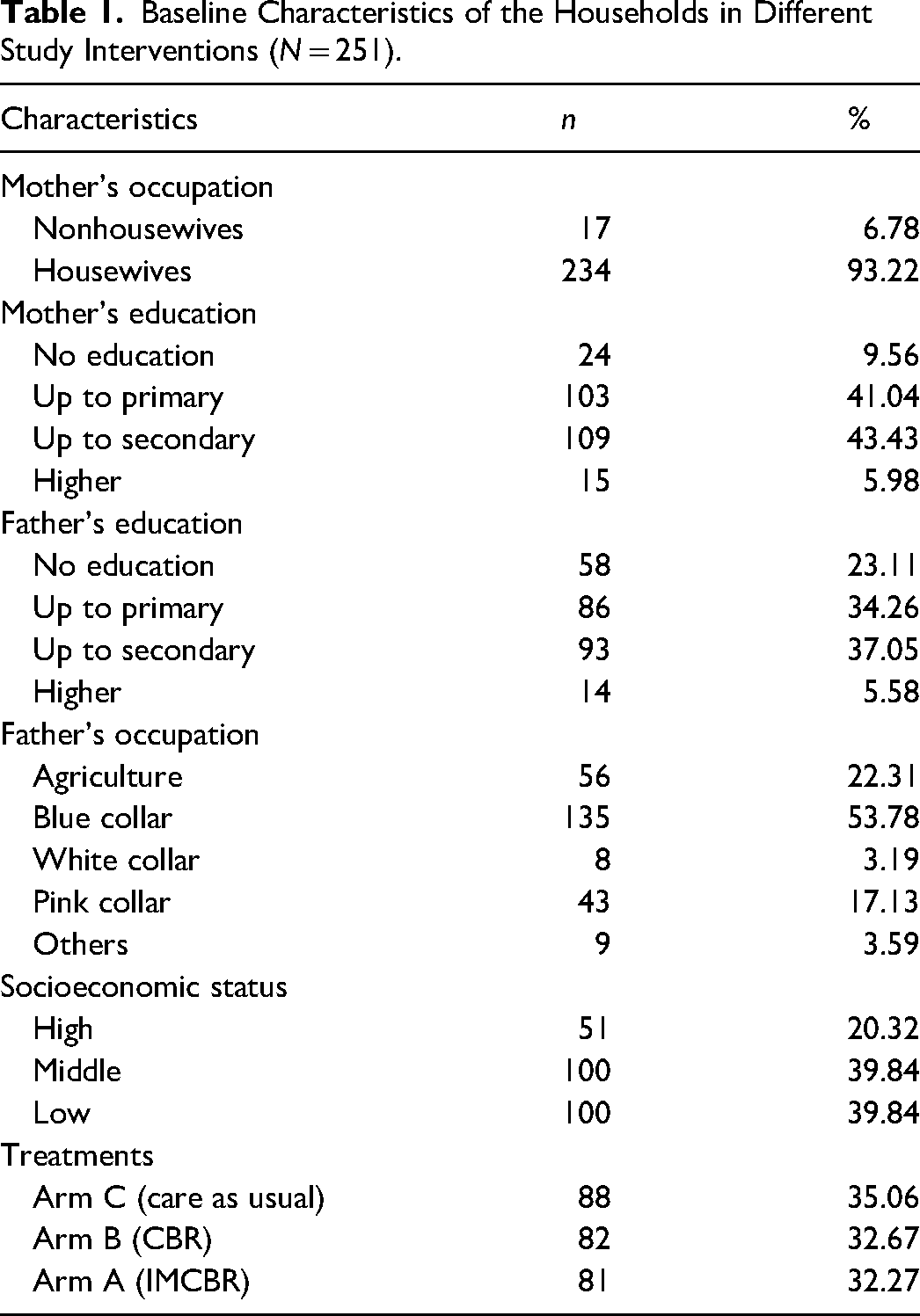
The baseline characteristics of the respondents are presented in Table 1. The majority of mothers were housewives (93.22%), and a significant proportion had attained education up to the secondary level (43.43%). Conversely, among fathers, the highest percentage had attained education up to the secondary level (37.05%), followed by those with education up to the primary level (34.26%). The predominant occupation among fathers was blue-collar jobs (54.78%), with agriculture being the next most common (22.31%), followed by pink-collar jobs (17.13%) and white-collar jobs (3.19%). The socioeconomic status of the households varied, with 39.84% classified as high, 39.40% as low, and 20.32% as middle. When we examined the baseline characteristics across the 3 arms, we found that all characteristics were similarly distributed (results not shown in the table).
Baseline Characteristics of the Households in Different Study Interventions (N = 251).
Household Food Insecurity Access Scale Score
A HFIASscale was developed separately for each arm and is presented in Figure 1. Initially, at baseline, we observed a higher level of food insecurity in Arm A, whereas Arms B and C exhibited comparable levels. Transitioning to the first follow-up period coinciding with the onset of the COVID-19 pandemic, all arms experienced a notable escalation in food insecurity, with Arm B registering the most substantial increase, eventually reaching a level comparable to that of Arm A. Subsequently, during the second follow-up period postpandemic, all arms demonstrated a decline in food insecurity scores, with the most significant reductions observed in Arms A and B.
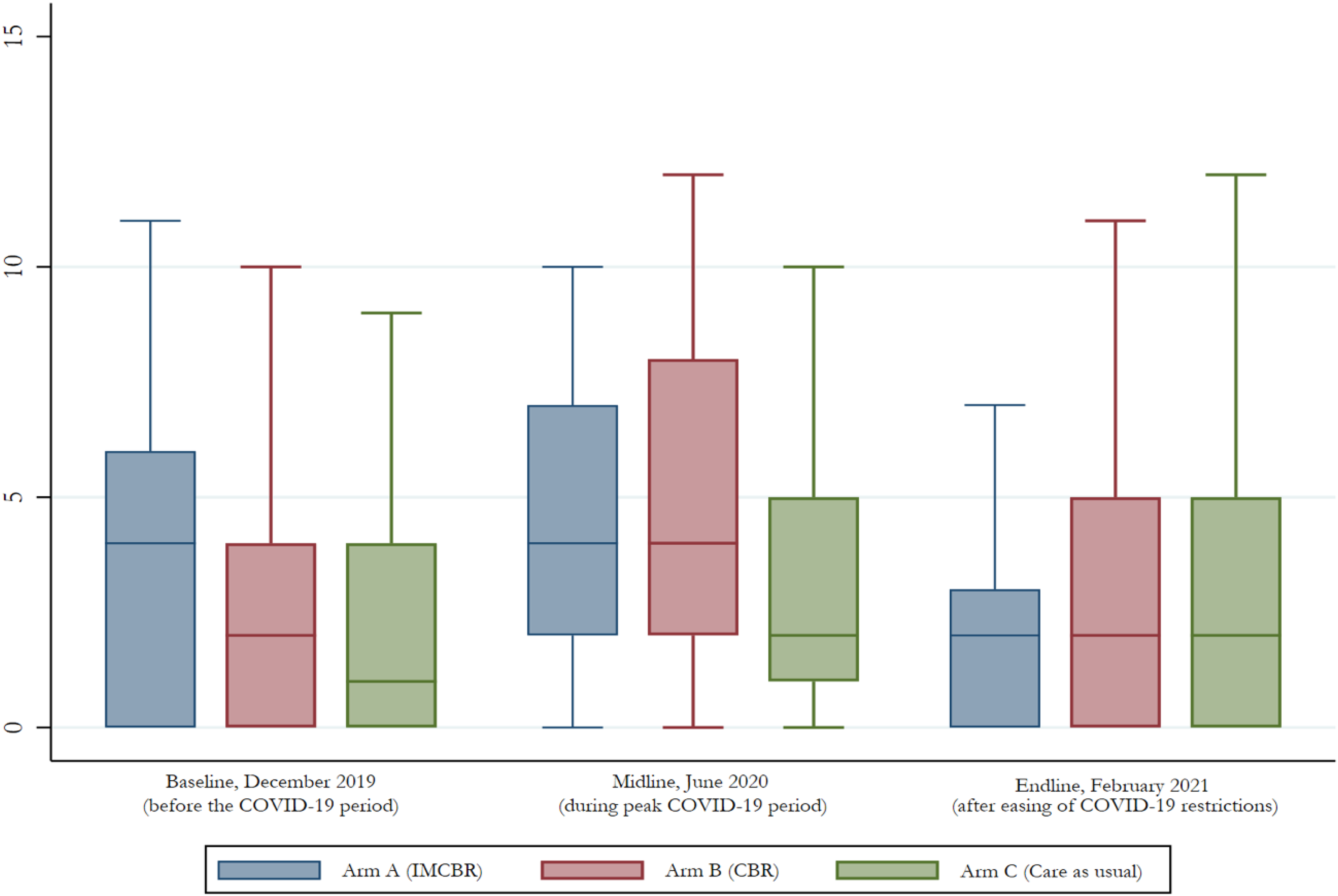
Box plots of the Household Food Insecurity Assess Score (HFIAS) for the baseline, first follow-up, and the second follow-up by interventions.
Impact of Microfinance-Based Livelihood Program on Household Food Insecurity
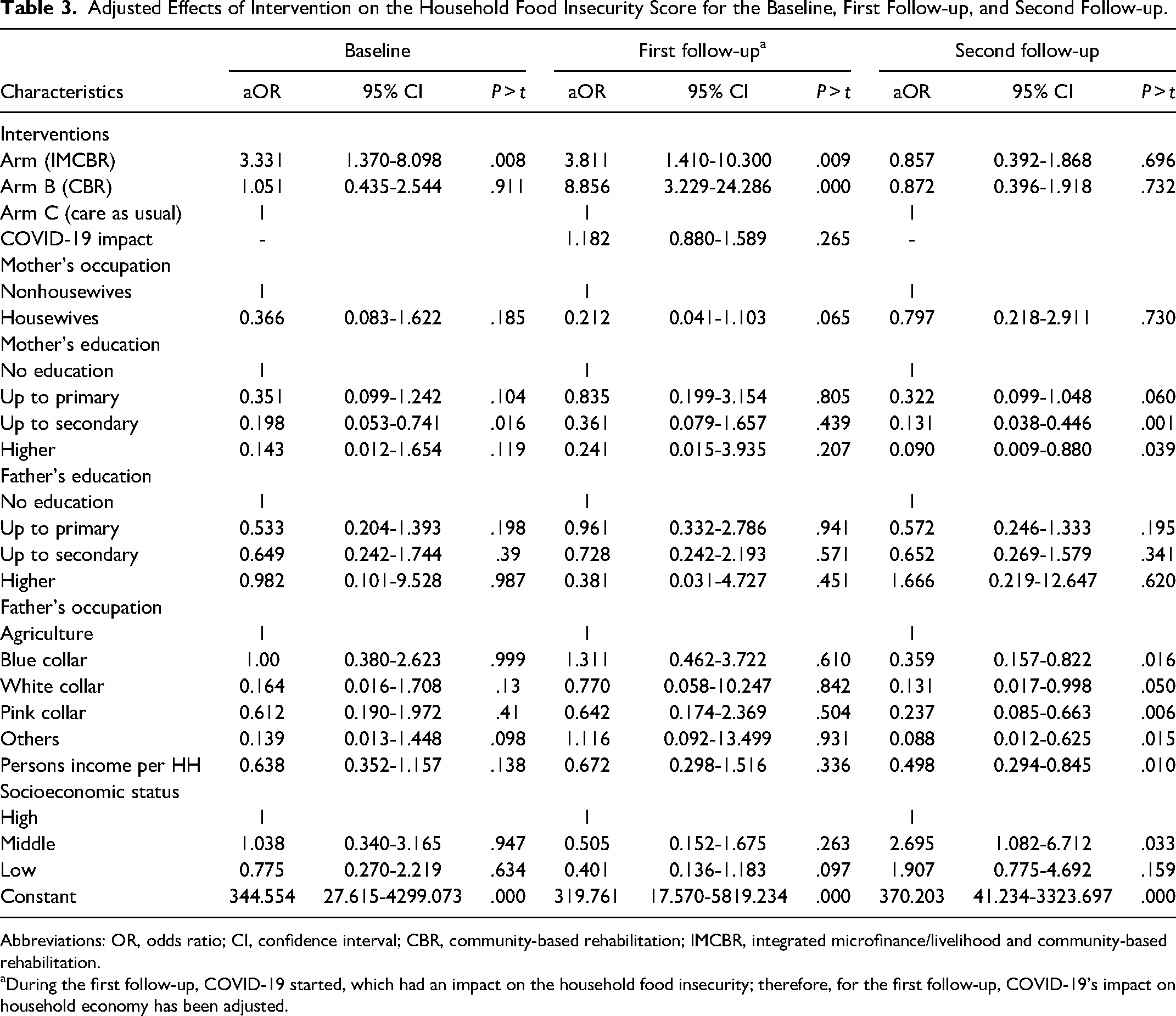
The impact of the microfinance-based livelihood program on household food insecurity was explored through both unadjusted and adjusted multivariate logistic regression analyses, with the results presented in Tables 2 and 3, respectively. In the unadjusted model, we observed a significant increase in the likelihood of food insecurity among participants in Arm A at both the baseline and first follow-up periods. Upon adjusting the model for respondents’ sociodemographic characteristics and their perceptions of the impact of COVID-19, compared to Arm C, participants in Arms A and B reported 3.81 times (95% CI = 1.41-10.30) and 8.86 times (95% CI = 3.23-24.29) higher likelihoods of food insecurity during the pandemic, respectively. While the likelihood of food insecurity for participants in Arm A remained similar to baseline levels (aOR = 3.33; 95% CI = 1.37-8.10) when compared to the same reference group, participants in Arm B experienced a substantial increase (aOR = 1.05; 95% CI = 0.43-2.54) (Table 3). However, both arms reported a decrease in the likelihood of food insecurity following the pandemic, although this decline was not statistically significant, with Arm B showing the most rapid decline compared to the COVID-19 period. Furthermore, in our analysis of the longitudinal effects of the intervention on household food insecurity scores, we observed that the probability of experiencing food insecurity was 1.18 times higher during the peak of the COVID-19 pandemic compared to the prepandemic period (Supplemental Table 1).
Adjusted Effects of Intervention on the Household Food Insecurity Score for the Baseline, First Follow-up, and Second Follow-up.
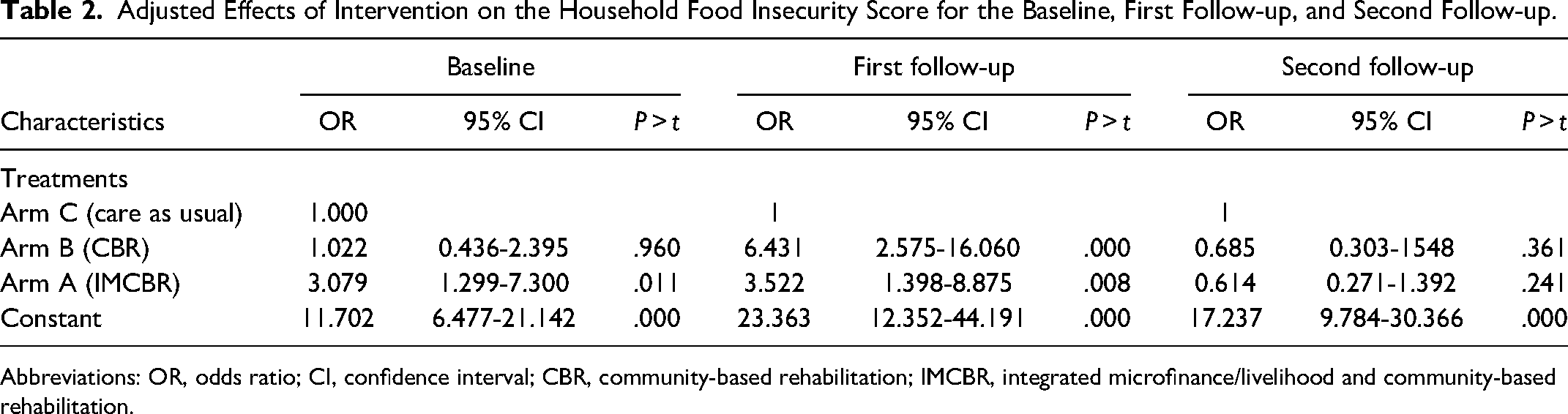
Abbreviations: OR, odds ratio; CI, confidence interval; CBR, community-based rehabilitation; IMCBR, integrated microfinance/livelihood and community-based rehabilitation.
Adjusted Effects of Intervention on the Household Food Insecurity Score for the Baseline, First Follow-up, and Second Follow-up.
Abbreviations: OR, odds ratio; CI, confidence interval; CBR, community-based rehabilitation; IMCBR, integrated microfinance/livelihood and community-based rehabilitation.
During the first follow-up, COVID-19 started, which had an impact on the household food insecurity; therefore, for the first follow-up, COVID-19’s impact on household economy has been adjusted.
Discussion
The objective of this study was to investigate the impact of microfinance-based livelihood interventions on household food insecurity. We observed a consistent level of household food insecurity across each time point, with a significant increase during the COVID-19 period. However, following the end of the pandemic, both Arms A and B reported a significant decline in food insecurity. Notably, Arm A, which received CBR integrated microfinance-based livelihood support, exhibited the fastest decrease in food insecurity compared to Arm B, which received CBR only. These findings suggest that microfinance-based livelihood programs can effectively mitigate food insecurity among the most vulnerable populations in Bangladesh, even during uncertain conditions such as the COVID-19 pandemic. Furthermore, this experience may be replicable in other LMICs, including Bangladesh.
We found higher levels of food insecurity among the ultra-poor families with persons with disability in Bangladesh. This observation aligns with previous studies conducted in LMICs and Bangladesh, where microfinance-based livelihood support has been explicitly studied.15–19 Several sociodemographic factors contribute to its prevalence, including unemployment, limited access to education, and inadequate healthcare services.23–27 The COVID-19 pandemic further exacerbated these challenges, resulting in a significant increase in food insecurity nationwide. 27 Lockdowns, movement restrictions, and economic disruptions led to the loss of livelihoods and income for many households, particularly those already vulnerable to food insecurity.27–29 With restricted access to markets, escalating food prices, and disruptions in supply chains, families encountered difficulties in obtaining essential food items.28,29 Moreover, measures implemented to contain the virus, such as social distancing and school closures, deprived many children of school meals, exacerbating the situation further. 30 Consequently, the COVID-19 pandemic not only underscored existing vulnerabilities but also deepened the food insecurity crisis in Bangladesh.
However, our analysis revealed that households receiving the IMCBR and CBR reported a notable 25% to 27% decrease in household food insecurity following the COVID-19 pandemic, with the most substantial decline observed among households receiving IMCBR. This finding suggests that households enrolled in these intervention arms were able to mitigate the impact of the pandemic on food insecurity more effectively. The mechanism underlying this outcome can be attributed to the fact that households participating in the microfinance program were able to utilize the funds to engage in income-generating activities.8,11 For instance, they could invest in purchasing agricultural inputs and equipment or engage in livestock rearing (eg, goat and lamb). 8 These activities contribute to increasing food production and establishing a safety-net during times of crisis, thereby rendering families more self-sufficient and less dependent on external assistance.
These findings suggest that microfinance-based livelihood programs can serve as an effective mechanism for building resilience among the ultra-poor populations in the face of economic or national disasters. This aligns with the substantial efforts of the Bangladesh government to enhance existing social safety-net and social empowerment programs in general and during the COVID-19 pandemic.31–33 Major Microfinance Institutions/NGOs in the country such as Grameen Bank, BRAC, ASA, and Proshika have extensive coverage of microfinance programs. 33 While the primary objective of these programs is poverty reduction, our study findings provide further evidence of their effectiveness in addressing household food insecurity. However, it is noteworthy that although existing microfinance programs do not specifically target households with persons with disabilities, our findings suggest that extending coverage of microfinance-based livelihood programs to people or households with disabilities, including those with CP, alongside their long-term rehabilitation efforts, could serve as a valuable safety-net for them during crises.
This study possesses several strengths as well as a few limitations. A primary strength lies in the analysis of data from a programmatic and open-label cluster randomized controlled trial, presenting household food insecurity among ultra-poor families in Bangladesh, a pioneering effort in the country. Advanced statistical models were employed, incorporating a range of covariates to assess the impact of microfinance-based livelihood programs on food insecurity among these vulnerable populations. Furthermore, the survey time frame enabled the depiction of household food insecurity status during the COVID-19 pandemic in Bangladesh. However, a significant limitation arose due to the unforeseen COVID-19 pandemic, which imposed various restrictions. These restrictions affected planned activities aimed at enhancing the effectiveness of livelihood support programs, resulting in suboptimal execution. Completing these activities adequately could have potentially further improved the effectiveness of such programs. Moreover, this study failed to consider a broad range of factors influencing household food insecurity, including geographical factors. Given that the study took place in rural areas abundant in natural food resources such as grass and leaves, which may influence returns from microfinance-based livelihood programs, the generalizability of findings to more resource-constrained urban areas may be limited. Despite these limitations, the study findings offer significant promise for the development of microfinance-based livelihood programs to support ultra-poor families in Bangladesh and other LMICs, including households with persons with disabilities.
Conclusion
The study highlights the significant impact of a microfinance-based livelihood program on mitigating household food insecurity among ultra-poor families of children with CP in Bangladesh. Despite facing higher levels of food insecurity exacerbated by sociodemographic factors and pandemic-induced economic disruptions, households enrolled in the IMCBR and CBR showed a notable decrease in food insecurity following the pandemic. These findings underscore the potential of microfinance-based livelihood programs to build resilience among the ultra-poor population, aligning with the government's efforts to enhance social safety-nets in Bangladesh. It offers valuable insights into the effectiveness of microfinance-based livelihood interventions and their potential to support vulnerable households in Bangladesh and similar LMICs. Moreover, it is recommended that integrating microfinance initiatives with long-term rehabilitation efforts for persons with disabilities could serve as a valuable strategy to address food insecurity and promote sustainable livelihoods in resource-constrained settings. Relevant ministries and bodies in Bangladesh, including the Ministry of Social Welfare, can integrate this understanding into their existing programs.
Supplemental Material
sj-docx-1-fnb-10.1177_03795721251348338 - Supplemental material for How a Microfinance-Based Livelihood Program can Combat Food Insecurity Among Families of Children With Cerebral Palsy in Bangladesh—Evidence From a Randomized Control Trial
Supplemental material, sj-docx-1-fnb-10.1177_03795721251348338 for How a Microfinance-Based Livelihood Program can Combat Food Insecurity Among Families of Children With Cerebral Palsy in Bangladesh—Evidence From a Randomized Control Trial by Nuruzzaman Khan, Mahmudul Hassan Al Imam, Israt Jahan, Mohammad Muhit, Nadia Badawi and Gulam Khandaker in Food and Nutrition Bulletin
Footnotes
Acknowledgments
The authors acknowledge the Research Foundation of Cerebral Palsy Alliance and international funding from CSF Global Bangladesh for providing funds to conduct the trial, the data of which we analyzed (Grant PG02218—Support CP Trial). The authors also extend sincere gratitude to the primary caregivers and children with CP for their valuable time and voluntary involvement in the SUPPORT CP trial. Additionally, the authors express heartfelt appreciation to the dedicated CSF Global team in Bangladesh for their diligent efforts and support.
Ethical Approval
This study has received approval from the Human Research Ethics Committee (HREC) of the Asian Institute of Disability and Development (reference number: Southasia-hrec-2019-5-03) and the National Research Ethics Committee (NREC) of Bangladesh Medical Research Council (BMRC) (reference number: BMRC/NREC/2016-2019/251; registration number: 224 17 06 2019). Additionally, it has been registered with the Australian New Zealand Clinical Trials Registry (ANZCTR) (registration number: ACTRN12619001750178; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=377428&isReview=true).
Authors’ Note
Consent to Participate: Prior to enrollment in the trial, informed written consent was obtained from primary caregivers of children with CP. Consent to Publication: Before enrollment in the trial, written informed consent was obtained from the primary caregivers of children with CP. The data analyzed in this study are nonidentifiable.
Author’s Contributions
Khan N and Khandaker G designed this study. Khan N analyzed the data and wrote the first version of the manuscript. Khandaker G, Imam MHA, Jahan I, and Muhit M critically reviewed the paper. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by CSF Global Bangladesh (grant number Grant PG02218—Support CP Trial).
Data Availability Statement
The authors were unable to provide the deidentified line-listed data due to potential sensitivities and identifying patient information contained therein. This decision is based on concerns regarding the sensitive nature of the topic and the risk of participant identification, particularly given the specific study location and unique characteristics of the participants. This restriction is mandated by the Asian Institute of Disability and Development (AIDD) Human Research Ethics Committee (HREC) as part of the approval process for the Bangladesh Medical Research Council ethics. Researchers seeking access to the data may contact the AIDD at the following address: AIDD, House # 76 & 78, Road # 14, Block B, Banani R/A, Dhaka – 1213, Bangladesh; Phone: +88-02-55040839; Email: disabilityasia@gmail.com.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.