
Abstract
Background
In Ethiopia, a school-based weekly iron and folic acid supplementation (WIFAS) program is being implemented to reduce burden of anemia in adolescent girls. While the program's impact on iron levels is well-studied, there is limited evidence on its effect on folate status.
Objective
The study was aimed at assessing the effect of the WIFAS on serum folate levels of school adolescent girls in Sidama Region, Southern Ethiopia.
Methods
A school-based cross-sectional study that compared the serum folate concentration among adolescent girls (10-19 years) enrolled in schools with (n = 165) and without (n = 165) the WIFAS program was carried out. Adolescent girls from both groups were sampled using multistage sampling procedure. The serum folate was compared between the 2 groups using mixed effects linear regression model.
Results
The study presented significantly higher mean (±standard deviation) serum folate concentration among girls from schools implementing the WIFAS program (9.76 ± 4.02 ng/mL) than their counterparts (7.38 ± 4.53 ng/mL) (β = 2.28, P < .001). The mean hemoglobin level was also higher in the WIFAS arm (13.07 ± 1.81 g/dL) than the comparator group (12.4 ± 1.93 g/dL (β = 0.86, P = .034).
Conclusion
The school-based WIFAS program showed positive association with serum folate and hemoglobin concentration in adolescent girls. This evidence should be used for advocating the scale-up of the program to areas with high prevalence of anemia and folic acid deficiencies.
Keywords
Background
Adolescence, the transitional phase between childhood and adulthood, is characterized by rapid physical, psychological, and social changes.1,2 Nutrition has a strong link to adolescent development playing a significant role in establishing lifelong health habits.3,4 Adolescent girls face heightened vulnerability to malnutrition due to increased requirements secondary to growth spurt, menstrual loss and possible teenage pregnancy.5,6 Malnutrition during adolescence has significant consequences for health and development3,5 including delayed sexual maturation, compromised immune function, reproductive health risks, and long-term impacts on cognitive abilities, education, and productivity.5,7
Epidemiological studies have highlighted that anemia is a major public health problem among women, including adolescent girls, worldwide.8,9 In 2019, the global prevalence of anemia among reproductive-age women was approximately 30%. 10 Likewise, more than 20% of reproductive age women in low- and middle-income countries were folate deficient.11,12 In Ethiopia, a significant prevalence of anemia (26%), iron-deficiency anemia (15%), and folate deficiency (57%) has been reported among adolescent girls. 13
Anemia among adolescent girls can be attributed to variety of causes. Nutritional anemia due to iron, folate, or vitamin B12 deficiency are likely common.8,14–16 Poor dietary intake, including inadequate consumption of iron-rich animal source foods, green leafy greens, and legumes, contribute to low iron levels. 17 Monthly menstrual blood loss leads to iron depletion specially in disadvantaged settings. 18 Repetitive infections and parasitic infestations may cause nutrient loss and hinder nutrient absorption, leading to anemia.16,19 Poverty, limited access to healthcare, and inadequate education on proper nutrition and hygiene practices worsen the problem.20,21
To address this issue, the World Health Organization (WHO) recommends intermittent supplementation of iron and folic acid (IFA) for school adolescent girls as a public health intervention in areas with an anemia prevalence exceeds 20%. 8 The intervention is a highly effective and quick means of improving iron and folate status, and reducing adolescent girls’ susceptibility to anemia. 22 Moreover, the intervention supplementation has been shown to be a cost-effective intervention for addressing anemia. 23
In Ethiopia, the Weekly Iron Folic Acid Supplementation (WIFAS) program is being implemented in selected schools as a public health intervention to address anemia among adolescent girls. 24 The effect of the intervention on iron status was evaluated before.22,25,26 However, there is an insufficient information regarding the impact of the intervention on the folate nutrition. This gap underscores the need for further investigation to thoroughly understand the comprehensive impacts of the WIFAS programs. Thus, this study was designed with major aims to determine the effect of WIFAS on serum folate level of the school adolescent girls in Sidama Region, Southern Ethiopia.
Methods and Materials
Study Setting
Sidama Region is one of the regional states of Ethiopia with a population size of nearly 5 million. The region is situated 273 km south of the capital Addis Ababa and has varying altitudes ranging from 500 to 3500 m above sea level. The livelihood of the population primarily relies on subsistence farming of enset, maize, wheat, barley, and teff. Coffee and khat are popular cash crops in the area. The region is administratively divided into 30 rural districts, 6 town administrations and a city administration.
In Ethiopia, the education system is organized into first (grades 1-4) and second cycle (grades 5-8) of primary education, followed by secondary education (grades 9-12). Since May 2022, the Sidama Region, in collaboration with Nutrition International and United Nations International Children's Emergency Fund, has been implementing a WIFA supplementation program. The WIFA supplement, containing 60 mg elemental iron and 0.4 mg folic acid, was implemented in conjugation with nutrition education to adolescent girls in selected schools in the region. It targets schools in the second cycle of elementary education and secondary education. Currently, the WIFAS program is being implemented in 9 of the 30 districts of the region. A total of 112 schools and 51 157 adolescent girls are benefiting from the program (22).
This study was conducted in 8 s cycle primary and secondary schools located in 4 rural districts (Malga, Dale, Hula, and Bona Zuria) of Sidama Region.
Study Participants and Eligibility Criteria
Adolescent girls enrolled in WIFAS implementing schools were considered as beneficiaries of the program. Conversely, those enrolled in non-WIFAS implementing school were taken as nonbeneficiaries. Adolescent girls, who were pregnant or in the postpartum period during the study, were excluded.
Sample Size Determination
An adequate sample size for estimating the effect of WIFAS program on folate level of the adolescent girls was calculated using the G*Power 3.1.9.4 program. 27 The assumptions taken into account were: 95% confidence level, 80% power, a one-to-one allocation ratio between the 2 groups, a medium effect size (d = 0.4), 1.5 design effect and 10% nonresponse rate. Ultimately, a sample size of 330 (165 each for both arms) was computed.
Variables of the Study
The exposure of interest was WIFAS status classified as beneficiary or nonbeneficiary. Adolescent girls were classified as WIFAS beneficiary and nonbeneficiary based their type of school enrollment. The main outcome of interest was serum folate status; while hemoglobin status was considered as a secondary outcome. Folate deficiency was defined as a serum folate level below 3 ng/mL or 6.8 nmol/L. 28 Hemoglobin status was categorized as anemic (Hb <12 g/dL), moderate anemia (8-12 g/dL), or severe anemia (<8 g/dL). 29
Adherence to WIFAS was determined based on the tablets consumed over the past 24 weeks as reported by the adolescent girls. Adolescent girls who took the complete set of tablets (24 tablets) within the previous 24 weeks were considered compliant, while those consumed 23 or less tablets were classified as noncompliant. The adherence status of each respondent was verified using records maintained by school health coordinators. 30
Adolescent girls’ nutritional knowledge on folate and anemia was assessed using 12 and 14 questions, respectively. Scores were assigned to each response. In this regard, correct responses were scored as 1, while incorrect ones were scored as zero, and a cumulative score was calculated for both domains. Nutritional knowledge is considered good for scores equal to or above the mean, and poor for scores below the mean.31,32
Body mass index-for-age z-score (BAZ) and height-for-age z-score (HAZ) were calculated based on the 2007 WHO reference values. Thinness was defined as a BAZ score below −2 standard deviations (SDs). Stunting referred to a HAZ score below −2 SDs. 33
The Productive Safety Net Program (PSNP) is a social protection initiative targeting food insecurity and poverty in vulnerable households through cash or food aid, public works, and community development interventions, categorizing households as enrolled (1) or not enrolled (0) based on economic vulnerability. 34
The study considered possible confounders such as father educational status, father's occupation, mother's occupation, family size, place of residence (urban vs rural), enrollment in PSNP, household wealth index, food insecurity status, dietary diversity score, girl's knowledge score on anemia, girl's knowledge score on folate, and hemoglobin level.
Sampling Procedure
This study utilized a multistage sampling technique. Initially, simple random sampling method was employed to select 4 districts, namely Malga, Dale, Hula, and Bona, from the total of 9 districts implementing the WIFAS in the region. Subsequently, 2 primary and junior schools (1—implementing and 1—not implementing the WIFAS program) were chosen from each of the 4 selected districts. In both groups, lists of enrolled adolescent girls and the study participants were selected using simple random sampling technique. The sample size was assigned to each group based on the probability proportion to size.
Data Collection Procedure and Instrument
Data were collected using a structured and pretested interviewer-administered questionnaire developed based on review of relevant literature. The questionnaire covered various aspects, including sociodemographic and economic information, dietary diversity, household food insecurity status, sanitation, and hygiene practices. The tool was initially developed in English and translated into Amharic by a proficient bilingual professional. It was subsequently backtranslated into English to assure consistency.
Dietary diversity was assessed according to the women dietary diversity score of the United Nation's Food and Agriculture Organization guideline, with respondents providing information on food consumption from 16 predefined food groups within the past 24 h. The overall dietary diversity score was calculated by summing the scores of all included food groups. 35
Household food security was evaluated using the Household Food Insecurity Access Scale, which examined the occurrence of 9 food insecurity-related events in the past 30 days. Based on the scale, households were classified as food secure or insecure. 36
Anthropometric measurements
Anthropometric measurements were taken following standard procedures and using calibrated equipment. To avoid interobserver variation, anthropometric measurements were collected by a trained and experienced nutritionist. The adolescent girl's height and weight were measured with her in light clothing and without shoes, using a standard SECA digital scale (Seca GmbH & Co. KG) for weight and a vertical wall measuring tape for height. Weight was measured to the nearest 100 g, and height was recorded to the nearest 0.1 cm.
Biological sample collection and laboratory analysis
Blood sample collection and laboratory analyses were carried out following standard procedures. A senior laboratory technologist drew 5 mL of venous blood from each adolescent girl. Hemoglobin concentration was measured in the field using a Hemocue photometer (Hb 301 + System) from venous blood. Hemoglobin concentrations were adjusted for altitude according to WHO standards. 29
The venous blood was allowed to settle for 40 min, centrifuged at speed of 4000 revolutions per minute for 5 min and serum was separated following standard procedure. The serum samples were then stored frozen at −20 °C and transported on dry ice to the International Clinical Laboratory Hawassa Hub for analysis. 28 Folate levels were determined using immune turbid metric methods with a clinical chemistry analyzer Cobas 6000 system (Roche Diagnostic GmbH). 37
Data Management and Analysis
Data were collected using KoboToolbox system and exported to STATA version 14.0 for data management and analysis. Categorical variables were summarized using frequency distributions, while numerical variables, after confirming normal distribution, were described using the mean and SD. The household's wealth index, a metrics of household living standard, was calculated using principal component analysis based on the ownership of valuable assets, housing conditions, and access to social services.
An independent sample t test was employed to compare the mean difference in serum folate and hemoglobin levels between the 2 groups. A mixed effect linear regression model with random intercept for school was applied to assess the association between the WIFAS program with serum folate and hemoglobin levels, while controlling for potential confounders. Prior to that, an intercept-only model was fitted and an intraclass correlation coefficient of 12.6%, which was above the minimum threshold of 5%, indicated for the mixed effect model.
The model assumptions (linearity, multicollinearity, normality, and homoscedasticity) were checked to be satisfied.38,39 The model fitness was assessed using Bayesian Information Criteria. Initially, the 2 groups were compared using χ2 or independent t test based on the nature of the variables. Potentially unbalanced variables (P < .25) were considered for multivariable adjustment. Accordingly, father educational status, father's occupation, mother's occupation, family size, place of residence, safety net program enrollment, household wealth index, food insecurity status, dietary diversity score, girl's knowledge score on anemia, and girl's knowledge score on folate were adjusted. Statistical significance was declared at a P value of <.05.
Anthropometric indices, specifically HAZ and BAZ, were generated using the WHO Anthro Plus software based on the WHO 2007 growth reference data.
Results
Sociodemographic and Economic Characteristics
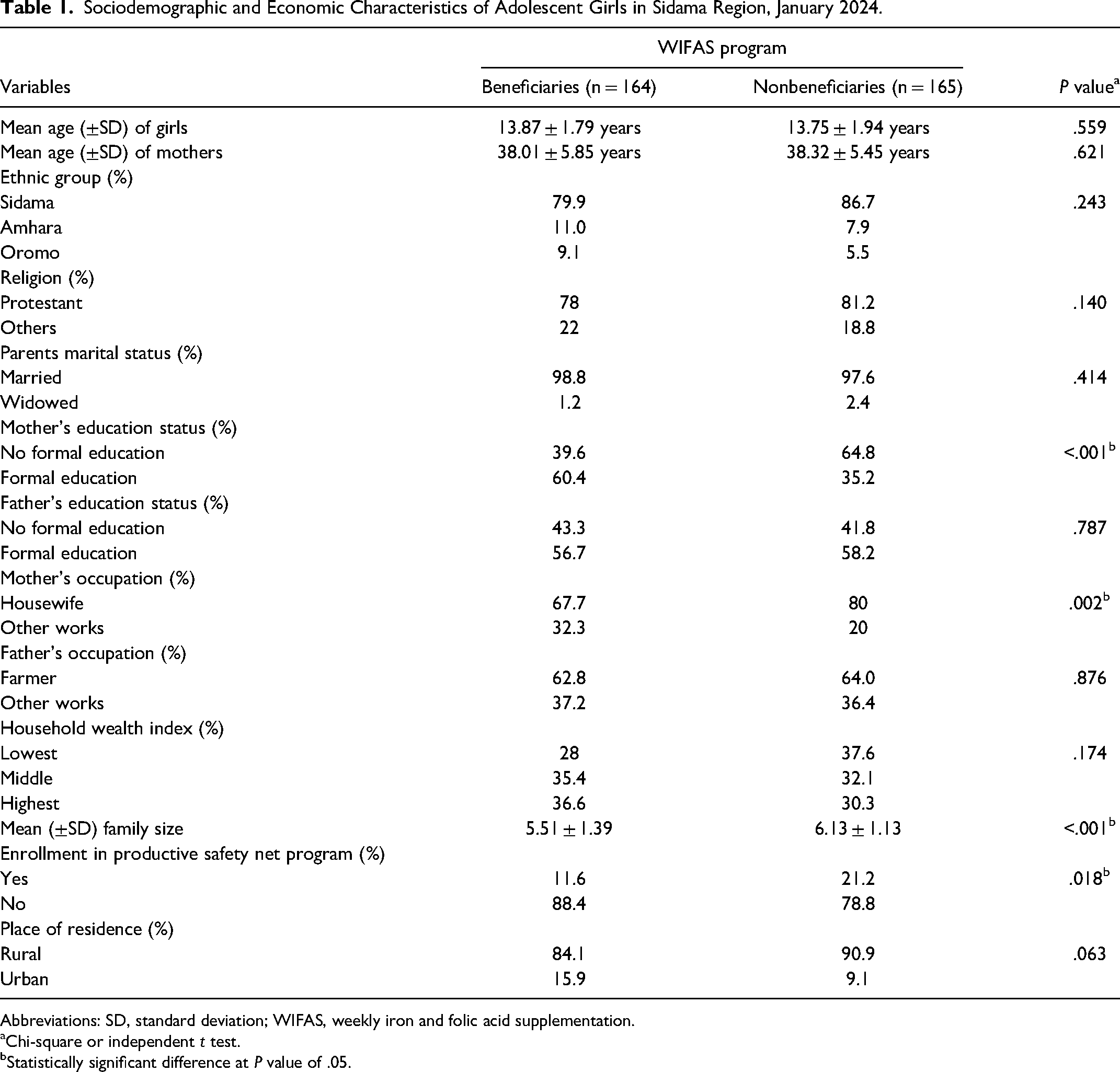
A total of 164 adolescent girls from WIFAS schools and 165 from non-WIFAS schools were enrolled. Of the respondents, 79.9% of WIFAS beneficiary girls and 86.7% of non-WIFAS beneficiaries were of Sidama ethnicity. Seventy-eight percent of respondents from WIFAS schools and 81.2% of respondents from non-WIFAS schools identified themselves as Protestant religion followers. Nearly all girls’ parents were married, with 97.6% at non-WIFAS schools and 98.8% at WIFAS schools. The mean (±SD) age of mothers was 38.01 ± 5.85 years for WIFAS beneficiary girls and 38.32 ± 5.45 years for nonbeneficiaries. The WIFAS beneficiary girls had a mean age of 13.87 ± 1.79 years, while nonbeneficiaries 13.75 ± 1.94 years (Table 1).
Sociodemographic and Economic Characteristics of Adolescent Girls in Sidama Region, January 2024.
Abbreviations: SD, standard deviation; WIFAS, weekly iron and folic acid supplementation.
Chi-square or independent t test.
Statistically significant difference at P value of .05.
Regarding mothers’ education, 60.4% of WIFAS beneficiary girls’ mothers had attended formal education, while 64.8% of nonbeneficiary girls’ mothers had no formal education. Slightly more than half of the girls’ fathers had attended formal education (56.7% WIFAS school, 58.2% non-WIFAS school). The majority of the mothers were housewives (67.7% WIFAS school, 80% non-WIFAS school). In both WIFAS beneficiary and non-beneficiary girls, around two-thirds of fathers were farmers (62.8% WIFAS, 64.0% non-WIFAS). Regarding household wealth, 28% of WIFAS beneficiary and 37.6% of nonbeneficiary girls were from poor households. The majority of families resided in rural areas (Table 1).
Among sociodemographic variables, significant differences were observed between the 2 groups in maternal education, mother's occupation, and family size (P < .05) (Table 1).
The PSNP enrollment varied significantly between beneficiary and nonbeneficiary households. Among the WIFAS beneficiary girls, 11.6% of the households were enrolled in the program, while the corresponding figure for nonbeneficiary girls’ households was 21.2% (Table 1).
Feeding Pattern and Girls’ Knowledge on Folate and Anemia
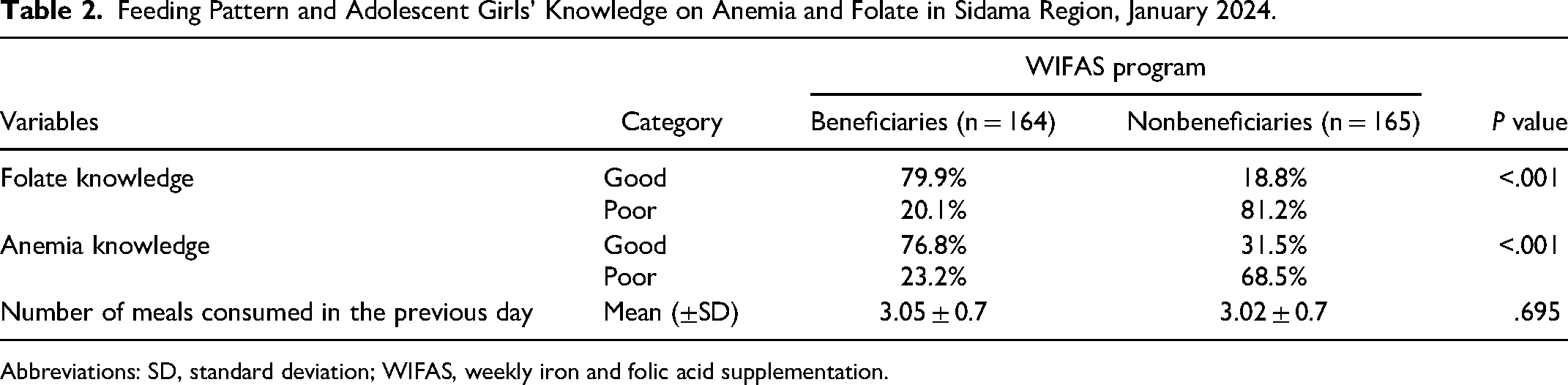
Weekly IFA supplementation beneficiary girls had significantly higher folate knowledge scores (5.05 ± 1.63) compared to nonbeneficiary ones (2.42 ± 1.61) (P < .001), with a mean difference of 2.63 (95% CI = 2.28-2.98). Similarly, WIFA beneficiary adolescent girls had significantly higher anemia knowledge scores (9.1 ± 2.2) compared to nonbeneficiary girls (6.2 ± 2.24), with a mean difference of 2.92 (95% CI = 2.44-3.41) (P < .001). About four-fifths (79.9%) of beneficiary girls had good knowledge of folate, while a mere 18.8% of nonbeneficiary girls possessed similar knowledge regarding folate. Among beneficiary adolescent girls, 76.8% had good knowledge of anemia, while only 31.5% of nonbeneficiary girls did (Table 2).
Feeding Pattern and Adolescent Girls’ Knowledge on Anemia and Folate in Sidama Region, January 2024.
Abbreviations: SD, standard deviation; WIFAS, weekly iron and folic acid supplementation.
The mean (±SD) number of meals consumed per day was 3.05 ± 0.7 for WIFAS beneficiary girls, and 3.02 ± 0.7 for nonbeneficiary girls, with no statistically significant difference between the 2 groups (Table 2).
Food Security, Dietary Diversity, and Anthropometric Status
The WIFAS nonbeneficiary girls were more food insecure (45.5%) compared to beneficiary girls (20.7%), with a statistically significant difference (P < .001). Starchy staples were the most consumed food group in the study area, with a mean dietary diversity score of 4.8 ± 1.49. Weekly IFA supplementation beneficiary girls had a higher mean (±SD) DDS compared to nonbeneficiary girls (5.05 ± 1.50 vs 4.31 ± 1.40) (P < .001). The mean (±SD) BAZ score was higher among beneficiary girls (−0.59 ± 1.12) compared to nonbeneficiary girls (−0.95 ± 1.28). Similarly, beneficiary girls had higher mean (±SD) HAZ (−0.88 ± 0.87) compared to nonbeneficiary girls (−1.13 ± 0.99). Overall, the observed mean differences in DDS, BAZ, and HAZ favored WIFAS beneficiary girls (Table 3). Girls from WIFAS nonbeneficiary schools had higher rates of stunting (55.1%) and thinness (43.3%) compared to girls from beneficiary schools (29.7% and 25%, respectively), with a significant difference (P < .001) (Table 3).
Food Security, Dietary Diversity, and Anthropometric status of Adolescent Girls in Sidama Region, January 2024.
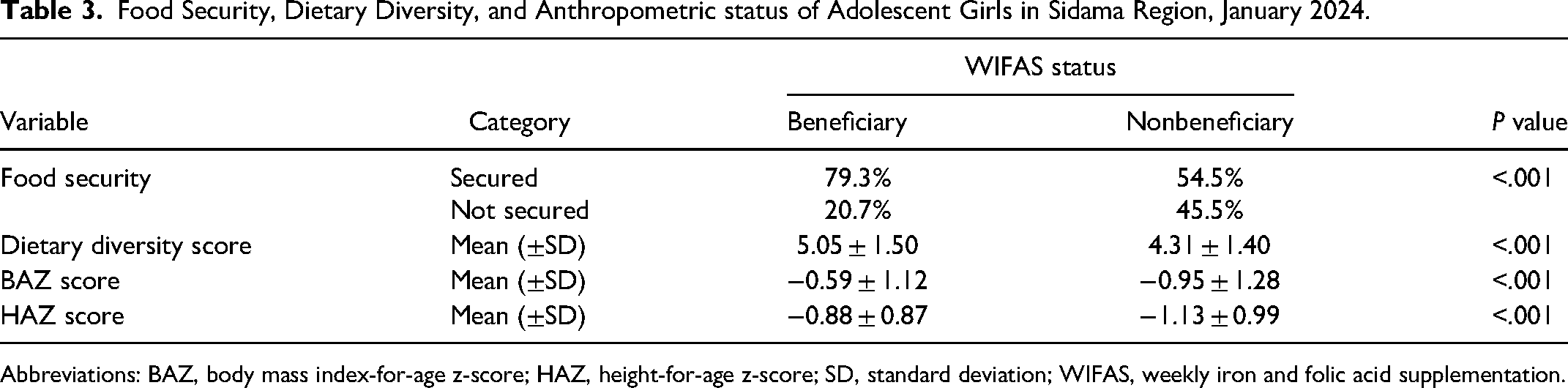
Abbreviations: BAZ, body mass index-for-age z-score; HAZ, height-for-age z-score; SD, standard deviation; WIFAS, weekly iron and folic acid supplementation.
Adherence to Weekly IFA Supplementation
The majority (81.1%) of WIFAS beneficiaries took a complete set of 24 tablets in the previous 6 months. However, a small percentage (18.9%) did not take the full set of tablets primarily due to fear of side effects. About half (49.4%) of WIFAS-beneficiary girls and over one-third (43.6%) of nonbeneficiary girls took deworming tablets in the last 6 months.
Prevalence of Folate Deficiency and Anemia Among Adolescent Girls
Among adolescent girls, serum folate levels ranged from 1.16 to 18.1 ng/mL, with a mean (±SD) value of 8.56 ± 4.44 ng/mL. Weekly IFA supplementation beneficiary girls had significantly higher serum folate levels compared to nonbeneficiary girls (9.76 ± 4.02 ng/mL vs 7.38 ± 4.53 ng/mL) (P < .001) (Table 4). The prevalence of folate deficiency among adolescent girls was 20.1% (95% CI = 15.9%-24.8%). Folate deficiency was more prevalent in nonbeneficiary girls. Hemoglobin levels ranged from 9.1 g/dL to 18.0 g/dL, with a mean value of 12.73 ± 1.90 g/dL. Beneficiary girls had a higher mean hemoglobin level compared to nonbeneficiary girls (13.30 ± 1.76 g/dL vs 12.27 ± 1.93 g/dL) (P < .001) (Table 4). The prevalence of anemia among adolescent girls was 41% (95% CI = 35.7%-46.6%). The prevalence of anemia was higher in nonbeneficiary girls compared to beneficiary girls (Figure 1).
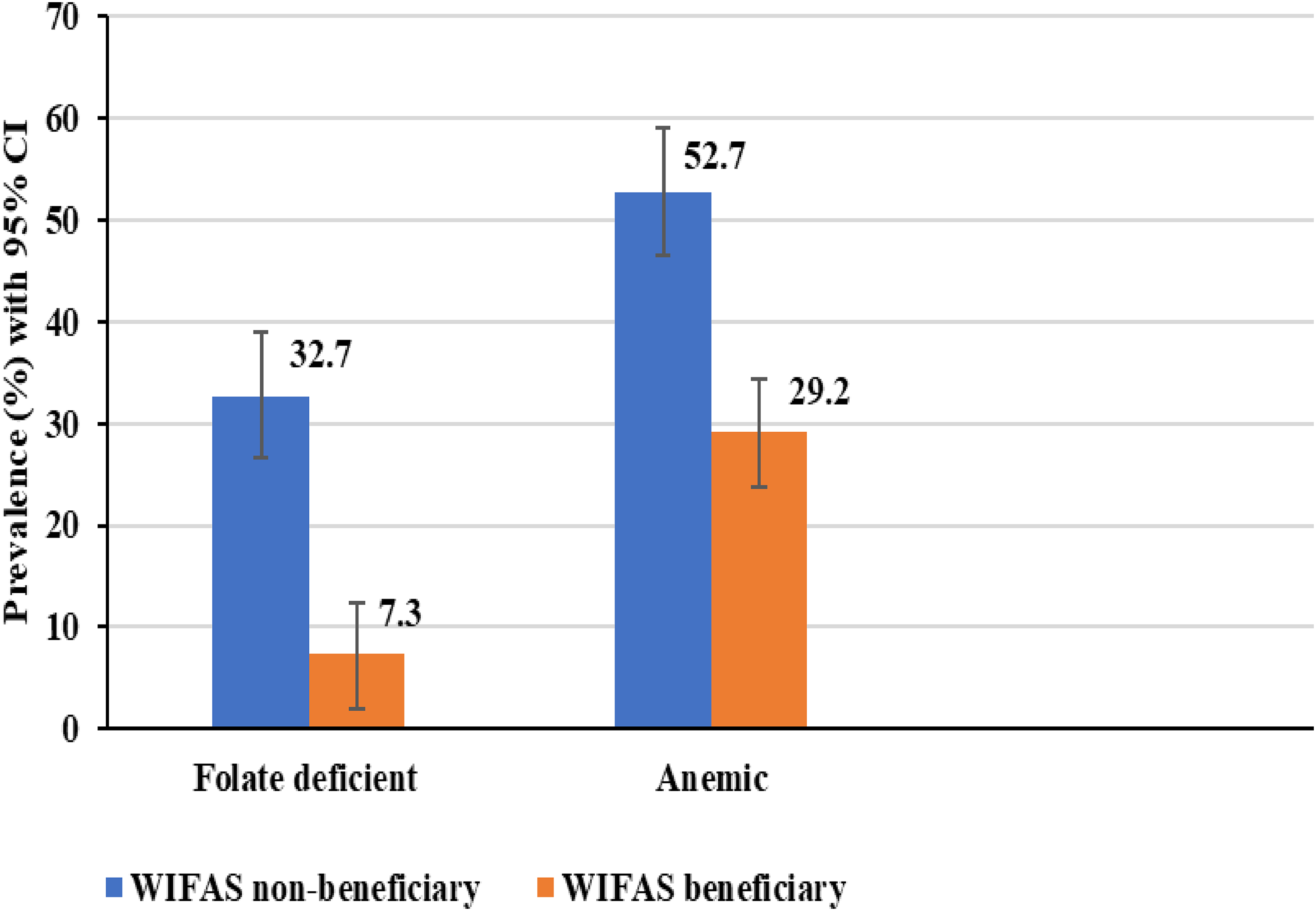
Prevalence of folate deficiency and anemia among adolescent girls in Sidama region, January 2024.
Serum Folate and Hemoglobin Levels of Adolescent Girls in Sidama Region, January 2024.

Abbreviations: SD, standard deviation; WIFAS, weekly iron and folic acid supplementation.
Effect of WIFAS on Serum Folate and Hemoglobin Status
The mixed effects linear regression model showed a significant positive effect of WIFAS supplementation on serum folate levels (β = 2.28, P < .001) (Table 5).
Effect of Weekly Iron and Folic Acid Supplementation on Serum Folate and Hemoglobin Level Among Adolescent Girls in Sidama Region, January 2024.a
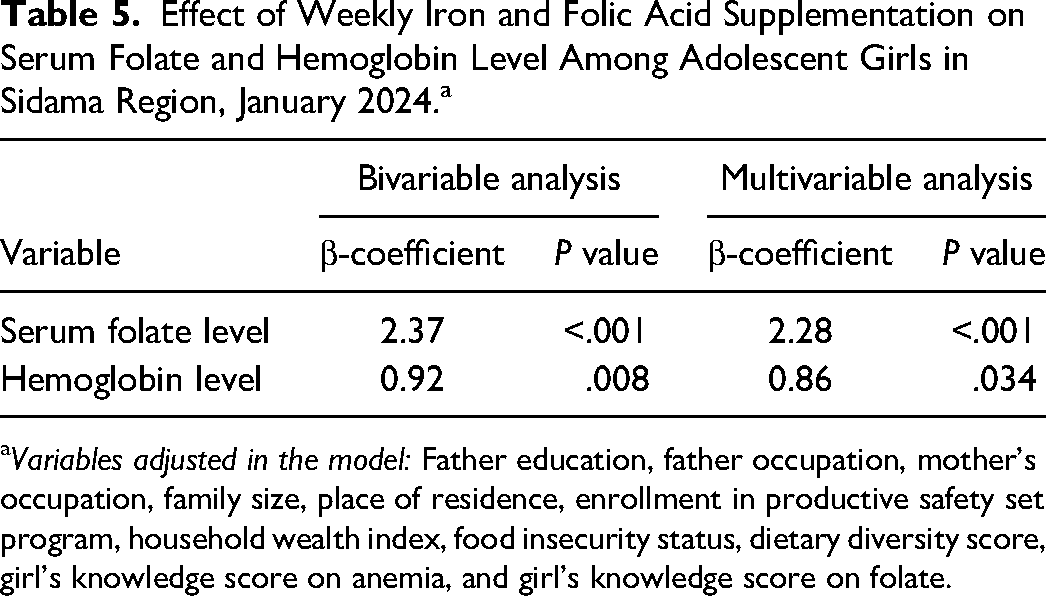
Variables adjusted in the model: Father education, father occupation, mother's occupation, family size, place of residence, enrollment in productive safety set program, household wealth index, food insecurity status, dietary diversity score, girl's knowledge score on anemia, and girl's knowledge score on folate.
Similarly, to determine the effect of WIFAS on hemoglobin level, a mixed-effects linear regression model was fixed. Hemoglobin levels were treated as the dependent variable, and school was included as a random effect. After adjusting for the same variables mentioned earlier as fixed effects, the model revealed a significant effect of WIFAS on hemoglobin levels (β = 0.86, P = .034). A significant difference in mean hemoglobin levels was observed between WIFAS beneficiaries and nonbeneficiaries (Table 5).
Discussion
This study assessed the effect of WIFAS program on serum folate concentration in adolescent girls of Sidama Region. The WIFAS significantly improved serum folate concentration and hemoglobin levels, reducing folate deficiency and anemia in girls.
The study presented a significant positive association between WIFAS and serum folate levels. A significant 2.37 ng/mL mean difference in serum folate level among the girls was identified in favor of the WIFAS beneficiaries. Similarly, folate deficiency was more prevalent among nonbeneficiary girls (32.7%) compared to their counterparts (7.3%). Studies from southern Ethiopia 25 and Nepal 40 concluded likewise. This can be explained by the fact that WIFA supplement ensures adequate folate availability, optimizes folate utilization, and enhances red blood cell function.
Our study identified a significant association between hemoglobin levels and WIFAS intake among adolescent girls. The WIFAS beneficiary girls were found to have higher mean hemoglobin and serum folate levels compared to their counterparts (a mean difference of 0.67 g/dL), indicating a positive effect of supplementation on this nutrient levels. Also, the prevalence of anemia among WIFAS nonbeneficiary girls was significantly higher than beneficiary girls (50.9% vs 31.1%). These findings align with studies conducted in Southern Ethiopia, 25 Western Kenya, 41 Ghana, 22 Nepal,40,42 Vietnam, 43 and India44,45 which also reported improvements in the indicated nutrients level, as well as a reduced prevalence of anemia among WIFAS users. This may be due to the fact that supplemented IFA improve hemoglobin levels in adolescent girls by addressing iron deficiency, supporting red blood cell production, and enhancing serum folate levels through providing additional folate for metabolic processes.
Starchy staples were the most consumed food group in the study area, with a mean dietary diversity score of 4.8. Consumption of a less diversified diet was more prevalent in nonbeneficiary (55.1%) girls compared with beneficiary (36.6%) groups. This finding was consistent with previous studies conducted in Bahr Dar City of Ethiopia, 46 Eastern Ethiopia, 47 Mozambique, 48 low- and middle-income countries, 49 and Germany. 50 The explanation for this could be that a lack of variety in their diet or limited dietary choices among school adolescent girls increases their susceptibility to micronutrient deficiencies, potentially resulting in low serum folate levels.
Food insecurity was a significant public health problem in the study area, affecting 33.1% of the households. We also observed differences in girls’ serum folate and hemoglobin levels based on household food security status. More than half (56%) of the folate-deficient and nearly two-thirds (64.2%) of the anemic girls came from food-insecure households, demonstrating statistically significant differences between the groups. This disparity may be attributed to the fact that food insecurity often results in reduced dietary variety and limited food choices, thereby increasing the likelihood of micronutrient deficiencies among adolescent girls and potentially leading to low levels of serum folate and anemia. 51
The adherence to supplemented WIFA tablets was assessed crucial for the success of the program. In this study, 81.1% of WIFAS beneficiaries consumed the complete set of 24 tablets in the previous month, indicating high adherence. However, a small percentage (18.9%) of beneficiary girls did not take the full set of tablets due to fears of experiencing side effects (stomachaches and nausea). Fear of side effects was one of the frequently reported causes of low adherence among adolescent girls to WIFAS programs. It poses a potential threat to the success of the program, preventing it from achieving its objective of addressing anemia among adolescent girls. 30
The strength of this study was the utilization of a comparative cross-sectional design to evaluate the effect of the WIFAS program on serum folate levels, which had not been previously investigated in the country. However, due to the observational nature of the study design, systematic baseline differences between the 2 groups could not be excluded. Besides, residual confounders stemming from unaddressed variables might have impacted the results. The use of nonstandardized nutritional literacy assessment tools may introduce measurement errors, and the study did not adjust for the actual intake or iron and folate status. Further research is needed to investigate the long-term effects of the WIFAS program and determine its sustained benefits.
Conclusion
The study demonstrated the beneficial impact of a school-based WIFAS program. It showed that the implementation of the program, along with nutrition education, resulted in significant improvements in serum folate levels and blood hemoglobin level among school adolescent girls in Sidama Region. Also, the program positively affected dietary diversity, and knowledge on folate and anemia.
Recommendation
Sidama Regional State Health Bureau, in collaboration with interested stakeholders, should expand the WIFAS program complemented with nutrition education to all schools found in the region to control anemia and improve the nutritional status of adolescent girls. Conjugating supplementation with nutrition education could significantly improve compliance.
Footnotes
Acknowledgments
The authors are grateful to Hawassa University, the Office of the President of the Sidama National Regional State, and the Norwegian Agency for Development Cooperation (NORAD) program for funding this study. The authors also appreciate the Education Offices of Malga, Dale, Hula, and Bona Zuria Districts, as well as the Directors of selected primary and junior schools. The authors sincerely thank the study participants, as well as the dedicated data collectors and supervisors who made this research possible.
Authors’ Contribution
A.B. implemented the study, analyzed the data, and drafted the manuscript. T.B. formulated the research question, designed and supervised the study, and finalized the manuscript. S.G. formulated the research question, designed the study, supervised the study, and finalized the manuscript. All authors reviewed the manuscript for important intellectual content and approved the final version for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study adhered to the guidelines outlined in the Declaration of Helsinki during its execution. The Institutional Review Board (IRB) of College of Medicine and Health Science, Hawassa University granted ethical clearance for this study (Protocol Number-IRB/026/16, Date-12/12/2023). Written informed consent was obtained from every respondent (mothers or adolescent girls) following a thorough explanation of the study objective. The study participants’ information was kept confidential using pseudonymous codes.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Hawassa University, Norwegian Agency for Development Cooperation (NORAD) and the Sidama National Regional State President Office.