
Abstract
Background:
Crucial gaps persist in knowledge, attitude, and practice (KAP) of adolescent girls that affect anemia and linear growth failure.
Objective:
To understand the role of KAP as a risk factor of anemia and linear growth problem in adolescent girls.
Methods:
We conducted a cross-sectional survey of 335 adolescent girls selected by clustered random sampling. The KAP questionnaire had 18 variables consisting of 9 knowledge, 3 attitude, and 6 practice components. Twelve variables addressed nutrition, dietary diversity, and health environments related to both anemia and stunting. The questionnaire was adapted from the 2014 Food and Agriculture Organization nutrition-related KAP guidelines for anemia. Dietary practice was evaluated from 2-day 24-hour recalls and a semi-quantitative food-frequency questionnaire. Associations between KAP and anemia, and height-for-age z-score (HAZ), were analyzed using multivariate logistic and linear regression models, respectively.
Results:
The mean hemoglobin (Hb) level was 119.7 g/L, with 44% of the adolescent girls being anemic (Hb < 120 g/L) and mean height was 151.0 cm with 25% being stunted (HAZ < −2 standard deviation [SD]). The median KAP score was 7 and ranged from 3 to 10. Low to moderate KAP scores were not significantly associated with being anemic (adjusted odds ratio [AOR] = 1.26; P = .43), however 1-point KAP score increment was associated with an increase of HAZ by 0.037 SD (P = .012).
Conclusions:
The KAP related to diet and healthy environments was not associated with anemia prevalence, but was positively associated with increased HAZ among adolescent girls. Strategy to reduce anemia risk in this population should combine KAP improvement with other known effective nutrition interventions.
Background
Anemia among adolescents is a global public health burden. 1 Indonesian National Health Survey (INHS) or Riskesdas 2018 reported that the national prevalence of anemia among adolescents aged 5 to 14 and 15 to 24 years was 26.8% and 32%, respectively. Adolescent girls are considered to be more at risk of anemia as they have high nutritional demands to account for their growth acceleration, sexual maturation, and future pregnancy. 3,4 Increase in growing body tissue and red cell mass causes a double iron requirement. Even when the growth spurt has passed, the risk of anemia is still high due to menstruation. 5 Furthermore, the aspect of future pregnancy becomes essential in low-resource settings where early marriage followed by early pregnancy is common. 6 In 2018, 59% of Indonesian adolescent girls aged between 10 and 19 years reported to have ever experienced pregnancy or are currently pregnant. 2 This high prevalence of adolescent pregnancies may increase fetal and infant morbidity and mortality given the high burden of anemia and micronutrient deficiencies in this population. 5
Anemia-stunting coexistence is prevalent in many low- and middle-income countries (LMICs). 7 -9 Shared factors, including poverty, limited education and access to knowledge, inadequate dietary and nutrient intake and infectious diseases, are suggested to contribute to anemia and stunting co-occurrence. 10 -14 In 2018, the prevalence of stunting among adolescent girls in Indonesia reached approximately 18.5%. 2 Stunting is associated with reduced growth potential, neurodevelopment and cognitive function, and increased future risks of chronic diseases. 15,16 Moreover, stunting bears intergenerational effects, as this condition in pregnancy contributes to maternal and fetal complications affecting health in the future. 17
Knowledge is an important factor, which is a cornerstone of attitude and practice changes to prevent anemia. 18 Limited access to knowledge has been postulated as one of the distal causes of the increase prevalence of anemia and stunting. 19 Greater nutrition-related knowledge, attitude, and practices (KAP) toward anemia were reported to enhance health behavior 20 that potentially helps prevent the occurrence of other health problem with shared risk factors, such as linear growth failure in adolescents. 11,21,22
Understanding the role of KAP in anemia is useful in capturing important messages to avoid miscommunication and skepticism toward the necessity and side effects of compliance with iron supplementation. Many studies have focused on descriptive information on KAP toward anemia, 23 -25 but its role on nutritional outcome is limited. Crucial gaps persist in KAP of adolescent girls that affect anemia and linear growth failure. Therefore, this research aimed to capture information on adolescent girls’ KAP toward anemia and analyzed its association with anemia and linear-growth outcome. The study result can help design preventive intervention programs and policies for improving adolescent girls’ KAP toward anemia.
Materials and Methods
Study Design and Participants
A cross-sectional study was conducted in 2016 among 335 school-going adolescent girls aged 12 to 19 years, who had menarche, and resided in Cimahi, Purwakarta, and Bandung Barat districts of West Java province as described previously elsewhere. 26 Only school-going girls were included, and these districts were selected based on the availability of a structured school-based iron-folic acid (IFA) supplementation program implemented in collaboration with the Indonesian government.
The participants’ recruitment involved permission and approval by the local government of West Java province to survey in the area at all levels, from both the provincial and district health offices, and at a subdistrict and village level. Participants and their parents were informed about the study method and asked for written informed assent and consent, respectively. Participants who were excluded were those who did not yet have menarche, resided outside of the sampling area, refused to give consent, and/or were unable to complete the study assessments.
Those participants recruited were selected in a 2-stage cluster sampling design, as previously described. 26 Clusters were selected based on the 2015 population census; 34 villages were selected by adopting a probability proportional to population size method, while households were listed from the chosen cluster to prepare a sampling frame for school-going girls in the intended age-group. The required number of respondents (10 in each cluster) was randomly selected from the households’ sampling frame. A village was divided into segments, each comprising of 200 households. One segment was then randomly selected from several segments in each village. If the desired number of households was not available in the selected segment, another randomly selected segment was covered to obtain the required number of respondents.
Theoretical Model
The theoretical perspective of this study is based on United Nations International Children’s Emergency Fund’s causal framework for child malnutrition and Agustina et al for maternal influence on the morbidity in children that was modified from Mosley, and Chen’s model for child mortality determinants in developing countries (Figure 1). 27,28 Socio-demographic factors, such as the district of residence, age, family type, education, and head of household's occupation; access to the KAP source of information; food security and policies are recognized as distal factors to anemia that may affect previous maternal and child care practices and the current adolescents’ KAP toward anemia, as intermediate factor. These factors will affect the diet quality, access to nutrient-rich diets, health, hygiene, sanitation, and underlying diseases as the proximal factors contributing to iron and other micronutrient deficiencies. Iron and other micronutrient deficiencies are risk factors for anemia. Meanwhile, the same factors, such as diet quality, health, hygiene, sanitation, and previous history of childhood undernutrition and micronutrient deficiencies may also affect future linear growth. 11,28 -30 The study observed the baseline data on KAP toward anemia, the current anemia and HAZ status of the adolescent girls.
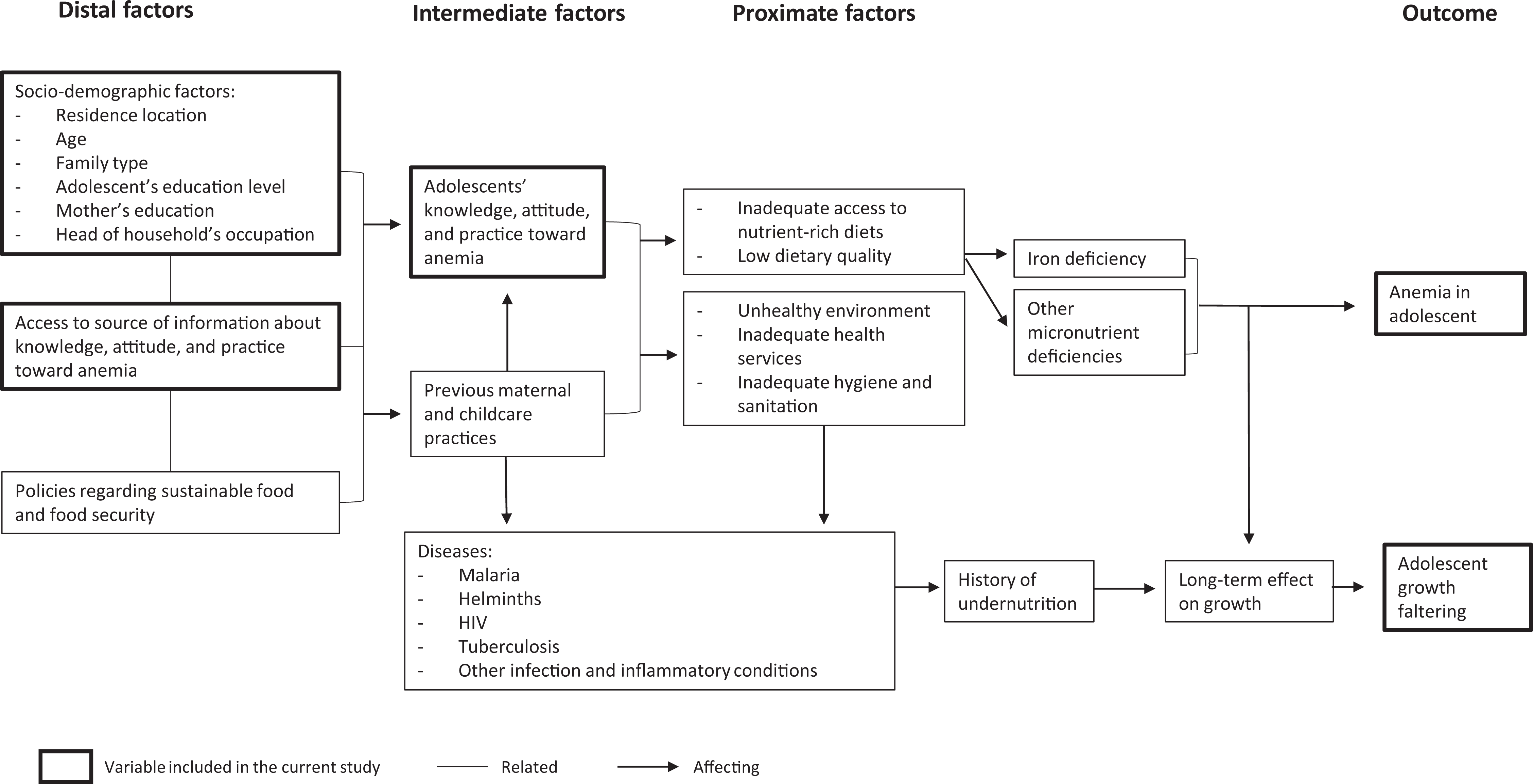
Theoretical framework of determinants of anemia and growth failure in adolescents. Based on the UNICEF framework of the determinants of child undernutrition, 28 the USAID Anemia Task Force conceptual framework, 30 and the WHO and the UNICEF joint statement on anemia. 29 UNICEF indicates United Nations International Children’s Emergency Fund; USAID, US Agency for International Development; WHO, World Health Organization.
Data Collection
The field enumerators interviewed the school-going adolescent girls at home independently from their mothers using a structured questionnaire on KAP toward anemia that was based on the 2014 Food and Agriculture Organization of the United Nations nutrition-related guidelines for iron deficiency anemia (IDA; Table 1). 31 Before data collection, the developed and translated KAP questionnaire was pretested in 2 villages that had not been included in the survey area. The enumerators were trained to undertake the interview correctly to minimize inter-interviewers bias. Questions regarding socio-demographic and household socio-economic conditions were also included in the interview. Among the socio-demographic characteristics were district of residence, family type, age, and education level. Information on the mother’s education and household head’s occupation was taken as proxies for household socio-economic conditions.
Determination of Score for Knowledge, Attitude, Practice Questionnaires Based on FAO Guidelines among School-Aged Children.a
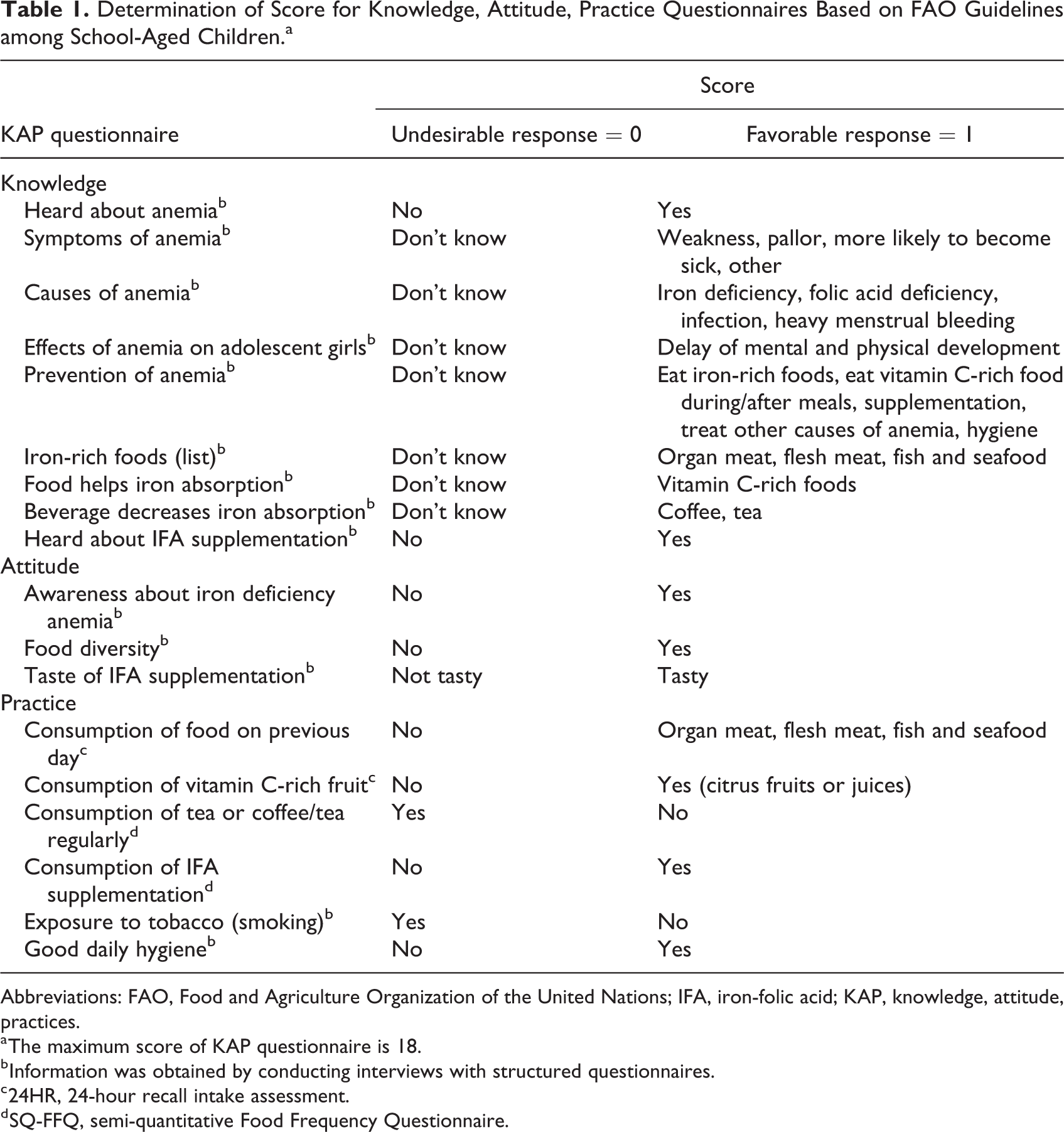
Abbreviations: FAO, Food and Agriculture Organization of the United Nations; IFA, iron-folic acid; KAP, knowledge, attitude, practices.
a The maximum score of KAP questionnaire is 18.
b Information was obtained by conducting interviews with structured questionnaires.
c 24HR, 24-hour recall intake assessment.
d SQ-FFQ, semi-quantitative Food Frequency Questionnaire.
The capillary fingerpick blood was drawn to measure the hemoglobin levels of adolescent girls in the field using a HemoCue201TM portable device. This device consists of a disposable microcuvette containing a reagent in a single purpose and designed photometer as applied elsewhere. 26 Anemia was defined according to the World Health Organization (WHO) criteria as hemoglobin level of <120 g/L, further categorized into mild (110-119 g/L), moderate (80-109 g/L), and severe (>80 g/L). The hemoglobin value was adjusted using the recommended altitude and smoking exposure adjustment. 32
The adolescent girls’ heights were measured at the village office or community gathering place by a trained nutritionist, using Shorr board fixed to the wall with a precision of 0.1 cm. Height was measured in a standing position without any footwear. The results were then plotted on the 2007 WHO growth chart for HAZ. 33 Linear growth failure or stunting was defined as HAZ < −2.0 SD. 34
Information on the actual nutrient intake was collected via a 2-day-repeated-24-hour recall; meanwhile, iron intake and habitual consumption data were measured from a semi-quantitative Food Frequency Questionnaire. The source of information about anemia was collected using an open-ended question. Identified sources of information were peers and family members, teachers and health care workers, mass media, and social media. No prior anemia prevention education had been given to the participants.
Measure of KAP
The total components of knowledge consisted of 9 variables: (1) heard about anemia, (2) symptoms of anemia, (3) causes of anemia, (4) effect of anemia on adolescent girls, (5) prevention of anemia, (6) iron-rich foods, (7) foods that help iron absorption, (8) beverages that decrease iron absorption, and (9) heard about IFA supplementation. The attitude questionnaire included 3 variables: (1) awareness about IDA, (2) food diversity, and (3) taste of the IFA supplementation; meanwhile, the practice questionnaire included 6 variables: (1) consumption of iron-rich foods on the previous day, (2) consumption of fruit high in vitamin C, (3) tea or coffee consumption, (4) IFA supplementation, (5) exposure to tobacco, and (6) hygiene practice contributing to the practice questionnaire. Each variable was scored as 0 or 1, with 1 representing a favorable response (Table 1). Finally, all variables were summed up into a total of 18.
The Cronbach α reliability coefficient of the KAP questionnaire was 0.70. This reliability coefficient is considered acceptable in most social science research studies and situations. 35
Data Analyses
Data quality management was carried out continuously from the field to the head office for data cleaning and analysis. The validity of the data was checked to ensure the data were correctly taken. The data were analyzed using SPSS for Windows 20.0. The normal distribution of continuous data was verified according to the Shapiro-Wilk test of normality. Frequency, mean, and SD were computed for normally distributed data. Median and interquartile range of 25th to 75th percentiles were presented for not normally distributed data. Chi-square and Pearson correlation were carried to investigate the correlation between anemia and stunting, as well as hemoglobin value and HAZ score.
Binary logistic regression was performed to identify the significant differences between 2 nominal groups with a set of significant P value <.05. Further, KAP scores were categorized into 3 groups based on the tertile values. Confounding factors were identified by performing logistic regression controlling for the socio-demographic and household socio-economic characteristics with anemia and linear growth failure outcomes and by comparing with P value <.25. Multivariate binary logistic regression was performed to identify the association between KAP and anemia prevalence with a set of significant P value <0.05. Multivariate linear regression model was also performed to assess the association of KAP score with hemoglobin levels and HAZ score.
Ethical Consideration
The Ethical Committee of the Faculty of Medicine Universitas Indonesia approved the research protocol (Ethics number: 72/UN2.F1/ETIK/2016), which guided the blood sample collection, testing methods, devices, and disposal procedures conducted in the field.
Results
Table 2 presents the general characteristics of 335 adolescent girls included in this study. Nearly half of the adolescent girls were anemic, with 23% mild, 19.4% moderate, and 1.8% severe anemia. The mean height was 151.0 cm, ranged from 136.4 cm to 180.3 cm, 25% were stunted. Most girls were Sundanese (93%), with a median age of 15 years. Approximately 63% of them were in junior high school, with the remainder at senior high school. Almost all of the adolescent girls used mass and social media as sources of anemia information. A few were informed about anemia by school and health staff (22%), their families, and their peers (17%). There was a correlation between hemoglobin value and HAZ score (P = .048, r = .379), however anemia and stunting were not associated (P = .325). (data not shown).
General Characteristic of the Adolescent Girls in West Java and Their Associations with Anemia (Hemoglobin < 120 g/L) and Stunting (HAZ < −2 SD) Prevalence.a
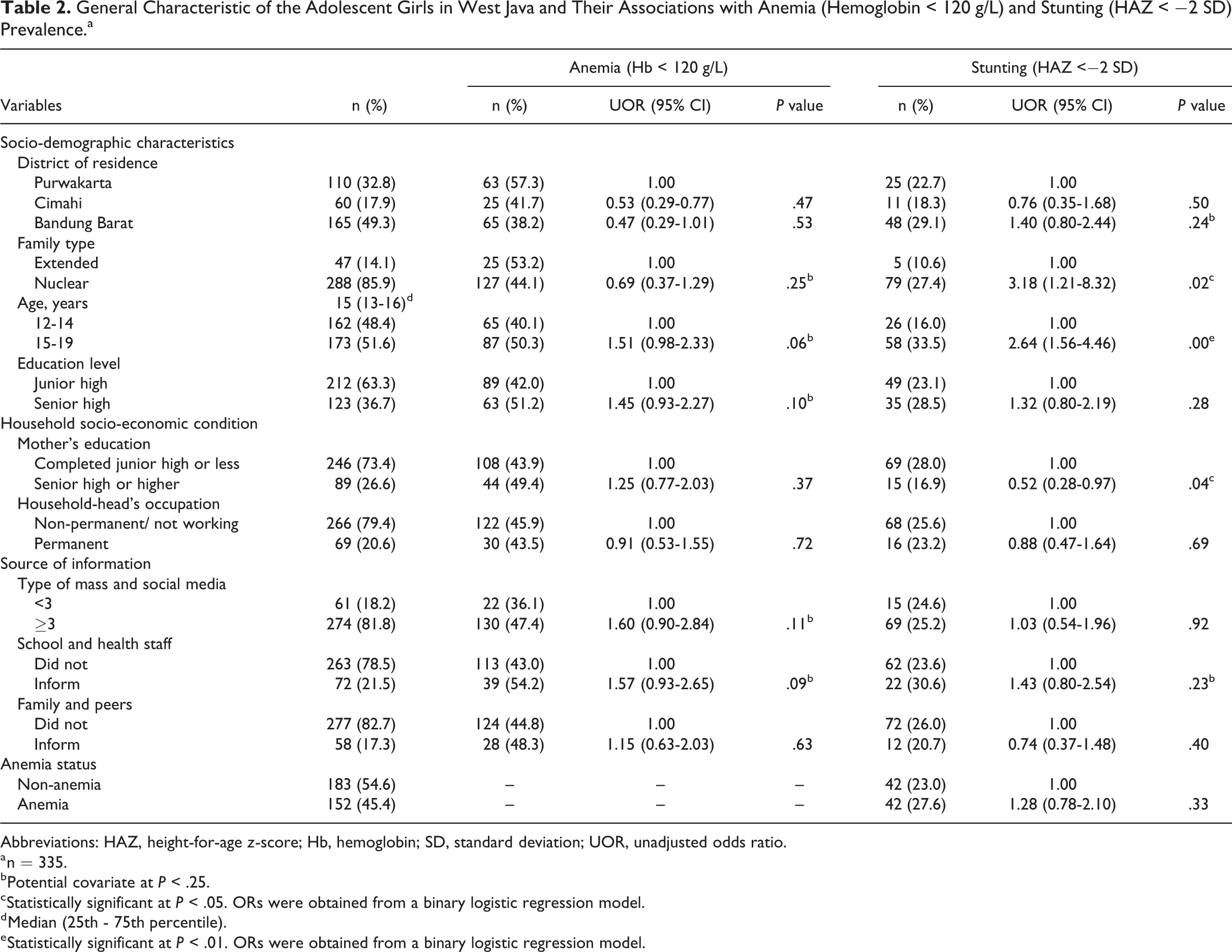
Abbreviations: HAZ, height-for-age z-score; Hb, hemoglobin; SD, standard deviation; UOR, unadjusted odds ratio.
a n = 335.
b Potential covariate at P < .25.
c Statistically significant at P < .05. ORs were obtained from a binary logistic regression model.
d Median (25th - 75th percentile).
e Statistically significant at P < .01. ORs were obtained from a binary logistic regression model.
Some variables in Table 2 were identified as covariates for anemia (P < .25): family type, the adolescent’s age and education level, the number of mass and social media as a source of information, and being informed about anemia by school and health staff. Socio-demographic factors associated with linear growth failure were adolescent girls who lived in a nuclear family and were among the “15 years and older” age-group. The factors mentioned above had a significantly higher risk of being stunted compared to those who lived with an extended family and were in the “younger than 15 years” age-group (odds ratio [OR] = 3.18, 95% CI = 1.21-8.32, P = .02 and OR = 2.64, 95% CI = 1.56-4.46, P = .00, respectively). Girls who had mothers with a senior high or higher education had significantly twice the lower risk of having stunting (OR = 0.52, 95% CI = 0.28-0.97, P = .04). District of residence and being informed about anemia by school and health staff were also identified as covariates for stunting.
Table 3 indicates that more than 60% of the adolescent girls had heard about anemia. Almost all of those who had heard of anemia knew about at least 1 symptom of anemia. Some were also able to identify the cause of anemia and its prevention; however, only around a third of those who had heard of anemia knew about its effects. The median (range) of the total KAP score was low, which was 7 (3-10) of 18 (maximum score). There was a strong correlation between knowledge and attitude scores. Knowledge and practice as well as attitude and practice scores were also significantly correlated (Supplementary 1). Some characteristic variables had higher odds of having a high total KAP score: attended senior high education level, were 15 to 19 years old, had mothers with a senior high or higher education, were in a setting where the head of the household had a permanent job, and were informed about anemia by school and health staff and their family and peers (Supplementary 2). However, none of the individual KAP variables were associated with anemia prevalence after adjusting for the covariates (Table 3). There was no association between the KAP score category based on the tertiles of total KAP scores with anemia prevalence (Table 4). The overall KAP scores were also not associated with hemoglobin value, however, access to media remained as an associated confounding factor in multivariate linear regression model (Supplementary 3).
Knowledge, Attitude, and Practices toward Anemia as Factors Associated with Anemia Prevalence among Adolescent Girls.a
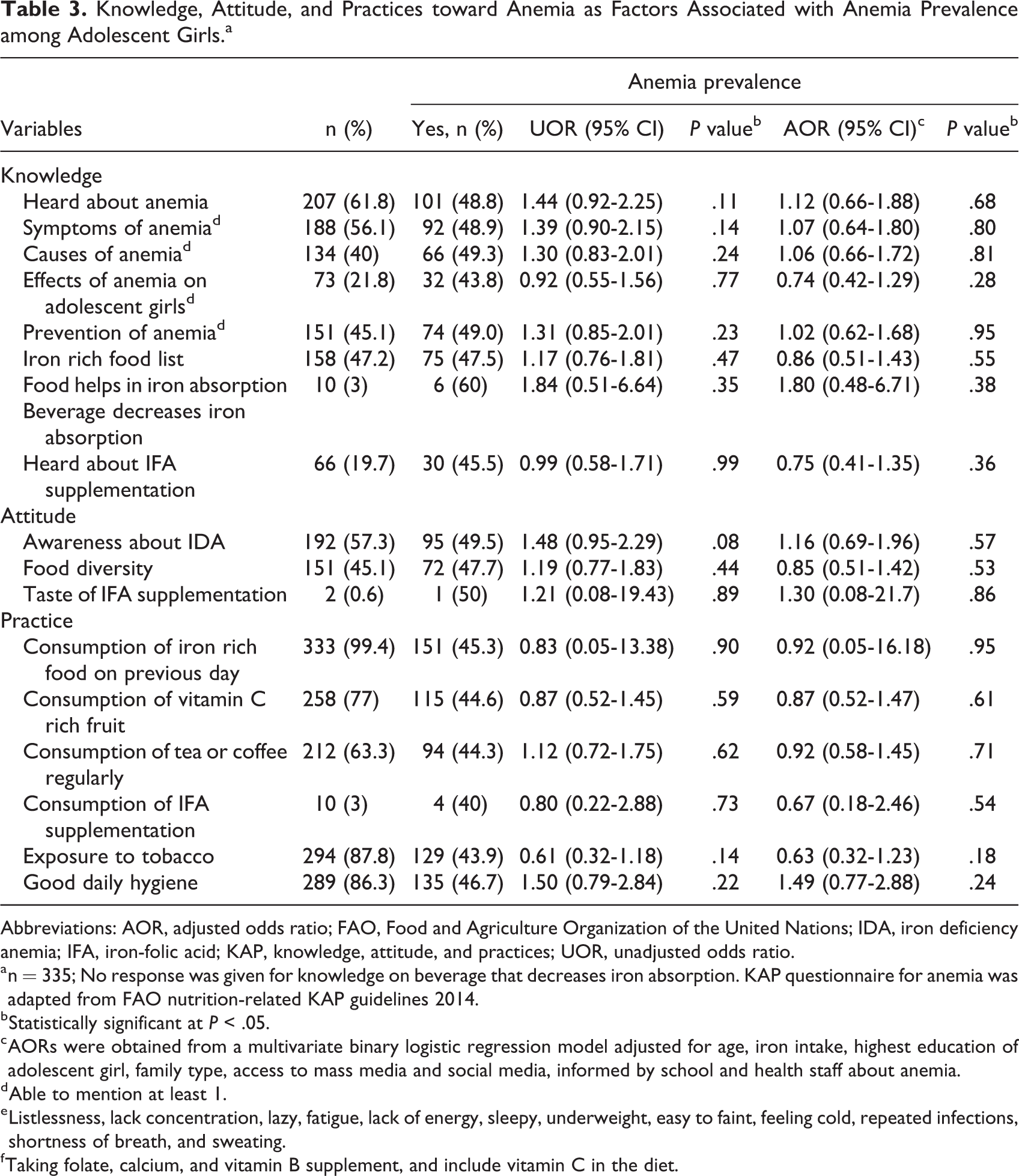
Abbreviations: AOR, adjusted odds ratio; FAO, Food and Agriculture Organization of the United Nations; IDA, iron deficiency anemia; IFA, iron-folic acid; KAP, knowledge, attitude, and practices; UOR, unadjusted odds ratio.
a n = 335; No response was given for knowledge on beverage that decreases iron absorption. KAP questionnaire for anemia was adapted from FAO nutrition-related KAP guidelines 2014.
b Statistically significant at P < .05.
c AORs were obtained from a multivariate binary logistic regression model adjusted for age, iron intake, highest education of adolescent girl, family type, access to mass media and social media, informed by school and health staff about anemia.
d Able to mention at least 1.
e Listlessness, lack concentration, lazy, fatigue, lack of energy, sleepy, underweight, easy to faint, feeling cold, repeated infections, shortness of breath, and sweating.
f Taking folate, calcium, and vitamin B supplement, and include vitamin C in the diet.
Association between Knowledge, Attitude, and Practices Score and Anemia among Adolescent Girls.a
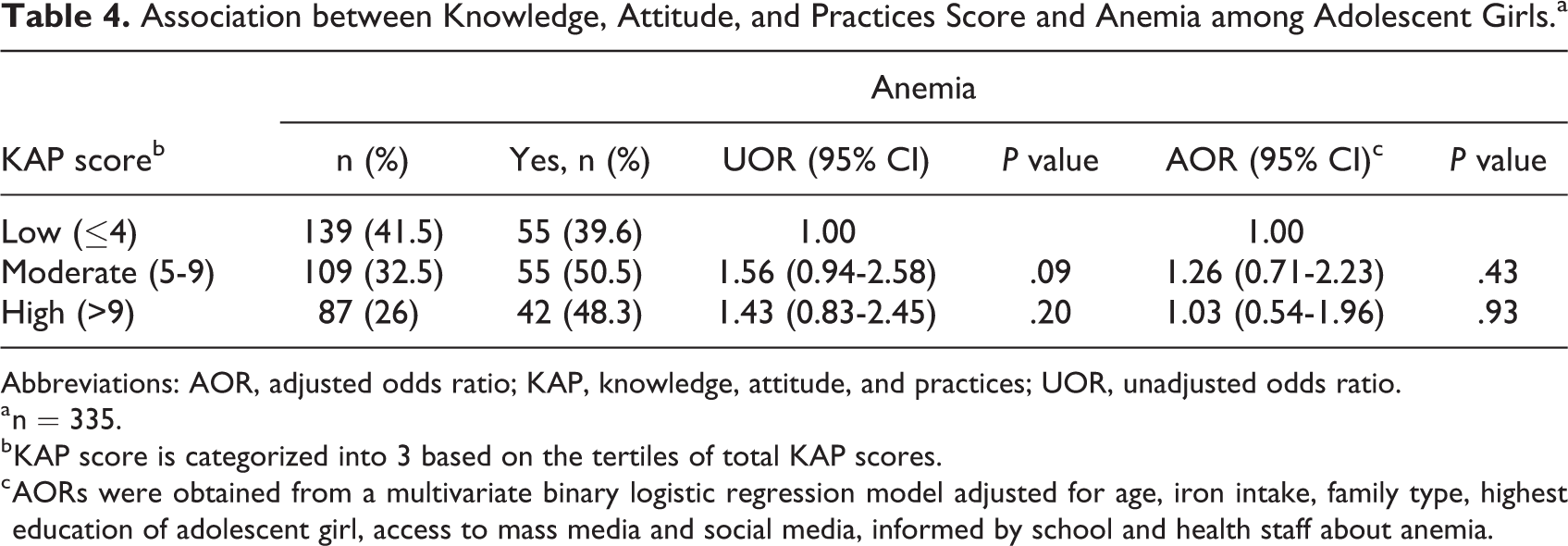
Abbreviations: AOR, adjusted odds ratio; KAP, knowledge, attitude, and practices; UOR, unadjusted odds ratio.
a n = 335.
b KAP score is categorized into 3 based on the tertiles of total KAP scores.
c AORs were obtained from a multivariate binary logistic regression model adjusted for age, iron intake, family type, highest education of adolescent girl, access to mass media and social media, informed by school and health staff about anemia.
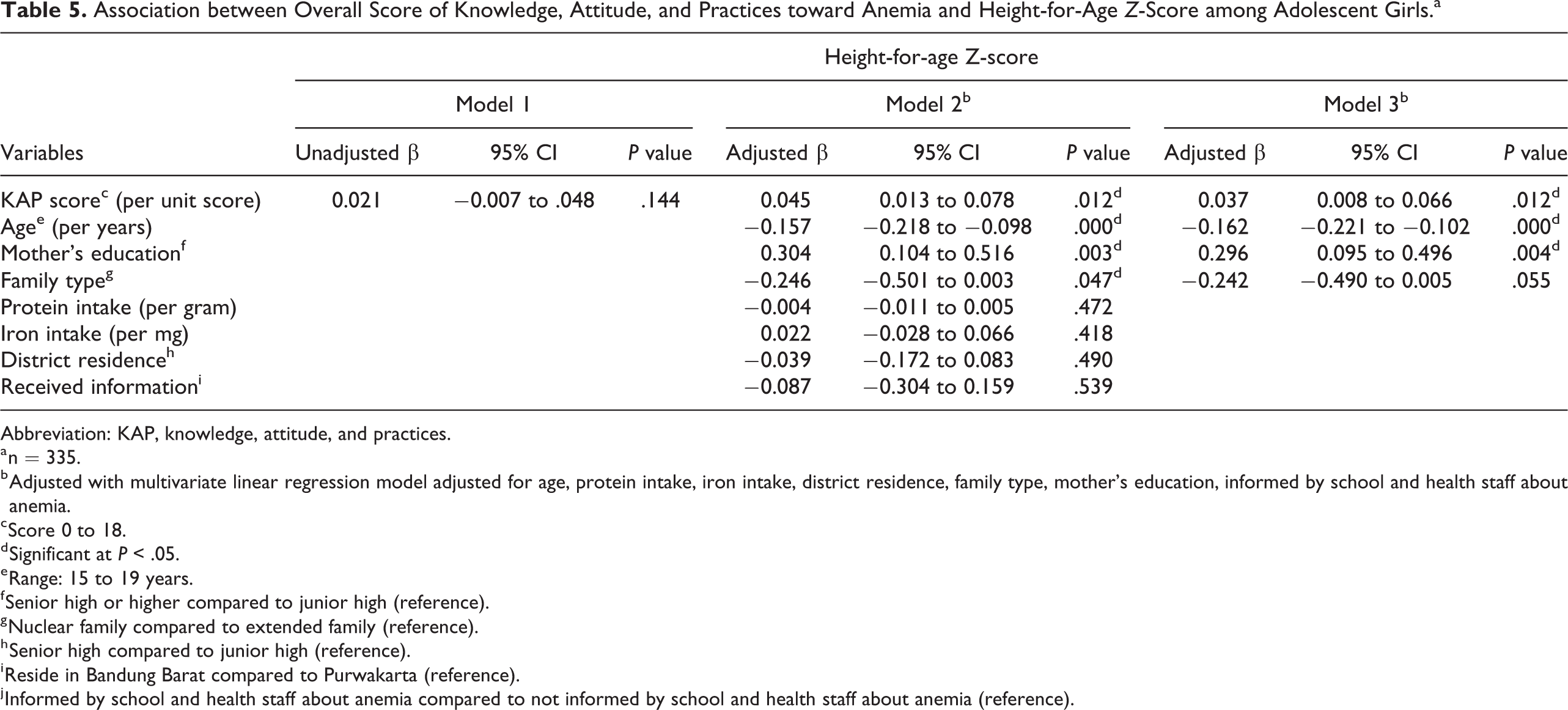
On the other hand, the KAP score was associated with HAZ score, as seen in the linear regression model (Table 5). Every increment of 1 point of the KAP score was associated with an increase in HAZ of 0.045 SD after adjustment for age, protein intake, iron intake, the district of residence, the family type, the mother’s education, and the availability of anemia information from school and health staff. The association of KAPs and HAZ remained significant (adjusted β = 0.037 SD, 95% CI = 0.008-0.06, P value = .012) even after removing several covariates, except for age, mothers’ education, and family type in the linear regression model. Some individual KAP variables also showed a protective tendency to stunting (Supplementary 4). Meanwhile, a higher level of maternal education was associated with an increased HAZ. A high KAP score also tended to be protective of stunting in a logistic regression model (Figure 2 and Supplementary 5) compared to a low KAP score (AOR 0.49, 95% CI = 0.21-1.11, P value = .09).
Association between Overall Score of Knowledge, Attitude, and Practices toward Anemia and Height-for-Age Z-Score among Adolescent Girls.a
Abbreviation: KAP, knowledge, attitude, and practices.
a n = 335.
b Adjusted with multivariate linear regression model adjusted for age, protein intake, iron intake, district residence, family type, mother’s education, informed by school and health staff about anemia.
c Score 0 to 18.
d Significant at P < .05.
e Range: 15 to 19 years.
f Senior high or higher compared to junior high (reference).
g Nuclear family compared to extended family (reference).
h Senior high compared to junior high (reference).
i Reside in Bandung Barat compared to Purwakarta (reference).
j Informed by school and health staff about anemia compared to not informed by school and health staff about anemia (reference).
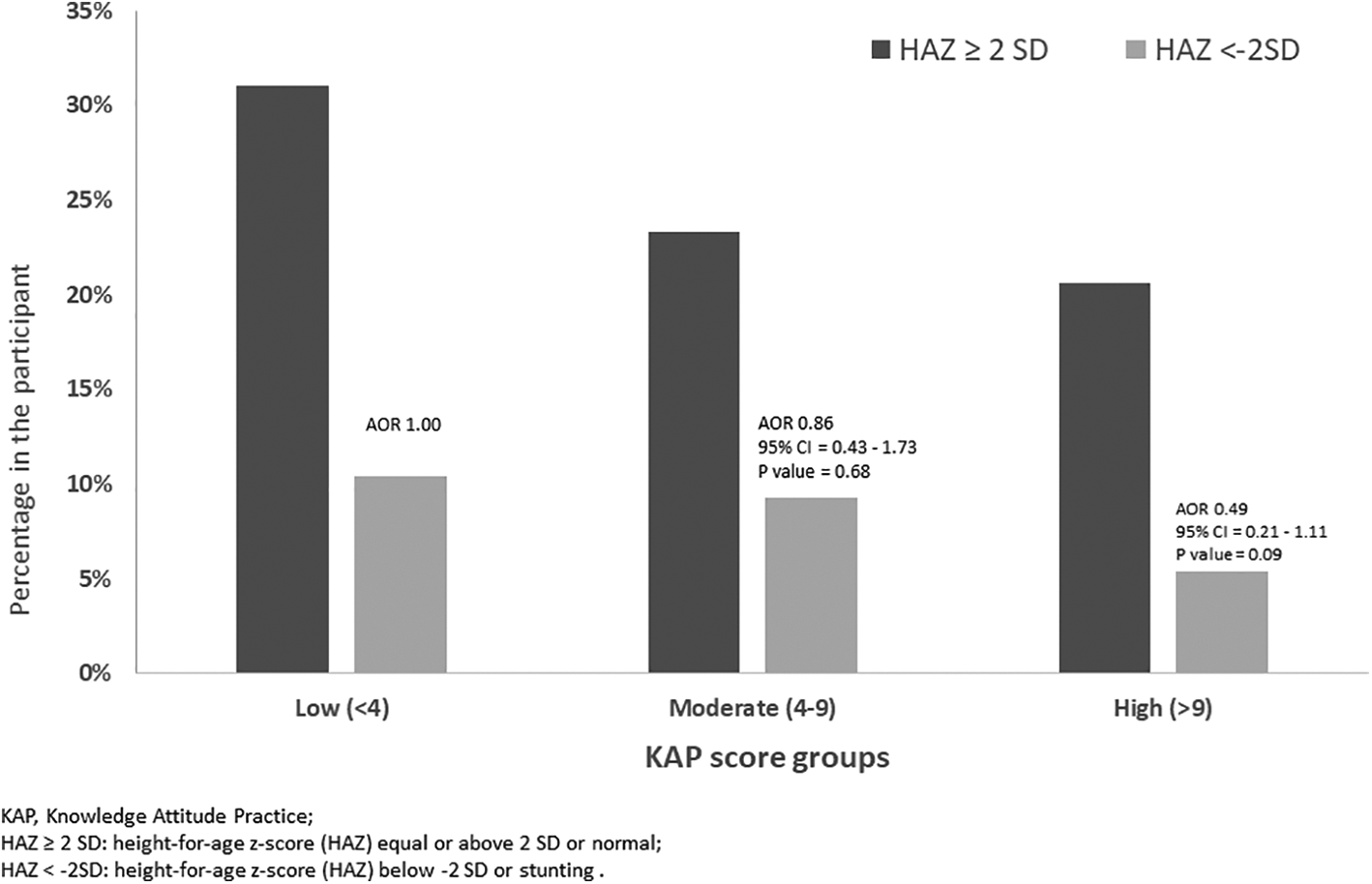
Association between knowledge, attitude, and practices scorea toward anemia and HAZ <−2 SD among adolescent girls (n = 335). aKAP score is categorized based on the tertiles of total KAP scores. AORs were obtained from a multivariate binary logistic regression model adjusted for age, protein intake, iron intake, district of residence, family type, mother’s education, informed by school and health staff about anemia. AOR indicates adjusted odds ratio; HAZ, height-for-age z-score; KAP, knowledge, attitude, and practices; SD, standard deviation; UOR, unadjusted odds ratio.
Discussion
The present study indicates that individual and overall KAP scores were not associated with anemia. Having high or moderate KAP scores compared to having low KAP score toward anemia was not associated with lower odds of being anemic in adolescent girls. Meanwhile, the overall KAP score toward anemia was associated with HAZ score among adolescent girls in this study area with a high prevalence of anemia and stunting. The increment of KAP score is linear with a significant increase in HAZ by 0.037 SD. The association remained significant with the inclusion of several or fewer covariates in the linear regression model. Adolescent girls with a high KAP score also tended to be protected from stunting.
The prevalence of anemia in the current study (45%) is relatively high, compared to the national prevalence at the time of data collection (18%-26%) 36 or within the known range of prevalence in West Java of 36% to 56%. 37 The current analysis did not show any significant association between KAP toward anemia with the occurrence of anemia in adolescent girls. A direct association between KAP toward anemia and its prevalence among adolescent girls has been suggested by studies in LMICs, for example, India, Palestine, and Sierra Leone, but the results were not conclusive. 20,38 -40 Attitude and practice scores were significantly correlated with hemoglobin levels in several studies. 20,39,41 Another study showed that hemoglobin level was significantly associated with regular intake and the meal-related time of iron supplement consumption in pregnant women but was not associated with receiving counseling regarding iron supplements. 25 A study in South Sulawesi, Indonesia, showed a direct negative association between consumption of a balanced diet and hypochromic microcytic anemia in adolescents (P = .048) without associations between anemia and the knowledge and attitude toward a balanced diet. 42 The different findings between the current studies and the others can be due to differences in the study design, use of the KAP questionnaire and scoring system tools, and population characteristics. The present study involved a study population that had not been given any intervention and education related to anemia prevention.
Distal factors to health outcomes (Figure 1), such as education, support a better KAP score toward anemia based on previous reports. 27,28 The accessibility of education in the form of mass and social media information could be obtained at any time and in any location. Such information could influence the population’s perspective and lifestyle depends on the reliability of the source. 43 The current finding on access to mass and social media and its inverse relationship with hemoglobin value marks the role of information channels in health behavior. The inability to access credible, reliable, and accurate information may negatively impact the knowledge of the population in general. 44 Public health intervention of nutrition education in adolescent girls has been reported to be successful in improving the KAP score toward anemia. 45,46 However, if the knowledge is not practiced well, it will not be effective in preventing anemia, as reported in the KAP toward anemia study in Bangladeshi adolescent girls. The study suggested education alone did not guarantee a direct association with lower anemia prevalence. 47 Access and compliance in IFA or multiple micronutrient supplementations still had prominent roles in reducing the risk of anemia. 47,48
The lack of association between KAP toward anemia and anemia prevalence in this study may have happened due to recall bias. Some KAP variables, such as the knowledge of beverages that decrease iron absorption and IFA tablets consumption, were experienced by only a few participants, causing only a small number that could be used for comparison between cases. However, efforts to control error from recall bias have been performed, as detailed in the Materials and Methods section.
Association between nutrition-related KAP and stunting had already been reported in previous studies. A descriptive study in a high-stunting-prevalence area reported that more than half of its school-going children had very poor nutritional KAP. 49 Another study in the Indonesian population also reported the anemia and stunting co-occurrences. The study suggested that iron supplementation and proper diet were also important in stunting prevention. 50 The adolescent girls in this population, as reported in another study in the same population, had poor dietary quality and diversity, implying a possible risk for micronutrient fulfillment. 26 The association between KAP toward anemia and HAZ in this study can be explained by the possibility of shared risk factors between anemia and linear growth impairment, such as household socioeconomic status, education, and childhood nutrition support as obtained by other studies. 1,28,30,51
Twelve of 18 variables of the current study’s KAP toward anemia questionnaire (Table 1) addressed aspects regarding nutrition, food diversity, and a healthy environment for both anemia and stunting. The education related to anemia content often overlaps with nutritional education. Understanding the importance of dietary habits, micronutrients, hygiene, sanitation, and disease prevention were emphasized in the efforts to reduce the risks of anemia and stunting. 30,52 Micronutrients are essential for both anemia and stunting prevention. An intervention study in Nepal showed that micronutrient powders, containing various vitamins and minerals, decreased both stunting and anemia prevalence in children. 53 Nutrient intake and dietary diversity improvement in anemia prevention conducted in Malawi were also shown to improve HAZ and reduce stunting prevalence. 54 Also, hygiene affects both anemia and stunting. Poor sanitation and hygiene contribute to a low hemoglobin level and anemia. 55 -57 Moreover, exposure to cigarette smoking, including being a passive smoker, is not only a risk for anemia but also a factor that is inversely associated with height in the growth period. 58 In general, the family is the initial source of information. Studies showed the positive impact of a mother’s education in their children’s knowledge and practice toward healthy behaviors. 51 The current study also observed the possible effect of the mother’s level of education in shaping the adolescent girl’s KAP and HAZ level. It was also reported that mother’s insufficient knowledge significantly increased the risk of stunting to more than 4-fold. 59 Therefore, it is possible that the association between the adolescent’s KAP toward anemia and HAZ level observed in this study was due to the mother’s knowledge and practice of child health which were transferred to their children, considering no intervention was taken in the current study.
Previous studies only evaluated or associated one of the individual KAP components with anemia incidence rather than associating overall KAP with anemia. 20,38 -40 To date, the present study is among a limited number of studies to have been conducted in LMICs to investigate the association between individual and overall KAP score with anemia and linear growth among adolescent girls. This study represents reliable findings, with good correlations between variables among participants’ KAP, in addition to the Cronbach α value of 0.71, indicating good internal consistency of items of the scales used in the questionnaire, 35 the use of a systematic random sampling method, as well as the involvement of trained enumerators and the application of pretested tools to minimize bias and error in participant selection and data collection. Although, due to the cross-sectional nature of the study, it cannot be concluded that by improving the KAP score, the possibility to be stunted will decrease.
This study results suggested that education toward anemia alone may not effectively prevent anemia. Direct known intervention such as micronutrient supplementations needs to be considered along with education related to anemia. 48 Moreover, in populations where anemia and stunting co-occurrence existed, public health intervention strategies should be prioritized and implemented in an integrative way. 60 Cohort or intervention study on KAP toward anemia is necessary to be carried out to confirm the current study’s findings.
Conclusions
The KAP toward anemia was not associated with anemia prevalence but was positively associated with increased HAZ among adolescent girls. Having high or moderate KAP score compared to having low moderate score toward anemia was not associated with the odds of being anemic in adolescents girls. Meanwhile, higher KAP toward anemia among adolescent girls was associated with higher HAZ. Strategy to reduce the risk of anemia in this population should combine KAP improvement with other known effective nutrition intervention (eg, micronutrient supplementation). Public health and nutrition education should integrate aspects that could contribute to anemia and stunting co-occurrence prevention.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721211011136 - Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721211011136 for Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls by Rina Agustina, Fadila Wirawan, Arini A. Sadariskar, Ainanur A. Setianingsing, Khairun Nadiya, Erfi Prafiantini, Eriana K. Asri, Tutut S. Purwanti, Sri Kusyuniati, Elvina Karyadi and Manoj K. Raut in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721211011136 - Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721211011136 for Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls by Rina Agustina, Fadila Wirawan, Arini A. Sadariskar, Ainanur A. Setianingsing, Khairun Nadiya, Erfi Prafiantini, Eriana K. Asri, Tutut S. Purwanti, Sri Kusyuniati, Elvina Karyadi and Manoj K. Raut in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-3-fnb-10.1177_03795721211011136 - Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls
Supplemental Material, sj-pdf-3-fnb-10.1177_03795721211011136 for Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls by Rina Agustina, Fadila Wirawan, Arini A. Sadariskar, Ainanur A. Setianingsing, Khairun Nadiya, Erfi Prafiantini, Eriana K. Asri, Tutut S. Purwanti, Sri Kusyuniati, Elvina Karyadi and Manoj K. Raut in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-4-fnb-10.1177_03795721211011136 - Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls
Supplemental Material, sj-pdf-4-fnb-10.1177_03795721211011136 for Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls by Rina Agustina, Fadila Wirawan, Arini A. Sadariskar, Ainanur A. Setianingsing, Khairun Nadiya, Erfi Prafiantini, Eriana K. Asri, Tutut S. Purwanti, Sri Kusyuniati, Elvina Karyadi and Manoj K. Raut in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-5-fnb-10.1177_03795721211011136 - Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls
Supplemental Material, sj-pdf-5-fnb-10.1177_03795721211011136 for Associations of Knowledge, Attitude, and Practices toward Anemia with Anemia Prevalence and Height-for-Age Z-Score among Indonesian Adolescent Girls by Rina Agustina, Fadila Wirawan, Arini A. Sadariskar, Ainanur A. Setianingsing, Khairun Nadiya, Erfi Prafiantini, Eriana K. Asri, Tutut S. Purwanti, Sri Kusyuniati, Elvina Karyadi and Manoj K. Raut in Food and Nutrition Bulletin
Footnotes
Authors’ Note
RA, EP, and MKR wrote the grant, designed, and conducted the study. AASe, FW, KN, AASa, and RA analyzed the data and drafted the manuscript. RA coordinated and decided on the final submission of the manuscript. EA, TSP, SK, EK, and MKR supervised the study preparation and final proofed the manuscript. All of the authors read and approved the final manuscript. The data set used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Acknowledgments
We thank all the adolescents and their parents for their enthusiasm in participating in the study. We thank all field supervisors, field pre-listers, and enumerators, who diligently and enthusiastically performed their task during the study conduct. We thank kaders (volunteer women), head of district, head of sub-district, head of villages, and local government in providing their assistance and cooperation in meeting the study subjects. We thank Winda Hutami for her technical assistance in conducting the study, and Okky Lupita in finalizing the data analyses. We thank Dr Fiastuti Witjaksono, Prof Budi Wiweko, Dr Yoga Devaera, and Lestari Octavia for their advices on the study proposal, project report, or paper development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work had been commissioned with a grant from Nutritional International’s (formerly Micronutrient Initiative) Right Start Project in Indonesia through the financial assistance of the Government of Canada through Global Affairs Canada (GAC) and the Ministry of Research, Technology, and Higher Education of the Republic of Indonesia (No. 1/E1/KP.PTNBH/2019 and 234/PKS/R/UI/2019). The funding body (GAC) had no role in the study design, collection, analysis or interpretation of data, or writing of the manuscript. The views expressed in this publication are of the authors and do not necessarily represent the views, decisions, or policies of the institutions with which the authors are affiliated.
This study and the manuscript based on the survey data collected as part of this program in two districts of West Java province, which supported the institutionalization of an innovative pilot demonstration of a health system strengthening initiative and approach, helped tailoring the support to the scaled implementation of an improved program model with increased Behaviour Change Intervention/ communication strategy and messaging based on the insights on knowledge, attitudes and practices about anaemia and about benefits of IFA collected in this study to reduce anemia among in-school adolescent girls in selected districts of selected provinces of West Java, Banten, East Java, and East Nusa Tenggara in Indonesia. In addition, it is a welcome addition and precursor to the literature on designing programs geared towards the reduction of anaemia among adolescent girls through IFA supplementation and promotion of minimum dietary diversity among in-school adolescent girls in a school based platform. It created a foray into adolescent nutrition programming, where high levels of anemia is quite prevalent among adolescent girls.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.