
Abstract
The moral imperative of public health systems is to maximize the health and welfare of the population to the extent possible. Constraints often include a lack of resources, political will, popular acceptance, or an acceptable safety margin. Major agencies have established iron, iodine, and vitamin A as the principal elements for micronutrients, with folate and zinc on the second plane. As the armamentarium of interventions to favor micronutrient nutrition, for example, preventive health measures, dietary improvement, forms of fortification, and nutrient supplements, is offered in public health policy. The utility of their merger with other nutrients, emergent nutrients, has been considered. The Latin America and Caribbean Region has unique characteristics. The scientific and epidemiology considerations for action in the Region’s health concern on 4 emergent nutrient deficiencies of public health—vitamins D and E, essential fatty acids, and choline—are reviewed.
Plain language title
Micronutrient Deficiencies of Interest in Latin America and the Caribbean
Plain language summary
The diets consumed in the diverse corners and societies in the nations of Latin America and the Caribbean area do not fully supply the vitamins and minerals needed by people of all ages and conditions. Some public health actions are being taken, but only against a limited selection of such nutrients as iron, vitamin A, iodine, and folic acid. The composition of diets and environmental conditions across the region suggests that 4 additional nutrients might be candidates for public health efforts. These include vitamin D, vitamin E, certain large fatty acid molecules, and choline.
Introduction
Public Health Nutrition: Prelude to Action
Fundamental nutritional biochemistry in the laboratory, before and during World War II, and a surge of interest in addressing deficiencies at a global level by the newly formed agencies of the United Nations, namely the World Health Organization (WHO), the Food and Agriculture Organization (FAO), and the United Nations Children’s Emergency Fund (UNICEF), all of them with interests in nutritional health began to focus their attention and resources in nutrition. 1,2 What dominated the action agenda was so-called protein-calorie (protein-energy) malnutrition, the dramatic manifestations of which, and high mortality intrigued and captivated interest. 3 The family of vitamins and most of the essential minerals, “micronutrients,” had been identified in the 1940s and 1950s. Again, it was the dramatic nature of overt deficiency manifestations and the implication of lethality that moved the UN agencies into public health action. Iodine deficiency produced goiters, cretinism, and fetal loss; its eradication has been championed by UNICEF, without which little progress is likely to have been made. World Health Organization oversaw the treatment of hypovitaminosis A, which produces severe ocular lesions, often leading to blindness. Mortality was associated with the consequences of blindness and to a propensity of vitamin A deficit to promote fatality in measles, which was then a prevalent infectious disease. Anemia was easy to diagnose and was found to be common in infants and women of reproductive age; anemia per se, however, is not exclusively of nutritional origin.
Historically, the treatment to endemic nutrient deficiencies depends on the convergence of (1) the state of science and technology; (2) the infrastructure delivery and surveillance outreach to the affected population; and (3) the policy and decision-making to bring resources to the task of combating a deficiency. There are 2 manners to view a definition and assessment of “nutritional deficiency.” One relates to the reserves or functional stores of a nutrient in the body; the other relates to the usual consumption of a nutrient in relation to the recommendation. They are both useful, although distinct, and one does not necessarily associate with the other. This is due to the fact that the amount of nutrient placed in the mouth and swallowed does not necessarily get into or remain in a nutritionally relevant and measurable pool. This is a concept introduced in 1973 by Herbert, 4 and subsequently refined, see Table 1.
The Possible Causes of Nutrient Deficiencies in Humans.a
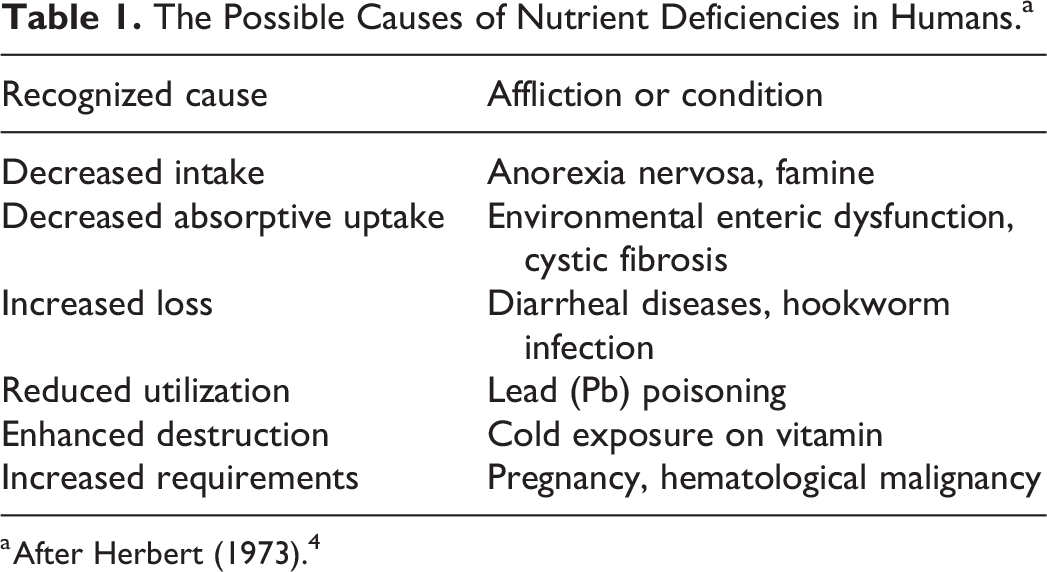
a After Herbert (1973). 4
The decision to invest resources in a campaign to improve the status of one or another nutrient, however, depends on the priority it achieves in the public health agenda. It can be argued that there are at least 4, if not more, emerging micronutrients that merit consideration for action. These are discussed here in the Latin American context.
Conditions in Latin America and the Caribbean and Insights on Micronutrient Status
Before one pronounces on or generalizes about a dietary or nutritional phenomenon, one must consider both the diversity and the commonality of the Region is composed of descendants of the original, indigenous inhabitants, those descended from the various colonizing countries of Europe (Spain, Portugal, France, the Netherlands, and Britain), and specific ethnic groups brought by the latter. The geography and topography are truly differentiated as well, with oceans, rivers, and lakes as waterways, along with deserts, grasslands, highlands, woodland forests, and tropical rainforests. Populations live on the shorelines of the Atlantic and Pacific Oceans and the Caribbean Sea, as well as at altitude in highlands from the Mexican and Central American Sierras and the South American Andes. Two major commonalities of the Region stand out. First, most of LAC is in the Tropics; only Uruguay does not have at least part of its territory below the Tropic of Cancer and above the Tropic of Capricorn. Second, LAC is the most heavily iced of regions, with 82% living in areas classified as “urban.” 5 In addition, one-third of the population of LAC earns below the poverty line, having been exacerbated by the COVID-19 pandemic. From the diversities outlined, ethnic cuisines, climatic and soil suitability for specific crops and livestock, and agronomic practices can be influential in what is available and selected to be consumed.
Vitamin D and Its Deficiency
Vitamin D is required for calcium metabolism and bone mineralization. As such, the original, and simplistic, history of vitamin D deals with the clinical condition of rickets which was prominent in the tenement-based slums of London in the mid-19th century, where sun exposure was severely limited. Eventually, the consumption of cod-liver oil became a prophylactic measure in Europe and North America. Recent investigation has found the biology and role of vitamin D is much more complex.
Chemical nature and dietary sources
Vitamin D has 3 primary vitamer forms: cholecalciferol (base form); 25-hydroxy cholecalciferol (transport form), and 1,25-hydroxy cholecalciferol (the active vitamin, acting through interaction with an intracellular system). For vitamin D, there are both dietary sources and an environmental-exposure source.
A form of endogenous cholesterol is converted into vitamin D at the dermis level of the skin. As stated, LAC is largely tropical in its geography. Heavily pigmented populations of African ascent have been settled on the islands of the Caribbean, the Central American Atlantic coastal regions, in the north and northeast of Brazil, and even in some coastal regions of Andean nations. Their skin color would reduce vitamin D biosynthesis in this segment, as would that of indigenous residents, as compared to Latin Americans of European ascent.
Also, for the Region, accessibility to rich dietary sources of vitamin D and preferential places for them in distinct cuisines is problematic. The richest sources are oily fish (salmon, cod, herring, and sardines), fish oils (such as cod-liver oil), egg yolk, meats, and some mushrooms. Notably, dairy products such as milk, yogurt, and butter, as well as margarine and some breakfast cereals, are generally and voluntarily fortified. Commercial milk and dairy became sources of this vitamin, in part, as they are fortified with the vitamin as ergosterol or cholecalciferol. In the Region, the many populations living in the highlands would be out of the range of a marine fish market 6 while African and indigenous ascendant individuals have an increased propensity to lactose intolerance and may eschew dairy foods. Cuts of beef liver and red meat are prohibitively expensive for those with limited resources.
Recommended daily intakes
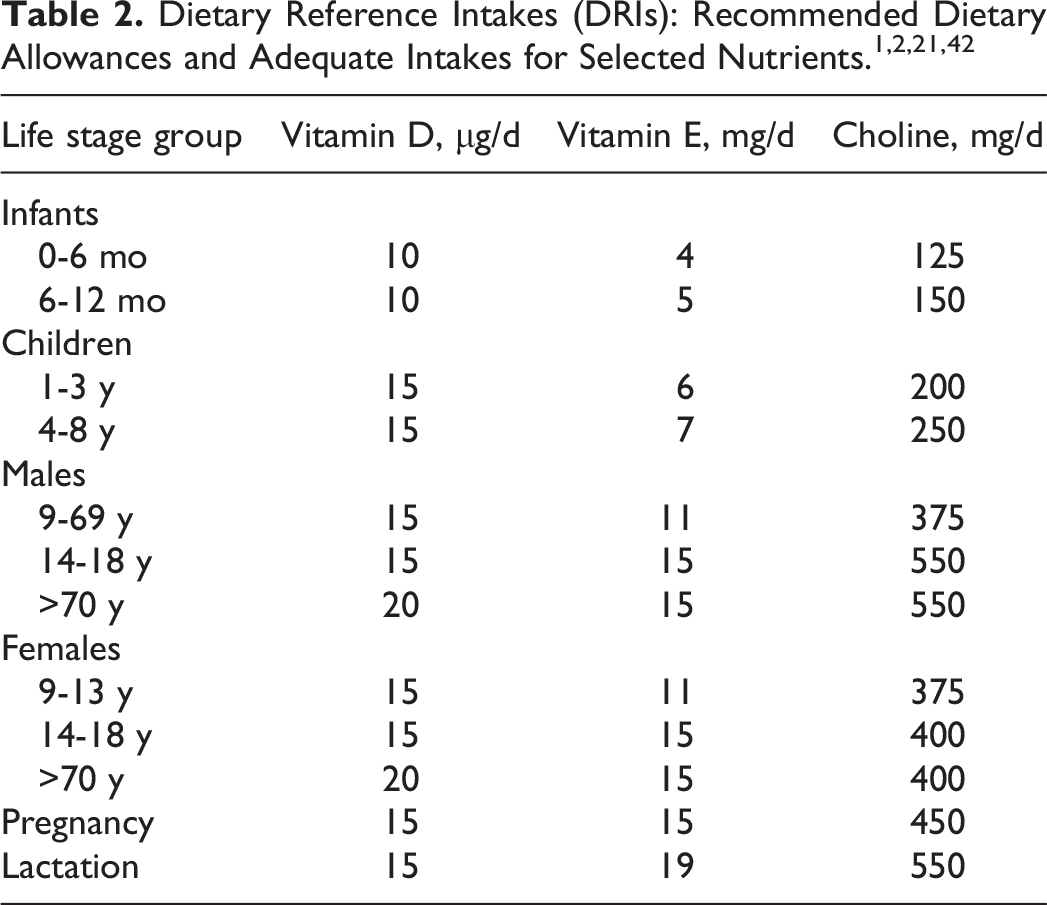
The combined solar and dietary contribution of vitamin D in the diet has implications for understanding intake recommendations. A current array of daily recommended intakes has been first prepared by the Food and Nutrition Board of the US National Academy of Sciences, revised in 2011 2 for the amount of the vitamin to be consumed to meet requirements see Table 2. The 2011 revision involved a doubling of recommendations, such that the adult indication went from 200 IU (5 µg) to 400 IU (10 µg). 2 The corresponding recommended intake from the United Nations agencies of FAO and WHO, emitted in 2004 (but elaborated in 1998) specifies 200 IU. 1
Public health implications
Circulating levels of 25-OH vitamin D represent a reliable biomarker of nutritional status. 7 The most commonly used convention is a 3-tiered cut-point system: deficient: <20 ng/mL (<50 nmol/L), insufficient: 20-30 ng/mL (50-75 nmol/L), sufficient: >30 ng/mL (>75 nmol/L).
Vitamin D may best be considered as a reemerging vitamin. As its deficiency leads to nutritional rickets, which was widely prevalent in the nations of North America and Europe. Beyond the intestinal and bone-level role of the vitamin in regulating bone mineralization, a broad constellation of non-osseous functions and actions has come to light over the past 2 decades. These are far too numerous to be detailed here but have important public health implications across the LAC region.
The source of vitamin D for first-semester infants would be human milk, and 200 IU (5 µg) of the vitamin would be required from this source daily. Numerous studies of the milk from Guatemalan mothers of all social strata have failed to find any whose estimated breast milk delivery would supply adequate vitamin (Zamora A: Unpublished findings).
A decade ago, Brito et al 8 reviewed the extant literature on vitamin D status from circulating 25-OH vitamin D reports in various nations of the Region. The theme has more recently been updated by Mendes et al, 9 writing from Brazil. Both documents were universally reflective of insufficient (20-30 ng/mL) and deficient (<20 ng/mL) concentrations of the biomarker. More recent publications have followed this pattern. Also, in Guatemala, we have documented the status of vitamin D, in elderly Mayan adults from the highlands. Sud et al 10 found an elevated prevalence of insufficiency and deficiency (96%) with women significantly poorer than men (48.4 vs 58.2 nmol/L), and rural lower than urban (47.4 vs 55.0 nmol/L). In a Caribbean coastal population of school children were divided among those with largely African ascent (Garifuna) and Mayans transmigrated from a highland setting (Kekchi). Paradoxically, the former had higher levels than the latter (29.8 ng/mL vs 25.8 ng/mL), but with insufficiency elevated overall (insufficient and deficient vitamin D: 72% in Mayans and 56% in African ascent). 11
There is active investigative interest in the ancillary functions and benefits of vitamin D at the present moment. The noted nutrition epidemiologist, Walter C. Willett has concluded in a lecture at the International Congress on Nutrition in Tokyo in 2022 that some level of vitamin D supplementation should be taken universally, depending on age and latitude of residence.
Options for action for vitamin D
The public health intervention strategies can be classified into 4 levels. The first is to eliminate ailments or conditions that interfere with their utilization as in the Herbert scheme. 4 For instance, the treatment of hookworm disease can stem the loss of blood a effectively eliminate iron deficiency anemia. 12 Similarly, treatment with sex hormones can reduce iron loss among women with excessive bleeding across the menstrual cycle. The second is to diversify of food selection to include greater amounts of a source(s) of the nutrient of interest. What is often not recognized on a programmatic basis are the trade-offs of substitution; that is the new foods have an energy content that can cause caloric imbalance or lack other nutrients that are marginal in the diet or challenge the household economy with their additional costs. There also may be cultural preference barriers to adopting greater intakes of a certain new nutrient source.
The third is fortification, which involves adding additional value to the diet by adding specific nutrients. This is usually as food fortification, 13,14 incorporating nutrients during processing. Within this realm of intervention is a specific variant called “biofortification” 15 -18 in which the nutrient(s) content of the edible portion by cross-breeding, genetic engineering is increasing the nutrient content of fertilizer or fodder. The final approach is supplementation with high-dose, and often periodic application, most common by an oral route, but occasionally by parenteral injection. 19
All 4 approaches apply to vitamin D. In the particular instance of vitamin D, there exists the unusual, but practical, approach of optimizing your solar exposure by adjustments in wardrobe attire and/or duration out of doors. Achieving these behavioral modifications would require education. No specific health interventions. Expansion of consumption of dairy products, fortified with vitamin D, might be achieved with concerted promotional actions. Reduction in the lactose content may increase the general acceptance in the Region, in which lactose intolerance is common. 20 The supplementation of vitamin D may be as justified in LAC as in the low latitudes of Canada.
Vitamin E and Its Deficiency
Vitamin E is a family of 16 vitamers: 8 tocopherols and 8 tocotrienols. The most common and biologically active is alpha-tocopherol, and for practical purposes in nutrition, it is the active nutrient. Vitamin E finds its nutritional role as an antioxidant in the lipid layer of cell membranes.
Recommended daily intakes
The nutrition community has 2 dispersed options for recommendations for daily intakes of alpha-tocopherol. Those of the US-Canadian dietary reference intakes dating to 1998 21 and shown in Table 2, and the second from the United Nations agencies of FAO and WHO, 2 elaborated in 1998 and released for publication in 2004. The estimates for daily recommendations for adults and most other groups of populations differ by being 50% less in the latter. The North American estimate for adults is 15 mg/day whereas that from the UN agencies is 7.5 mg. The magnitude of this discrepancy makes assessment of intake deficits difficult from survey data.
Public health implications
More or less adequate dietary intake of vitamin E would depend on the degree of consumption of rich sources of the vitamin, notably as alpha-tocopherol. Edible oils are the most commonly consumed sources of vitamin E. Wheat germ oil is the richest source (133 mg of alpha-tocopherol/100 g) followed by sunflower oil (48 mg); palm, peanut, and corn (maize) oils are moderate, whereas soybean, olive, and coconut oil are depleted (<10 mg). 21 Of course, local cuisine can be a determinant of its consumption; for instance, corn tortillas, tamales, and arepas are prepared without frying and with minimal oil. Nuts and seeds are also rich sources of alpha-tocopherol, but potentially problematic for young children’s diets.
Selection of dietary sources, in turn, is based on structural factors of availability (being grown or imported into an area), accessibility (ability to afford and purchase), and cultural factors such as cuisine (composition of preferred recipes and meals). Studies of the consumption of vitamin E are scarce in the Region. In lactating women in 2 regions of Brazil intakes were below UN recommendation in both Rio de Janeiro 22 and Natal. 23 All 411 adolescents in Pernambuco, Brazil, had vitamin E intakes below UN agency recommendations. 24
A provisional cutoff for low circulating alpha-tocopherol is >11 µmol/L, but this is far from universal among authors. Intriguing findings from across the Region raise the correlation-causation question of observed vitamin E status, that is whether a condition or illness adversely affects status, 4 a preexisting vitamin deficiency predisposes to the adversity, or neither. Cut-off criteria were variable across the literature cited, but consistent within reports. A 3-nation collaboration in Argentina, Brazil, and Mexico demonstrated that HIV exposed/infected children had lower vitamin E status than nonexposed peers (P < .05). 25 In a survey in Lima, Peru, the household contacts of HIV-infected persons showed inferior vitamin E status than participants from families who were HIV-free (P for trend, < .005). 26 Seventy percent of preschoolers sampled in the state of Queretaro, Mexico, had deficient circulating vitamin E concentration. 27
In the metabolic domain, the homozygous state (RR) for a leptin gene polymorphism, LEPR Q223 R, in a combination of vitamin A and E deficiencies enhanced the risk factors of cardiovascular disease 28 in adolescents in Rio de Janeiro. At the other end of the age spectrum in Mexican adults over 60 years, the ∼20% prevalence of vitamin E deficiency was associated with other biomarkers and anthropometric variables in determining cardiovascular risk scores. 29 Finally, again in the area of metabolic health, in a case–control design study in healthy adults in Durango, Mexico, 30 newly diagnosed with prediabetes had lower vitamin E status than controls (P = .03).
Evidence for insufficient vitamin E states is widespread in the Region. On the one hand, in free-living individuals, deficiency of vitamin E does not produce clinical manifestations that would draw an outcry for redress. On the other hand, however, when examined in the Region, either from a dietary intake or a circulating vitamin concentration perspective, indications of insufficiency abound as shown here. The challenge is to motivate and move to action without specific visible and tangible signs.
Options for action on vitamin E
Oil, seeds, and nuts are the richest sources of alpha-tocopherol, and maximizing their consumption in the diet is the first strategy for adequacy of intake. A number of alimentary track conditions, such as tropical sprue, environmental enteropathic dysfunction, and celiac disease, reduce the efficiency of fat absorption, but not differential for tocopherols. The technology for the biofortification of oils with vitamin E is emerging. 31,32 Supplemental forms of vitamin E with dosages up to 1000 IU are available in over-the-market settings worldwide, but no population-based interventions are recognized. 30
Long-Chain Polyunsaturated Fatty Acids Omega-3 and Omega 6
All fatty acids form part of the macronutrients of the diet to store and supply energy. A small subclass of fatty acids, broadly termed “essential fatty acids,” has cellular functions that have brought them to be classified as micronutrients as well.
Chemical nature and dietary sources
Long-chain polyunsaturated fatty acids (LC-PUFAs) are fatty acids with 18 or more carbons. Although LC-PUFAs are required in higher than trace amounts, these are considered micronutrients because humans do not produce them, and they have specific metabolic functions and health-protection roles. The LC-PUFAs have 2 species defined by the configuration of the double-bonds at the methyl end of the fatty acid: omega-6 (n-6) and omega-3 (n-3). 31
The omega 6 LC-PUFA, with 18 carbons, is linoleic acid consumed primarily from edible vegetable oils, with seeds and nuts as well as eggs and meats as additional sources. The n-6 species with specific micronutrient functions is arachidonic acid with 20 carbons. Plants cannot lengthen linoleic acid to C-20, such that animal-sourced foods such as meat, poultry, fish, egg, and dairy are the dietary sources. Arachidonic acid is important in metabolic signaling and inflammatory regulation. The corresponding 18-carhon omega-3 LC-PUFA is alpha-linolenic acid found in edible oils derived from rapeseeds, flaxseeds, and soybeans. The n-3 species with specific micronutrient functions are eicosopentaenoic acid (EPA) with 20 carbons, and docohexaenoic acid (DHA) with a 22-carbon chain length. 31,32
The richest dietary sources of these fatty acids are marine fish, especially from far northern and southern oceans. 33 It is notable that small amounts of the precursor C-18 LC-PUFAs can be converted to the higher order species, but this is limited by the small capacity of the “elongate” enzyme system and the competition between n-6 and n-3 for metabolic access.
Recommended daily intakes
There are no official recommendations of daily dietary intakes of long-chain fatty acids, and consensus has not been reached in various offerings on the theme. There have been many calls for recommendations. 34 One perspective has been to observe the combined intake of DHA and EPA from foods and beverages in the diets of the US population, which are medians of 50 mg and 20 mg, respectively. 35 What is consensus is that this 70 mg of total acids is woefully inadequate.
Public health implications
Long-chain polyunsaturated fatty acids biology is extensive and elaborate, covering clotting, inflammation, mood, behavior, resolution of inflammation, cellular signaling, and regulation of transcription. For the adult population, the omega-3 Index is an issue of emerging concern. Promoted by Harris, 36 this ratio is simply the weight balance of the n-3 to n-6 in a blood sample. Its gradation across a population of adults has an association with the occurrence of cardiovascular incidents. A ratio of >8.0 proved to be virtual assurance against cardiovascular disease (CVD) whereas a ratio <4.0 was associated with an elevated incidence of events. The predominance of urban residences and lifestyles in the region militates in favor of underlying CVD risk. Unfortunately, surveillance of the omega-3 ratio in Latin American adults is limited. 36
Guatemala appears to have a situation of excessively low n-3 ratios and status. Even in a sample of women and schoolchildren on the Pacific coast, removed a bit inland from the shoreline itself, the median ratio for the women was 3.37 and the children was 3.77. 37 That is, the median ratio is below the critical level of 4.0. In Guatemala, in preschool children attending centers in the highlands, median ratios were even lower, at ∼3.2, among the lowest ever seen in a population study (Soto-Mendez: unpublished findings). The ages, diets, and lifestyles of these rural-dwelling Guatemalans in studies with CeSSIAM, however, may mitigate the strength of any association with CVD.
Long-chain polyunsaturated fatty acids are a class of micronutrients that surely have been overlooked and underappreciated in the Region. Insufficiency is not unique to the Region, but the meager and dispersed evidence available points to its widespread extent. In a global analysis of fats and oils consumption the authors confirmed that Latin America and Oceania were the 2 regions with greater statistical uncertainty when reporting seafood and plant omega-3 intakes. 38 In addition, in the latest multicentric nutritional study developed in Latin America, the authors reported data from 8 countries including, Argentia, Brazil, Chile, Colombia, Costa Rica, Ecuador, Perú, and Venezuela. Ecuador reported higher percentage of energy coming from polyunsaturated fatty acids and Chile showed the lowest percentage when compared to the rest of nations, 9% and 7%, respectively. 39 Demography in the geographical distribution, influencing dietary habits, influences the consumption of the most important food sources of these nutrients. In the abovementioned global analysis, the authors confirmed that highest intakes of seafood omega-3 fatty acids were reported in islands nations (Maldives, Barbados, the Seychelles and Iceland) and lowest intakes in Zimbabwe, Lebanon, the Palestinian territory, Botswana, and Guinea-Bissau. 38 An additional consideration is the multi-milligram amounts for daily consumption to meet estimated physiological needs, sparsely contained in the food supply.
Options for action for LC-PUFAs
The ratio of total omega-6 fatty acids to total Omega-3s is a negative factor for the nutriture of the latter. An omega-6:omega-3 ratio in excess of 6 is considered to be detrimental to the latter class of fatty acids. Cultural, economic, and even geographical factors can determine nutritional status. Not all populations of the Region either have the custom or resources to consume marine-origin foods and in highland areas these sources are unavailable. Fish and shellfish from colder waters are richer in LC-PUFA, 33 whereas our Region is tropical.
As to food fortification, some lipid base is needed, as in milk, yogurt, cheese, butter, or margarine; as oral supplements of DHA and EPA for pregnant and lactating women, but widespread supplementation for this group is not common. Creative innovation is needed to address the conundrums for LC-PUFA interventions.
Choline and Its Deficiency
Choline has been considered to be an essential nutrient and has had official intake recommendations since 1998. 40
Chemical nature and dietary sources
Choline is a small, polar molecule of 104.2 g/mol. Choline exists in the organism, not in free molecular form, but rather conjugated to a number of molecular species, with these conjugates serving diverse functions. The best known is acetylcholine, a “cholinergic” neurotransmitter, but also occurs in phospholipids, including phosphatidylcholine and others, associated with cell membranes.
The principal choline-rich foods for human consumption, ordered by the content of the nutrient are organ meats, eggs, beef, soybeans, chicken breast, and fish, 41 majority of which are animal-sourced foods, with affordability challenges for those of lower economic means. Limited amounts are found in some mushrooms and legume seeds.
Recommended daily intakes
Despite the obscurity in nutritional interest, which is reflected in the scarcity of information available on the intake of this nutrient in the Latin American region, choline is relatively abundant. Among the micronutrients, only calcium and phosphorus have daily intake recommendations in excess of those for choline on a weight per day, and marginally higher than magnesium. The column in Table 2 gives the recommended dietary allowances and adequate intakes for this nutrient. 42 Accordingly, an exclusively breastfed infant would need 125 mg. Adult men and lactating mothers have a recommended intake of over half a gram.
Public health implications
Florid choline-deficiency manifestations are not found in free-living human populations. Zeisel and da Costa, 42 however, outline the potential roles of low choline intakes in hepatic diseases and cardiovascular illness. There is no reliable biomarker for human choline status. Dietary intake provides the only window. A limited number of survey data on choline intake have come from the Region and have been published from Mexico, Brazil, and Guatemala, the majority in the context of oral intervention trials. 43 -48 Most showed intakes of the participants well below the recommended levels. Given that rich sources of choline, such as poultry and their eggs, are mainstays in the diets even of low-income residents of LAC, with persistent low intake rates, there may not be much elasticity across that pathway. Various supplements have been explored. 22,23,25 A novel idea for consideration would be choline supplements for chickens and ducks to potentially increase its density in the white-muscle meat and the derivative eggs.
Options for action for choline
Health conditions that interfere with the utilization of choline are clearly recognized. Purified choline is bitter tasting, and levels of 450 mg achieved with the chemical form would not likely be tolerated, in its various organized forms in neurotransmitters and cellular lipids, it is palatable. Eggs and poultry are the sources most commonly accessible to the Latin American population. Oral supplementation would probably not be a justifiable solution to follow intakes with current delivery technology.
Conclusion
There would seem to be a threshold of palpable adverse consequences that a nutrient deficiency has to transcend before health authorities look for measures to reduce its prevalence in a society. Here we review current knowledge of epidemiology with respect to 4 additional micronutrients with a high potential for a concern that might prompt population or community action.
An alternative justification is one based on justice and human rights. If one accepts that all people have the human right to a nutritious and healthy diet, then some work needs to be done on the vitamin D and E density side to attain the stated goal. Vitamin D and E, LC-PUFAs, and choline are orphaned micronutrients lacking the constituency on the scientific side nor on the policy side.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241257008 - Perspective on Emerging Micronutrient Deficiencies in Latin America and the Caribbean
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241257008 for Perspective on Emerging Micronutrient Deficiencies in Latin America and the Caribbean by Noel W. Solomons in Food and Nutrition Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received financial support for the publication of this article from Fundación Iberoamericana de Nutrición-FINUT.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.